Exploratory Pilot Study of Circulating Biomarkers in Metastatic Renal Cell Carcinoma

 , , , , , ,
, , , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Patient Characteristics
Study Population
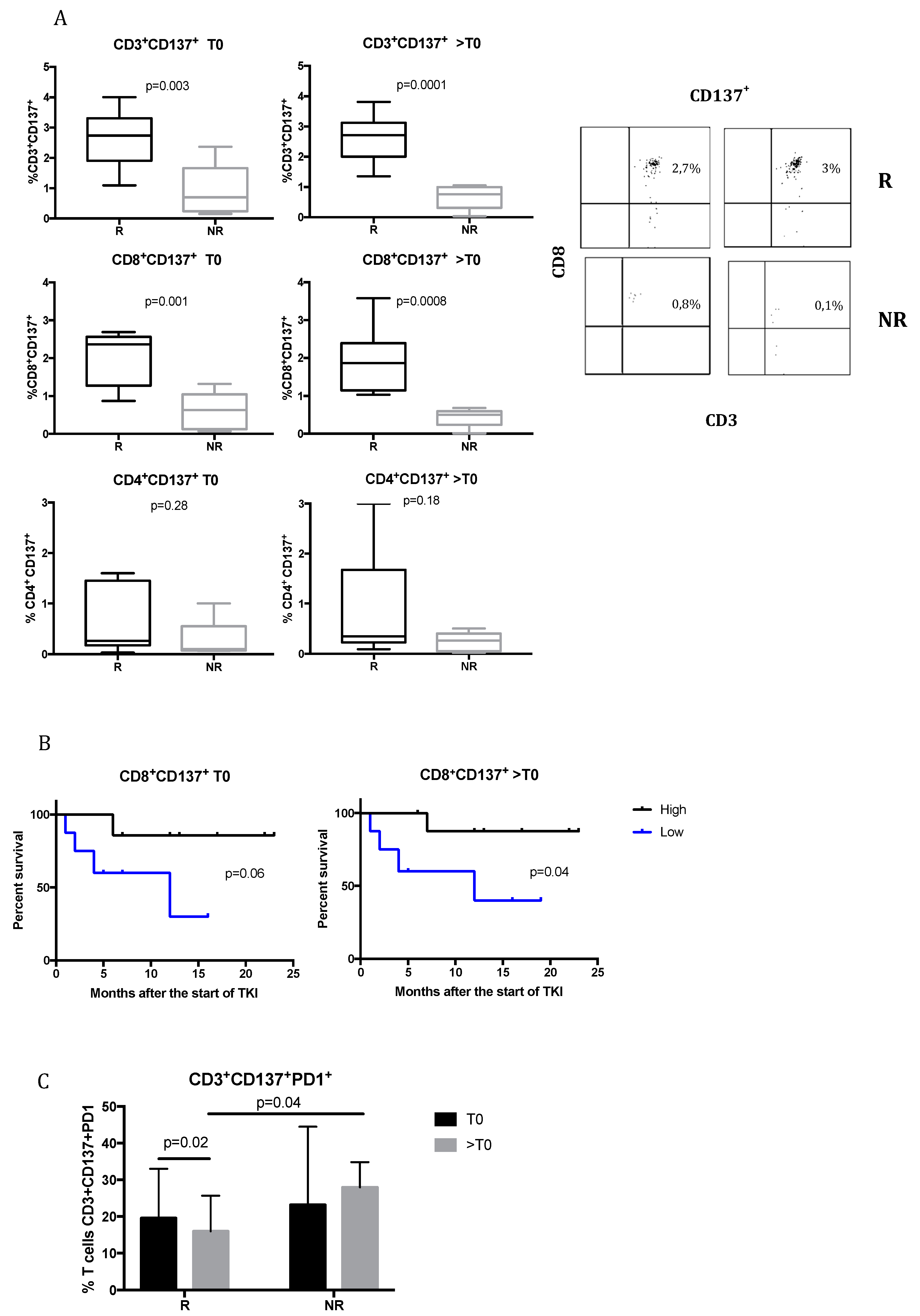
2.2. CD137+ T Cells Are Associated with the Response to TKIs in mRCC Patients
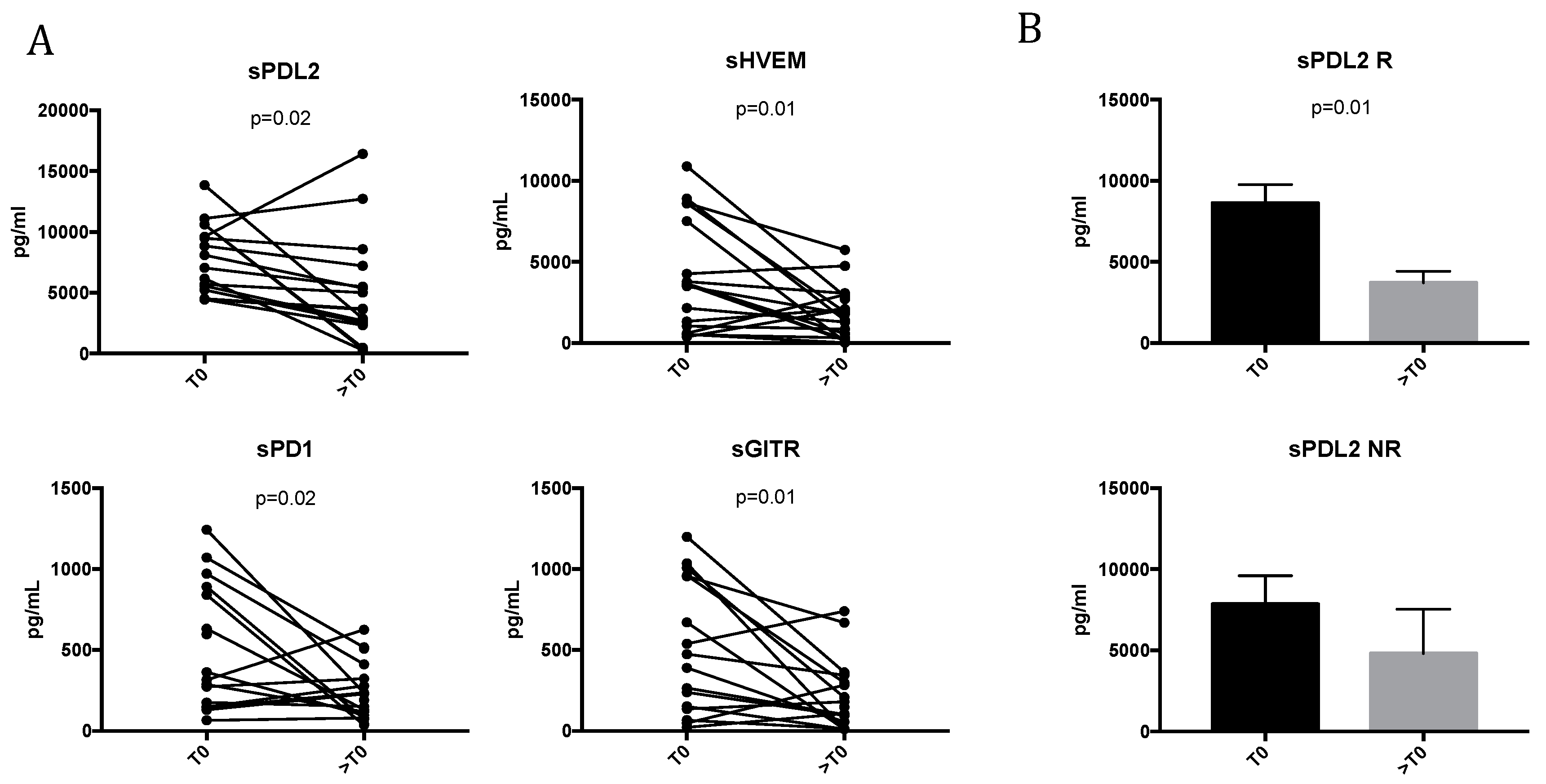
2.3. TKI Treatment Modulates Soluble Immune Molecules
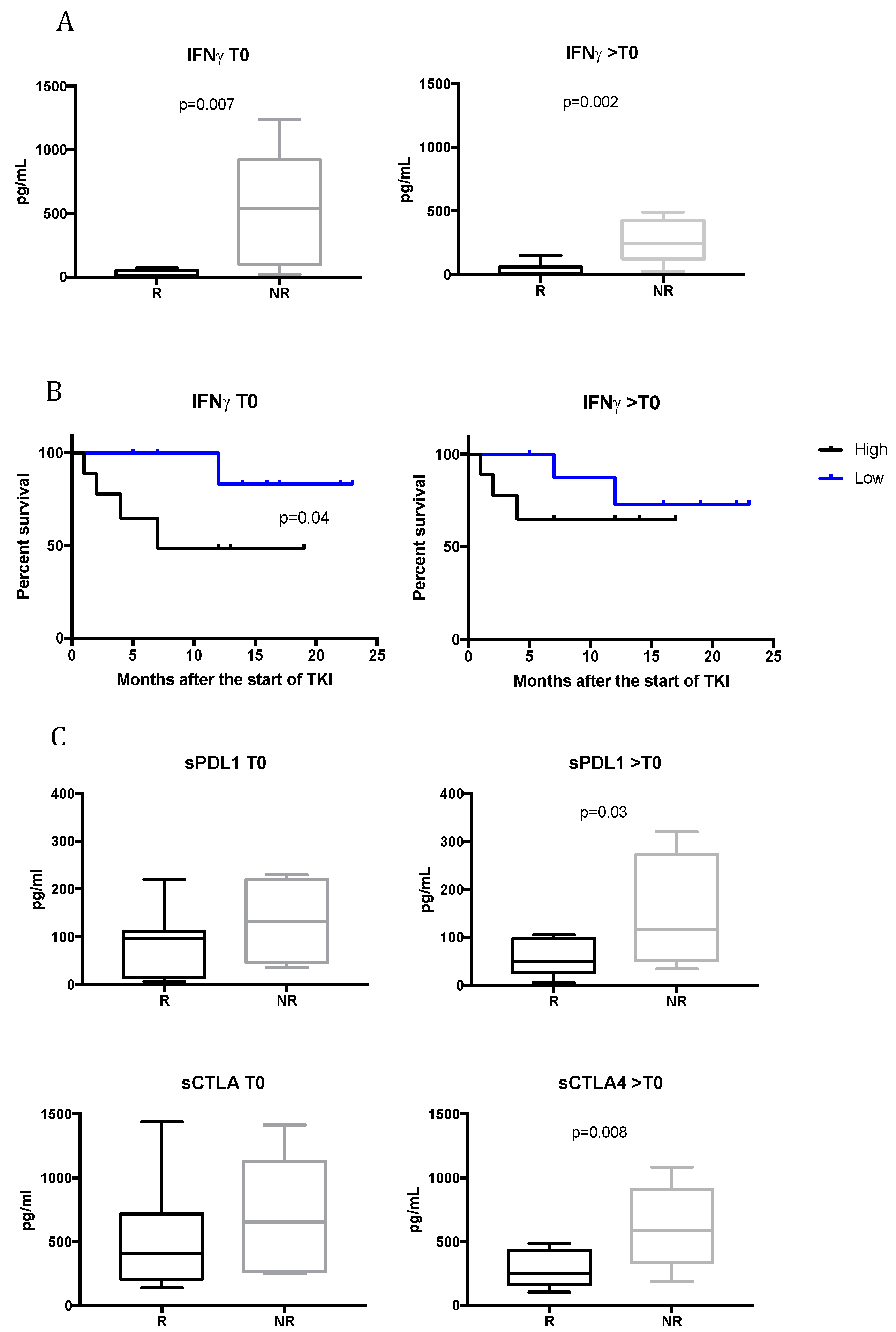
2.4. TKI Responsive Patients Have Low Levels of Serum IFNγ
2.5. Upregulation of sPDL1 and sCTLA4 in Non-Responsive Patients During TKI Treatment
3. Discussion
4. Materials and Methods
4.1. Patient Selection
4.2. PBMC (Peripheral Blood Mononuclear Cells) Purification and Sera Collection
4.3. Immune Phenotype
- T cell exhaustion/activation: Anti-CD3-APC-H7/CD8-PerCp-Cy5.5/CD137-PeCy7/PD1-PE/C TLA4-APC/Tim3-BB515;
- T regulatory cells: Anti-CD4-APC-H7/CD25-PE/CD45RA-BB515/FoxP3-Alexa647.
4.4. Inflammatory Cytokine, Chemokine and Soluble Checkpoint Inhibitor Detection
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Motzer, R.J.; Escudier, B.; Tomczak, P.; Hutson, T.E.; Michaelson, M.D.; Negrier, S.; Oudard, S.; Gore, M.E.; Tarazi, J.; Hariharan, S.; et al. Axitinib versus sorafenib as second-line treatment for advanced renal cell carcinoma: Overall survival analysis and updated results from a randomised phase 3 trial. Lancet Oncol. 2013, 14, 552–562. [Google Scholar] [CrossRef]
- Kotecha, R.R.; Motzer, R.J.; Voss, M.H. Towards individualized therapy for metastatic renal cell carcinoma. Nat. Rev. Clin. Oncol. 2019, 16, 621–633. [Google Scholar] [CrossRef] [PubMed]
- Grivennikov, S.I.; Greten, F.R.; Karin, M. Immunity, inflammation, and cancer. Cell 2010, 140, 883–899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santoni, M.; Pantano, F.; Amantini, C.; Nabissi, M.; Conti, A.; Burattini, L.; Zoccoli, A.; Berardi, R.; Santoni, G.; Tonini, G.; et al. Emerging strategies to overcome the resistance to current mTOR inhibitors in renal cell carcinoma. Biochim. Biophys. Acta Rev. Cancer 2014, 1845, 221–231. [Google Scholar] [CrossRef]
- Gustafson, M.P.; Lin, Y.; Bleeker, J.S.; Warad, D.; Tollefson, M.K.; Crispen, P.L.; Bulur, P.A.; Harrington, S.M.; Laborde, R.R.; Gastineau, D.A.; et al. Intratumoral CD14+ cells and circulating CD14+HLA-DRlo/neg monocytes correlate with decreased survival in patients with clear cell renal cell carcinoma. Clin. Cancer Res. 2015, 21, 4224–4233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirsch, L.; Flippot, R.; Escudier, B.; Albiges, L. Immunomodulatory Roles of VEGF Pathway Inhibitors in Renal Cell Carcinoma. Drugs 2020, 80, 1169–1181. [Google Scholar] [CrossRef]
- Rassy, E.; Flippot, R.; Albiges, L. Tyrosine kinase inhibitors and immunotherapy combinations in renal cell carcinoma. Ther. Adv. Med. Oncol. 2020, 12. [Google Scholar] [CrossRef] [Green Version]
- Alfaro, C.; Suarez, N.; Gonzalez, A.; Solano, S.; Erro, L.; Dubrot, J.; Palazon, A.; Hervas-Stubbs, S.; Gurpide, A.; Lopez-Picazo, J.M.; et al. Influence of bevacizumab, sunitinib and sorafenib as single agents or in combination on the inhibitory effects of VEGF on human dendritic cell differentiation from monocytes. Br. J. Cancer 2009, 100, 1111–1119. [Google Scholar] [CrossRef]
- Napoletano, C.; Ruscito, I.; Bellati, F.; Zizzari, I.G.; Rahimi, H.; Gasparri, M.L.; Antonilli, M.; Panici, P.B.; Rughetti, A.; Nuti, M. Bevacizumab-based chemotherapy triggers immunological effects in responding multi-treated recurrent ovarian cancer patients by favoring the recruitment of effector T cell subsets. J. Clin. Med. 2019, 8, 380. [Google Scholar] [CrossRef] [Green Version]
- Zizzari, I.G.; Napoletano, C.; Botticelli, A.; Caponnetto, S.; Calabrò, F.; Gelibter, A.; Rughetti, A.; Ruscito, I.; Rahimi, H.; Rossi, E.; et al. TK inhibitor pazopanib primes DCs by downregulation of the β-catenin pathway. Cancer Immunol. Res. 2018, 6, 711–722. [Google Scholar] [CrossRef] [Green Version]
- Draghiciu, O.; Nijman, H.W.; Hoogeboom, B.N.; Meijerhof, T.; Daemen, T. Sunitinib depletes myeloid-derived suppressor cells and synergizes with a cancer vaccine to enhance antigen-specific immune responses and tumor eradication. Oncoimmunology 2015, 4, e989764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adotevi, O.; Pere, H.; Ravel, P.; Haicheur, N.; Badoual, C.; Merillon, N.; Medioni, J.; Peyrard, S.; Roncelin, S.; Verkarre, V.; et al. A decrease of regulatory T cells correlates with overall survival after sunitinib-based antiangiogenic therapy in metastatic renal cancer patients. J. Immunother. 2010, 33, 991–998. [Google Scholar] [CrossRef] [PubMed]
- Gu, D.; Ao, X.; Yang, Y.; Chen, Z.; Xu, X. Soluble immune checkpoints in cancer: Production, function and biological significance. J. Immunotherap. Cancer 2018, 6, 132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daassi, D.; Mahoney, K.M.; Freeman, G.J. The importance of exosomal PDL1 in tumour immune evasion. Nat. Rev. Immunol. 2020, 20, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Dong, M.P.; Enomoto, M.; Thuy, L.T.T.; Hai, H.; Hieu, V.N.; Hoang, D.V.; Iida-Ueno, A.; Odagiri, N.; Amano-Teranishi, Y.; Hagihara, A.; et al. Clinical significance of circulating soluble immune checkpoint proteins in sorafenib-treated patients with advanced hepatocellular carcinoma. Sci. Rep. 2020, 10, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Melero, I.; Murillo, O.; Dubrot, J.; Hervás-Stubbs, S.; Perez-Gracia, J.L. Multi-layered action mechanisms of CD137 (4-1BB)-targeted immunotherapies. Trends Pharmacol. Sci. 2008, 29, 383–390. [Google Scholar] [CrossRef]
- Dahal, L.N.; Schwarz, H.; Ward, F.J. Hiding in plain sight: Soluble immunomodulatory receptors. Trends Immunol. 2018, 39, 771–774. [Google Scholar] [CrossRef]
- Heo, S.K.; Ju, S.A.; Kim, G.Y.; Park, S.M.; Back, S.H.; Park, N.H.; Min, Y.J.; An, W.G.; Thi Nguyen, T.H.; Kim, S.M.; et al. The presence of high level soluble herpes virus entry mediator in sera of gastric cancer patients. Exp. Mol. Med. 2012, 44, 149–158. [Google Scholar] [CrossRef]
- Wang, Q.; Zhang, J.; Tu, H.; Liang, D.; Chang, D.W.; Ye, Y.; Wu, X. Soluble immune checkpoint-related proteins as predictors of tumor recurrence, survival, and T cell phenotypes in clear cell renal cell carcinoma patients. J. Immunotherap. Cancer 2019, 7, 334. [Google Scholar] [CrossRef]
- Zaidi, M.R. The interferon-gamma paradox in cancer. J. Interferon Cytokine Res. 2019, 39, 30–38. [Google Scholar] [CrossRef]
- D’Aniello, C.; Berretta, M.; Cavaliere, C.; Rossetti, S.; Facchini, B.A.; Iovane, G.; Mollo, G.; Capasso, M.; Della Pepa, C.; Pesce, L.; et al. Biomarkers of prognosis and efficacy of anti-angiogenic therapy in metastatic clear cell renal cancer. Front. Oncol. 2019, 9, 1400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nuti, M.; Zizzari, I.G.; Botticelli, A.; Rughetti, A.; Marchetti, P. The ambitious role of anti angiogenesis molecules: Turning a cold tumor into a hot one. Cancer Treat. Rev. 2018, 70, 41–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rijnders, M.; de Wit, R.; Boormans, J.L.; Lolkema, M.P.J.; van der Veldt, A.A.M. Systematic review of immune checkpoint inhibition in urological cancers. Eur. Urol. 2017, 72, 411–423. [Google Scholar] [CrossRef]
- Nong, J.; Wang, J.; Gao, X.; Zhang, Q.; Yang, B.; Yan, Z.; Wang, X.; Yi, L.; Wang, Q.; Gao, Y.; et al. Circulating CD137 + CD8 + T cells accumulate along with increased functional regulatory T cells and thoracic tumour burden in lung cancer patients. Scand. J. Immunol. 2019, 89, e12765. [Google Scholar] [CrossRef]
- Perez-Ruiz, E.; Etxeberria, I.; Rodriguez-Ruiz, M.E.; Melero, I. Anti-CD137 and PD1/PD-L1 antibodies en route toward clinical synergy. Clin. Cancer Res. 2017, 23, 5326–5328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shuford, W.W.; Klussman, K.; Tritchler, D.D.; Loo, D.T.; Chalupny, J.; Siadak, A.W.; Brown, T.J.; Emswiler, J.; Raecho, H.; Larsen, C.P.; et al. 4-1BB costimulatory signals preferentially induce CD8+ T cell proliferation and lead to the amplification in vivo of cytotoxic T cell responses. J. Exp. Med. 1997, 186, 47–55. [Google Scholar] [CrossRef]
- Seo, S.K.; Choi, J.H.; Kim, Y.H.; Kang, W.J.; Park, H.Y.; Suh, J.H.; Choi, B.K.; Vinay, D.S.; Kwon, B.S. 4-1BB-mediated immunotherapy of rheumatoid arthritis. Nat. Med. 2004, 10, 1088–1094. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, C.; Mittler, R.S.; Vella, A.T. Cutting edge: 4-1BB is a bona fide CD8 T cell survival signal. J. Immunol. 1999, 162, 5037–5040. [Google Scholar]
- Agarwal, A.; Newell, K.A. The role of positive costimulatory molecules in transplantation and tolerance. Curr. Opin. Organ Transplant. 2008, 13, 366–372. [Google Scholar] [CrossRef]
- Vinay, D.S.; Kwon, B.S. 4-1BB (CD137), an inducible costimulatory receptor, as a specific target for cancer therapy. BMB Rep. 2014, 47, 122–129. [Google Scholar] [CrossRef] [Green Version]
- Choi, B.K.; Lee, S.C.; Lee, M.J.; Kim, Y.H.; Kim, Y.W.; Ryu, K.W.; Lee, J.H.; Shin, S.M.; Lee, S.H.; Suzuki, S.; et al. 4-1BB-based isolation and expansion of CD8+ T cells specific for self-tumor and non-self-tumor antigens for adoptive T-cell therapy. J. Immunother. 2014, 37, 225–236. [Google Scholar] [CrossRef]
- Wolfl, M.; Kuball, J.; Ho, W.Y.; Nguyen, H.; Manley, T.J.; Bleakley, M.; Greenberg, P.D. Activation-induced expression of CD137 permits detection, isolation, and expansion of the full repertoire of CD8+ T cells responding to antigen without requiring knowledge of epitope specificities. Blood 2007, 110, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Freeman, Z.T.; Nirschl, T.R.; Hovelson, D.H.; Johnston, R.J.; Engelhardt, J.J.; Selby, M.J.; Kochel, C.M.; Lan, R.Y.; Zhai, J.Y.; Ghasemzadeh, A.; et al. A conserved intratumoral regulatory T cell signature identifies 4-1BB as a pan-cancer target. J. Clin. Investig. 2020, 130, 1405–1416. [Google Scholar] [CrossRef]
- Azpilikueta, A.; Agorreta, J.; Labiano, S.; Pérez-Gracia, J.L.; Sánchez-Paulete, A.R.; Aznar, M.A.; Ajona, D.; Gil-Bazo, I.; Larrayoz, M.; Teijeira, A.; et al. Successful immunotherapy against a transplantable mouse squamous lung carcinoma with anti-PD1 and anti-CD137 monoclonal antibodies. J. Thorac. Oncol. 2016, 11, 524–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bian, B.; Fanale, D.; Dusetti, N.; Roque, J.; Pastor, S.; Chretien, A.S.; Incorvaia, L.; Russo, A.; Olive, D.; Iovanna, J. Prognostic significance of circulating PD1, PD-L1, pan-BTN3As, BTN3A1 and BTLA in patients with pancreatic adenocarcinoma. Oncoimmunology 2019, 8, e1561120. [Google Scholar] [CrossRef] [Green Version]
- Finke, J.H.; Rini, B.; Ireland, J.; Rayman, P.; Richmond, A.; Golshayan, A.; Wood, L.; Elson, P.; Garcia, J.; Dreicer, R.; et al. Sunitinib reverses type-1 immune suppression and decreases T-regulatory cells in renal cell carcinoma patients. Clin. Cancer Res. 2008, 14, 6674–6682. [Google Scholar] [CrossRef] [Green Version]
- Yuan, H.; Cai, P.; Li, Q.; Wang, W.; Sun, Y.; Xu, Q.; Gu, Y. Axitinib augments antitumor activity in renal cell carcinoma via STAT3-dependent reversal of myeloid-derived suppressor cell accumulation. Biomed. Pharmacother. 2014, 68, 751–756. [Google Scholar] [CrossRef]
- Hipp, M.M.; Hilf, N.; Walter, S.; Werth, D.; Brauer, K.M.; Radsak, M.P.; Weinschenk, T.; Singh-Jasuja, H.; Brossart, P. Sorafenib, but not sunitinib, affects function of dendritic cells and induction of primary immune responses. Blood 2008, 111, 5610–5620. [Google Scholar] [CrossRef] [Green Version]
- Shin, S.J.; Jeon, Y.K.; Kim, P.J.; Cho, Y.M.; Koh, J.; Chung, D.H.; Go, H. Clinicopathologic analysis of PD-L1 and PD-L2 expression in renal cell carcinoma: Association with oncogenic proteins status. Ann. Surg. Oncol. 2016, 23, 694–702. [Google Scholar] [CrossRef]
- Enblad, G.; Karlsson, H.; Gammelgård, G.; Wenthe, J.; Lövgren, T.; Amini, R.M.; Wikstrom, K.I.; Essand, M.; Savoldo, B.; Hallböök, H.; et al. A phase I/IIa trial using CD19-targeted third-generation CAR T cells for lymphoma and leukemia. Clin. Cancer Res. 2018, 24, 6185–6194. [Google Scholar] [CrossRef] [Green Version]
- Mojic, M.; Takeda, K.; Hayakawa, Y. The dark side of IFN-γ: Its role in promoting cancer immunoevasion. Int. J. Mol. Sci. 2018, 19, 89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Diaz, A.; Shin, D.S.; Moreno, B.H.; Saco, J.; Escuin-Ordinas, H.; Rodriguez, G.A.; Zaretsky, J.M.; Sun, L.; Hugo, W.; Wang, X.; et al. Interferon receptor signaling pathways regulating PD-L1 and PD-L2 expression. Cell Rep. 2017, 19, 1189–1201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayers, M.; Ribas, A.; Mcclanahan, T.K. IFN-g g-related mRNA profile predicts clinical response to PD1 blockade The Journal of Clinical Investigation. J. Clin. Investig. 2017, 127, 2930–2940. [Google Scholar] [CrossRef] [PubMed]
- Abiko, K.; Matsumura, N.; Hamanishi, J.; Horikawa, N.; Murakami, R.; Yamaguchi, K.; Yoshioka, Y.; Baba, T.; Konishi, I.; Mandai, M. IFN-γ from lymphocytes induces PD-L1 expression and promotes progression of ovarian cancer. Br. J. Cancer 2015, 112, 1501–1509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellucci, R.; Martin, A.; Bommarito, D.; Wang, K.; Hansen, S.H.; Freeman, G.J.; Ritz, J. Interferon-γ-induced activation of JAK1 and JAK2 suppresses tumor cell susceptibility to NK cells through upregulation of PD-L1 expression. Oncoimmunology 2015, 4. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Huang, A.C.; Zhang, W.; Zhang, G.; Wu, M.; Xu, W.; Yu, Z.; Yang, J.; Wang, B.; Sun, H.; et al. Exosomal PD-L1 contributes to immunosuppression and is associated with anti-PD1 response. Nature 2018, 560, 382–386. [Google Scholar] [CrossRef]
- Chen, Y.; Li, M.; Liu, J.; Pan, T.; Zhou, T.; Liu, Z.; Tan, R.; Wang, X.; Tian, L.; Chen, E.; et al. sPD-L1 expression is associated with immunosuppression and infectious complications in patients with acute pancreatitis. Scand. J. Immunol. 2017, 86, 100–106. [Google Scholar] [CrossRef] [Green Version]
- Fukuda, T.; Kamai, T.; Masuda, A.; Nukui, A.; Abe, H.; Arai, K.; Yoshida, K.I. Higher preoperative serum levels of PD-L1 and B7-H4 are associated with invasive and metastatic potential and predictable for poor response to VEGF-targeted therapy and unfavorable prognosis of renal cell carcinoma. Cancer Med. 2016, 5, 1810–1820. [Google Scholar] [CrossRef] [Green Version]
- Sharma, P.; Hu-Lieskovan, S.; Wargo, J.A.; Ribas, A. Primary, adaptive, and acquired resistance to cancer immunotherapy. Cell 2017, 168, 707–723. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | All Patients (N = 20) (100%) |
|---|---|
| Age (years) | 56.5 |
| Median Age (range) | (36–78) |
| Gender | |
| Male | 15 (75) |
| Female | 5 (25) |
| Risk Factors | 9 |
| Smoking history (SH) | (45) |
| Histology | |
| Clear cell carcinoma | 16 (80) |
| Other | 4 (20) |
| Fuhrman grading | |
| G2 | 7 (35) |
| G3 | 9 (45) |
| Unknown | 4 (20) |
| Metastatic site at diagnosis | |
| Liver | 4 (20) |
| Nodal | 8 (40) |
| Lung | 12 (60) |
| Bone | 5 (25) |
| Brain | 3 (15) |
| Adrenal | 1 (5) |
| IMDC score | |
| Poor risk | 5 (25) |
| Intermediate | 10 (50) |
| Good risk | 5 (25) |
| I-line treatment | 20 |
| Sunitinib | 8 (40) |
| Pazopanib | 12 (60) |
| II-line treatment | 10 (50) |
| Nivolumab | 10 (100) |
| III-line treatment | 2 |
| Cabozantinib | 2 |
| mRCC Patients | Baseline | During TKI Treatment |
|---|---|---|
| Responsive patients | High CD3+CD8+CD137+ Low PD1 on CD137+ T cells Low IFNγ | High CD3+CD8+CD137+ Low IFNγ Low sPDL2 |
| Non-responsive patients | Low CD3+CD8+CD137+ High IFNγ | Low CD3+CD8+CD137+ High PD1 on CD137 T cells High IFNγ High sPDL1 High sCTLA4 |
| sICs modulated by TKI | sPDL2, sHVEM, sPD1, sGITR | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zizzari, I.G.; Napoletano, C.; Di Filippo, A.; Botticelli, A.; Gelibter, A.; Calabrò, F.; Rossi, E.; Schinzari, G.; Urbano, F.; Pomati, G.; et al. Exploratory Pilot Study of Circulating Biomarkers in Metastatic Renal Cell Carcinoma. Cancers 2020, 12, 2620. https://doi.org/10.3390/cancers12092620
Zizzari IG, Napoletano C, Di Filippo A, Botticelli A, Gelibter A, Calabrò F, Rossi E, Schinzari G, Urbano F, Pomati G, et al. Exploratory Pilot Study of Circulating Biomarkers in Metastatic Renal Cell Carcinoma. Cancers. 2020; 12(9):2620. https://doi.org/10.3390/cancers12092620
Chicago/Turabian StyleZizzari, Ilaria Grazia, Chiara Napoletano, Alessandra Di Filippo, Andrea Botticelli, Alain Gelibter, Fabio Calabrò, Ernesto Rossi, Giovanni Schinzari, Federica Urbano, Giulia Pomati, and et al. 2020. "Exploratory Pilot Study of Circulating Biomarkers in Metastatic Renal Cell Carcinoma" Cancers 12, no. 9: 2620. https://doi.org/10.3390/cancers12092620
APA StyleZizzari, I. G., Napoletano, C., Di Filippo, A., Botticelli, A., Gelibter, A., Calabrò, F., Rossi, E., Schinzari, G., Urbano, F., Pomati, G., Scagnoli, S., Rughetti, A., Caponnetto, S., Marchetti, P., & Nuti, M. (2020). Exploratory Pilot Study of Circulating Biomarkers in Metastatic Renal Cell Carcinoma. Cancers, 12(9), 2620. https://doi.org/10.3390/cancers12092620