Long-Term Treatment of Cancer-Associated Thrombosis (CAT) Beyond 6 Months in the Medical Practice: USCAT, a 432-Patient Retrospective Non-Interventional Study


 , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Inclusion Criteria
2.2. Study Outcomes
2.3. Data Management and Statistics
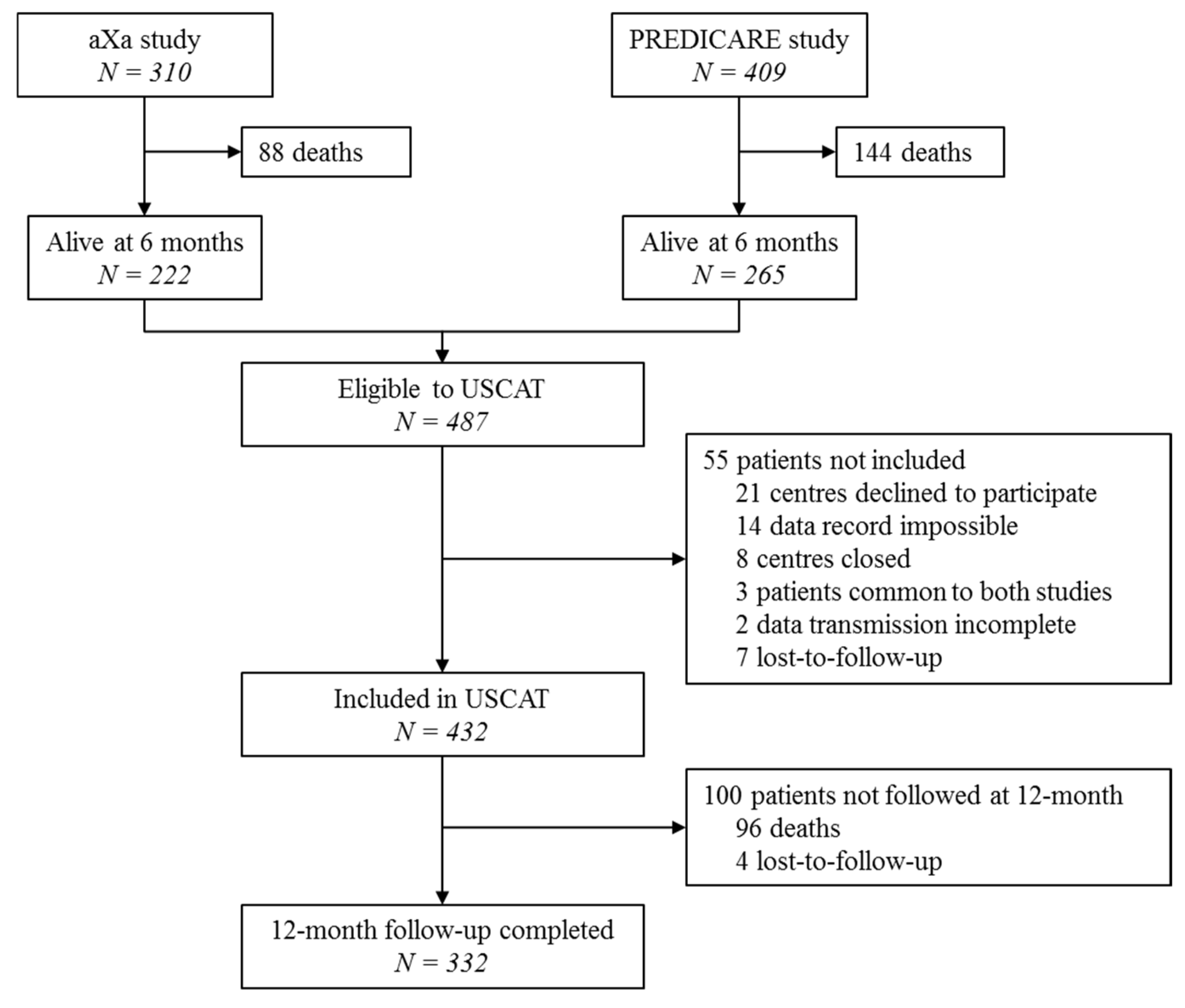
3. Results
3.1. Maintained Anticoagulant Treatment Beyond 6 Months Following the Index VTE
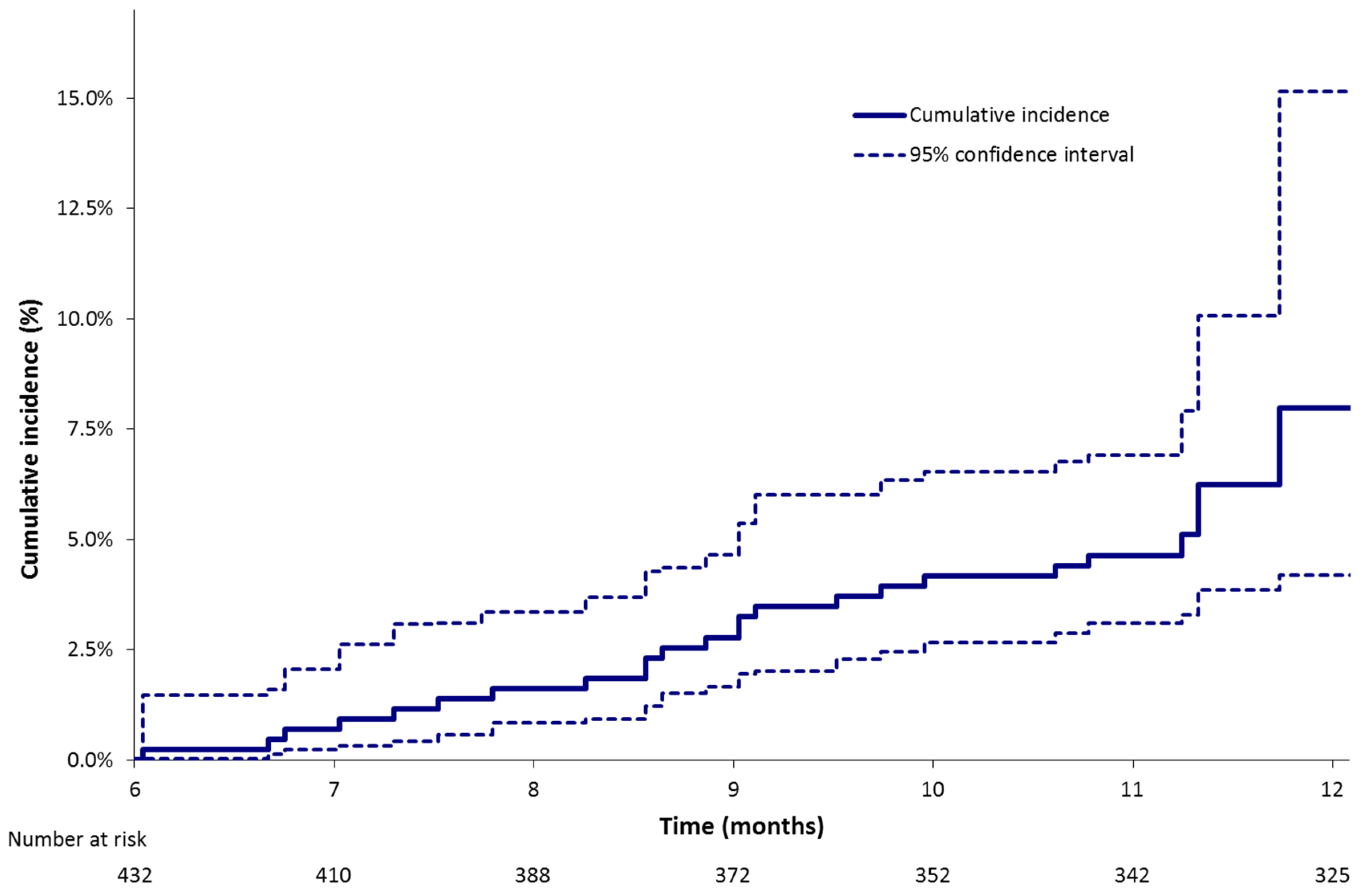
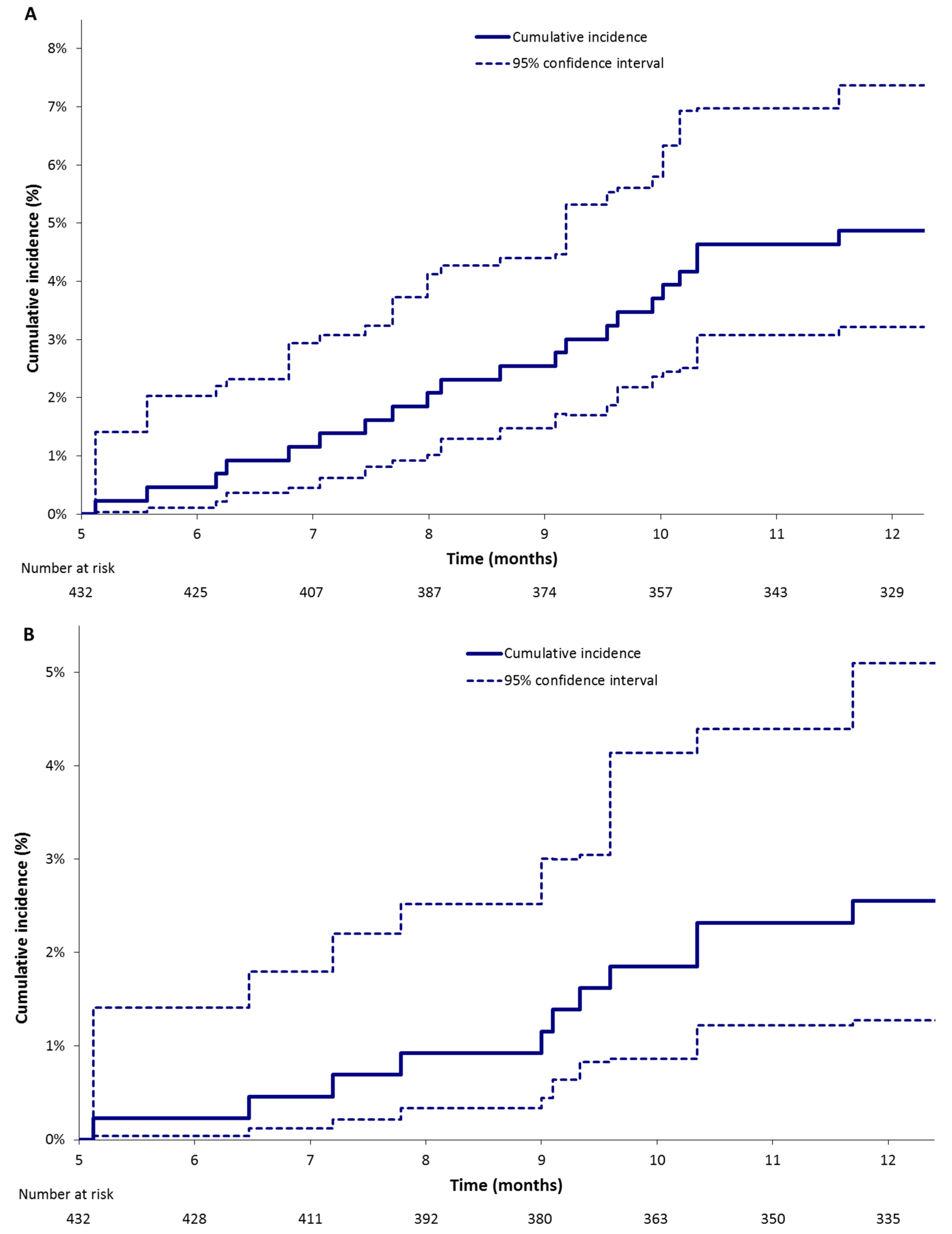
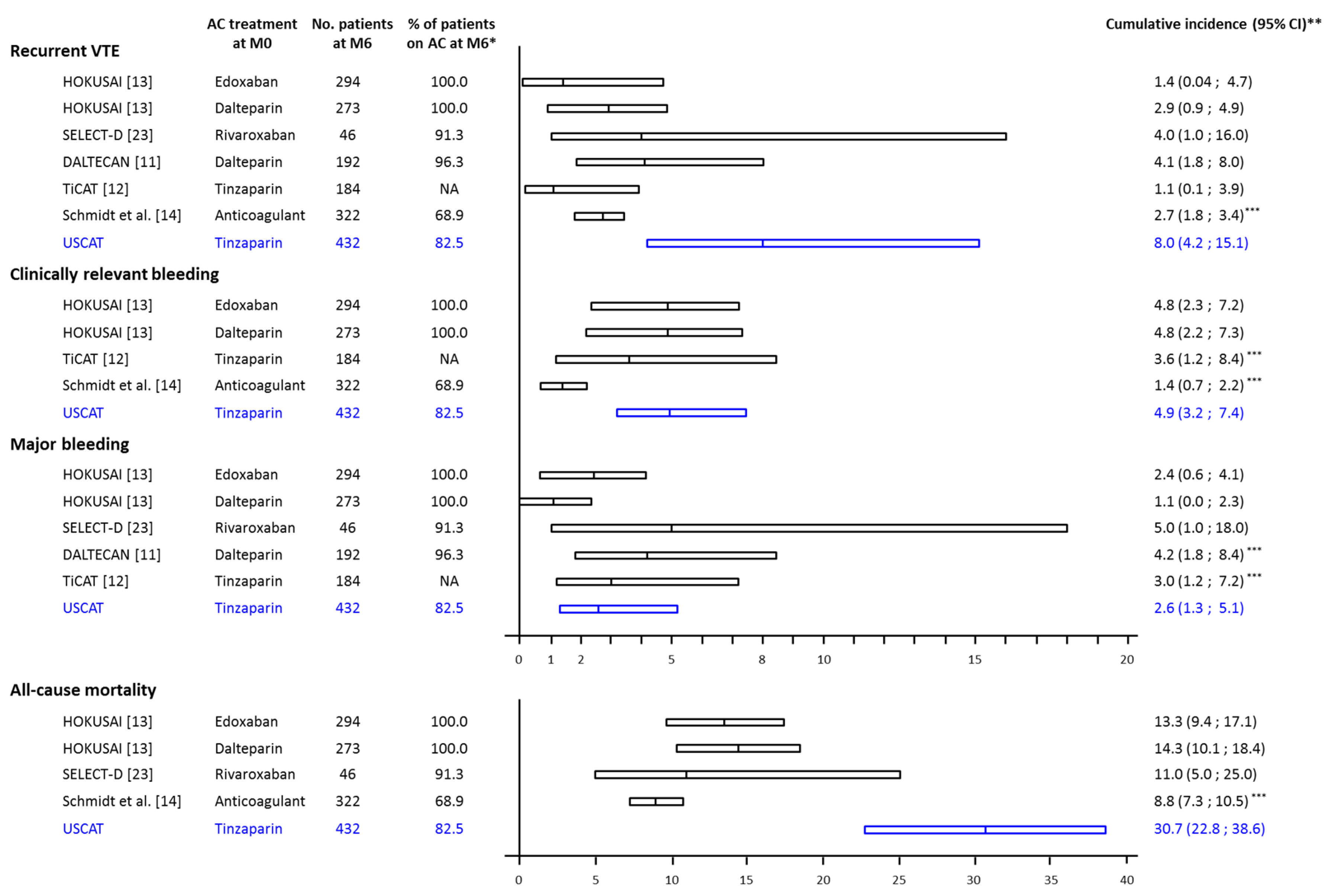
3.2. Clinical Outcomes Beyond 6 Months
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix
Investigators and Study Centers
References
- Ay, C.; Pabinger, I.; Cohen, A.T. Cancer-associated venous thromboembolism: Burden, mechanisms, and management. Thromb. Haemost. 2017, 117, 219–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prandoni, P.; Lensing, A.W.; Piccioli, A.; Bernardi, E.; Simioni, P.; Girolami, B.; Marchiori, A.; Sabbion, P.; Prins, M.H.; Noventa, F.; et al. Recurrent venous thromboembolism and bleeding complications during anticoagulant treatment in patients with cancer and venous thrombosis. Blood 2002, 100, 3484–3488. [Google Scholar] [CrossRef] [Green Version]
- Sorensen, H.T.; Mellemkjaer, L.; Olsen, J.H.; Baron, J.A. Prognosis of cancers associated with venous thromboembolism. N. Engl. J. Med. 2000, 343, 1846–1850. [Google Scholar] [CrossRef] [PubMed]
- Farge, D.; Frere, C.; Connors, J.M.; Ay, C.; Khorana, A.A.; Munoz, A.; Brenner, B.; Kakkar, A.; Rafii, H.; Solymoss, S.; et al. 2019 international clinical practice guidelines for the treatment and prophylaxis of venous thromboembolism in patients with cancer. Lancet Oncol. 2019, 20, e566–e581. [Google Scholar] [CrossRef] [Green Version]
- Kearon, C.; Akl, E.A.; Ornelas, J.; Blaivas, A.; Jimenez, D.; Bounameaux, H.; Huisman, M.; King, C.S.; Morris, T.A.; Sood, N.; et al. Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. Chest 2016, 149, 315–352. [Google Scholar] [CrossRef] [PubMed]
- Key, N.S.; Khorana, A.A.; Kuderer, N.M.; Bohlke, K.; Lee, A.Y.Y.; Arcelus, J.I.; Wong, S.L.; Balaban, E.P.; Flowers, C.R.; Francis, C.W.; et al. Venous Thromboembolism Prophylaxis and Treatment in Patients With Cancer: ASCO Clinical Practice Guideline Update. J. Clin. Oncol. 2020, 38, 496–520. [Google Scholar] [CrossRef]
- Sanchez, O.; Benhamou, Y.; Bertoletti, L.; Constans, J.; Couturaud, F.; Delluc, A.; Elias, A.; Fischer, A.M.; Frappe, P.; Gendron, N.; et al. Recommendations for best practice in the management of venous thromboembolic disease in adults. Long version. Rev. Mal. Respir. 2019, 19, 3210–3214. [Google Scholar] [CrossRef]
- Kearon, C.; Ageno, W.; Cannegieter, S.C.; Cosmi, B.; Geersing, G.J.; Kyrle, P.A.; Subcommittees on Control of Anticoagulation; Predictive and Diagnostic Variables in Thrombotic Disease. Categorization of patients as having provoked or unprovoked venous thromboembolism: Guidance from the SSC of ISTH. J. Thromb. Haemost. 2016, 14, 1480–1483. [Google Scholar] [CrossRef]
- Khorana, A.A.; Carrier, M.; Garcia, D.A.; Lee, A.Y. Guidance for the prevention and treatment of cancer-associated venous thromboembolism. J. Thromb. Thrombolysis 2016, 41, 81–91. [Google Scholar] [CrossRef] [Green Version]
- Streiff, M.B.; Holmstrom, B.; Angelini, D.; Ashrani, A.; Bockenstedt, P.L.; Chesney, C.; Fanikos, J.; Fenninger, R.B.; Fogerty, A.E.; Gao, S.; et al. NCCN Guidelines Version 1.2020 Cancer-Associated Venous Thromboembolic Disease. J. Natl. Compr. Cancer Netw. 2020. Available online: https://www.nccn.org/professionals/physician_gls/pdf/vte.pdf (accessed on 3 August 2020).
- Francis, C.W.; Kessler, C.M.; Goldhaber, S.Z.; Kovacs, M.J.; Monreal, M.; Huisman, M.V.; Bergqvist, D.; Turpie, A.G.; Ortel, T.L.; Spyropoulos, A.C.; et al. Treatment of venous thromboembolism in cancer patients with dalteparin for up to 12 months: The DALTECAN Study. J. Thromb. Haemost. 2015, 13, 1028–1035. [Google Scholar] [CrossRef] [PubMed]
- Jara-Palomares, L.; Solier-Lopez, A.; Elias-Hernandez, T.; Asensio-Cruz, M.; Blasco-Esquivias, I.; Marin-Barrera, L.; de la Borbolla-Artacho, M.R.; Praena-Fernandez, J.M.; Montero-Romero, E.; Navarro-Herrero, S.; et al. Tinzaparin in cancer associated thrombosis beyond 6months: TiCAT study. Thromb. Res. 2017, 157, 90–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Nisio, M.; van Es, N.; Carrier, M.; Wang, T.F.; Garcia, D.; Segers, A.; Weitz, J.; Buller, H.; Raskob, G. Extended treatment with edoxaban in cancer patients with venous thromboembolism: A post-hoc analysis of the Hokusai-VTE Cancer study. J. Thromb. Haemost. 2019, 17, 1866–1874. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, R.A.; Al Zaki, A.; Desilet, N.; Szefer, E.; Ratnaweera, N.; Peterson, E.; Lee, A.Y.Y. Patient characteristics and long-term outcomes beyond the first 6 months after a diagnosis of cancer-associated venous thromboembolism. Thromb. Res. 2020, 188, 106–114. [Google Scholar] [CrossRef]
- Meyer, G.; Chapelle, C.; Girard, P.; Scotté, F.; Lamblin, A.; Laporte, S. Validation of the Ottawa Score in Cancer Patients with Venous Thromboembolism. the Predicare Cohort Study. Blood 2019, 134, 167. [Google Scholar] [CrossRef]
- Schulman, S.; Kearon, C. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J. Thromb. Haemost. 2005, 3, 692–694. [Google Scholar] [CrossRef]
- Kaatz, S.; Ahmad, D.; Spyropoulos, A.C.; Schulman, S.; the Subcommittee on Control of Anticoagulation. Definition of clinically relevant non-major bleeding in studies of anticoagulants in atrial fibrillation and venous thromboembolic disease in non-surgical patients: Communication from the SSC of the ISTH. J. Thromb. Haemost. 2015, 13, 2119–2126. [Google Scholar] [CrossRef]
- Scotte, F.; Leroy, P.; Chastenet, M.; Aumont, L.; Benatar, V.; Elalamy, I. Treatment and Prevention of Cancer-Associated Thrombosis in Frail Patients: Tailored Management. Cancers (Basel) 2019, 11, 48. [Google Scholar] [CrossRef] [Green Version]
- Mahé, I.; Chidiac, J.; Pinson, M.; Swarnkar, P.; Nelson, A.; Noble, S. Patients experience of living with cancer associated thrombosis in France (Le PELICAN). Thromb. Res. 2020, 194, 66–71. [Google Scholar] [CrossRef]
- Kraaijpoel, N.; Di Nisio, M.; Mulder, F.I.; van Es, N.; Beyer-Westendorf, J.; Carrier, M.; Garcia, D.; Grosso, M.; Kakkar, A.K.; Mercuri, M.F.; et al. Clinical Impact of Bleeding in Cancer-Associated Venous Thromboembolism: Results from the Hokusai VTE Cancer Study. Thromb. Haemost. 2018, 118, 1439–1449. [Google Scholar] [CrossRef]
- Mahé, I.; Elalamy, I.; Gerotziafas, G.T.; Girard, P. Treatment of Cancer-Associated Thrombosis: Beyond HOKUSAI. TH Open 2019, 3, e309–e315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahé, I.; Chidiac, J.; Bertoletti, L.; Font, C.; Trujillo-Santos, J.; Peris, M.; Perez Ductor, C.; Nieto, S.; Grandone, E.; Monreal, M.; et al. The Clinical Course of Venous Thromboembolism May Differ According to Cancer Site. Am. J. Med. 2017, 130, 337–347. [Google Scholar] [CrossRef] [PubMed]
- Marshall, A.; Levine, M.; Hill, C.; Hale, D.; Thirlwall, J.; Wilkie, V.; French, K.; Kakkar, A.; Lokare, A.; Maraveyas, A.; et al. Treatment of cancer-associated venous thromboembolism: 12-month outcomes of the placebo versus rivaroxaban randomization of the SELECT-D Trial (SELECT-D: 12m). J. Thromb. Haemost. 2020, 18, 905–915. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| International Guidelines | Long-Term Anticoagulation | Treatment Duration |
|---|---|---|
| ACCP [5] | LMWH over VKA (Grade 2B), dabigatran (Grade 2C), rivaroxaban (Grade 2C), apixaban (Grade 2C), or edoxaban (Grade 2C) | >3 months in patients at low bleeding risk (1B) or high risk of bleeding (2B) |
| ASCO [6] | LMWH, edoxaban, or rivaroxaban for at least 6 months are preferred because of improved efficacy over vitamin K antagonists (VKA). Caution with DOAC warranted in settings with high risk for mucosal bleeding. Drug-drug interaction should be checked prior to using a DOAC (strong) | Anticoagulation with LMWH, DOAC, or VKA beyond the initial 6 months should be offered to select patients with active cancer, such as those with metastatic disease or those receiving chemotherapy (weak to moderate). |
| ACI FORUM [9] | LMWH | At least 6 months Stop treatment in the absence of tumor activity of antineoplastic treatment On the contrary, maintain treatment beyond 6 months with periodic re-evaluation of benefit/risk ratio |
| ITAC-CME [4] | LMWH preferred to VKA (1A) DOAC if CrCl ≥ 30 mL/min, in the absence of drug-drug interactions or insufficient digestive absorption (1A) Precaution if GI cancer | At least 6 months (1A) Beyond 6 months discuss prolongation case by case based on the analysis of benefit/risk ratio (Guidance) |
| NCCN [10] | LMWH recommended Category 1 recommendations for both edoxaban and apixaban VKA possible | At least 3 months Maintain treatment as long cancer is active, anti-neoplastic treatment maintained or increased risk of VTE recurrence (2A) |
| IFS [7] | LMWH recommended (1+) DOAC if LMWH not tolerated (2+) | At least 6 months Maintain treatment beyond 6 months as long cancer is active, based on patient’s preference, bleeding risk: LMWH (2+), VKA (2+) or DOAC (2+) full treatment dose |
| Patient Characteristics | All Patients (n = 432) |
|---|---|
| Mean age (years) ± SD | 66.5 ± 12.7 |
| Age ≥ 75 years, no. (%) | 128 (29.6) |
| Male sex, no. (%) | 207 (47.9) |
| Site of cancer disease, no. (%) | |
| Solid tumour | 394 (91.2) |
| Colorectal | 85 (21.6) |
| Lung | 79 (20.1) |
| Breast | 66 (16.8) |
| Genitourinary | 62 (15.7) |
| Gynaecologic | 42 (10.7) |
| Pancreas | 14 (3.6) |
| Upper gastrointestinal | 13 (3.0) |
| Hepatobiliary | 10 (2.5) |
| Other | 23 (5.3) |
| Haematologic tumour | 30 (6.9) |
| Non-Hodgkin lymphoma | 14 (46.7) |
| Multiple myeloma | 7 (23.3) |
| Leukaemia | 7 (23.3) |
| Hodgkin lymphoma | 2 (6.7) |
| Other | 8 (1.9) |
| Stage (n = 390), no. (%) | |
| 1 | 45 (11.5) |
| 2 | 25 (6.4) |
| 3 or 4 | 320 (82.1) |
| Cancer evolution (n = 424), no. (%) | |
| Remission | 66 (15.6) |
| Stability | 141 (33.3) |
| Progression | 217 (51.2) |
| Index VTE *, no. (%) | |
| PE ± DVT | 318 (73.6) |
| DVT alone | 114 (26.4) |
| -Proximal DVT | 70 |
| -Distal DVT | 54 |
| -Unclear | 2 |
| Anticoagulant treatment (n = 422), no. (%) | |
| Stopped before the end of the initial 6-month treatment period | 60 (14.2) |
| Stopped at the end of the initial 6-month treatment period | 14 (3.3) |
| Maintained at 6 months | 348 (82.5) |
| LMWH | 256 (73.6) |
| VKA | 56 (16.1) |
| DOAC | 30 (8.6) |
| UFH | 3 (0.9) |
| Fondaparinux | 3 (0.9) |
| Clinical Outcomes | All Patients n = 432 * | According to the Type of Cancer | According to the State of Cancer | ||||
|---|---|---|---|---|---|---|---|
| Colorectal n = 85 | Lung n = 79 | Breast n = 66 | Other n = 202 | Cancer Progression n = 217 | Metastatic Cancer n = 320 | ||
| VTE recurrence¶ | 8.0 (4.2; 15.1) | 12.6 (4.6; 34.3) | 13.8 (8.4; 22.8) | 1.5 (0.3; 8.4) | 3.5 (1.7; 7.0) | 10.6 (5.3; 21.2) | 8.7 (5.1; 14.9) |
| CRB **¶ | 4.9 (3.2; 7.4) | 5.8 (2.5; 13.6) | 1.3 (0.2; 9.1) | 4.5 (1.5; 13.8) | 6.0 (3.4; 10.4) | 8.8 (5.6; 13.7) | 5.3 (3.2; 8.8) |
| Major bleeding¶ | 2.6 (1.3; 5.1) | 5.8 (2.6; 13.2) | 0 (0.0) | 1.5 (0.2; 12.1) | 2.5 (1.2; 5.3) | 5.1 (2.8; 9.1) | 2.8 (1.4; 5.6) |
| Deaths § | 30.7 (22.8; 38.6) | 24.2 (11.4; 37.1) | 42.2 (25.0; 59.4) | 15.2 (6.5; 23.8) | 34.5 (19.9; 49.1) | 52.9 (41.0; 64.8) | 36.7 (27.6; 45.7) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahé, I.; Plaisance, L.; Chapelle, C.; Laporte, S.; Planquette, B.; Bertoletti, L.; Couturaud, F.; Falvo, N.; Falchero, L.; Mahé, I.; et al. Long-Term Treatment of Cancer-Associated Thrombosis (CAT) Beyond 6 Months in the Medical Practice: USCAT, a 432-Patient Retrospective Non-Interventional Study. Cancers 2020, 12, 2256. https://doi.org/10.3390/cancers12082256
Mahé I, Plaisance L, Chapelle C, Laporte S, Planquette B, Bertoletti L, Couturaud F, Falvo N, Falchero L, Mahé I, et al. Long-Term Treatment of Cancer-Associated Thrombosis (CAT) Beyond 6 Months in the Medical Practice: USCAT, a 432-Patient Retrospective Non-Interventional Study. Cancers. 2020; 12(8):2256. https://doi.org/10.3390/cancers12082256
Chicago/Turabian StyleMahé, Isabelle, Ludovic Plaisance, Céline Chapelle, Silvy Laporte, Benjamin Planquette, Laurent Bertoletti, Francis Couturaud, Nicolas Falvo, Lionel Falchero, Isild Mahé, and et al. 2020. "Long-Term Treatment of Cancer-Associated Thrombosis (CAT) Beyond 6 Months in the Medical Practice: USCAT, a 432-Patient Retrospective Non-Interventional Study" Cancers 12, no. 8: 2256. https://doi.org/10.3390/cancers12082256
APA StyleMahé, I., Plaisance, L., Chapelle, C., Laporte, S., Planquette, B., Bertoletti, L., Couturaud, F., Falvo, N., Falchero, L., Mahé, I., Helfer, H., Chidiac, J., & Meyer, G. (2020). Long-Term Treatment of Cancer-Associated Thrombosis (CAT) Beyond 6 Months in the Medical Practice: USCAT, a 432-Patient Retrospective Non-Interventional Study. Cancers, 12(8), 2256. https://doi.org/10.3390/cancers12082256