Hypopigmented Mycosis Fungoides: Loss of Pigmentation Reflects Antitumor Immune Response in Young Patients

 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Characteristics of Hypopigmented Mycosis Fungoides
3. Immunopathogenesis of Alibert-Bazin and Hypopigmented Mycosis Fungoides
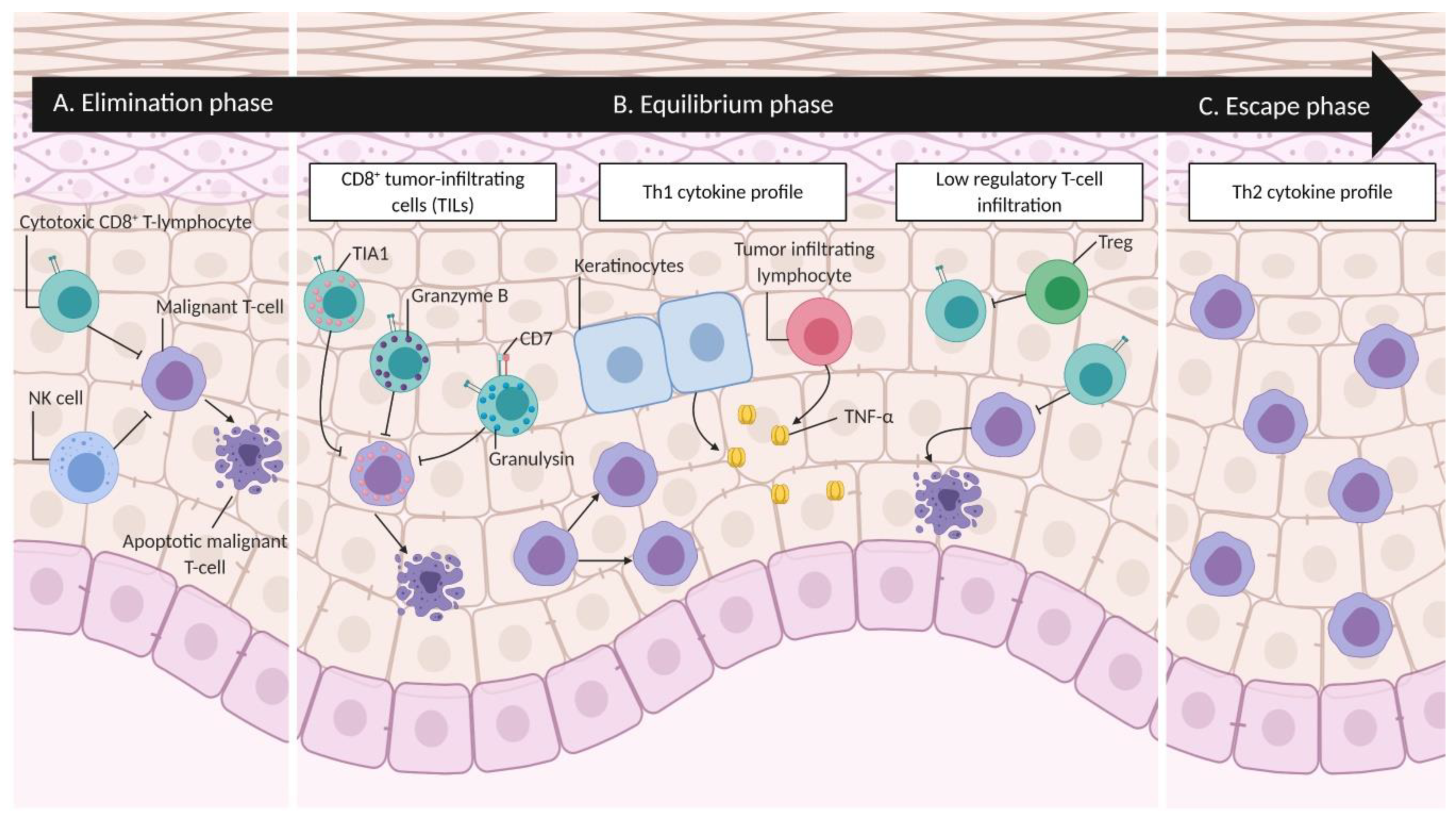
4. Cancer Immunoediting in Mycosis Fungoides
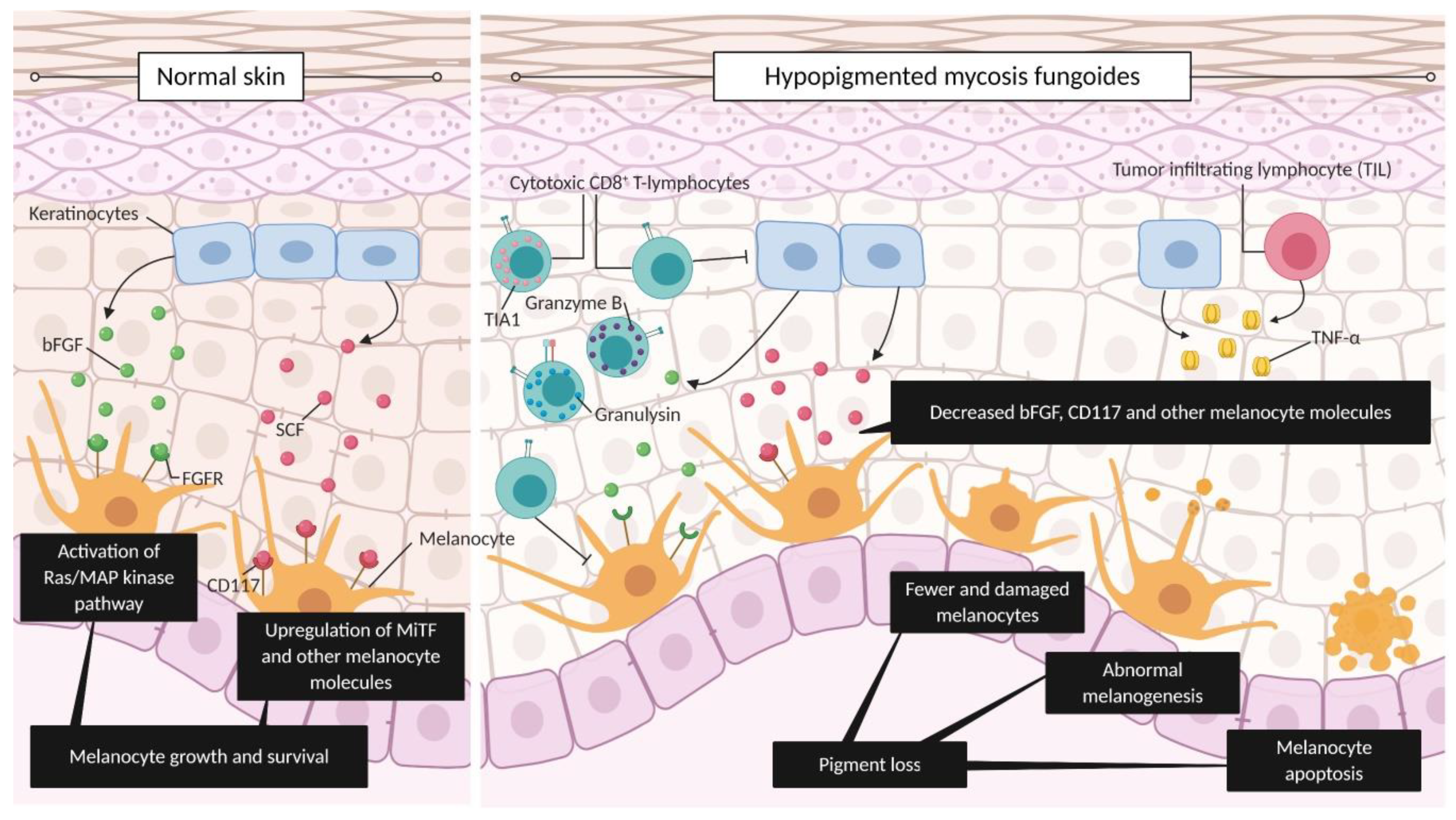
5. Hypopigmentation as a Surrogate Marker of Antitumor Immune Response in MF
6. Clinical/Demographic Patient Characteristics as a Result of Antitumor Immune Response
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Pulitzer, M. Cutaneous T-cell Lymphoma. Clin. Lab. Med. 2017, 37, 527–546. [Google Scholar] [CrossRef] [PubMed]
- Bagherani, N.; Smoller, B.R. An overview of cutaneous T cell lymphomas. F1000Res. 2016, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghazawi, F.M.; Alghazawi, N.; Le, M.; Netchiporouk, E.; Glassman, S.J.; Sasseville, D.; Litvinov, I.V. Environmental and Other Extrinsic Risk Factors Contributing to the Pathogenesis of Cutaneous T Cell Lymphoma (CTCL). Front. Oncol. 2019, 9, 300. [Google Scholar] [CrossRef] [PubMed]
- Querfeld, C.; Zain, J.; Rosen, S.T. Primary Cutaneous T-Cell Lymphomas: Mycosis Fungoides and Sezary Syndrome. Cancer Treat. Res. 2019, 176, 225–248. [Google Scholar] [CrossRef] [PubMed]
- Litvinov, I.V.; Tetzlaff, M.T.; Rahme, E.; Habel, Y.; Risser, D.R.; Gangar, P.; Jennings, M.A.; Pehr, K.; Prieto, V.G.; Sasseville, D.; et al. Identification of geographic clustering and regions spared by cutaneous T-cell lymphoma in Texas using 2 distinct cancer registries. Cancer 2015, 121, 1993–2003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howard, M.S.; Smoller, B.R. Mycosis fungoides: Classic disease and variant presentations. Semin. Cutan. Med. Surg. 2000, 19, 91–99. [Google Scholar] [CrossRef]
- Jawed, S.I.; Myskowski, P.L.; Horwitz, S.; Moskowitz, A.; Querfeld, C. Primary cutaneous T-cell lymphoma (mycosis fungoides and Sezary syndrome): Part I. Diagnosis: Clinical and histopathologic features and new molecular and biologic markers. J. Am. Acad. Derm. 2014, 70, 205.e1–205.e16. [Google Scholar] [CrossRef]
- Furlan, F.C.; Sanches, J.A. Hypopigmented mycosis fungoides: A review of its clinical features and pathophysiology. Bras. Derm. 2013, 88, 954–960. [Google Scholar] [CrossRef] [Green Version]
- Rodney, I.J.; Kindred, C.; Angra, K.; Qutub, O.N.; Villanueva, A.R.; Halder, R.M. Hypopigmented mycosis fungoides: A retrospective clinicohistopathologic study. J. Eur. Acad. Derm. Venereol. 2017, 31, 808–814. [Google Scholar] [CrossRef]
- Castano, E.; Glick, S.; Wolgast, L.; Naeem, R.; Sunkara, J.; Elston, D.; Jacobson, M. Hypopigmented mycosis fungoides in childhood and adolescence: A long-term retrospective study. J. Cutan. Pathol. 2013, 40, 924–934. [Google Scholar] [CrossRef]
- Rowe, B.; Shevchenko, A.; Yosipovitch, G. Leser-Trelat Sign in Tumor-Stage Mycosis Fungoides. Dermatol. Online J. 2016, 22. [Google Scholar]
- Furlan, F.C.; de Paula Pereira, B.A.; da Silva, L.F.; Sanches, J.A. Loss of melanocytes in hypopigmented mycosis fungoides: A study of 18 patients. J. Cutan. Pathol. 2014, 41, 101–107. [Google Scholar] [CrossRef] [PubMed]
- El-Darouti, M.A.; Marzouk, S.A.; Azzam, O.; Fawzi, M.M.; Abdel-Halim, M.R.; Zayed, A.A.; Leheta, T.M. Vitiligo vs. hypopigmented mycosis fungoides (histopathological and immunohistochemical study, univariate analysis). Eur. J. Derm. 2006, 16, 17–22. [Google Scholar]
- Hodak, E.; Phenig, E.; Amichai, B.; Feinmesser, M.; Kuten, A.; Maron, L.; Sahar, D.; Bergman, R.; David, M. Unilesional mycosis fungoides: A study of seven cases. Dermatology 2000, 201, 300–306. [Google Scholar] [CrossRef]
- Amorim, G.M.; Niemeyer-Corbellini, J.P.; Quintella, D.C.; Cuzzi, T.; Ramos, E.S.M. Hypopigmented mycosis fungoides: A 20-case retrospective series. Int. J. Derm. 2018, 57, 306–312. [Google Scholar] [CrossRef]
- Ardigo, M.; Borroni, G.; Muscardin, L.; Kerl, H.; Cerroni, L. Hypopigmented mycosis fungoides in Caucasian patients: A clinicopathologic study of 7 cases. J. Am. Acad. Derm. 2003, 49, 264–270. [Google Scholar] [CrossRef]
- Whittam, L.R.; Calonje, E.; Orchard, G.; Fraser-Andrews, E.A.; Woolford, A.; Russell-Jones, R. CD8-positive juvenile onset mycosis fungoides: An immunohistochemical and genotypic analysis of six cases. Br. J. Derm. 2000, 143, 1199–1204. [Google Scholar] [CrossRef]
- El-Shabrawi-Caelen, L.; Cerroni, L.; Medeiros, L.J.; McCalmont, T.H. Hypopigmented mycosis fungoides: Frequent expression of a CD8+ T-cell phenotype. Am. J. Surg. Pathol. 2002, 26, 450–457. [Google Scholar] [CrossRef]
- Ngo, J.T.; Trotter, M.J.; Haber, R.M. Juvenile-onset hypopigmented mycosis fungoides mimicking vitiligo. J. Cutan. Med. Surg. 2009, 13, 230–233. [Google Scholar] [CrossRef]
- Litvinov, I.V.; Shtreis, A.; Kobayashi, K.; Glassman, S.; Tsang, M.; Woetmann, A.; Sasseville, D.; Odum, N.; Duvic, M. Investigating potential exogenous tumor initiating and promoting factors for Cutaneous T-Cell Lymphomas (CTCL), a rare skin malignancy. Oncoimmunology 2016, 5, e1175799. [Google Scholar] [CrossRef] [Green Version]
- Gallardo, F.; Sandoval, J.; Diaz-Lagares, A.; Garcia, R.; D’Altri, T.; Gonzalez, J.; Alegre, V.; Servitje, O.; Crujeiras, A.B.; Stefansson, O.A.; et al. Notch1 Pathway Activation Results from the Epigenetic Abrogation of Notch-Related MicroRNAs in Mycosis Fungoides. J. Invest. Derm. 2015, 135, 3144–3152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lundin Brockdorff, J.; Woetmann, A.; Mustelin, T.; Kaltoft, K.; Zhang, Q.; Wasik, M.A.; Ropke, C.; Odum, N. SHP2 regulates IL-2 induced MAPK activation, but not Stat3 or Stat5 tyrosine phosphorylation, in cutaneous T cell lymphoma cells. Cytokine 2002, 20, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Ghazawi, F.M.; Netchiporouk, E.; Rahme, E.; Tsang, M.; Moreau, L.; Glassman, S.; Provost, N.; Gilbert, M.; Jean, S.E.; Pehr, K.; et al. Comprehensive analysis of cutaneous T-cell lymphoma (CTCL) incidence and mortality in Canada reveals changing trends and geographic clustering for this malignancy. Cancer 2017, 123, 3550–3567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghazawi, F.M.; Netchiporouk, E.; Rahme, E.; Tsang, M.; Moreau, L.; Glassman, S.; Provost, N.; Gilbert, M.; Jean, S.E.; Roshdy, O.; et al. Distribution and Clustering of Cutaneous T-Cell Lymphoma (CTCL) Cases in Canada During 1992 to 2010. J. Cutan. Med. Surg. 2018, 22, 154–165. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.J.; Hess, S.; Richardson, S.K.; Newton, S.; Showe, L.C.; Benoit, B.M.; Ubriani, R.; Vittorio, C.C.; Junkins-Hopkins, J.M.; Wysocka, M.; et al. Immunopathogenesis and therapy of cutaneous T cell lymphoma. J. Clin. Investig. 2005, 115, 798–812. [Google Scholar] [CrossRef] [Green Version]
- Kupper, T.S.; Fuhlbrigge, R.C. Immune surveillance in the skin: Mechanisms and clinical consequences. Nat. Rev. Immunol. 2004, 4, 211–222. [Google Scholar] [CrossRef]
- Girardi, M.; Heald, P.W.; Wilson, L.D. The pathogenesis of mycosis fungoides. N. Engl. J. Med. 2004, 350, 1978–1988. [Google Scholar] [CrossRef] [PubMed]
- Krejsgaard, T.; Lindahl, L.M.; Mongan, N.P.; Wasik, M.A.; Litvinov, I.V.; Iversen, L.; Langhoff, E.; Woetmann, A.; Odum, N. Malignant inflammation in cutaneous T-cell lymphoma-a hostile takeover. Semin. Immunopathol. 2017, 39, 269–282. [Google Scholar] [CrossRef]
- Krejsgaard, T.; Willerslev-Olsen, A.; Lindahl, L.M.; Bonefeld, C.M.; Koralov, S.B.; Geisler, C.; Wasik, M.A.; Gniadecki, R.; Kilian, M.; Iversen, L.; et al. Staphylococcal enterotoxins stimulate lymphoma-associated immune dysregulation. Blood 2014, 124, 761–770. [Google Scholar] [CrossRef] [PubMed]
- Sommer, V.H.; Clemmensen, O.J.; Nielsen, O.; Wasik, M.; Lovato, P.; Brender, C.; Eriksen, K.W.; Woetmann, A.; Kaestel, C.G.; Nissen, M.H.; et al. In vivo activation of STAT3 in cutaneous T-cell lymphoma. Evidence for an antiapoptotic function of STAT3. Leukemia 2004, 18, 1288–1295. [Google Scholar] [CrossRef] [Green Version]
- Litvinov, I.V.; Cordeiro, B.; Fredholm, S.; Odum, N.; Zargham, H.; Huang, Y.; Zhou, Y.; Pehr, K.; Kupper, T.S.; Woetmann, A.; et al. Analysis of STAT4 expression in cutaneous T-cell lymphoma (CTCL) patients and patient-derived cell lines. Cell Cycle 2014, 13, 2975–2982. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Netchiporouk, E.; Litvinov, I.V.; Moreau, L.; Gilbert, M.; Sasseville, D.; Duvic, M. Deregulation in STAT signaling is important for cutaneous T-cell lymphoma (CTCL) pathogenesis and cancer progression. Cell Cycle 2014, 13, 3331–3335. [Google Scholar] [CrossRef] [PubMed]
- Sibbesen, N.A.; Kopp, K.L.; Litvinov, I.V.; Jonson, L.; Willerslev-Olsen, A.; Fredholm, S.; Petersen, D.L.; Nastasi, C.; Krejsgaard, T.; Lindahl, L.M.; et al. Jak3, STAT3, and STAT5 inhibit expression of miR-22, a novel tumor suppressor microRNA, in cutaneous T-Cell lymphoma. Oncotarget 2015, 6, 20555–20569. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.; Litvinov, I.V.; Wang, Y.; Su, M.W.; Tu, P.; Jiang, X.; Kupper, T.S.; Dutz, J.P.; Sasseville, D.; Zhou, Y. Thymocyte selection-associated high mobility group box gene (TOX) is aberrantly over-expressed in mycosis fungoides and correlates with poor prognosis. Oncotarget 2014, 5, 4418–4425. [Google Scholar] [CrossRef] [PubMed]
- Dulmage, B.O.; Akilov, O.; Vu, J.R.; Falo, L.D.; Geskin, L.J. Dysregulation of the TOX-RUNX3 pathway in cutaneous T-cell lymphoma. Oncotarget 2019, 10, 3104–3113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willerslev-Olsen, A.; Litvinov, I.V.; Fredholm, S.M.; Petersen, D.L.; Sibbesen, N.A.; Gniadecki, R.; Zhang, Q.; Bonefeld, C.M.; Wasik, M.A.; Geisler, C.; et al. IL-15 and IL-17F are differentially regulated and expressed in mycosis fungoides (MF). Cell Cycle 2014, 13, 1306–1312. [Google Scholar] [CrossRef] [Green Version]
- Lindahl, L.M.; Fredholm, S.; Joseph, C.; Nielsen, B.S.; Jonson, L.; Willerslev-Olsen, A.; Gluud, M.; Blumel, E.; Petersen, D.L.; Sibbesen, N.; et al. STAT5 induces miR-21 expression in cutaneous T cell lymphoma. Oncotarget 2016, 7, 45730–45744. [Google Scholar] [CrossRef] [Green Version]
- Lefrancois, P.; Tetzlaff, M.T.; Moreau, L.; Watters, A.K.; Netchiporouk, E.; Provost, N.; Gilbert, M.; Ni, X.; Sasseville, D.; Duvic, M.; et al. TruSeq-Based Gene Expression Analysis of Formalin-Fixed Paraffin-Embedded (FFPE) Cutaneous T-Cell Lymphoma Samples: Subgroup Analysis Results and Elucidation of Biases from FFPE Sample Processing on the TruSeq Platform. Front. Med. (Lausanne) 2017, 4, 153. [Google Scholar] [CrossRef] [Green Version]
- Krejsgaard, T.; Litvinov, I.V.; Wang, Y.; Xia, L.; Willerslev-Olsen, A.; Koralov, S.B.; Kopp, K.L.; Bonefeld, C.M.; Wasik, M.A.; Geisler, C.; et al. Elucidating the role of interleukin-17F in cutaneous T-cell lymphoma. Blood 2013, 122, 943–950. [Google Scholar] [CrossRef] [Green Version]
- Le, M.; Ghazawi, F.M.; Netchiporouk, E.; Litvinov, I.V. The Novel Role of Antibiotic Treatment in the Management of Cutaneous T-Cell Lymphoma (CTCL) Patients. J. Cutan. Med. Surg. 2020. [Google Scholar] [CrossRef]
- Shalabi, D.; Bistline, A.; Alpdogan, O.; Kartan, S.; Mishra, A.; Porcu, P.; Nikbakht, N. Immune evasion and current immunotherapy strategies in mycosis fungoides (MF) and Sezary syndrome (SS). Chin. Clin. Oncol 2019, 8, 11. [Google Scholar] [CrossRef]
- Wong, H.K.; Mishra, A.; Hake, T.; Porcu, P. Evolving insights in the pathogenesis and therapy of cutaneous T-cell lymphoma (mycosis fungoides and Sezary syndrome). Br. J. Haematol. 2011, 155, 150–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunn, G.P.; Old, L.J.; Schreiber, R.D. The immunobiology of cancer immunosurveillance and immunoediting. Immunity 2004, 21, 137–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Litvinov, I.V.; Netchiporouk, E.; Cordeiro, B.; Dore, M.A.; Moreau, L.; Pehr, K.; Gilbert, M.; Zhou, Y.; Sasseville, D.; Kupper, T.S. The Use of Transcriptional Profiling to Improve Personalized Diagnosis and Management of Cutaneous T-cell Lymphoma (CTCL). Clin. Cancer Res. 2015, 21, 2820–2829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Litvinov, I.V.; Jones, D.A.; Sasseville, D.; Kupper, T.S. Transcriptional profiles predict disease outcome in patients with cutaneous T-cell lymphoma. Clin. Cancer Res. 2010, 16, 2106–2114. [Google Scholar] [CrossRef] [Green Version]
- Hoppe, R.T.; Medeiros, L.J.; Warnke, R.A.; Wood, G.S. CD8-positive tumor-infiltrating lymphocytes influence the long-term survival of patients with mycosis fungoides. J. Am. Acad. Derm. 1995, 32, 448–453. [Google Scholar] [CrossRef]
- Felgar, R.E.; Macon, W.R.; Kinney, M.C.; Roberts, S.; Pasha, T.; Salhany, K.E. TIA-1 expression in lymphoid neoplasms. Identification of subsets with cytotoxic T lymphocyte or natural killer cell differentiation. Am. J. Pathol. 1997, 150, 1893–1900. [Google Scholar]
- Hodak, E.; David, M.; Maron, L.; Aviram, A.; Kaganovsky, E.; Feinmesser, M. CD4/CD8 double-negative epidermotropic cutaneous T-cell lymphoma: An immunohistochemical variant of mycosis fungoides. J. Am. Acad. Derm. 2006, 55, 276–284. [Google Scholar] [CrossRef]
- Ito, A.; Sugita, K.; Ikeda, A.; Yamamoto, O. CD4/CD8 Double-negative Mycosis Fungoides: A Case Report and Literature Review. Yonago Acta Med. 2019, 62, 153–158. [Google Scholar] [CrossRef] [Green Version]
- Nasu-Tababuchi, M.; Fujimura, T.; Kakizaki, A.; Shido, K.; Hatchome, N.; Kusakari, Y.; Aiba, S. Hypopigmented mycosis fungoides: An immunological investigation of tumor-infiltrating T cells. Dermatol. Sin. 2016, 34, 96–98. [Google Scholar] [CrossRef] [Green Version]
- Bots, M.; Medema, J.P. Granzymes at a glance. J. Cell Sci. 2006, 119, 5011–5014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Youssef, R.; Mahgoub, D.; Zeid, O.A.; Abdel-Halim, D.M.; El-Hawary, M.; Hussein, M.F.; Morcos, M.A.; Aboelfadl, D.M.; Abdelkader, H.A.; Abdel-Galeil, Y.; et al. Hypopigmented Interface T-Cell Dyscrasia and Hypopigmented Mycosis Fungoides: A Comparative Study. Am. J. Derm. 2018, 40, 727–735. [Google Scholar] [CrossRef] [PubMed]
- Krensky, A.M.; Clayberger, C. Biology and clinical relevance of granulysin. Tissue Antigens 2009, 73, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Seif El Nasr, H.; Shaker, O.G.; Fawzi, M.M.; El-Hanafi, G. Basic fibroblast growth factor and tumour necrosis factor alpha in vitiligo and other hypopigmented disorders: Suggestive possible therapeutic targets. J. Eur. Acad. Derm. Venereol. 2013, 27, 103–108. [Google Scholar] [CrossRef]
- Chuang, G.S.; Wasserman, D.I.; Byers, H.R.; Demierre, M.F. Hypopigmented T-cell dyscrasia evolving to hypopigmented mycosis fungoides during etanercept therapy. J. Am. Acad. Derm. 2008, 59, S121–S122. [Google Scholar] [CrossRef]
- Tsang, M.; Gantchev, J.; Netchiporouk, E.; Moreau, L.; Ghazawi, F.M.; Glassman, S.; Sasseville, D.; Litvinov, I.V. A study of meiomitosis and novel pathways of genomic instability in cutaneous T-cell lymphomas (CTCL). Oncotarget 2018, 9, 37647–37661. [Google Scholar] [CrossRef]
- Litvinov, I.V.; Tetzlaff, M.T.; Thibault, P.; Gangar, P.; Moreau, L.; Watters, A.K.; Netchiporouk, E.; Pehr, K.; Prieto, V.G.; Rahme, E.; et al. Gene expression analysis in Cutaneous T-Cell Lymphomas (CTCL) highlights disease heterogeneity and potential diagnostic and prognostic indicators. Oncoimmunology 2017, 6, e1306618. [Google Scholar] [CrossRef]
- Lefrancois, P.; Xie, P.; Wang, L.; Tetzlaff, M.T.; Moreau, L.; Watters, A.K.; Netchiporouk, E.; Provost, N.; Gilbert, M.; Ni, X.; et al. Gene expression profiling and immune cell-type deconvolution highlight robust disease progression and survival markers in multiple cohorts of CTCL patients. Oncoimmunology 2018, 7, e1467856. [Google Scholar] [CrossRef] [Green Version]
- Gantchev, J.; Martinez Villarreal, A.; Xie, P.; Lefrancois, P.; Gunn, S.; Netchiporouk, E.; Sasseville, D.; Litvinov, I.V. The Ectopic Expression of Meiosis Regulatory Genes in Cutaneous T-Cell Lymphomas (CTCL). Front. Oncol. 2019, 9, 429. [Google Scholar] [CrossRef]
- Gantchev, J.; Martinez Villarreal, A.; Gunn, S.; Zetka, M.; Odum, N.; Litvinov, I.V. The ectopic expression of meiCT genes promotes meiomitosis and may facilitate carcinogenesis. Cell Cycle 2020, 19, 837–854. [Google Scholar] [CrossRef]
- Litvinov, I.V.; Kupper, T.S.; Sasseville, D. The role of AHI1 and CDKN1C in cutaneous T-cell lymphoma progression. Exp. Derm. 2012, 21, 964–966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Litvinov, I.V.; Zhou, Y.; Kupper, T.S.; Sasseville, D. Loss of BCL7A expression correlates with poor disease prognosis in patients with early-stage cutaneous T-cell lymphoma. Leuk. Lymphoma 2013, 54, 653–654. [Google Scholar] [CrossRef] [PubMed]
- Lindahl, L.M.; Willerslev-Olsen, A.; Gjerdrum, L.M.R.; Nielsen, P.R.; Blumel, E.; Rittig, A.H.; Celis, P.; Herpers, B.; Becker, J.C.; Stausbol-Gron, B.; et al. Antibiotics inhibit tumor and disease activity in cutaneous T-cell lymphoma. Blood 2019, 134, 1072–1083. [Google Scholar] [CrossRef]
- Wu, C.S.; Lan, C.C.; Chiou, M.H.; Yu, H.S. Basic fibroblast growth factor promotes melanocyte migration via increased expression of p125(FAK) on melanocytes. Acta Derm. Venereol. 2006, 86, 498–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, Z.N.; Tretiakova, M.S.; Shea, C.R.; Petronic-Rosic, V.M. Decreased CD117 expression in hypopigmented mycosis fungoides correlates with hypomelanosis: Lessons learned from vitiligo. Mod. Pathol. 2006, 19, 1255–1260. [Google Scholar] [CrossRef] [Green Version]
- Wankowicz-Kalinska, A.; van den Wijngaard, R.M.; Tigges, B.J.; Westerhof, W.; Ogg, G.S.; Cerundolo, V.; Storkus, W.J.; Das, P.K. Immunopolarization of CD4+ and CD8+ T cells to Type-1-like is associated with melanocyte loss in human vitiligo. Lab. Invest. 2003, 83, 683–695. [Google Scholar] [CrossRef] [Green Version]
- Herrmann, J.L.; Syklawer, E.; Tarrillion, M.; Duvic, M.; Hughey, L.C. Concomitant mycosis fungoides and vitiligo: How mycosis fungoides may contribute to melanocyte destruction. Dermatology 2015, 230, 143–149. [Google Scholar] [CrossRef]
- Rodrigues, M. Skin Cancer Risk (Nonmelanoma Skin Cancers/Melanoma) in Vitiligo Patients. Derm. Clin. 2017, 35, 129–134. [Google Scholar] [CrossRef]
- Paulson, K.G.; Lahman, M.C.; Chapuis, A.G.; Brownell, I. Immunotherapy for skin cancer. Int. Immunol. 2019, 31, 465–475. [Google Scholar] [CrossRef] [Green Version]
- Larsabal, M.; Marti, A.; Jacquemin, C.; Rambert, J.; Thiolat, D.; Dousset, L.; Taieb, A.; Dutriaux, C.; Prey, S.; Boniface, K.; et al. Vitiligo-like lesions occurring in patients receiving anti-programmed cell death-1 therapies are clinically and biologically distinct from vitiligo. J. Am. Acad. Derm. 2017, 76, 863–870. [Google Scholar] [CrossRef]
- Hua, C.; Boussemart, L.; Mateus, C.; Routier, E.; Boutros, C.; Cazenave, H.; Viollet, R.; Thomas, M.; Roy, S.; Benannoune, N.; et al. Association of Vitiligo With Tumor Response in Patients With Metastatic Melanoma Treated With Pembrolizumab. JAMA Derm. 2016, 152, 45–51. [Google Scholar] [CrossRef] [Green Version]
- Ouwerkerk, W.; van den Berg, M.; van der Niet, S.; Limpens, J.; Luiten, R.M. Biomarkers, measured during therapy, for response of melanoma patients to immune checkpoint inhibitors: A systematic review. Melanoma Res. 2019, 29, 453–464. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.C.; Consuegra, G.; Chou, S.; Fernandez Penas, P. Vitiligo-like depigmentation in oncology patients treated with immunotherapies for nonmelanoma metastatic cancers. Clin. Exp. Derm. 2019, 44, 643–646. [Google Scholar] [CrossRef] [PubMed]
- Yazganoglu, K.D.; Topkarci, Z.; Buyukbabani, N.; Baykal, C. Childhood mycosis fungoides: A report of 20 cases from Turkey. J. Eur. Acad. Derm. Venereol. 2013, 27, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Wain, E.M.; Orchard, G.E.; Whittaker, S.J.; Spittle, M.S.M.F.; Russell-Jones, R. Outcome in 34 patients with juvenile-onset mycosis fungoides: A clinical, immunophenotypic, and molecular study. Cancer 2003, 98, 2282–2290. [Google Scholar] [CrossRef] [PubMed]
- Cervini, A.B.; Torres-Huamani, A.N.; Sanchez-La-Rosa, C.; Galluzzo, L.; Solernou, V.; Digiorge, J.; Rubio, P. Mycosis Fungoides: Experience in a Pediatric Hospital. Actas Dermosifiliogr. 2017, 108, 564–570. [Google Scholar] [CrossRef]
- Simon, A.K.; Hollander, G.A.; McMichael, A. Evolution of the immune system in humans from infancy to old age. Proc. Biol. Sci. 2015, 282, 20143085. [Google Scholar] [CrossRef]
- Derhovanessian, E.; Solana, R.; Larbi, A.; Pawelec, G. Immunity, ageing and cancer. Immun. Ageing 2008, 5, 11. [Google Scholar] [CrossRef] [Green Version]
- Sigal, M.; Grossin, M.; Laroche, L.; Basset, F.; Aitken, G.; Haziza, J.L.; Belaich, S. Hypopigmented mycosis fungoides. Clin. Exp. Derm. 1987, 12, 453–454. [Google Scholar] [CrossRef]
- Stone, M.L.; Styles, A.R.; Cockerell, C.J.; Pandya, A.G. Hypopigmented mycosis fungoides: A report of 7 cases and review of the literature. Cutis 2001, 67, 133–138. [Google Scholar]
- Pradhan, D.; Jedrych, J.J.; Ho, J.; Akilov, O.E. Hypopigmented Mycosis Fungoides with Large Cell Transformation in a Child. Pediatr. Dermatol. 2017, 34, e260–e264. [Google Scholar] [CrossRef] [PubMed]
- Geller, S.; Lebowitz, E.; Pulitzer, M.P.; Horwitz, S.M.; Moskowitz, A.J.; Dusza, S.; Myskowski, P.L. Outcomes and prognostic factors in African American and black patients with mycosis fungoides/Sezary syndrome: Retrospective analysis of 157 patients from a referral cancer center. J. Am. Acad. Dermatol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Furlan, F.C.; Pereira, B.A.; Sotto, M.N.; Sanches, J.A. Hypopigmented mycosis fungoides versus mycosis fungoides with concomitant hypopigmented lesions: Same disease or different variants of mycosis fungoides? Dermatology 2014, 229, 271–274. [Google Scholar] [CrossRef] [PubMed]
- Lambroza, E.; Cohen, S.R.; Phelps, R.; Lebwohl, M.; Braverman, I.M.; DiCostanzo, D. Hypopigmented variant of mycosis fungoides: Demography, histopathology, and treatment of seven cases. J. Am. Acad. Derm. 1995, 32, 987–993. [Google Scholar] [CrossRef]
- Moulonguet, I.; Robert, C.; Baudot, N.; Flageul, B.; Dubertret, L. Hypopigmented mycosis fungoides in a light-skinned woman. Br. J. Derm. 1998, 139, 341–343. [Google Scholar] [CrossRef]
- Grunwald, M.H.; Amichai, B. Localized hypopigmented mycosis fungoides in a 12-year-old caucasian boy. J. Derm. 1999, 26, 70–71. [Google Scholar] [CrossRef]
- Quaglino, P.; Zaccagna, A.; Verrone, A.; Dardano, F.; Bernengo, M.G. Mycosis fungoides in patients under 20 years of age: Report of 7 cases, review of the literature and study of the clinical course. Dermatology 1999, 199, 8–14. [Google Scholar] [CrossRef]
- Qari, M.S.; Li, N.; Demierre, M.F. Hypopigmented mycosis fungoides: Case reports and literature review. J. Cutan Med. Surg. 2000, 4, 142–148. [Google Scholar] [CrossRef]
- Gulekon, A.; Ozsoy, E.; Gurer, M.A.; Ataoglu, O. Hypopigmented mycosis fungoides in an adolescent Turkish boy. Int. J. Derm. 2005, 44, 795–796. [Google Scholar] [CrossRef]
- Hodak, E.; Klein, T.; Gabay, B.; Ben-Amitai, D.; Bergman, R.; Gdalevich, M.; Feinmesser, M.; Maron, L.; David, M. Familial mycosis fungoides: Report of 6 kindreds and a study of the HLA system. J. Am. Acad. Derm. 2005, 52, 393–402. [Google Scholar] [CrossRef]
- Wain, E.M.; Orchard, G.E.; Mayou, S.; Atherton, D.J.; Misch, K.J.; Russell-Jones, R. Mycosis fungoides with a CD56+ immunophenotype. J. Am. Acad. Derm. 2005, 53, 158–163. [Google Scholar] [CrossRef]
- Onsun, N.; Kural, Y.; Su, O.; Demirkesen, C.; Buyukbabani, N. Hypopigmented mycosis fungoides associated with atopy in two children. Pediatr. Derm. 2006, 23, 493–496. [Google Scholar] [CrossRef] [PubMed]
- Grover, S.; Verma, R.; Mani, N.S.; Grewal, R.S.; Singh, G.K. Primary Cutaneous T-cell Lymphoma: Two Rare Presentations. Med. J. Armed Forces India 2010, 66, 73–75. [Google Scholar] [CrossRef] [Green Version]
- Koorse, S.; Tirumalae, R.; Yeliur, I.K.; Jayaseelan, E. Clinicopathologic profile of hypopigmented mycosis fungoides in India. Am. J. Derm. 2012, 34, 161–164. [Google Scholar] [CrossRef] [PubMed]
- Hassab-El-Naby, H.M.; El-Khalawany, M.A. Hypopigmented mycosis fungoides in Egyptian patients. J. Cutan. Pathol. 2013, 40, 397–404. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.A.; Yu, J.B. Hypopigmented mycosis fungoides in a chinese woman. Indian J. Dermatol. 2013, 58, 161. [Google Scholar] [CrossRef]
- Alhumidi, A.A. Hypopigmented mycosis fungoides in Saudi Arabia, epidemiological and pathological study. J. Dermatol. Dermatol. Surg. 2014, 18, 8–12. [Google Scholar] [CrossRef] [Green Version]
- Boulos, S.; Vaid, R.; Aladily, T.N.; Ivan, D.S.; Talpur, R.; Duvic, M. Clinical presentation, immunopathology, and treatment of juvenile-onset mycosis fungoides: A case series of 34 patients. J. Am. Acad. Derm. 2014, 71, 1117–1126. [Google Scholar] [CrossRef]
- Abdel-Halim, M.; El-Nabarawy, E.; El Nemr, R.; Hassan, A.M. Frequency of hypopigmented mycosis fungoides in Egyptian patients presenting with hypopigmented lesions of the trunk. Am. J. Derm. 2015, 37, 834–840. [Google Scholar] [CrossRef]
- Mateeva, V.; Kadurina, M. Clinical, Histological and Immunohistochemical Changes in Hypopigmented Mycosis Fungoides in Response to Narrow-Band UVB Phototherapy. J. Pigment. Disord. 2015, 2. [Google Scholar] [CrossRef] [Green Version]
- Joseph, M.X.; Brown, A.D.; Davis, L.S. The importance of lymph node examination: Simultaneous diagnosis of hypopigmented mycosis fungoides and follicular B-cell lymphoma. Jaad Case Rep. 2018, 4, 590–592. [Google Scholar] [CrossRef] [PubMed]
- Vilas Boas, P.; Hernandez-Aragues, I.; Suarez-Fernandez, R.; Campos-Dominguez, M. Hypopigmented patches on the buttocks of a 7-year-old boy. Clin. Exp. Derm. 2018, 43, 485–487. [Google Scholar] [CrossRef] [PubMed]
- Landgrave-Gomez, I.; Ruiz-Arriaga, L.F.; Toussaint-Caire, S.; Vega-Memije, M.E.; Lacy-Niebla, R.M. Epidemiological, clinical, histological, and immunohistochemical study on hypopigmented epitheliotropic T-cell dyscrasia and hypopigmented mycosis fungoides. Int. J. Dermatol 2019. [Google Scholar] [CrossRef] [PubMed]
- el-Hoshy, K.; Hashimoto, K. Adolescence mycosis fungoides: An unusual presentation with hypopigmentation. J. Derm. 1995, 22, 424–427. [Google Scholar] [CrossRef]
- Ben-Amitai, D.; Michael, D.; Feinmesser, M.; Hodak, E. Juvenile mycosis fungoides diagnosed before 18 years of age. Acta Derm. Venereol. 2003, 83, 451–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsiao, P.F.; Hsiao, C.H.; Tsai, T.F.; Jee, S.H. Minimal residual disease in hypopigmented mycosis fungoides. J. Am. Acad. Dermatol. 2006, 54, S198–S201. [Google Scholar] [CrossRef]
- Ozcan, D.; Seckin, D.; Ozdemir, B.H. Hypopigmented macules in an adult male patient. Clin. Exp. Derm. 2008, 33, 667–668. [Google Scholar] [CrossRef]
- Cho-Vega, J.H.; Tschen, J.A.; Duvic, M.; Vega, F. Early-stage mycosis fungoides variants: Case-based review. Ann. Diagn. Pathol. 2010, 14, 369–385. [Google Scholar] [CrossRef]
- Nanda, A.; AlSaleh, Q.A.; Al-Ajmi, H.; Al-Sabah, H.; Elkashlan, M.; Al-Shemmari, S.; Demierre, M.F. Mycosis fungoides in Arab children and adolescents: A report of 36 patients from Kuwait. Pediatr. Derm. 2010, 27, 607–613. [Google Scholar] [CrossRef]
- Khopkar, U.; Doshi, B.R.; Dongre, A.M.; Gujral, S. A study of clinicopathologic profile of 15 cases of hypopigmented mycosis fungoides. Indian J. Dermatol. Venereol. Leprol. 2011, 77, 167–173. [Google Scholar] [CrossRef]
- Rizzo, F.A.; Vilar, E.G.; Pantaleao, L.; Fonseca, E.C.; Magrin, P.F.; Henrique-Xavier, M.; Rochael, M.C. [Mycosis fungoides in children and adolescents: A report of six cases with predominantly hypopigmentation, along with a literature review]. Derm. Online J. 2012, 18, 5. [Google Scholar]
- Uhlenhake, E.E.; Mehregan, D.M. Annular hypopigmented mycosis fungoides: A novel ringed variant. J. Cutan. Pathol. 2012, 39, 535–539. [Google Scholar] [CrossRef] [PubMed]
- Wongpraparut, C.; Setabutra, P. Phototherapy for hypopigmented mycosis fungoides in Asians. Photodermatol. Photoimmunol. Photomed. 2012, 28, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Gameiro, A.; Gouveia, M.; Tellechea, O.; Moreno, A. Childhood hypopigmented mycosis fungoides: A commonly delayed diagnosis. BMJ Case Rep. 2014. [Google Scholar] [CrossRef] [Green Version]
- Heng, Y.K.; Koh, M.J.; Giam, Y.C.; Tang, M.B.; Chong, W.S.; Tan, S.H. Pediatric mycosis fungoides in Singapore: A series of 46 children. Pediatr. Derm. 2014, 31, 477–482. [Google Scholar] [CrossRef] [PubMed]
- Fatemi Naeini, F.; Abtahi-Naeini, B.; Sadeghiyan, H.; Nilforoushzadeh, M.A.; Najafian, J.; Pourazizi, M. Mycosis fungoides in Iranian population: An epidemiological and clinicopathological study. J. Ski. Cancer 2015, 306543. [Google Scholar] [CrossRef] [PubMed]
- Naeini, F.F.; Soghrati, M.; Abtahi-Naeini, B.; Najafian, J.; Rajabi, P. Co-existence of various clinical and histopathological features of mycosis fungoides in a young female. Indian J. Dermatol. 2015, 60, 214. [Google Scholar] [CrossRef]
- Ichimura, Y.; Sugaya, M.; Morimura, S.; Suga, H.; Sato, S.; Mori, S.; Takahashi, H.; Akutsu, Y. Two cases of CD8-positive hypopigmented mycosis fungoides without TOX expression. Int J. Dermatol. 2016, 55, e164–e167. [Google Scholar] [CrossRef]
- Valencia Ocampo, O.J.; Julio, L.; Zapata, V.; Correa, L.A.; Vasco, C.; Correa, S.; Velasquez-Lopera, M.M. Mycosis Fungoides in Children and Adolescents: A Series of 23 Cases. Actas Dermosifiliogr. 2019. [Google Scholar] [CrossRef]
- Kalay Yildizhan, I.; Sanli, H.; Akay, B.N.; Surgun, E.; Heper, A. CD8(+) cytotoxic mycosis fungoides: A retrospective analysis of clinical features and follow-up results of 29 patients. Int J. Derm. 2020, 59, 127–133. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study | Number of Patients | T-Cell Phenotype | Age of Onset (years) | Fitzpatrick Phototype/Color of Skin/ Ethnicity | Stage at Diagnosis | Disease Progressed |
|---|---|---|---|---|---|---|
| Sigal et al., 1987 [79] | 1 | CD4+ | 64 | Caucasian | NS a | Yes a |
| Lambroza et al., 1995 [84] | 1 | CD4+ | 25 | Trinidadian | IB | No |
| Moulonguet et al., 1998 [85] | 1 | CD4+ | 31 | Caucasian/Light skinned | IA | No |
| Grunwald and Amichai, 1999 [86] | 1 | CD4+ | 12 | Caucasian | NS | No |
| Quaglino et al., 1999 [87] | 1 | CD4+ | 16 | White | IA | No |
| Qari et al., 2000 [88] | 3 | CD4+: 2 patients CD4+/CD8+: 1 patient | 31 (mean) | Hispanic, Portuguese black, and African- American | NS | NS |
| Stone et al., 2001 [80] | 1 | CD4+ | 56 | Black | I | Yes b |
| Ardigo et al., 2003 [16] | 5 | CD4+: 4 CD4+/CD8+: 1 | 34.4 (mean) | Caucasian | NS | NS |
| Gulekon et al., 2005 [89] | 1 | CD4+ | 3 | Turkish | NS | NS |
| Hodak et al., 2005 [90] | 2 | CD4+ | 1 (mean) | NS | IB and IA | 1 patient (IIA) |
| Wain et al., 2005 [91] | 2 | CD56+ | 21.5 (mean) | Asian and Somalian | IA and IB | No |
| Onsun et al., 2006 [92] | 1 | CD4+ | 8 | Type II | IB | No |
| Hodak et al., 2006 [48] | 5 | CD4–/CD8– | 17.8 (mean at diagnosis) | NS | IA: 1 patient IB: 4 patients | No |
| Grover et al., 2010 [93] | 1 | CD4+ | 2 | Indian | IB | No |
| Koorse et al., 2012 [94] | 4 | CD4+ | NS | Indian | NS | NS |
| Hassab-El-Naby and El-Khalawany, 2013 [95] | 9 | CD4+ | 37 (mean) | Type III: 4 patients Type IV: 5 patients | IA: 7 patients IB: 2 patients | No |
| Zhang and Yu, 2013 [96] | 1 | CD4+/CD8+ | 9 | Chinese | NS | NS |
| Alhumidi, 2014 [97] | 4 | CD4+: 2 patients CD4+/CD8+: 2 patients | 23 (mean) | Saudi Arabian Type III | NS | No c |
| Boulos et al., 2014 [98] | 7 | CD4+ | 8.8 (mean) | IA: 3 patients IB: 4 patients | 1 patient (IB) | |
| Furlan et al., 2014 [12] | 4 | CD4+ | 31 (mean) | Caucasian mixed race and black | IA: 1 patient IB: 2 patients IIA: 1 patient | NS |
| Abdel-Halin et al., 2015 [99] | 8 | CD4+: 3 patients CD4+/CD8+: 5 patients | NS | Egyptian | NS | NS |
| Mateeva and Kadurina, 2015 [100] | 1 | CD4+ | 22 | Caucasian/Bulgarian descent Type III | NS | No |
| Rowe et al., 2016 [11] | 1 | CD4+ | 71 | Dark skin | NS d | NS |
| Cervini et al., 2017 [76] | 8 | CD4+: 2 patients CD4+/CD8+: 6 patients | 11.8 (mean at diagnosis) | Argentinian | IA: 1 patient IB: 7 patients | Yes e |
| Rodney et al., 2017 [9] | 5 | CD4+: 3 patients CD4+/CD8+: 2 patients | 36 (mean) | African-American and African | IA: 1 patient IB: 4 patients | No |
| Joseph et al., 2018 [101] | 1 | CD4+ | 50 | NS | IA | No |
| Vilas Boas et al., 2018 [102] | 1 | CD4+ | 5 | Hispanic | NS | NS |
| Landgrave-Gomez et al., 2019 [103] | 6 | CD4+: 2 patients CD4+/CD8+: 4 patients | NS | NS | NS | NS |
| Study | Number of Patients | Age of Onset (years) | Fitzpatrick Phototype/Color of Skin/ Ethnicity | Other Variants of MF as Published | Stage at Diagnosis | Disease Progressed |
|---|---|---|---|---|---|---|
| Sigal et al., 1987 [79] | 1 | 64 | White | Erythematous papules | NS a | Yes a |
| el-Hoshy and Hashimoto, 1995 [104] | 1 | 15 | Black | Erythematous nodules | NS | No |
| Lambroza et al., 1995 [84] | 1 | 21 | Jamaican-American | Hyperpigmented | IB | No |
| Qari et al., 2000 [88] | 3 | 25.3 (mean) | Hispanic/dark and Portuguese/black | Red papules, pink patches, erythematous, and scaly plaques | NS | No |
| Stone et al., 2000 [80] | 1 | 56 | Type V | Hyperpigmented macules later evolved to erythematous lesions | I | Yes b |
| Ardigo et al., 2003 [16] | 6 | 30.1 (mean) | Caucasian | Erythematous lesions | NS | 2 patients c |
| Ben-Amitai et al., 2003 [105] | 5 | 4.6 (mean) | Light and pigmented | Classic erythematous lesions | IA: 2 patients IB: 3 patients | No |
| Wain et al., 2003 [75] | 2 | 10.5 (mean) | NS | Poikiloderma and pilotropic | IB | No |
| Hodak et al., 2005 [90] | 2 | 1 (mean) | NS | Psoriasiform | IB and IA | 1 patient (IIA) |
| Wain et al., 2005 [91] | 2 | 21.5 (mean) | Asian and Somalian | Poikiloderma and hyperpigmented | IA and IB | No |
| Hodak et al., 2006 [48] | 1 | 12 (at diagnosis) | NS | Classic | IB | No |
| Hsiao et al., 2006 [106] | 1 | 12 | NS | Hyperpigmented | IA | No |
| Onsun et al., 2006 [92] | 1 | 5 (mean) | Type II: 1 patient Type III: 1 patient | Erythematous | IB | No |
| Ozcan et al., 2008 [107] | 1 | 30 | Turkish | Erythematous | NS | NS |
| Cho-Vega et al., 2010 [108] | 1 | 34 | African-American | Poikiloderma | IB | No |
| Nanda et al., 2010 [109] | 3 | 7.5 (mean) | Bedouin and Kuwaiti | Pityriasis lichenoides chronica-like and folliculotropic | IA, IB, and IIA | NS |
| Khopkar et al., 2011 [110] | 5 | 19 (mean) | Asian with dark skin type | Poikiloderma and erythematous | NS d | NS d |
| Yazganoglu et al., 2013 [74] | 8 | 6.1 (mean) | NS | Erythematous and purpuric | IA: 5 patients IB: 3 patients | No |
| Rizzo et al., 2012 [111] | 1 | 15 (at diagnosis) | NS | Erythematous | IB | NS |
| Uhlenhake and Mehregan, 2012 [112] | 1 | 49 | African-American | Hypopigmented macules with hyperpigmented/erythematous centers | NS | NS |
| Wongpraparut and Setabutra, 2012 [113] | 1 | 36 | Type IV | Erythematous | IA | No |
| Ahumidi, 2014 [97] | 1 | 5 | Type III e | Pink papules | NS | NS |
| Furlan et al., 2014 [83] | 14 | 29.5 (median) | Mixed race, Caucasian, Black, and Asian/Brazilian | Erythematous, poikiloderma, hyperpigmented, purpuric, and hyperkeratotic | IA: 7 patients IB: 6 patients IIA: 1 patient | NS |
| Gameiro et al., 2014 [114] | 1 | 5 | Type III | Erythematous papules | IB | No |
| Heng et al., 2014 [115] | 11 | NS | Chinese, Malay, Indian, and others | Red, scaly papules and plaques | NS | NS |
| Fatemi Naeini et al., 2015 [116] | 2 | NS | Iranian | NS | NS | NS |
| Naeini et al., 2015 [117] | 1 | 26 | Iranian | Erythematous | IB | NS |
| Ichimura et al., 2016 [118] | 1 | 20 | Japanese | Scaly erythema | IB | No |
| Cervini et al., 2017 [76] | 2 | 11 (mean at diagnosis) | Argentinian | Classic MF | IVA2f and IB | No |
| Pradhan et al., 2017 [81] | 1 | 2 | Iranian | Large cell transformation | IB | No |
| Landgrave-Gomez et al., 2019 [103] | NS | NS | Hispanic | Hyperpigmentation and erythema | NS | NS |
| Valencia Ocampo et al., 2019 [119] | 5 | 7.8 (mean) | Type II: 1 patient Type III: 1 patient Type IV: 2 patients Type V: 1 patient | Erythematous | IA: 1 patient IB: 4 patients | No |
| Geller et al., 2019 [82] | 34 | NS | African-American | Erythematous and hyperpigmented | NS | No |
| Kalay et al., 2020 [120] | 4 | 30.5 (mean at diagnosis) | Turkish | Follicular hyperkeratosis, erythematous, and hyperpigmented | IA | No |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez Villarreal, A.; Gantchev, J.; Lagacé, F.; Barolet, A.; Sasseville, D.; Ødum, N.; Charli-Joseph, Y.V.; Hernández Salazar, A.; Litvinov, I.V. Hypopigmented Mycosis Fungoides: Loss of Pigmentation Reflects Antitumor Immune Response in Young Patients. Cancers 2020, 12, 2007. https://doi.org/10.3390/cancers12082007
Martínez Villarreal A, Gantchev J, Lagacé F, Barolet A, Sasseville D, Ødum N, Charli-Joseph YV, Hernández Salazar A, Litvinov IV. Hypopigmented Mycosis Fungoides: Loss of Pigmentation Reflects Antitumor Immune Response in Young Patients. Cancers. 2020; 12(8):2007. https://doi.org/10.3390/cancers12082007
Chicago/Turabian StyleMartínez Villarreal, Amelia, Jennifer Gantchev, François Lagacé, Augustin Barolet, Denis Sasseville, Niels Ødum, Yann Vincent Charli-Joseph, Amparo Hernández Salazar, and Ivan V. Litvinov. 2020. "Hypopigmented Mycosis Fungoides: Loss of Pigmentation Reflects Antitumor Immune Response in Young Patients" Cancers 12, no. 8: 2007. https://doi.org/10.3390/cancers12082007
APA StyleMartínez Villarreal, A., Gantchev, J., Lagacé, F., Barolet, A., Sasseville, D., Ødum, N., Charli-Joseph, Y. V., Hernández Salazar, A., & Litvinov, I. V. (2020). Hypopigmented Mycosis Fungoides: Loss of Pigmentation Reflects Antitumor Immune Response in Young Patients. Cancers, 12(8), 2007. https://doi.org/10.3390/cancers12082007