pT1 Colorectal Cancer Detected in a Colorectal Cancer Mass Screening Program: Treatment and Factors Associated with Residual and Extraluminal Disease

 ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Study Design
2.2. Description of the Galician CRC Screening Program
2.3. Baseline Data
2.4. Treatment and Histology
2.5. Outcomes
- Endoscopic resection: We determined that endoscopic resection was achieved if the resection was considered complete by the endoscopist, either piecemeal or in block.
- Surgical rescue: We defined surgical rescue as when surgical resection was indicated after an initial complete endoscopic resection.
- Residual disease after endoscopic resection: We define it as residual adenocarcinoma in the intestinal wall, in the lymph node or a relapse during follow-up.
- Extraluminal disease after surgical resection: We define it as a lymph node involvement detected in the surgical specimen or a relapse during follow-up.
2.6. Statistical Analysis
2.7. Ethical Issues
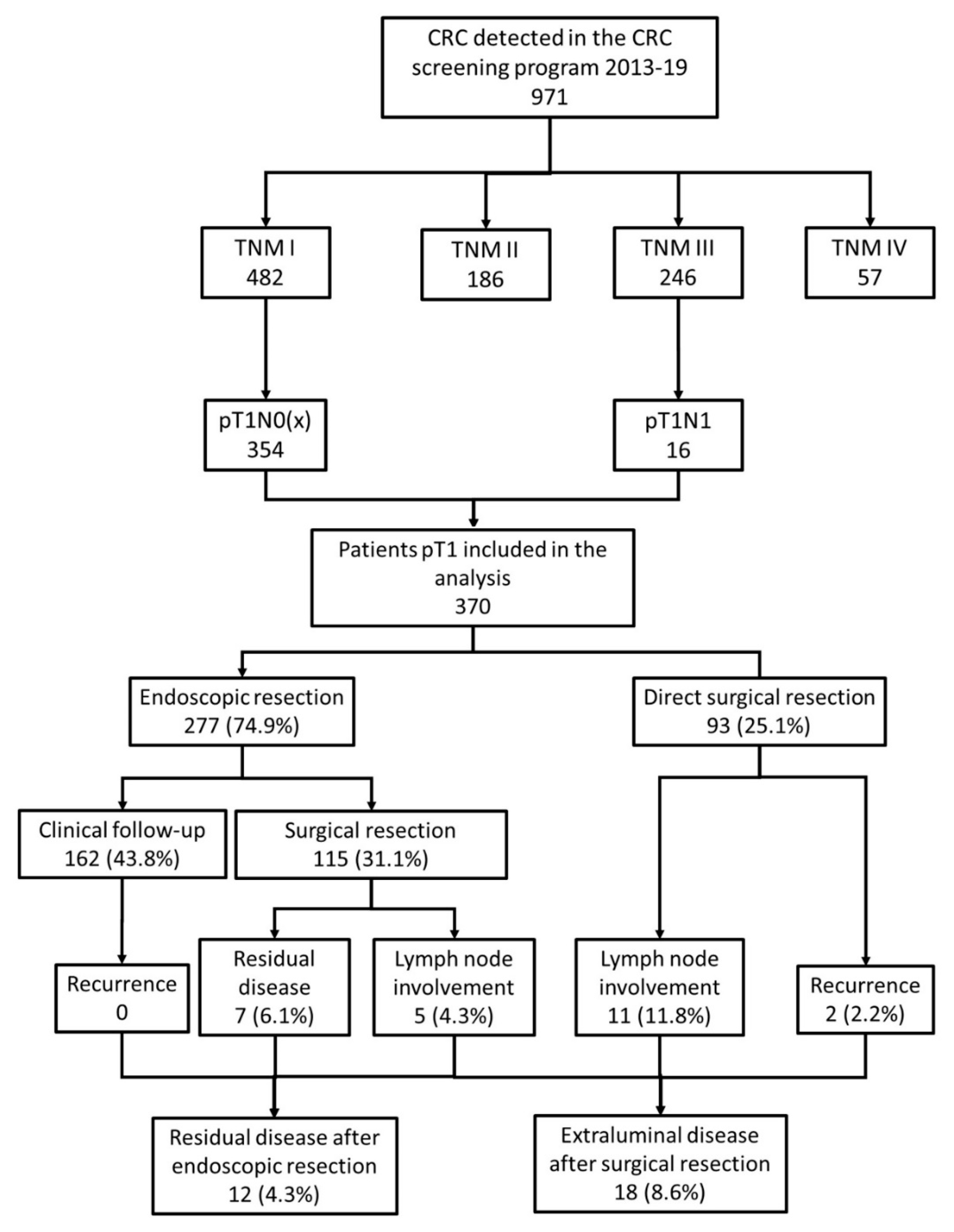
3. Results
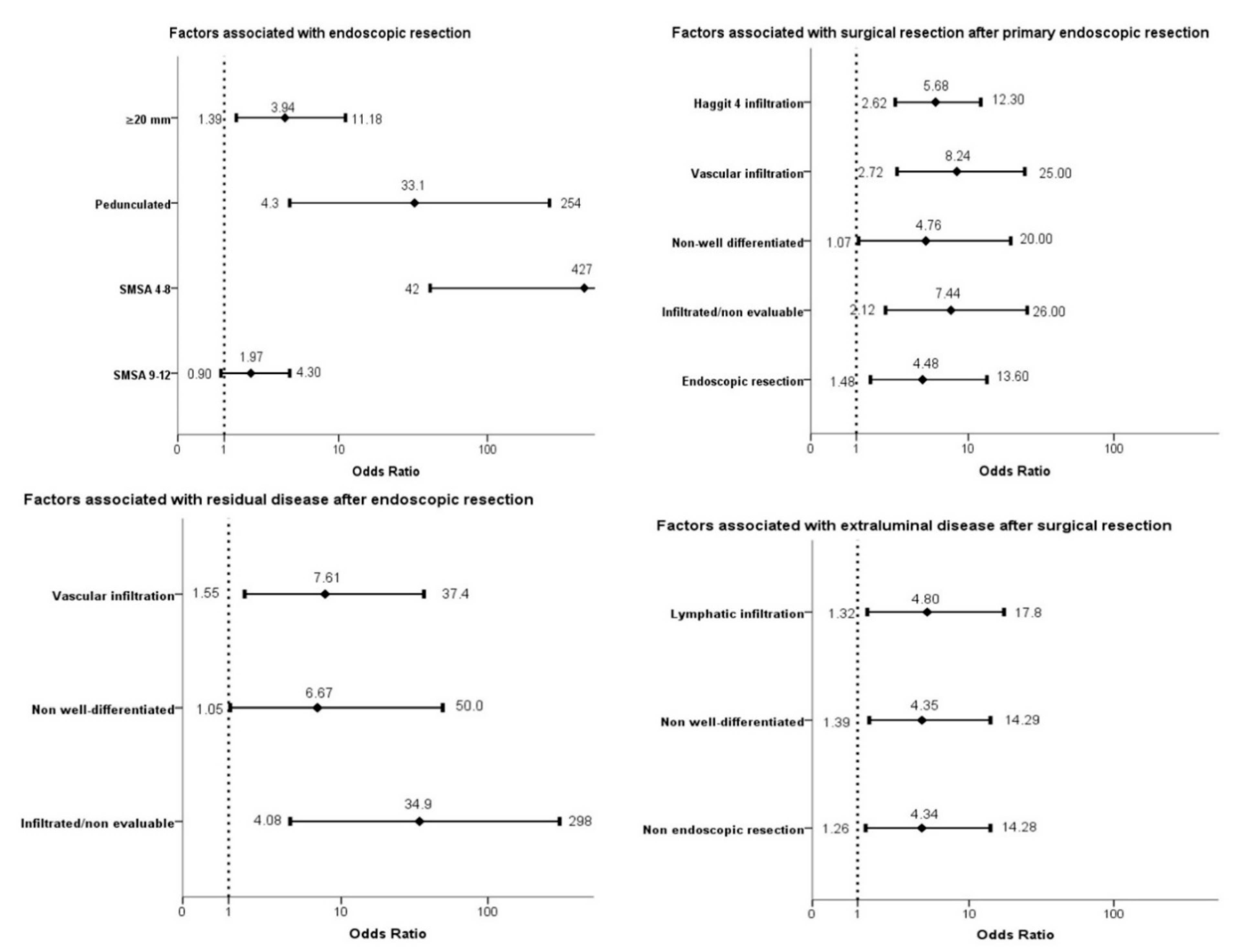
3.1. Endoscopic Resection
3.2. Surgery Rescue and Residual Disease after Endoscopic Resection
3.3. Surgery and Related Complications
3.4. Extraluminal Disease after Surgery Resection
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization Cancer Today. International Agency for Research on Cancer. Available online: https://gco.iarc.fr/today/home (accessed on 23 May 2020).
- Lin, J.S.; Piper, M.A.; Perdue, L.A.; Rutter, C.M.; Webber, E.M.; O’Connor, E.; Smith, N.; Whitlock, E.P. Screening for Colorectal Cancer: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2016, 315, 2576–2594. [Google Scholar] [CrossRef] [Green Version]
- Canadian Task Force on Preventive Health Care; Bacchus, C.M.; Dunfield, L.; Gorber, S.C.; Holmes, N.M.; Birtwhistle, R.; Dickinson, J.A.; Lewin, G.; Singh, H.; Klarenbach, S.; et al. Recommendations on screening for colorectal cancer in primary care. CMAJ 2016, 188, 340–348. [Google Scholar] [CrossRef] [Green Version]
- Cubiella, J.; Marzo-Castillejo, M.; Mascort-Roca, J.J.; Amador-Romero, F.J.; Bellas-Beceiro, B.; Clofent-Vilaplana, J.; Carballal, S.; Ferrándiz-Santos, J.; Gimeno-García, A.Z.; Jover, R.; et al. Clinical practice guideline. Diagnosis and prevention of colorectal cancer. 2018 Update. Gastroenterol. Hepatol. 2018, 41, 585–596. [Google Scholar] [CrossRef] [PubMed]
- Zorzi, M.; Fedeli, U.; Schievano, E.; Bovo, E.; Guzzinati, S.; Baracco, S.; Fedato, C.; Saugo, M.; Dei Tos, A.P. Impact on colorectal cancer mortality of screening programmes based on the faecal immunochemical test. Gut 2015, 64, 784–790. [Google Scholar] [CrossRef] [PubMed]
- Levin, T.R.; Corley, D.A.; Jensen, C.D.; Schottinger, J.E.; Quinn, V.P.; Zauber, A.G.; Lee, J.K.; Zhao, W.K.; Udaltsova, N.; Ghai, N.R.; et al. Effects of Organized Colorectal Cancer Screening on Cancer Incidence and Mortality in a Large Community-Based Population. Gastroenterology 2018, 155, 1383–1391.e5. [Google Scholar] [CrossRef] [PubMed]
- UK National Screening Committee (UK NSC) Criteria for Appraising the Viability, Effectiveness and Appropriateness of A Screening Programme Updated 23 October 2015. Available online: https://www.gov.uk/government/publications/evidence-review-criteria-national-screening-programmes/criteria-for-appraising-the-viability-effectiveness-and-appropriateness-of-a-screening-programme (accessed on 2 June 2020).
- Ferlitsch, M.; Moss, A.; Hassan, C.; Bhandari, P.; Dumonceau, J.-M.; Paspatis, G.; Jover, R.; Langner, C.; Bronzwaer, M.; Nalankilli, K.; et al. Colorectal polypectomy and endoscopic mucosal resection (EMR): European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy 2017, 49, 270–297. [Google Scholar] [CrossRef] [Green Version]
- Portillo, I.; Arana-Arri, E.; Idigoras, I.; Bilbao, I.; Martínez-Indart, L.; Bujanda, L.; Gutierrez-Ibarluzea, I. Colorectal and interval cancers of the Colorectal Cancer Screening Program in the Basque Country (Spain). World J. Gastroenterol. 2017, 23, 2731–2742. [Google Scholar] [CrossRef]
- Antonelli, G.; Vanella, G.; Orlando, D.; Angeletti, S.; Di Giulio, E. Recurrence and cancer-specific mortality after endoscopic resection of low- and high-risk pT1 colorectal cancers: A meta-analysis. Gastrointest. Endosc. 2019, 90, 559–569.e3. [Google Scholar] [CrossRef]
- The American Joint Committee on Cancer; Edge, S.B.; Byrd, D.R.; Compton, C.C.; Fritz, A.G.; Greene, F.L.; Trotti, A. (Eds.) AJCC Cancer Staging Manual, 7th ed.; Springer: Berlin/Heidelberg, Germany, 2010; ISBN 978-0-387-88440-0. [Google Scholar]
- European Colorectal Cancer Screening Guidelines Working Group; von Karsa, L.; Patnick, J.; Segnan, N.; Atkin, W.; Halloran, S.; Lansdorp-Vogelaar, I.; Malila, N.; Minozzi, S.; Moss, S.; et al. European guidelines for quality assurance in colorectal cancer screening and diagnosis: Overview and introduction to the full supplement publication. Endoscopy 2013, 45, 51–59. [Google Scholar] [CrossRef] [Green Version]
- Jover, R.; Herráiz, M.; Alarcón, O.; Brullet, E.; Bujanda, L.; Bustamante, M.; Campo, R.; Carreño, R.; Castells, A.; Cubiella, J.; et al. Clinical practice guidelines: Quality of colonoscopy in colorectal cancer screening. Endoscopy 2012, 44, 444–451. [Google Scholar] [CrossRef] [Green Version]
- Lambert, R.; Lightdale, C.J. The Paris endoscopic classification of superficial neoplastic lesions: Esophagus, stomach, and colon: November 30 to December 1, 2002. Gastrointest Endosc. 2003, 58, S3–S43. [Google Scholar]
- Sidhu, M.; Tate, D.J.; Desomer, L.; Brown, G.; Hourigan, L.F.; Lee, E.Y.T.; Moss, A.; Raftopoulos, S.; Singh, R.; Williams, S.J.; et al. The size, morphology, site, and access score predicts critical outcomes of endoscopic mucosal resection in the colon. Endoscopy 2018, 50, 684–692. [Google Scholar] [CrossRef] [Green Version]
- Clavien, P.A.; Barkun, J.; De Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; De Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The clavien-dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassan, C.; Pickhardt, P.J.; Di Giulio, E.; Hunink, M.G.M.; Zullo, A.; Nardelli, B.B. Value-of-information analysis to guide future research in the management of the colorectal malignant polyp. Dis. Colon Rectum 2010, 53, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Bosch, S.; Teerenstra, S.; De Wilt, J.W.; Cunningham, C.; Nagtegaal, I. Predicting lymph node metastasis in pT1 colorectal cancer: A systematic review of risk factors providing rationale for therapy decisions. Endoscopy 2013, 45, 827–834. [Google Scholar] [CrossRef] [Green Version]
- Vermeer, N.C.A.; Backes, Y.; Snijders, H.S.; Bastiaannet, E.; Liefers, G.J.; Moons, L.M.G.; van de Velde, C.J.H.; Peeters, K.C.M.J. National cohort study on postoperative risks after surgery for submucosal invasive colorectal cancer. BJS Open 2019, 3, 210–217. [Google Scholar] [CrossRef] [Green Version]
- Giglia, M.D.; Stein, S.L. Overlooked Long-Term Complications of Colorectal Surgery. Clin. Colon Rectal Surg. 2019, 32, 204–211. [Google Scholar] [CrossRef]
- Beaton, C.; Twine, C.P.; Williams, G.L.; Radcliffe, A.G. Systematic review and meta-analysis of histopathological factors influencing the risk of lymph node metastasis in early colorectal cancer. Color. Dis. 2013, 15, 788–797. [Google Scholar] [CrossRef]
- Mou, S.; Soetikno, R.; Shimoda, T.; Rouse, R.; Kaltenbach, T. Pathologic predictive factors for lymph node metastasis in submucosal invasive (T1) colorectal cancer: A systematic review and meta-analysis. Surg. Endosc. Other Interv. Tech. 2013, 27, 2692–2703. [Google Scholar] [CrossRef]
- Wada, H.; Shiozawa, M.; Katayama, K.; Okamoto, N.; Miyagi, Y.; Rino, Y.; Masuda, M.; Akaike, M. Systematic review and meta-analysis of histopathological predictive factors for lymph node metastasis in T1 colorectal cancer. J. Gastroenterol. 2015, 50, 727–734. [Google Scholar] [CrossRef]
- Choi, J.Y.; Jung, S.-A.; Shim, K.-N.; Cho, W.Y.; Keum, B.; Byeon, J.-S.; Huh, K.C.; Jang, B.I.; Chang, D.K.; Jung, H.-Y.; et al. Meta-analysis of predictive clinicopathologic factors for lymph node metastasis in patients with early colorectal carcinoma. J. Korean Med. Sci. 2015, 30, 398–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antonelli, G.; Berardi, G.; Rampioni Vinciguerra, G.; Brescia, A.; Ruggeri, M.; Mercantini, P.; Corleto, V.; D’Ambra, G.; Pilozzi, E.; Hassan, C.; et al. Clinical management of endoscopically resected pT1 colorectal cancer. Endosc. Int. Open 2018, 06, E1462–E1469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, S.; Miskovic, D.; Bhandari, P.; Dolwani, S.; McKaig, B.; Pullan, R.; Rembacken, B.; Riley, S.; Rutter, M.D.; Suzuki, N.; et al. A novel method for determining the difficulty of colonoscopic polypectomy. Frontline Gastroenterol. 2013, 4, 244–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Backes, Y.; de Vos Tot Nederveen Cappel, W.H.; Van Bergeijk, J.; Ter Borg, F.; Schwartz, M.P.; Spanier, B.W.M.; Geesing, J.M.J.; Kessels, K.; Kerkhof, M.; Groen, J.N.; et al. Risk for Incomplete Resection after Macroscopic Radical Endoscopic Resection of T1 Colorectal Cancer: A Multicenter Cohort Study. Am. J. Gastroenterol. 2017, 112, 785–796. [Google Scholar] [CrossRef]
- Vermeer, N.C.A.; de Neree Tot Babberich, M.P.M.; Fockens, P.; Nagtegaal, I.D.; van de Velde, C.J.H.; Dekker, E.; Tanis, P.J.; Peeters, K.C.M.J. Multicentre study of surgical referral and outcomes of patients with benign colorectal lesions. BJS Open 2019, 3, 687–695. [Google Scholar] [CrossRef] [Green Version]
- Brockmoeller, S.F.; West, N.P. Predicting systemic spread in early colorectal cancer: Can we do better? World J. Gastroenterol. 2019, 25, 2887–2897. [Google Scholar] [CrossRef]
- Puig, I.; López-Cerón, M.; Arnau, A.; Rosiñol, Ò.; Cuatrecasas, M.; Herreros-de-Tejada, A.; Ferrández, Á.; Serra-Burriel, M.; Nogales, Ó.; Vida, F.; et al. Accuracy of the Narrow-Band Imaging International Colorectal Endoscopic Classification System in Identification of Deep Invasion in Colorectal Polyps. Gastroenterology 2019, 156, 75–87. [Google Scholar] [CrossRef]
- Overwater, A.; Kessels, K.; Elias, S.G.; Backes, Y.; Spanier, B.W.M.; Seerden, T.C.J.; Pullens, H.J.M.; de Vos Tot Nederveen Cappel, W.H.; Van Den Blink, A.; Offerhaus, G.J.A.; et al. Endoscopic resection of high-risk T1 colorectal carcinoma prior to surgical resection has no adverse effect on long-term outcomes. Gut 2018, 67, 284–290. [Google Scholar] [CrossRef]
- Mangas-Sanjuan, C.; Jover, R.; Cubiella, J.; Marzo-Castillejo, M.; Balaguer, F.; Bessa, X.; Bujanda, L.; Bustamante, M.; Castells, A.; Diaz-Tasende, J.; et al. Endoscopic surveillance after colonic polyps and colorrectal cancer resection. 2018 update. Gastroenterol. Hepatol. 2019, 42, 188–201. [Google Scholar] [CrossRef]
- Senore, C.; Giovo, I.; Ribaldone, D.G.; Ciancio, A.; Cassoni, P.; Arrigoni, A.; Fracchia, M.; Silvani, M.; Segnan, N.; Saracco, G.M. Management of Pt1 tumours removed by endoscopy during colorectal cancer screening: Outcome and treatment quality indicators. Eur. J. Surg. Oncol. 2018, 44, 1873–1879. [Google Scholar] [CrossRef]
- Kaltenbach, T.; Anderson, J.C.; Burke, C.A.; Dominitz, J.A.; Gupta, S.; Lieberman, D.; Robertson, D.J.; Shaukat, A.; Syngal, S.; Rex, D.K. Endoscopic Removal of Colorectal Lesions—Recommendations by the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology 2020, 158, 1095–1129. [Google Scholar] [CrossRef] [PubMed]
- Cubiella, J.; Castells, A.; Andreu, M.; Bujanda, L.; Carballo, F.; Jover, R.; Lanas, Á.; Morillas, J.D.; Salas, D.; Quintero, E.; et al. Correlation between adenoma detection rate in colonoscopy- and fecal immunochemical testing-based colorectal cancer screening programs. United Eur. Gastroenterol. J. 2017, 5, 255–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bara, T.; Bancu, S.; Egyed, I.Z.; Gurzu, S.; Bancu, L.; Azamfirei, L.; Feher, A.M. Sentinel lymph node mapping in colorectal cancer. Chirurgia 2011, 106, 195–198. [Google Scholar]
- Suzuki, S.; Fukunaga, Y.; Tamegai, Y.; Akiyoshi, T.; Konishi, T.; Nagayama, S.; Saito, S.; Ueno, M. The short-term outcomes of laparoscopic-endoscopic cooperative surgery for colorectal tumors (LECS-CR) in cases involving endoscopically unresectable colorectal tumors. Surg. Today 2019, 49, 1051–1057. [Google Scholar] [CrossRef] [PubMed]
- Goo, J.J.; Ryu, D.G.; Kim, H.W.; Park, S.B.; Kang, D.H.; Choi, C.W.; Kim, S.J.; Nam, H.S.; Kim, H.S.; Son, G.M.; et al. Efficacy of preoperative colonoscopic tattooing with indocyanine green on lymph node harvest and factors associated with inadequate lymph node harvest in colorectal cancer. Scand. J. Gastroenterol. 2019, 54, 666–672. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables Evaluated | Endoscopic Resection (n = 277) | Direct Surgery (n = 93) | Odd Ratio (95% CI) 1 | Odd Ratio (95% CI) 2 | |
|---|---|---|---|---|---|
| Gender (n = 370) |
| 87 (76.3%) 190 (74.2%) | 27 (23.7%) 66 (25.8%) | 1 0.90 (0.53–1.50) | |
| Age (n = 370) |
| 97 (75.8%) 180 (74.4%) | 31 (24.2%) 62 (25.6%) | 1 0.93 (0.56–1.52) | |
| PS (n = 361) |
| 236 (74.7%) 39 (84.8%) | 80 (25.3%) 7 (15.2%) | 1 1.84 (0.79–4.28) | |
| ASA (n = 361) |
| 161 (71.6%) 99 (83.2%) 14 (73.7%) | 64 (28.4%) 18 (16.8%) 5 (26.3%) | 1 2.20 (1.22–3.90) 1.11 (0.38–3.21) | |
| Fecal Hb (n = 370) |
| 178 (74.2%) 99 (76.2%) | 62 (25.8%) 31 (23.8%) | 1 1.11 (0.68–1.82) | |
| N. colonoscopies (n = 346) |
| 242 (76.8%) 26 (83.9%) | 73 (23.2%) 5 (16.1%) | 1 1.56 (0.58–4.23) | |
| Lesion size (n = 370) |
| 160 (85.6%) 117 (63.9%) | 27 (14.4%) 66 (36.1%) | 1 0.30 (0.18–0.50) | 1 3.94 (1.39–11.18) |
| Morphology (n = 370) |
| 103 (53.1%) 174 (98.9%) | 91 (46.9%) 2 (1.1%) | 1 76.8 (18.5–318.6) | 1 33.1 (4.3–254) |
| Location (splenic flexure) (n = 370) |
| 21 (46.7%) 256 (78.8%) | 24 (53.3%) 69 (21.2%) | 1 4.24 (2.23–8.10) | |
| SMSA classification (n = 370) |
| 34 (45.3%) 50 (49.5%) 203 (95.5%) | 41 (54.7%) 51 (50.5%) 1 (0.5%) | 1 1.67 (0.89–3.17) 346 (46–2636) | 1 1.97 (0.90–4.30) 427 (42–4263) |
| Endoscopist ADR (n = 369) |
| 58 (65.9%) 61 (78.2%) 71 (77.2%) 87 (78.4%) | 30 (34.1%) 17 (21.8%) 21 (22.8%) 24 (21.6%) | 1 1.85 (0.93–3.72) 1.75 (0.91–3.37) 1.87 (0.99–3.52) | |
| Endoscopist number of colonoscopies (n = 369) |
| 35 (81.4%) 242 (74.2%) | 8 (18.6%) 84 (25.8%) | 1 0.66 (0.29–1.48) | |
| High-risk CRC clinic (n = 370) |
| 84 (77.8%) 193 (73.7%) | 24 (22.2%) 69 (26.3%) | 1 0.80 (0.47–1.36) | |
| Complexity of hospital (n = 370) |
| 149 (70.3%) 128 (81.0%) | 63 (29.7%) 30 (19.0%) | 1 1.80 (1.10–2.96) | |
| Variables Evaluated | Clinical Follow-up (n = 162) | Surgical Resection (n = 115) | Odd Ratio (95% CI) 1 | Odd Ratio (95% CI) 2 | |
|---|---|---|---|---|---|
| Gender (n = 277) |
| 52 (59.8%) 110 (57.9%) | 35 (40.2%) 80 (42.1%) | 1 1.08 (0.64–1.81) | |
| Age (n = 277) |
| 55 (56.7%) 107 (59.5%) | 42 (43.3%) 73 (40.5%) | 1 0.89 (0.54–1.47) | |
| Colonoscopies (n = 258) |
| 134 (57.8%) 21 (80.8%) | 98 (42.2%) 5 (19.2%) | 1 0.32 (0.12–0.89) | |
| Lesion size (n = 277) |
| 96 (60.0%) 66 (56.4%) | 64 (40.0%) 51 (43.6%) | 1 1.16 (0.72–1.88) | |
| Morphology (n = 277) |
| 36 (35.0%) 126 (72.4%) | 67 (65.0%) 48 (27.6%) | 1 0.20 (0.12–0.35) | |
| Location (splenic flexure) (n = 277) |
| 7 (33.3%) 155 (60.6%) | 14 (66.7%) 101 (39.4%) | 1 0.33 (0.13–0.83) | |
| SMSA classification (n = 277) |
| 138 (68.0%) 21 (42.0%) 3 (12.5%) | 65 (32.0%) 29 (58.0%) 21 (87.5%) | 1 2.93 (1.55–5.53) 14.8 (4.3–51.6) | |
| Endoscopic resection (n = 277) |
| 152 (68.5%) 10 (18.2%) | 70 (31.5%) 45 (81.8%) | 1 9.78 (4.66–20.5) | 1 4.48 (1.48–13.6) |
| Infiltration of the border (n = 277) |
| 154 (71.3%) 8 (13.1%) | 62 (28.7%) 53 (86.9%) | 1 16.5 (7.40–36.6) | 1 7.44 (2.12–26.0) |
| Well-differentiated (n = 277) |
| 5 (23.8%) 157 (61.4%) | 16 (76.2%) 99 (38.6%) | 5.00 (1.81–14.3) 1 | 4.76 (1.07–20.0) 1 |
| Lymphatic infiltration (n = 264) |
| 153 (61.7%) 2 (12.5%) | 95 (38.3%) 14 (87.5%) | 1 11.3 (2.51–50.7) | |
| Vascular infiltration (n = 277) |
| 153 (67.0%) 9 (26.5%) | 90 (37.0%) 25 (73.5%) | 1 4.72 (2.11–10.5) | 1 8.24 (2.72–25.0) |
| Tumor budding (n = 48) |
| 13 (61.9%) 16 (59.3%) | 8 (38.1%) 11 (40.7%) | 1 1.12 (0.35–3.6) | |
| Haggitt classification (n = 224) |
| 102 (85.6%) 34 (33.3%) | 20 (16.4%) 68 (66.7%) | 1 10.2 (5.42–19.2) | 1 5.68 (2.62–12.3) |
| High-risk pT1 CRC (n = 277) |
| 130 (76.9%) 32 (29.6%) | 39 (23.1%) 76 (70.4%) | 1 7.92 (4.58–13.6) | |
| Endoscopist ADR (n = 277) |
| 29 (50.0%) 36 (52.1%) 48 (67.6%) 49 (56.3%) | 29 (50.0%) 25 (47.9%) 23 (32.4%) 38 (43.7%) | 1 0.69 (0.34–1.43) 0.48 (0.23–0.98) 0.78 (0.40–1.51) | |
| Endoscopist number of colonoscopies (n = 277) |
| 25 (71.5%) 137 (56.6%) | 10 (28.5%) 105 (43.4%) | 1 1.92 (0.88–4.16) | |
| Complexity of hospital (n = 370) |
| 81 (54.4%) 81 (63.3%) | 68 (45.6%) 47 (36.7%) | 1 0.69 (0.42–1.12) | |
| Variables Evaluated | No Residual Disease (n = 265) | Residual Disease (n = 12) | Odd Ratio (95% CI) 1 | Odds Ratio (95% CI) 2 | |
|---|---|---|---|---|---|
| Diameter (n = 277) |
| 153 (95.6%) 112 (45.8%) | 7 (4.4%) 5 (4.2%) | 1 0.98 (0.30–3.15) | |
| Morphology (n = 277) |
| 95 (92.8%) 170 (97.7%) | 8 (7.8%) 4 (2.3%) | 1 0.28 (0.08–0.95) | |
| Location (splenic flexure) (n = 277) |
| 21 (100%) 244 (95.3%) | 0 12 (4.7%) | ||
| SMSA classification (n = 277) |
| 196 (96.5%) 47 (94.0%) 22 (91.7%) | 7 (3.5%) 3 (6.0%) 2 (8.3%) | 1 1.79 (0.44–7.17) 2.54 (0.50–13.0) | |
| Endoscopic resection (n = 277) |
| 214 (96.4%) 51 (92.7%) | 8 (3.6%) 4 (7.3%) | 1 2.10 (0.61–7.24) | |
| Infiltration of the border (n = 277) |
| 213 (98.6%) 52 (85.3%) | 3 (1.4%) 9 (14.7%) | 1 12.3 (3.21–47.0) | 1 34.9 (4.08–298) |
| Well-differentiated (n = 277) |
| 18 (85.7%) 247 (96.5%) | 3 (14.3%) 9 (3.5%) | 4.5 (1.14–20.0) 1 | 6.67 (1.05–50.0) 1 |
| Lymphatic infiltration (n = 264) |
| 240 (96.8%) 14 (87.5%) | 8 (3.2%) 2 (12.5%) | 1 4.29 (0.83–22.1) | |
| Vascular infiltration (n = 277) |
| 236 (97.1%) 29 (85.3%) | 7 (2.9%) 5 (14.7%) | 1 5.91 (1.73–19.5) | 1 7.61 (1.55–37.4) |
| Tumor budding (n = 48) |
| 21 (100%) 26 (78.8%) | 0 7 (21.2%) | ||
| Haggitt classification (n = 224) |
| 121 (91.2%) 93 (91.2%) | 1 (0.8%) 9 (8.8%) | 1 11.7 (1.46–94.1) | |
| High-risk pT1CRC (n = 277) |
| 168 (99.4%) 97 (89.8%) | 1 (0.6%) 11 (10.2%) | 1 19.0 (2.4–149) | |
| Surgery and Associated Complications | Number | |
|---|---|---|
| Surgical approach (n = 208) |
| 142 (68.3%) 15 (7.2%) 35 (16.8%) 16 (7.7%) |
| Type of surgery (n = 208) |
| 33 (15.9%) 17 (8.2%) 87 (41.8%) 45 (21.6%) 3 (1.4%) 3 (1.4%) 4 (1.9%) 16 (7.7%) |
| Length of hospitalization (days) | 7 (IQR 6–9.75) | |
| In-hospital complications (n = 208) |
| 154 (74.0%) 32 (10.6%) 18 (8.7%) 11 (5.3%) 3 (1.4%) 0 (0.0%) |
| Follow-up after discharge (months) | 25.6 (18.5–35.4) | |
| Complications after discharge (n = 208) | 34 (16.3%) | |
| Death | 11 (3.0%) | |
| Variables Evaluated | No Extraluminal Disease (n = 190) | Extraluminal Disease (n = 18) | Odd Ratio (95%CI) 1 | Odds Ratio (95% CI) 2 | |
|---|---|---|---|---|---|
| Diameter (n = 208) |
| 93 (90.3%) 97 (92.4%) | 10 (9.7%) 8 (7.6%) | 1 0.77 (0.29–2.03) | |
| Morphology (n = 208) |
| 142 (89.9%) 48 (96.0%) | 16 (10.1%) 2 (4.0%) | 1 0.37 (0.08–1.67) | |
| Location (splenic flexure) (n = 208) |
| 36 (94.7%) 154 (90.6%) | 2 (5.3%) 16 (9.4%) | 1 1.87 (0.41–8.5) | |
| SMSA classification (n = 208) |
| 61 (92.2%) 71 (88.8%) 58 (93.6%) | 5 (7.8%) 9 (11.2%) 4 (6.4%) | 1 1.55 (0.49–4.86) 0.84 (0.21–3.29) | |
| Endoscopic resection (n = 208) |
| 80 (86.0%) 110 (95.7%) | 13 (14.0%) 5 (4.3%) | 3.57 (1.22–10.0) 1 | 4.34 (1.26–14.28) 1 |
| Well-differentiated (n = 204) |
| 159 (93.5%) 27 (79.4%) | 11 (6.5%) 7 (20.6%) | 3.70 (1.35–11.11) 1 | 4.35 (1.39–14.29) 1 |
| Lymphatic infiltration (n = 193) |
| 159 (93.6%) 18 (78.3%) | 11 (6.4%) 5 (21.7%) | 1 4.01 (1.25–12.8) | 1 4.80 (1.32–17.8) |
| Vascular infiltration (n = 199) |
| 152 (93.3%) 30 (83.3%) | 11 (6.7%) 6 (16.7%) | 1 2.76 (0.95–8.05) | |
| Tumor budding (n = 65) |
| 41 (87.2%) 17 (94.4%) | 6 (12.8%) 1 (5.6%) | 1 0.40 (0.04–3.60) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cubiella, J.; González, A.; Almazán, R.; Rodríguez-Camacho, E.; Fontenla Rodiles, J.; Domínguez Ferreiro, C.; Tejido Sandoval, C.; Sánchez Gómez, C.; de Vicente Bielza, N.; Lorenzo, I.P.-R.; et al. pT1 Colorectal Cancer Detected in a Colorectal Cancer Mass Screening Program: Treatment and Factors Associated with Residual and Extraluminal Disease. Cancers 2020, 12, 2530. https://doi.org/10.3390/cancers12092530
Cubiella J, González A, Almazán R, Rodríguez-Camacho E, Fontenla Rodiles J, Domínguez Ferreiro C, Tejido Sandoval C, Sánchez Gómez C, de Vicente Bielza N, Lorenzo IP-R, et al. pT1 Colorectal Cancer Detected in a Colorectal Cancer Mass Screening Program: Treatment and Factors Associated with Residual and Extraluminal Disease. Cancers. 2020; 12(9):2530. https://doi.org/10.3390/cancers12092530
Chicago/Turabian StyleCubiella, Joaquín, Antía González, Raquel Almazán, Elena Rodríguez-Camacho, Juana Fontenla Rodiles, Carmen Domínguez Ferreiro, Coral Tejido Sandoval, Cristina Sánchez Gómez, Natalia de Vicente Bielza, Isabel Peña-Rey Lorenzo, and et al. 2020. "pT1 Colorectal Cancer Detected in a Colorectal Cancer Mass Screening Program: Treatment and Factors Associated with Residual and Extraluminal Disease" Cancers 12, no. 9: 2530. https://doi.org/10.3390/cancers12092530
APA StyleCubiella, J., González, A., Almazán, R., Rodríguez-Camacho, E., Fontenla Rodiles, J., Domínguez Ferreiro, C., Tejido Sandoval, C., Sánchez Gómez, C., de Vicente Bielza, N., Lorenzo, I. P. -R., & Zubizarreta, R. (2020). pT1 Colorectal Cancer Detected in a Colorectal Cancer Mass Screening Program: Treatment and Factors Associated with Residual and Extraluminal Disease. Cancers, 12(9), 2530. https://doi.org/10.3390/cancers12092530