Single-Drug Approach with Edoxaban is Effective for Resolving Non-Acute Cancer-Associated Venous Thrombosis: A Single-Arm Retrospective Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Background of This Study
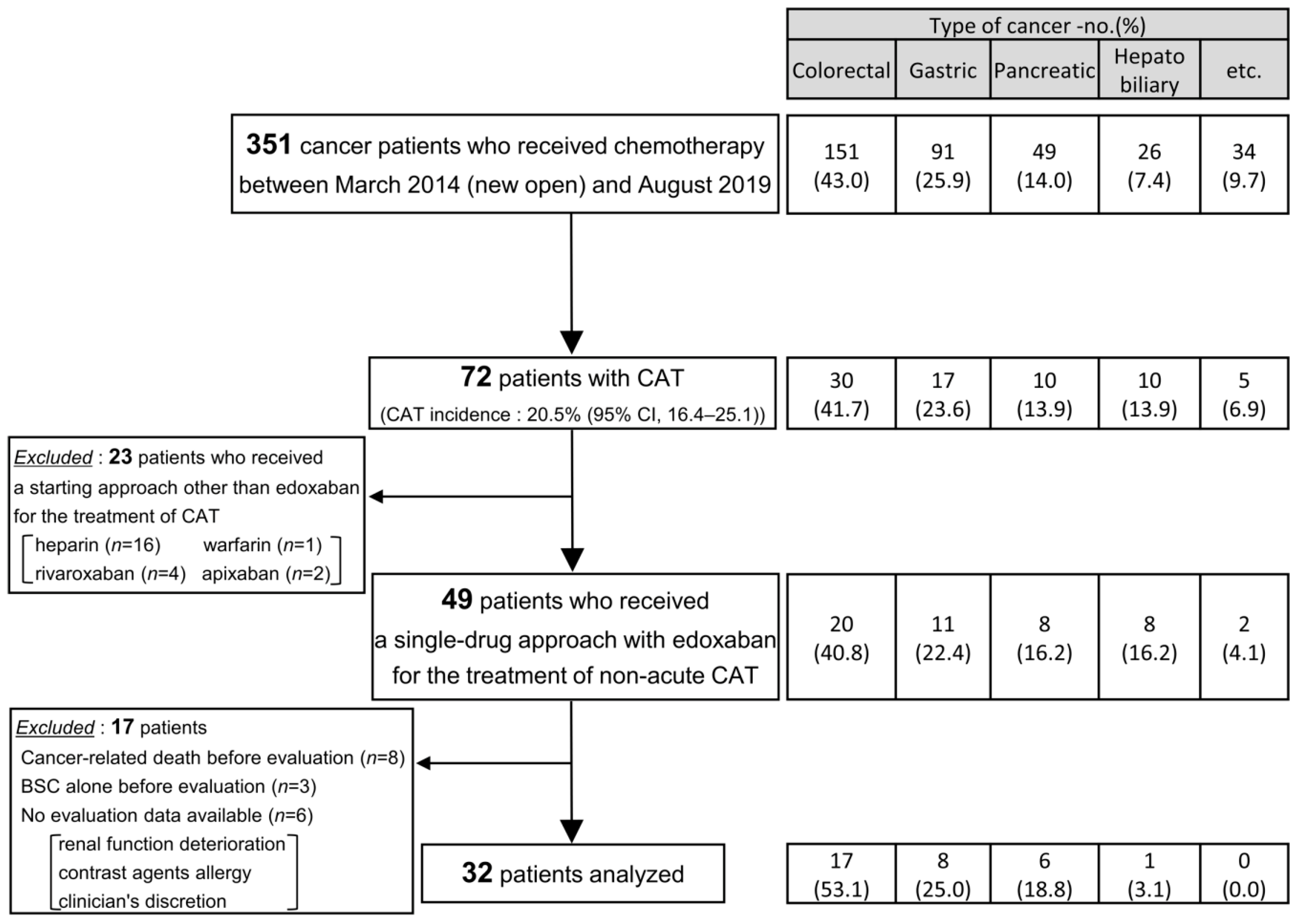
2.2. Patients
2.3. Treatment
2.4. Evaluations
2.5. Statistical Analysis
3. Results
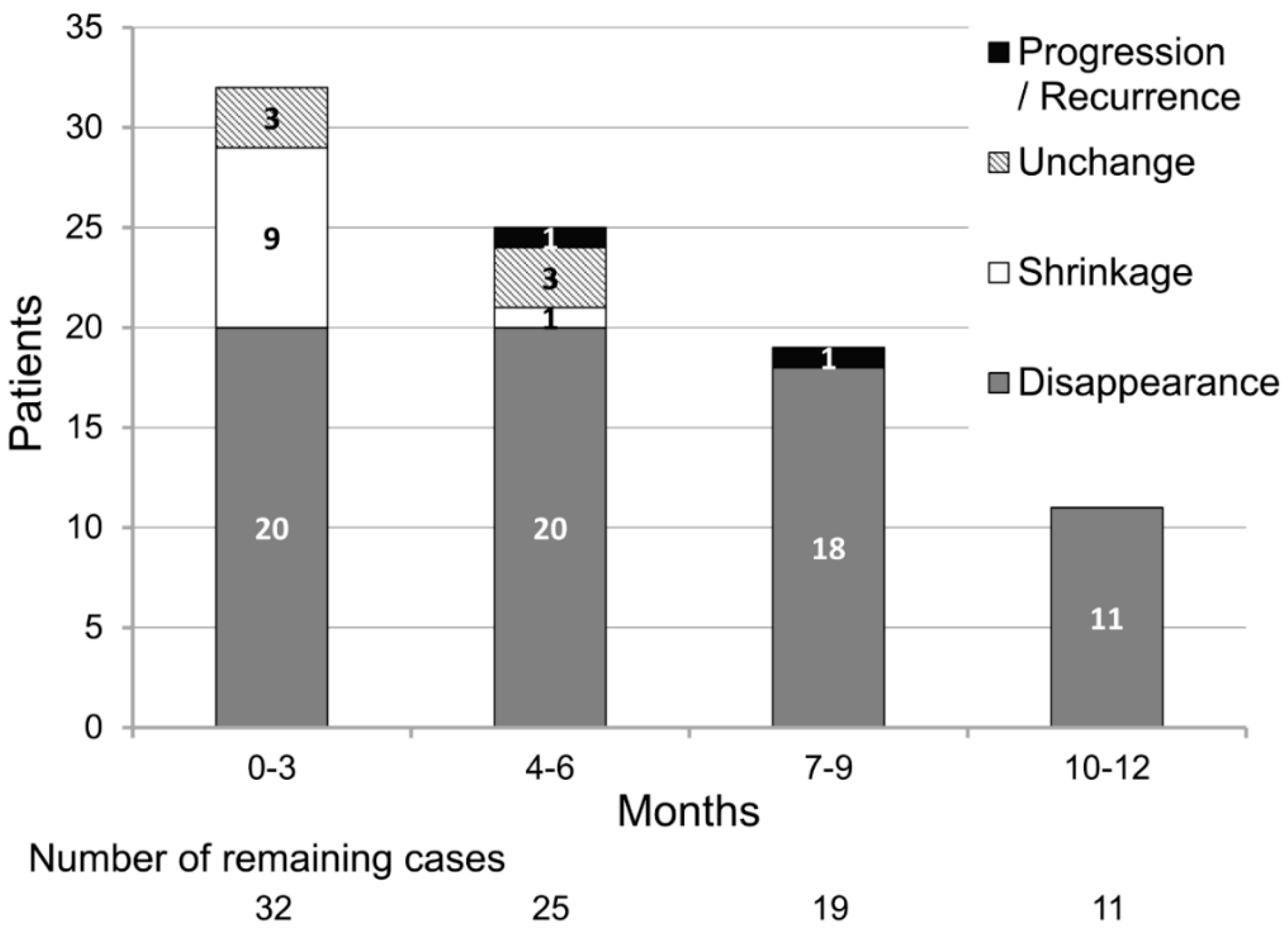
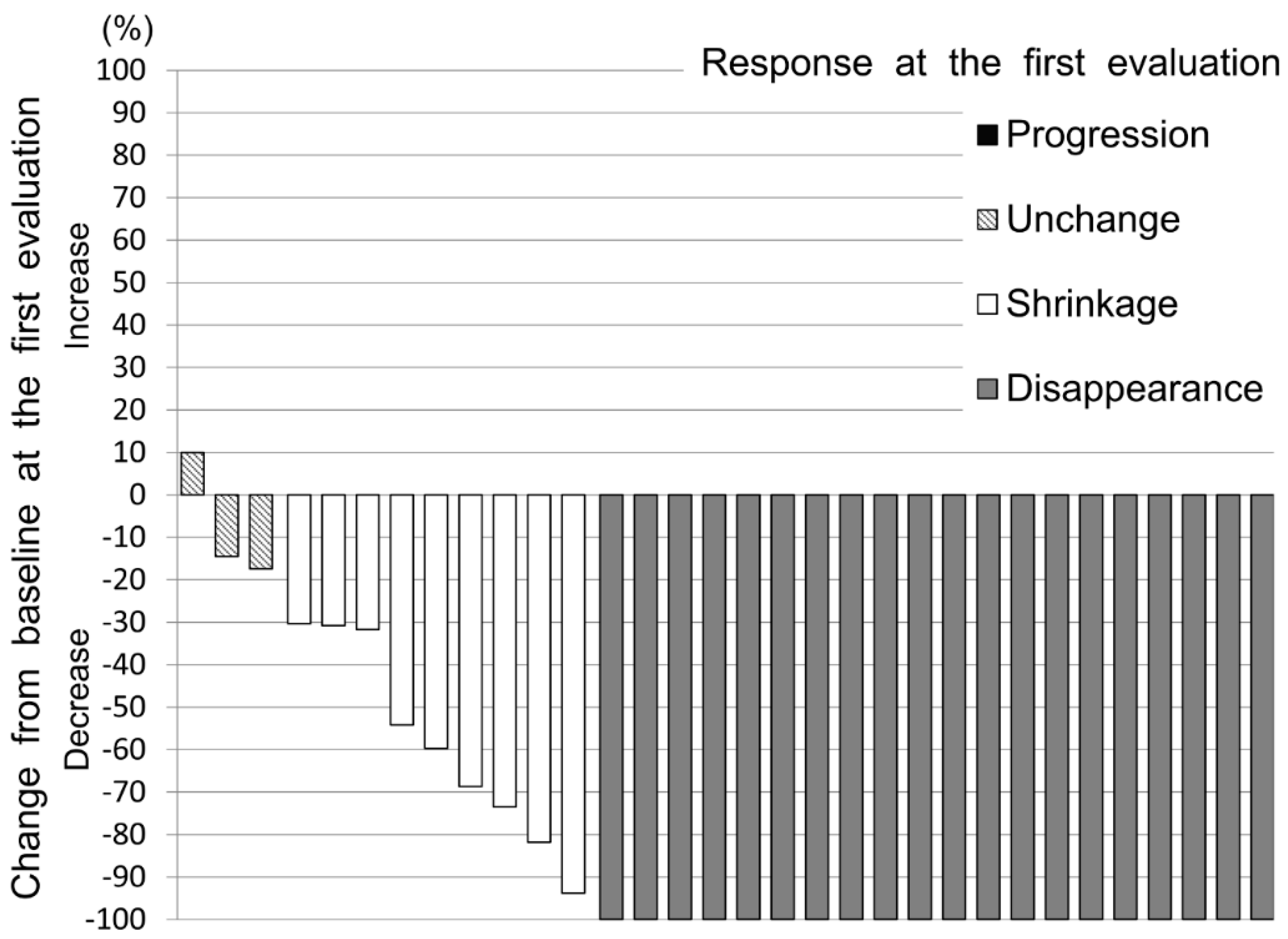
3.1. Primary Endpoint
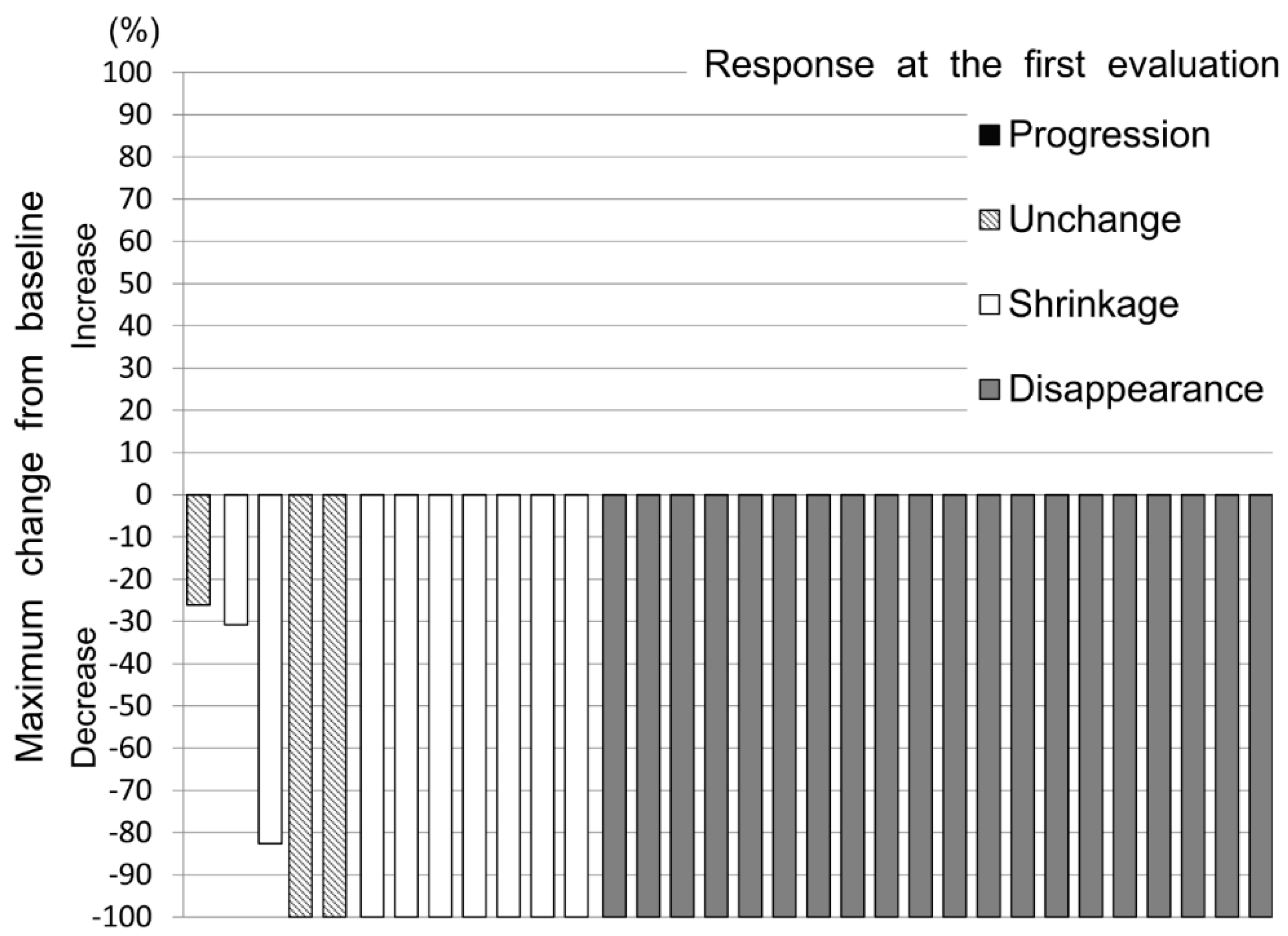
3.2. Secondary Endpoints
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Nakamura, M.; Miyata, T.; Ozeki, Y.; Takayama, M.; Komori, K.; Yamada, N.; Origasa, H.; Satokawa, H.; Maeda, H.; Tanabe, N.; et al. Current venous thromboembolism management and outcomes in Japan. Circ. J. 2014, 78, 708–717. [Google Scholar] [CrossRef] [Green Version]
- Walker, A.J.; Card, T.; West, J.; Crooks, C.J.; Grainge, M. Incidence of venous thromboembolism in patients with cancer—A cohort study using linked United Kingdom databases. Eur. J. Cancer 2013, 49, 1404–1413. [Google Scholar] [CrossRef] [PubMed]
- Perre, A.; Markman, M. Extended venous thromboembolism prophylaxis for high-risk patients undergoing surgery for malignancy. Case Rep. Oncol. 2011, 4, 115–117. [Google Scholar] [CrossRef] [PubMed]
- Blom, J.W.; Doggen, C.J.; Osanto, S.; Rosendaal, F.R. Malignancies, prothrombotic mutations, and the risk of venous thrombosis. JAMA 2005, 293, 715–722. [Google Scholar] [CrossRef] [PubMed]
- Cronin-Fenton, D.P.; Søndergaard, F.; A Pedersen, L.; Fryzek, J.P.; Cetin, K.; Acquavella, J.; Baron, J.A.; Soerensen, H.T. Hospitalisation for venous thromboembolism in cancer patients and the general population: A population-based cohort study in Denmark, 1997–2006. Br. J. Cancer 2010, 103, 947–953. [Google Scholar] [CrossRef] [Green Version]
- Trinh, V.Q.; Karakiewicz, P.I.; Sammon, J.; Sun, M.; Sukumar, S.; Gervais, M.K.; Shariat, S.F.; Tian, Z.; Kim, S.P.; Kowalczyk, K.J.; et al. Venous thromboembolism after major cancer surgery: Temporal trends and patterns of care. JAMA Surg. 2014, 149, 43–49. [Google Scholar] [CrossRef] [Green Version]
- Khorana, A.A.; Kuderer, N.M.; Culakova, E.; Lyman, G.H.; Francis, C.W. Development, and validation of a predictive model for chemotherapy-associated thrombosis. Blood 2008, 111, 4902–4907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ay, C.; Pabinger, I. VTE risk assessment in cancer. Who needs prophylaxis and who does not? Hamostaseologie 2015, 35, 319–324. [Google Scholar]
- Khorana, A.A.; Francis, C.W.; Culakova, E.; Kuderer, N.M.; Lyman, G.H. Thromboembolism is a leading cause of death in cancer patients receiving outpatient chemotherapy. J. Thromb. Haemost. 2007, 5, 632–634. [Google Scholar] [CrossRef]
- Kearon, C.; Akl, E.A.; Ornelas, J.; Blaivas, A.; Jimenez, D.; Bounameaux, H.; Huisman, M.; King, C.S.; Morris, T.A.; Sood, N.; et al. Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. Chest 2016, 149, 315–352. [Google Scholar] [CrossRef]
- Raskob, G.E.; van Es, N.; Verhamme, P.; Carrier, M.; di Nisio, M.; Garcia, D.; Grosso, M.A.; Kakkar, A.K.; Kovacs, M.J.; Mercuri, M.F.; et al. Edoxaban for the Treatment of Cancer-Associated Venous Thromboembolism. New Engl. J. Med. 2018, 378, 615–624. [Google Scholar] [CrossRef] [PubMed]
- Key, N.S.; Khorana, A.A.; Kuderer, N.M.; Bohlke, K.; Lee, A.Y.Y.; Arcelus, J.I.; Wong, S.L.; Balaban, E.P.; Flowers, C.R.; Francis, C.W.; et al. Venous Thromboembolism Prophylaxis and Treatment in Patients With Cancer: ASCO Clinical Practice Guideline Update. J. Clin. Oncol. 2020, 38, 496–520. [Google Scholar] [CrossRef] [PubMed]
- Pabinger-Fasching, I.; Ay, C. Biomarkers and Venous Thromboembolism. Arter. Thromb. Vasc. Boil. 2009, 29, 332–336. [Google Scholar] [CrossRef] [PubMed]
- Ay, C.; Dunkler, D.; Marosi, C.; Chiriac, A.-L.; Vormittag, R.; Simanek, R.; Quehenberger, P.; Zielinski, C.; Pabinger, I. Prediction of venous thromboembolism in cancer patients. Blood 2010, 116, 5377–5382. [Google Scholar] [CrossRef] [PubMed]
- Reitter, E.-M.; Kaider, A.; Ay, C.; Quehenberger, P.; Marosi, C.; Zielinski, C.; Pabinger-Fasching, I. Longitudinal analysis of hemostasis biomarkers in cancer patients during antitumor treatment. J. Thromb. Haemost. 2016, 14, 294–305. [Google Scholar] [CrossRef] [PubMed]
- Riondino, S.; Ferroni, P.; Zanzotto, F.M.; Roselli, M.; Guadagni, F. Predicting VTE in Cancer Patients: Candidate Biomarkers and Risk Assessment Models. Cancers 2019, 11, 95. [Google Scholar] [CrossRef] [Green Version]
- Pabinger, I.; van Es, N.; Heinze, G.; Posch, F.; Riedl, J.; Reitter, E.M.; di Nisio, M.; Cesarman-Maus, G.; Kraaijpoel, N.; Zielinski, C.C.; et al. A clinical prediction model for cancer-associated venous thromboembolism: A development and validation study in two independent prospective cohorts. Lancet Haematol. 2018, 5, e289–e298. [Google Scholar] [CrossRef]
- Farge, D.; Frere, C.; Connors, J.M.; Ay, C.; Khorana, A.A.; Munoz, A.; Brenner, B.; Kakkar, A.; Rafii, H.; Solymoss, S.; et al. 2019 international clinical practice guidelines for the treatment and prophylaxis of venous thromboembolism in patients with cancer. Lancet Oncol. 2019, 20, e566–e581. [Google Scholar] [CrossRef] [Green Version]
- Vedantham, S.; Thorpe, P.E.; Cardella, J.F.; Grassi, C.J.; Patel, N.H.; Ferral, H.; Hofmann, L.V.; Janne d’Othee, B.M.; Antonaci, V.P.; Brountzos, E.N.; et al. Quality improvement guidelines for the treatment of lower extremity deep vein thrombosis with use of endovascular thrombus removal. J. Vasc. Interv. Radiol. 2006, 17, 435–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Schulman, S.; Kearon, C. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J. Thromb. Haemost. 2005, 3, 692–694. [Google Scholar] [CrossRef] [PubMed]
- Yamada, N.; Hirayama, A.; Maeda, H.; Sakagami, S.; Shikata, H.; Prins, M.H.; Lensing, A.W.; Kato, M.; Onuma, J.; Miyamoto, Y.; et al. Oral rivaroxaban for Japanese patients with symptomatic venous thromboembolism—The J-EINSTEIN DVT and PE program. Thromb. J. 2015, 13, 2. [Google Scholar] [CrossRef] [Green Version]
- Young, A.M.; Marshall, A.; Thirlwall, J.; Chapman, O.; Lokare, A.; Hill, C.; Hale, D.; Dunn, J.A.; Lyman, G.H.; Hutchinson, C.; et al. Comparison of an Oral Factor Xa Inhibitor With Low Molecular Weight Heparin in Patients With Cancer With Venous Thromboembolism: Results of a Randomized Trial (SELECT-D). J. Clin. Oncol. 2018, 36, 2017–2023. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Antona, C.; Sayi, J.G.; Gustafsson, L.L.; Bertilsson, L.; Ingelman-Sundberg, M. Phenotype–genotype variability in the human CYP3A locus as assessed by the probe drug quinine and analyses of variant CYP3A4 alleles. Biochem. Biophys. Res. Commun. 2005, 338, 299–305. [Google Scholar] [CrossRef]
- Burnett, A.E.; Mahan, C.E.; Vazquez, S.R.; Oertel, L.B.; Garcia, D.A.; Ansell, J. Guidance for the practical management of the direct oral anticoagulants (DOACs) in VTE treatment. J. Thromb. Thrombolysis 2016, 41, 206–232. [Google Scholar] [CrossRef] [Green Version]
- Rodger, M.A.; Kahn, S.R.; Wells, P.S.; Anderson, D.A.; Chagnon, I.; le Gal, G.; Solymoss, S.; Crowther, M.; Perrier, A.; White, R.; et al. Identifying unprovoked thromboembolism patients at low risk for recurrence who can discontinue anticoagulant therapy. CMAJ 2008, 179, 417–426. [Google Scholar] [CrossRef] [Green Version]
- Kearon, C.; Spencer, F.A.; O’Keeffe, D.; Parpia, S.; Schulman, S.; Baglin, T.; Stevens, S.M.; Kaatz, S.; Bauer, K.A.; Douketis, J.D.; et al. D-dimer testing to select patients with a first unprovoked venous thromboembolism who can stop anticoagulant therapy: A cohort study. Ann. Intern. Med. 2015, 162, 27–34. [Google Scholar] [CrossRef]
- Palareti, G.; Cosmi, B.; Legnani, C.; Tosetto, A.; Brusi, C.; Iorio, A.; Pengo, V.; Ghirarduzzi, A.; Pattacini, C.; Testa, S.; et al. D-dimer testing to determine the duration of anticoagulation therapy. N. Engl. J. Med. 2006, 355, 1780–1789. [Google Scholar] [CrossRef]
- Douketis, J.; Tosetto, A.; Marcucci, M.; Baglin, T.; Cushman, M.; Eichinger, S.; Palareti, G.; Poli, D.; Tait, C.; Iorio, A. Patient-Level Meta-analysis: Effect of Measurement Timing, Threshold, and Patient Age on Ability ofd-Dimer Testing to Assess Recurrence Risk After Unprovoked Venous Thromboembolism. Ann. Intern. Med. 2010, 153, 523–531. [Google Scholar] [CrossRef] [PubMed]
- Cosmi, B.; Legnani, C.; Tosetto, A.; Pengo, V.; Ghirarduzzi, A.; Testa, S.; Prisco, D.; Poli, D.; Tripodi, A.; Palareti, G.; et al. Sex, age and normal post-anticoagulation D-dimer as risk factors for recurrence after idiopathic venous thromboembolism in the Prolong study extension. J. Thromb. Haemost. 2010, 8, 1933–1942. [Google Scholar] [CrossRef] [PubMed]
- Carrier, M.; le Gal, G.; Wells, P.S.; Fergusson, D.A.; Ramsay, T.; Rodger, M. Systematic review: The Trousseau syndrome revisited: Should we screen extensively for cancer in patients with venous thromboembolism? Ann. Intern. Med. 2008, 149, 323–333. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Patients (n = 32) |
|---|---|
| Age—year (IQR) | 68 (60.75–75.25) |
| Sex—no. (%) | |
| Male | 14 (43.8) |
| Female | 18 (56.3) |
| Body surface area—m2 (IQR) | 1.52 (1.38–1.60) |
| Body weight—kg (IQR) | 50.55 (45.28–57.05) |
| ≤60 kg—no. (%) | 25 (78.1) |
| >60 kg—no. (%) | 7 (21.9) |
| Creatinine Clearance (Cockcroft-Gault Equation)—mL/min (IQR) | 66.71 (54.10–85.84) |
| ≤50 mL/min—no. (%) | 7 (21.9) |
| >50 mL/min—no. (%) | 25 (78.1) |
| The dose of edoxaban—no. (%) | |
| 30 mg | 25 (78.1) |
| 60 mg | 7 (21.9) |
| Type of thrombosis—no. (%) | |
| Pulmonary embolism | 8 (25.0) |
| Proximal deep-venous thrombosis | 9 (28.1) |
| Distal deep-venous thrombosis | 21 (65.6) |
| Symptomatic venous thromboembolism | 4 (12.5) |
| Type of diagnosis—no. (%) | |
| Symptomatic CAT diagnosed more than 14 days after onset | 4 (12.5) |
| Asymptomatic CAT diagnosed by the D-dimer/CT approach | 28 (87.5) |
| Chemotherapy target—no. (%) | |
| Primary advanced | 22 (68.8) |
| Recurrence | 7 (21.9) |
| Adjuvant | 3 (9.4) |
| The number of chemotherapy lines—no. (%) | |
| 0 | 3 (9.4) |
| 1 | 23 (71.9) |
| 2 | 5 (15.6) |
| 3 | 0 (0.0) |
| 4 or more | 1 (3.1) |
| ECOG performance status—no. (%) | |
| 0 | 18 (56.3) |
| 1 | 12 (37.5) |
| 2 | 2 (6.3) |
| 3 | 0 (0.0) |
| 4 | 0 (0.0) |
| Administration history of VEGF inhibitors—no. (%) | 9 (28.1) |
| Onset during the administration of VEGF inhibitors—no. (%) | 8 (25.0) |
| Follow-up period—day (IQR) | 335.5 (245–390) |
| Endpoints | Patients (n = 32) |
|---|---|
| Primary endpoint | |
| Thrombus disappearance at the first evaluation—no. (%; 95% CI) | 20 (62.5; 43.7–78.9) |
| Secondary endpoints | |
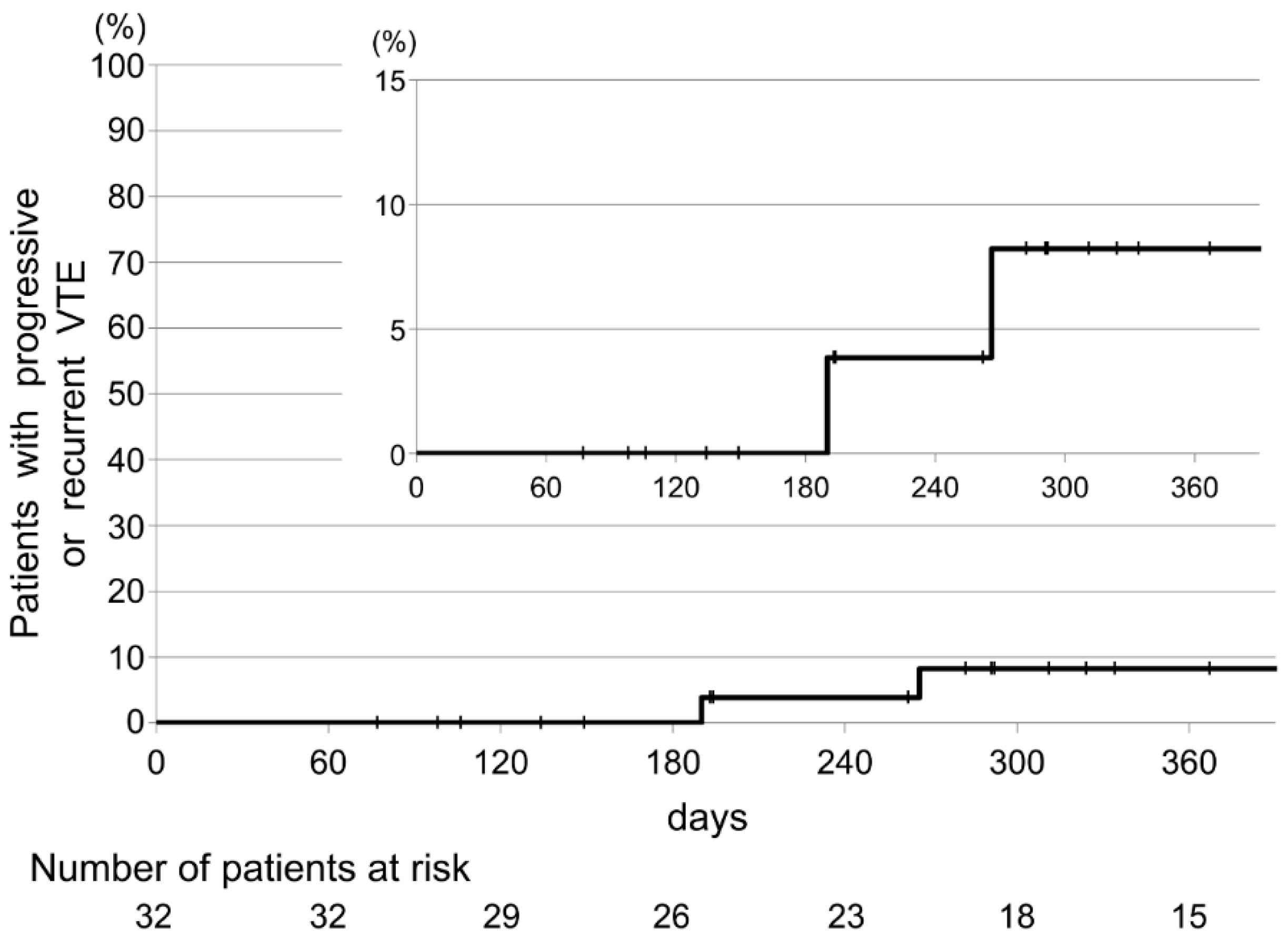
| Recurrent venous thromboembolism—no. (%; 95% CI) | 2 (6.25; 0.8–20.8) |
| Recurrent pulmonary embolism—no. (%; 95% CI) | 1 (3.13; 0.1–16.2) |
| Recurrent deep-vein thrombosis—no. (%; 95% CI) | 2 (6.25; 0.8–20.8) |
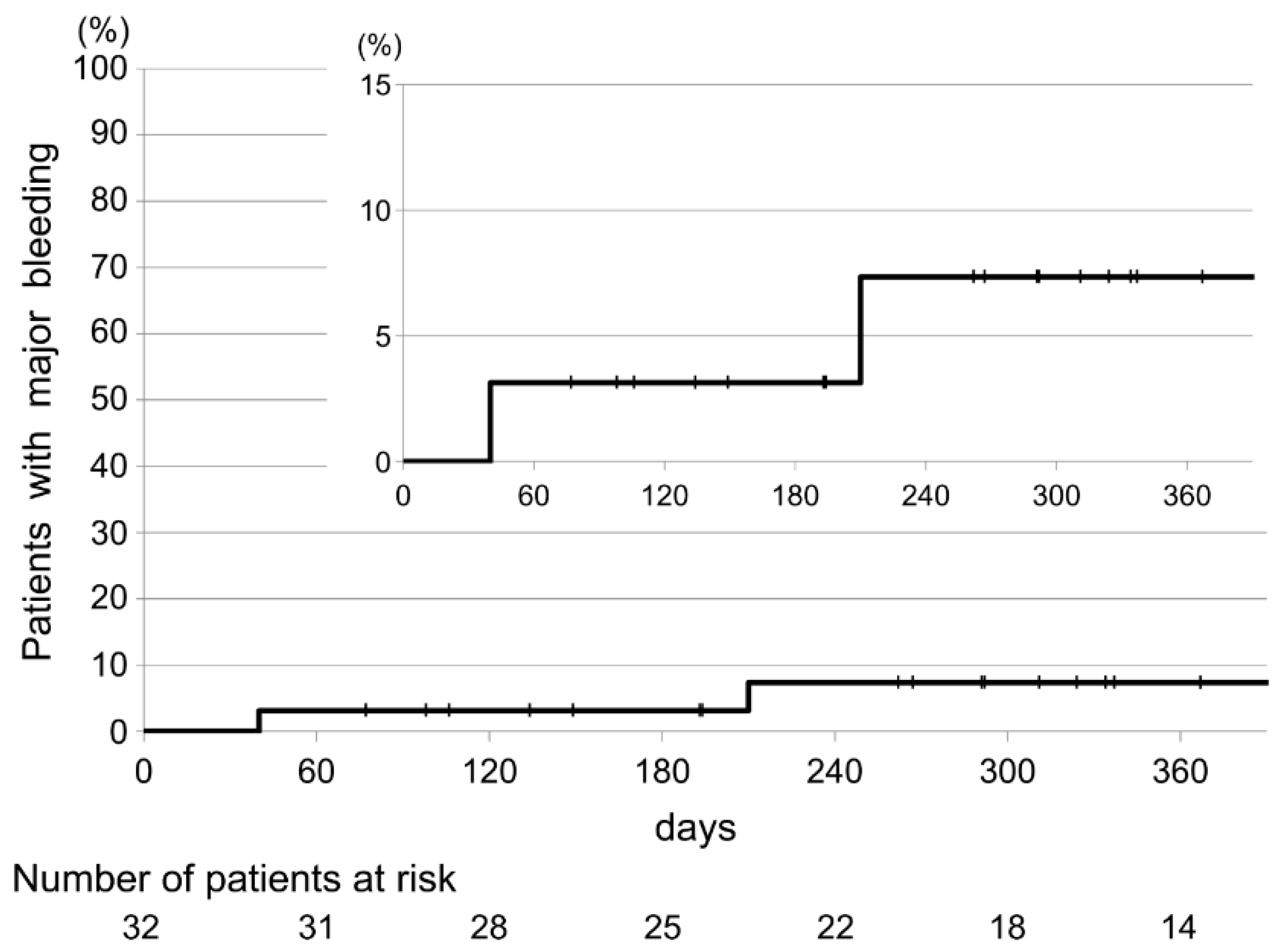
| Major bleeding—no. (%; 95% CI) | 2 (6.25; 0.8–20.8) |
| Fatal bleeding—no. (%; 95% CI) | 0 (0.00; 0.0–8.9) |
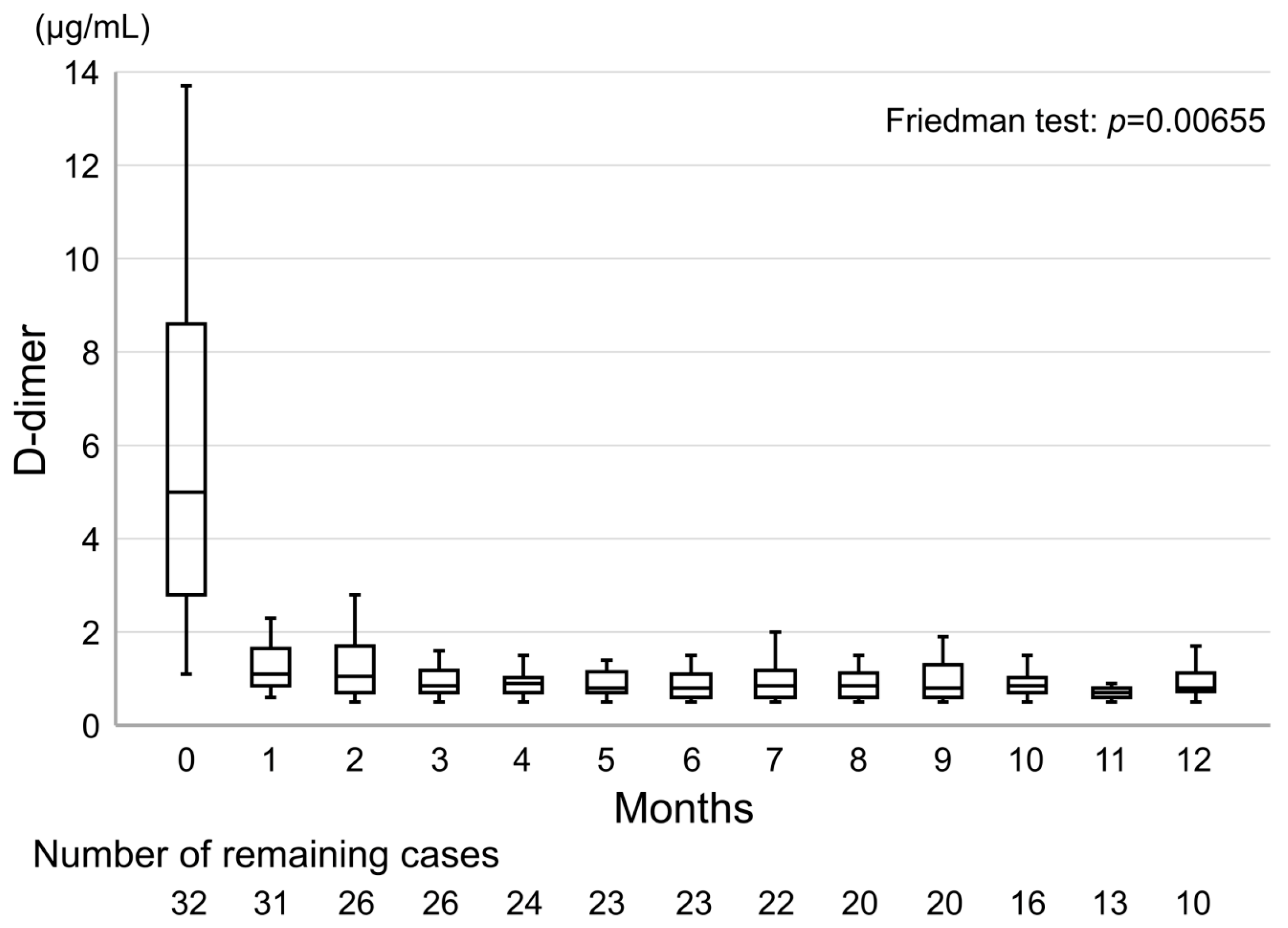
| Median D-dimer levels at diagnosis—μg/mL (IQR) | 5.0 (2.80–8.60) |
| Median D-dimer levels after 1 month—μg/mL (IQR) | 1.1 (0.85–1.65) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toshima, H.; Hisamatsu, A.; Kobayashi, K.; Ishida, H.; Shimada, K. Single-Drug Approach with Edoxaban is Effective for Resolving Non-Acute Cancer-Associated Venous Thrombosis: A Single-Arm Retrospective Analysis. Cancers 2020, 12, 1711. https://doi.org/10.3390/cancers12071711
Toshima H, Hisamatsu A, Kobayashi K, Ishida H, Shimada K. Single-Drug Approach with Edoxaban is Effective for Resolving Non-Acute Cancer-Associated Venous Thrombosis: A Single-Arm Retrospective Analysis. Cancers. 2020; 12(7):1711. https://doi.org/10.3390/cancers12071711
Chicago/Turabian StyleToshima, Hirokazu, Atsushi Hisamatsu, Kouji Kobayashi, Hiroo Ishida, and Ken Shimada. 2020. "Single-Drug Approach with Edoxaban is Effective for Resolving Non-Acute Cancer-Associated Venous Thrombosis: A Single-Arm Retrospective Analysis" Cancers 12, no. 7: 1711. https://doi.org/10.3390/cancers12071711
APA StyleToshima, H., Hisamatsu, A., Kobayashi, K., Ishida, H., & Shimada, K. (2020). Single-Drug Approach with Edoxaban is Effective for Resolving Non-Acute Cancer-Associated Venous Thrombosis: A Single-Arm Retrospective Analysis. Cancers, 12(7), 1711. https://doi.org/10.3390/cancers12071711