
Socio-Economic Deprivation and Symptom Burden in UK Hospice Patients with Advanced Cancer—Findings from a Longitudinal Study


Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
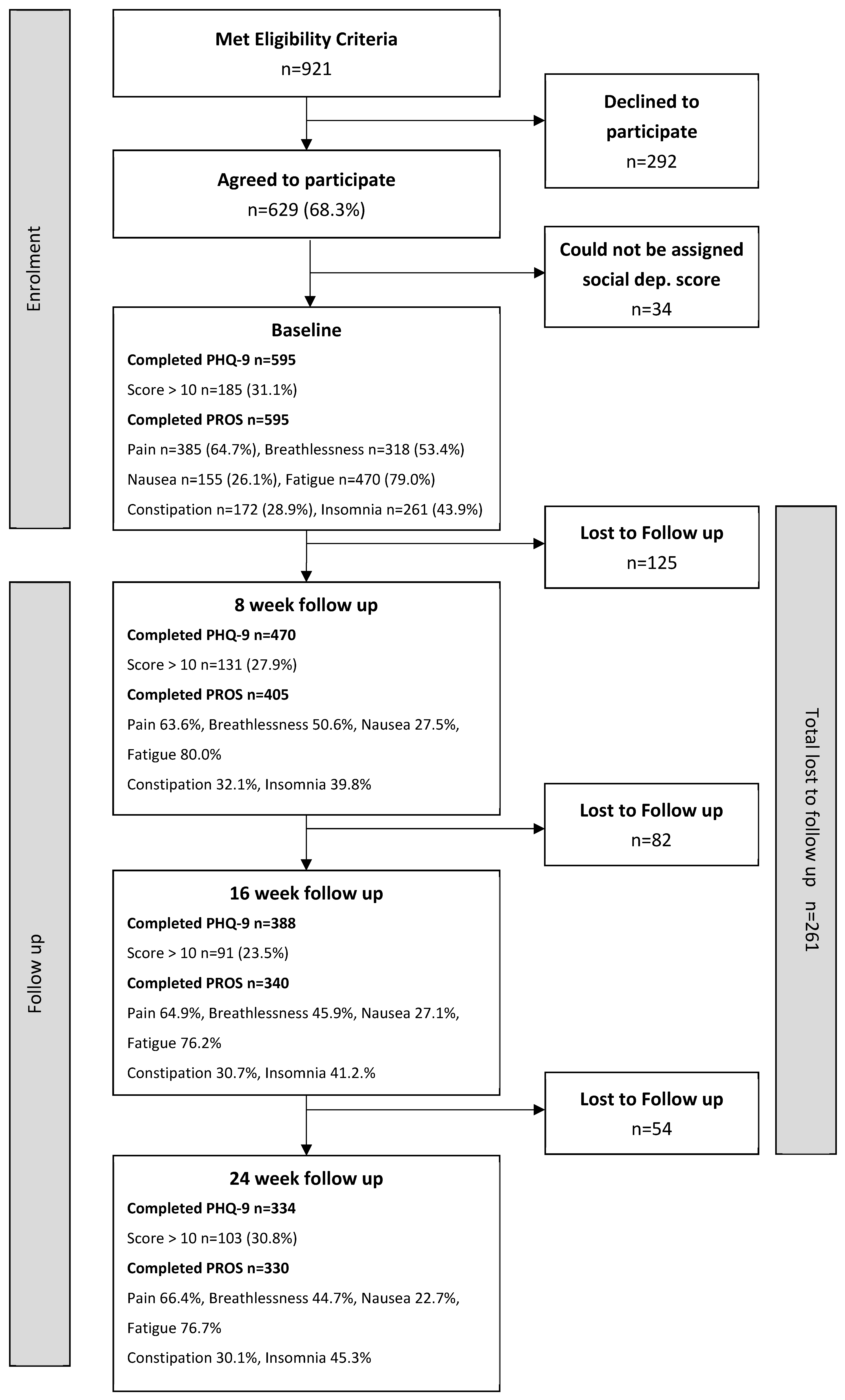
2.1. Recruitment
2.2. Information Collected in the Baseline Interview
2.3. Postcode and the Index of Multiple Deprivation Score
2.4. Psychological and Physical Health Outcomes
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Patients in This Study
3.2. Patients Reporting Being a Depression Case
3.3. Patients Reporting Physical Health Symptoms
3.4. Socio-Economic Deprivation, Patient Characteristics and Health Outcomes
3.5. Socio-Economic Deprivation and Survival
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Forbes, L.; Warburton, F.; Richards, M.; Ramirez, A. Risk factors for delay in symptomatic presentation: A survey of cancer patients. Br. J. Cancer 2014, 111, 581–588. [Google Scholar] [CrossRef]
- Davis, L.; Coburn, N.; Hallet, J.; Earle, C.; Liu, Y.; Myrehaug, S.; Mahar, A. Material deprivation and access to cancer care in a universal health care system. Cancer 2020, 126, 4545–4555. [Google Scholar] [CrossRef]
- Lewis, J.; DiGiacomo, M.; Currow, D.; Davidson, P. Dying in the Margins: Understanding Palliative Care and Socioeconomic Deprivation in the Developed World. J. Pain Symptom Manag. 2011, 42, 105–118. [Google Scholar] [CrossRef] [PubMed]
- Burt, J.; Plant, H.; Omar, R.; Raine, R. Equity of use of specialist palliative care by age: Cross sectional study of lung cancer patients. Palliat. Med. 2010, 24, 641–650. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.; Sleeman, K.; Leniz, J.; Wilson, R.; Higginson, I.; Verne, J.; Maddocks, M.; Murtagh, F. Socioeconomic position and use of healthcare in the last year of life: A systematic review and meta-analysis. PLoS ONE 2019. [Google Scholar] [CrossRef]
- Mondor, L.; Wodchis, W.; Tanuseputro, P. Persistent socioeconomic inequalities in location of death and receipt of palliative care: A population-based cohort study. Palliat. Med. 2020, 34, 1393–1401. [Google Scholar] [CrossRef]
- Grande, G.E.; Addington-Hall, J.M.; Todd, C.J. Place of death and access to home care services: Are certain patient groups at a disadvantage? Soc. Sci. Med. 1998, 47, 565–579. [Google Scholar] [CrossRef]
- Higginson, I.J.; Jarman, B.; Astin, P.; Dolan, S. Do social factors affect where patients die: An analysis of 10 years of cancer deaths in England. J. Public Health Med. 1999, 21, 22–28. [Google Scholar] [CrossRef] [Green Version]
- Campbell, M.; Grande, G.; Wilson, C.; Caress, A.L.; Roberts, D. Exploring differences in referrals to a hospice at home service in two socio-economically distinct areas of Manchester, UK. Palliat. Med. 2010, 24, 403–409. [Google Scholar] [CrossRef]
- Macfarlane, M.; Carduff, E. Does place of death vary by deprivation for patients known to specialist palliative care services ? BMJ Support. Pall. Care 2016, 8, 428–430. [Google Scholar] [CrossRef]
- ONS National Survey of Bereaved People (VOICES) 2012, NHS England. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/healthcaresystem/bulletins/nationalsurveyofbereavedpeoplevoices/2014-03-06 (accessed on 8 May 2021).
- ONS National Survey of Bereaved People 2015, NHS England. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/healthcaresystem/bulletins/nationalsurveyofbereavedpeoplevoices/england2015 (accessed on 8 April 2021).
- Currow, D.C.; Allingham, S.; Bird, S.; Yates, P.; Lewis, J.; Dawber, J.; Eagar, K. Referral patterns and proximity to palliative care inpatient services by level of socio-economic disadvantage. A national study using spatial analysis. BMC Health Serv. Res. 2012, 12, 424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malhotra, C.; Harding, R.; Teo, I.; Ozdemir, S.; Koh, G.; Neo, P.; Lee, L.; Kanesvaran, R.; Finkelstein, E. COMPASS Study team Financial difficulties are associated with greater total pain and suffering among patients with advanced cancer: Results from the COMPASS study. Support. Care Cancer 2000, 28, 3781–3789. [Google Scholar] [CrossRef]
- Sleeman, K.; Davies, J.; Verne, J.; Gao, W.; Higginson, I. The changing demographics of inpatient hospice death: Population-based, cross-sectional study in England, 1993–2012. Lancet 2015, 385 (Suppl. 1). [Google Scholar] [CrossRef]
- Ziwary, S.R.; Samad, D.; Johnson, C.D.; Edwards, R.T. Impact of place of residence on place of death in Wales: An observational study. BMC Palliat. Care. 2017, 16, 72. [Google Scholar] [CrossRef] [Green Version]
- Dixon, J.; King, D.; Matosevic, T.; Clark, M.; Knapp, M. Equity in Provision of Palliative Care in the UK: Review of Evidence; Report PSSU; London School of Economics (LSE): England, UK, 2015. [Google Scholar]
- Burt, J. Back to basics: Researching equity in palliative care. Palliat. Med. 2012, 26, 5–6. [Google Scholar] [CrossRef] [PubMed]
- Lloyd-Williams, M.; Payne, S.; Reeve, J.; Dona, R.K. Thoughts of self-harm and depression as prognostic factors in palliative care patients. J. Affect. Disord. 2014, 166, 324–329. [Google Scholar] [CrossRef]
- Lloyd-Williams, M.; Payne, S.; Reeve, J.; Kolamunnage Dona, R. Antidepressant medication in patients with advanced cancer--an observational study. QJM 2013, 106, 995–1001. [Google Scholar] [CrossRef] [Green Version]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, R.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Index of Multiple Deprivation for England; Her Majesty’s Service Government (HMS Gov): London, England, 2015.
- Spitzer, R.L.; Kroenke, K.; Williams, J.P. The Patient Health Questionnaire Primary Care Study Group. Validation and utility of a self-report version of PRIME-MD. JAMA 1999, 282, 1737–1744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ell, K.; Xie, B.; Quon, B.; Quinn, D.I.; Dwight-Johnson, M.; Lee, P.-J. Randomized controlled trial of collaborative care management of depression among low-income patients with cancer. J. Clin. l Oncol. 2008, 26, 4488–4496. [Google Scholar] [CrossRef] [Green Version]
- Lorant, V.; Croux, C.; Weich, S.; Deliege, D.; Mackenbach, J.; Ansseau, M. Depression and socio-economic risk factors: 7-Year longitudinal population study. Br. J. Psychiatry 2007, 190, 293–298. [Google Scholar] [CrossRef]
- Fagundes, C.; Jones, D.; Vichaya, E.; Lu, C.; Cleeland, C.S. Socioeconomic status is associated with depressive severity among patients with advanced non-small-cell lung cancer: Treatment setting and minority status do not make a difference. J. Thorac. Oncol. 2014, 9, 1459–1463. [Google Scholar] [CrossRef] [Green Version]
- Austin, P.; Wiley, S.; Mc Evoy, P.; Archer, L. Depression and anxiety in palliative care inpatients compared with those receiving palliative care at home. Palliat. Supportive Care 2011, 9, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Saastamoinen, P.; Leino-Arjas, P.; Laaksonen, M.; Lahelma, E. Socio-economic differences in the prevalence of acute, chronic and disabling chronic pain among ageing employees. Pain 2005, 114, 364–371. [Google Scholar] [CrossRef] [PubMed]
- Klein, J.; Hofresuter-Gatgens, K.; Ludecke, D.; Fisch, M.; Graefen, M.; Knesebeck, O. Socioeconomic status and health-related quality of life among patients with prostate cancer 6 months after radical prostatectomy: A longitudinal analysis. BMJ Open 2016, 6, e010968. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.L.; Kroenke, K.; Wu, J.; Tu, W.; Theobald, D.; Rawl, S.M. Predictors of cancer-related pain improvement over time. Psychosom Med. 2012, 74, 642–647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bubis, L.; Davis, L.; Mahar, A.; Barbera, L.; Qing, L.; Moody, L.; Karanicolas, P.; Rinku, S.; Coburn, N. Symptom Burden in the First Year After Cancer Diagnosis: An Analysis of Patient-Reported Outcomes. JCO 2018, 36, 1103–1121. [Google Scholar] [CrossRef] [PubMed]
- McLean, G.; Gunn, J.; Wyke, S.; Guthrie, B.; Watt, G.; Blane, D.; Mercer, S. The influence of socioeconomic deprivation on multimorbidity at different ages: A cross-sectional study. Br. J. Gen. Pract. 2014, 64, 440–447. [Google Scholar] [CrossRef] [Green Version]
- Malhotra, C.; Krishnan, A.; Yong, J.; Teo, I.; Ozdemir, S.; Ning, X.; Hapuarachchi, T.; Palat, G.; Bhatnagar, S.; Khan, A.; et al. Socio-economic inequalities in suffering at the end of life among advanced cancer patients: Results from the, APPROACH. study in five Asian countries. Int. J. Equity Health 2020, 19, 158. [Google Scholar] [CrossRef]
- Kim, S.; Knight, S.; Tomori, C.; Colella, K.; Schoor, R.; Shih, L.; Kuzel, T.; Nadler, R.; Bennett, C. Health literacy and shared decision making for prostate cancer patients with low socioeconomic status. Cancer Investig. 2001, 19, 684–691. [Google Scholar] [CrossRef]
- Noordman, J.; van Vliet, L.; Kaunang, M.; van den Muijsenbergh, M.; Boland, G.; van Dulmen, S. Towards appropriate information provision for and decision-making with patients with limited health literacy in hospital-based palliative care in Western countries: A scoping review into available communication strategies and tools for healthcare providers. BMC Palliat. Care 2019, 18, 37. [Google Scholar] [CrossRef] [Green Version]
- Willems, S.; De Maesschalck, S.; Deveugele, M.; Derese, A.; De Maeseneer, J. Socio-economic status of the patient and doctor–patient communication: Does it make a difference? Patient Educ. Couns. 2005, 56, 139–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, S.; Harris, R.; Brown, S.; Humphris, G.; Zhou, Y.; Rogers, S. High levels of socioeconomic deprivation did not inhibit patients’ communication of concerns in head and neck cancer review clinics. Br. J. Oral Maxillofac. Surg. 2018, 56, 536–539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woods, L.; Rachet, B.; Coleman, P. Origins of socio-economic inequalities in cancer survival: A review. Ann. Oncol. 2006, 17, 5–19. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Neighbourhood (LSOA) of Residence | |||
|---|---|---|---|---|
| Higher Deprivation | Intermediate Deprivation | Lower Deprivation | p-Value | |
| − | Q1/Q2 | Q3 | Q4/Q5 | |
| − | % (n/N) | % (n/N) | % (n/N) | p |
| Gender | ||||
| Male | 47.9 (93/194) | 16.0 (31/194) | 36.1 (70/194) | 0.38 |
| Female | 47.9 (192/401) | 20.2 (81/401) | 31.9 (128/401) | |
| Age group | ||||
| Aged under 60 | 51.2 (83/162) | 18.5 (30/162) | 30.2 (49/162) | 0.35 |
| Aged 60–70 | 42.2 (86/204) | 21.1 (43/204) | 36.8 (75/204) | |
| Aged over 70 | 50.9 (116/228) | 17.1 (39/228) | 32.0 (73/228) | |
| Marital status | ||||
| Married/cohabiting | 40.8 (130/319) | 20.1 (64/319) | 39.2 (125/319) | 0.01 |
| Divorced/widowed/single (living alone) | 55.4 (113/204) | 18.6 (38/204) | 26.0 (53/204) | |
| Divorced/widowed/single (not living alone) | 56.4 (31/55) | 16.4 (9/55) | 27.3 (15/55) | |
| Type of cancer | ||||
| Breast | 44.9 (92/205) | 17.6 (36/205) | 37.6 (77/205) | 0.02 |
| Gastrointestinal | 57.1 (60/105) | 17.1 (18/105) | 25.7 (27/105) | |
| Lung | 57.4 (39/68) | 23.5 (16/68) | 19.1 (13/68) | |
| Head and neck | 62.5 (20/32) | 15.6 (5/32) | 21.9 (7/32) | |
| Male specific | 40.7 (22/54) | 13.0 (7/54) | 46.3 (25/54) | |
| Female specific | 42.0 (21/50) | 26.0 (13/50) | 32.0 (16/50) | |
| Other | 38.3 (31/81) | 21.0 (17/81) | 40.7 (33/81) | |
| Time since cancer diagnosis | ||||
| In previous 12 months | 51.6 (113/219) | 19.6 (43/219) | 28.8 (63/219) | 0.20 |
| More than 12 months | 45.7 (172/376) | 18.4 (69/376) | 35.9 (135/376) | |
| Given sufficient information at diagnosis | ||||
| No | 50.0 (93/186) | 22.6 (42/186) | 27.4 (51/186) | 0.007 |
| Yes | 47.2 (185/392) | 16.8 (66/392) | 36.0 (141/392) | |
| Neighbourhood (LSOA) of Residence | ||||
|---|---|---|---|---|
| Characteristics | Higher Deprivation | Intermediate Deprivation | Lower Deprivation | p-Value |
| − | Q1/Q2 | Q3 | Q4/Q5 | |
| − | % (n/N) | % (n/N) | % (n/N) | p |
| ECOG score | ||||
| 0/1 | 45.1 (128/284) | 19.7 (56/284) | 35.2 (100/284) | 0.04 |
| 2 | 47.5 (76/160) | 23.8 (38/160) | 28.8 (46/160) | |
| 3–4 | 53.6 (81/151) | 11.9 (18/151) | 34.4 (52/151) | |
| Depression | ||||
| PHQ score < 10 | 44.6 (183/410) | 19.3 (79/410) | 36.1 (148/410) | 0.04 |
| PHQ score ≥ 10 | 55.1 (102/185) | 17.8 (33/185) | 27.0 (50/185) | |
| Reported physical symptom | ||||
| Pain | ||||
| No | 43.3 (91/210) | 16.2 (34/210) | 40.5 (85/210) | 0.02 |
| Yes | 50.4 (194/385) | 20.3 (78/385) | 29.4 (113/385) | |
| Breathlessness | ||||
| No | 46.2 (128/277) | 18.1 (50/277) | 35.7 (99/277) | 0.49 |
| Yes | 49.4 (157/318) | 19.5 (62/318) | 31.1 (99/318) | |
| Nausea | ||||
| No | 50.0 (220/440) | 17.7 (78/440) | 32.3 (142/440) | 0.21 |
| Yes | 41.9 (65/155) | 21.9 (34/155) | 36.1 (56/155) | |
| Fatigue | ||||
| No | 48.8 (61/125) | 17.6 (22/125) | 33.6 (42/125) | 0.92 |
| Yes | 47.7 (224/470) | 19.1 (90/470) | 33.2 (156/470) | |
| Constipation | ||||
| No | 45.4 (192/243) | 17.7 (75/423) | 36.9 (156/423) | 0.01 |
| Yes | 54.1 (93/172) | 21.5 (37/172) | 24.4 (42/172) | |
| Insomnia | ||||
| No | 48.8 (163/334) | 20.1 (67/334) | 31.1 (104/334) | 0.41 |
| Yes | 46.7 (122/261) | 17.2 (45/261) | 36.0 (94/261) | |
| No of reported physical symptoms | ||||
| 0–3 | 46.3 (174/376) | 17.6 (66/376) | 36.2 (136/376) | 0.14 |
| 4–6 | 50.7 (111/219) | 21.0 (46/219) | 28.3 (62/219) | |
| Global symptom severity rating (mean) (95% CI) | 5.0 (4.7–5.3) | 4.9 (4.5–5.3) | 4.5 (4.3–4.7) | 0.04 |
| Characteristics | Unadjusted OR (95% CI) | p | Adjusted * OR (95% CI) | p |
|---|---|---|---|---|
| Depression case (PHQ ≥ 10) Q1 vs. Q5 | 1.81 (1.09–3.01) | 0.02 | 1.75 (1.04–2.96) | 0.03 |
| Pain Q1 vs. Q5 | 1.99 (1.01–3.93) | 0.04 | 2.18 (1.09–4.39) | 0.03 |
| Breathlessness Q1 vs. Q5 | 1.16 (0.68–1.97) | 0.58 | 1.18 (0.68–2.07) | 0.54 |
| Nausea Q1 vs. Q5 | 0.75 (0.45–1.25) | 0.26 | 0.66 (0.39–1.12) | 0.12 |
| Fatigue Q1 vs. Q5 | 0.35 (0.13–0.94) | 0.04 | 0.34 (0.12–0.96) | 0.04 |
| Constipation Q1 vs. Q5 | 1.79 (1.07–2.99) | 0.03 | 1.75 (1.04–2.96 | 0.02 |
| Insomnia Q1 vs. Q5 | 1.04 (0.62–1.74) | 0.89 | 0.99 (0.58–1.72) | 0.99 |
| Residence in LSOA | Unadjusted β (95% CI) | p | Adjusted β (95% CI) | p |
|---|---|---|---|---|
| Social deprivation quintile | − | − | − | − |
| Q5 (least deprived) | 1.00 | − | 1.00 | − |
| Q4 | 0.14 (−0.76, 0.52) | 0.46 | 0.12 (−0.74, 0.50) | 0.54 |
| Q3 | 0.49 (0.11, 0.87) | 0.01 | 0.48 (0.09, 0.86) | 0.01 |
| Q2 | 0.47 (0.10, 0.85) | 0.01 | 0.45 (0.07, 0.84) | 0.02 |
| Q1 (most deprived) | 0.62 (0.27, 0.97) | 0.001 | 0.62 (0.25, 0.98) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lloyd-Williams, M.; Shiels, C.; Dowrick, C.; Kissane, D. Socio-Economic Deprivation and Symptom Burden in UK Hospice Patients with Advanced Cancer—Findings from a Longitudinal Study. Cancers 2021, 13, 2537. https://doi.org/10.3390/cancers13112537
Lloyd-Williams M, Shiels C, Dowrick C, Kissane D. Socio-Economic Deprivation and Symptom Burden in UK Hospice Patients with Advanced Cancer—Findings from a Longitudinal Study. Cancers. 2021; 13(11):2537. https://doi.org/10.3390/cancers13112537
Chicago/Turabian StyleLloyd-Williams, Mari, Christopher Shiels, Christopher Dowrick, and David Kissane. 2021. "Socio-Economic Deprivation and Symptom Burden in UK Hospice Patients with Advanced Cancer—Findings from a Longitudinal Study" Cancers 13, no. 11: 2537. https://doi.org/10.3390/cancers13112537
APA StyleLloyd-Williams, M., Shiels, C., Dowrick, C., & Kissane, D. (2021). Socio-Economic Deprivation and Symptom Burden in UK Hospice Patients with Advanced Cancer—Findings from a Longitudinal Study. Cancers, 13(11), 2537. https://doi.org/10.3390/cancers13112537