
Gemcitabine/Nab-Paclitaxel versus FOLFIRINOX in Locally Advanced Pancreatic Cancer: A European Multicenter Study

 , ,
, ,  ,
,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Chemotherapy Regimens
2.3. Outcome Evaluation
2.4. Statistical Analyses
3. Results
3.1. Study Population
3.2. Therapeutic Sequence and Events Potentially Impacting Survival
3.3. Survival and Prognostic Factors
3.4. Predictors of Tumor Response and Secondary Surgery
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting Cancer Incidence and Deaths to 2030: The Unexpected Burden of Thyroid, Liver, and Pancreas Cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quante, A.S.; Ming, C.; Rottmann, M.; Engel, J.; Boeck, S.; Heinemann, V.; Westphalen, C.B.; Strauch, K. Projections of Cancer Incidence and Cancer-Related Deaths in Germany by 2020 and 2030. Cancer Med. 2016, 5, 2649–2656. [Google Scholar] [CrossRef]
- Balaban, E.P.; Mangu, P.B.; Khorana, A.A.; Shah, M.A.; Mukherjee, S.; Crane, C.H.; Javle, M.M.; Eads, J.R.; Allen, P.; Ko, A.H.; et al. Locally Advanced, Unresectable Pancreatic Cancer: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2016, 34, 2654–2668. [Google Scholar] [CrossRef] [PubMed]
- Ducreux, M.; Cuhna, A.S.; Caramella, C.; Hollebecque, A.; Burtin, P.; Goéré, D.; Seufferlein, T.; Haustermans, K.; Van Laethem, J.L.; Conroy, T.; et al. Cancer of the Pancreas: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2015, 26 (Suppl. 5), v56–v68. [Google Scholar] [CrossRef]
- Neuzillet, C.; Gaujoux, S.; Williet, N.; Bachet, J.-B.; Bauguion, L.; Colson Durand, L.; Conroy, T.; Dahan, L.; Gilabert, M.; Huguet, F.; et al. Pancreatic Cancer: French Clinical Practice Guidelines for Diagnosis, Treatment and Follow-up (SNFGE, FFCD, GERCOR, UNICANCER, SFCD, SFED, SFRO, ACHBT, AFC). Dig. Liver Dis. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver 2018, 50, 1257–1271. [Google Scholar] [CrossRef]
- Rocha Lima, C.M.; Green, M.R.; Rotche, R.; Miller, W.H.; Jeffrey, G.M.; Cisar, L.A.; Morganti, A.; Orlando, N.; Gruia, G.; Miller, L.L. Irinotecan plus Gemcitabine Results in No Survival Advantage Compared with Gemcitabine Monotherapy in Patients with Locally Advanced or Metastatic Pancreatic Cancer despite Increased Tumor Response Rate. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2004, 22, 3776–3783. [Google Scholar] [CrossRef] [PubMed]
- Louvet, C.; Labianca, R.; Hammel, P.; Lledo, G.; Zampino, M.G.; André, T.; Zaniboni, A.; Ducreux, M.; Aitini, E.; Taïeb, J.; et al. Gemcitabine in Combination with Oxaliplatin Compared with Gemcitabine Alone in Locally Advanced or Metastatic Pancreatic Cancer: Results of a GERCOR and GISCAD Phase III Trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2005, 23, 3509–3516. [Google Scholar] [CrossRef]
- Philip, P.A.; Mooney, M.; Jaffe, D.; Eckhardt, G.; Moore, M.; Meropol, N.; Emens, L.; O’Reilly, E.; Korc, M.; Ellis, L.; et al. Consensus Report of the National Cancer Institute Clinical Trials Planning Meeting on Pancreas Cancer Treatment. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2009, 27, 5660–5669. [Google Scholar] [CrossRef]
- Van Laethem, J.-L.; Verslype, C.; Iovanna, J.L.; Michl, P.; Conroy, T.; Louvet, C.; Hammel, P.; Mitry, E.; Ducreux, M.; Maraculla, T.; et al. New Strategies and Designs in Pancreatic Cancer Research: Consensus Guidelines Report from a European Expert Panel. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2012, 23, 570–576. [Google Scholar] [CrossRef]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouché, O.; Guimbaud, R.; Bécouarn, Y.; Adenis, A.; Raoul, J.-L.; Gourgou-Bourgade, S.; de la Fouchardière, C.; et al. FOLFIRINOX versus Gemcitabine for Metastatic Pancreatic Cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Hoff, D.D.; Ervin, T.; Arena, F.P.; Chiorean, E.G.; Infante, J.; Moore, M.; Seay, T.; Tjulandin, S.A.; Ma, W.W.; Saleh, M.N.; et al. Increased Survival in Pancreatic Cancer with Nab-Paclitaxel plus Gemcitabine. N. Engl. J. Med. 2013, 369, 1691–1703. [Google Scholar] [CrossRef] [Green Version]
- Marthey, L.; Sa-Cunha, A.; Blanc, J.F.; Gauthier, M.; Cueff, A.; Francois, E.; Trouilloud, I.; Malka, D.; Bachet, J.B.; Coriat, R.; et al. FOLFIRINOX for Locally Advanced Pancreatic Adenocarcinoma: Results of an AGEO Multicenter Prospective Observational Cohort. Ann. Surg. Oncol. 2015, 22, 295–301. [Google Scholar] [CrossRef]
- Sadot, E.; Doussot, A.; O’Reilly, E.M.; Lowery, M.A.; Goodman, K.A.; Do, R.K.G.; Tang, L.H.; Gönen, M.; D’Angelica, M.I.; DeMatteo, R.P.; et al. FOLFIRINOX Induction Therapy for Stage 3 Pancreatic Adenocarcinoma. Ann. Surg. Oncol. 2015, 22, 3512–3521. [Google Scholar] [CrossRef] [Green Version]
- Suker, M.; Beumer, B.R.; Sadot, E.; Marthey, L.; Faris, J.E.; Mellon, E.A.; El-Rayes, B.F.; Wang-Gillam, A.; Lacy, J.; Hosein, P.J.; et al. FOLFIRINOX for Locally Advanced Pancreatic Cancer: A Systematic Review and Patient-Level Meta-Analysis. Lancet Oncol. 2016, 17, 801–810. [Google Scholar] [CrossRef] [Green Version]
- Auclin, E.; Marthey, L.; Mas, L.; Francois, E.; Sa Cunha, A.; Bachet, J.B.; Tougeron, D.; Vienot, A.; Lecomte, T.; Hautefeuille, V.; et al. Folfirinox in Locally Advanced (La) and Borderline Resectable (Br) Pancreatic Adenocarcinoma: Update of the Ageo Cohort. Ann. Oncol. 2019, 30 (Suppl. 5), V253–V324. [Google Scholar] [CrossRef]
- Petrelli, F.; Coinu, A.; Borgonovo, K.; Cabiddu, M.; Ghilardi, M.; Lonati, V.; Aitini, E.; Barni, S.; Gruppo Italiano per lo Studio dei Carcinomi dell’Apparato Digerente (GISCAD). FOLFIRINOX-Based Neoadjuvant Therapy in Borderline Resectable or Unresectable Pancreatic Cancer: A Meta-Analytical Review of Published Studies. Pancreas 2015, 44, 515–521. [Google Scholar] [CrossRef]
- Kunzmann, V.; Martens, U.M.; Alguel, H.; Siveke, J.T.; Goekkurt, E.; Pelzer, U.; Siegler, G.M.; Hennes, E.; Waldschmidt, D.; Jakobs, R.; et al. Secondary Resectability in Locally Advanced Pancreatic Cancer (LAPC) after Nab-Paclitaxel/Gemcitabine- versus FOLFIRINOX-Based Induction Chemotherapy: Interim Results of a Randomized Phase II AIO Trial (NEOLAP). J. Clin. Oncol. 2018, 36, e348. [Google Scholar] [CrossRef]
- Philip, P.A.; Lacy, J.; Portales, F.; Sobrero, A.; Pazo-Cid, R.; Manzano Mozo, J.L.; Kim, E.J.; Dowden, S.; Zakari, A.; Borg, C.; et al. Nab-Paclitaxel plus Gemcitabine in Patients with Locally Advanced Pancreatic Cancer (LAPACT): A Multicentre, Open-Label Phase 2 Study. Lancet Gastroenterol. Hepatol. 2020, 5, 285–294. [Google Scholar] [CrossRef]
- NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ®). Pancreatic Adenocarcinoma. Version 2. 2017. Available online: https://www.nccn.org/professionals/physician_gls/pdf/pancreatic.pdf (accessed on 24 June 2017).
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New Response Evaluation Criteria in Solid Tumours: Revised RECIST Guideline (Version 1.1). Eur. J. Cancer Oxf. Engl. 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Muranaka, T.; Kuwatani, M.; Komatsu, Y.; Sawada, K.; Nakatsumi, H.; Kawamoto, Y.; Yuki, S.; Kubota, Y.; Kubo, K.; Kawahata, S.; et al. Comparison of Efficacy and Toxicity of FOLFIRINOX and Gemcitabine with Nab-Paclitaxel in Unresectable Pancreatic Cancer. J. Gastrointest. Oncol. 2017, 8, 566–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tahara, J.; Shimizu, K.; Otsuka, N.; Akao, J.; Takayama, Y.; Tokushige, K. Gemcitabine plus Nab-Paclitaxel vs. FOLFIRINOX for Patients with Advanced Pancreatic Cancer. Cancer Chemother. Pharmacol. 2018, 82, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Peterson, S.L.; Husnain, M.; Pollack, T.; Pimentel, A.; Loaiza-Bonilla, A.; Westendorf-Overley, C.; Ratermann, K.; Anthony, L.; Desimone, P.; Goel, G.; et al. Neoadjuvant Nab-Paclitaxel and Gemcitabine in Borderline Resectable or Locally Advanced Unresectable Pancreatic Adenocarcinoma in Patients Who Are Ineligible for FOLFIRINOX. Anticancer Res. 2018, 38, 4035–4039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vogl, U.M.; Andalibi, H.; Klaus, A.; Vormittag, L.; Schima, W.; Heinrich, B.; Kafka, A.; Winkler, T.; Öhler, L. Nab-Paclitaxel and Gemcitabine or FOLFIRINOX as First-Line Treatment in Patients with Unresectable Adenocarcinoma of the Pancreas: Does Sequence Matter? BMC Cancer 2019, 19, 28. [Google Scholar] [CrossRef] [Green Version]
- Papneja, N.; Zaidi, A.; Chalchal, H.; Moser, M.; Tan, K.; Olson, C.; Haider, K.; Shaw, J.; Ahmed, S. Comparisons of Outcomes of Real-World Patients with Advanced Pancreatic Cancer Treated with FOLFIRINOX Versus Gemcitabine and Nab-Paclitaxel: A Population-Based Cohort Study. Pancreas 2019, 48, 920–926. [Google Scholar] [CrossRef]
- Chiorean, E.G.; Cheung, W.Y.; Giordano, G.; Kim, G.; Al-Batran, S.-E. Real-World Comparative Effectiveness of Nab-Paclitaxel plus Gemcitabine versus FOLFIRINOX in Advanced Pancreatic Cancer: A Systematic Review. Ther. Adv. Med. Oncol. 2019, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macedo, F.I.; Ryon, E.; Maithel, S.K.; Lee, R.M.; Kooby, D.A.; Fields, R.C.; Hawkins, W.G.; Williams, G.; Maduekwe, U.; Kim, H.J.; et al. Survival Outcomes Associated with Clinical and Pathological Response Following Neoadjuvant FOLFIRINOX or Gemcitabine/Nab-Paclitaxel Chemotherapy in Resected Pancreatic Cancer. Ann. Surg. 2019, 270, 400–413. [Google Scholar] [CrossRef]
- Chan, K.K.W.; Guo, H.; Cheng, S.; Beca, J.M.; Redmond-Misner, R.; Isaranuwatchai, W.; Qiao, L.; Earle, C.; Berry, S.R.; Biagi, J.J.; et al. Real-World Outcomes of FOLFIRINOX vs. Gemcitabine and Nab-Paclitaxel in Advanced Pancreatic Cancer: A Population-Based Propensity Score-Weighted Analysis. Cancer Med. 2020, 9, 160–169. [Google Scholar] [CrossRef]
- Wolfe, A.R.; Prabhakar, D.; Yildiz, V.O.; Cloyd, J.M.; Dillhoff, M.; Abushahin, L.; Alexandra Diaz, D.; Miller, E.D.; Chen, W.; Frankel, W.L.; et al. Neoadjuvant-Modified FOLFIRINOX vs. Nab-Paclitaxel plus Gemcitabine for Borderline Resectable or Locally Advanced Pancreatic Cancer Patients Who Achieved Surgical Resection. Cancer Med. 2020, 9, 4711–4723. [Google Scholar] [CrossRef]
- Perri, G.; Prakash, L.; Qiao, W.; Varadhachary, G.R.; Wolff, R.; Fogelman, D.; Overman, M.; Pant, S.; Javle, M.; Koay, E.J.; et al. Response and Survival Associated with First-Line FOLFIRINOX vs. Gemcitabine and Nab-Paclitaxel Chemotherapy for Localized Pancreatic Ductal Adenocarcinoma. JAMA Surg. 2020, 155, 832–839. [Google Scholar] [CrossRef]
- Weniger, M.; Moir, J.; Damm, M.; Maggino, L.; Kordes, M.; Rosendahl, J.; Ceyhan, G.O.; Schorn, S. RESPECT-study group Neoadjuvant Therapy in Elderly Patients Receiving FOLFIRINOX or Gemcitabine/Nab-Paclitaxel for Borderline Resectable or Locally Advanced Pancreatic Cancer Is Feasible and Lead to a Similar Oncological Outcome Compared to Non-Aged Patients–Results of the RESPECT-Study. Surg. Oncol. 2020, 35, 285–297. [Google Scholar] [CrossRef]
- Petrillo, A.; Pappalardo, A.; Calabrese, F.; Tirino, G.; Pompella, L.; Ventriglia, J.; Laterza, M.M.; Caterino, M.; Sforza, V.; Iranzo, V.; et al. First Line Nab-Paclitaxel plus Gemcitabine in Elderly Metastatic Pancreatic Patients: A Good Choice beyond Age. J. Gastrointest. Oncol. 2019, 10, 910–917. [Google Scholar] [CrossRef]
- De Vita, F.; Ventriglia, J.; Febbraro, A.; Laterza, M.M.; Fabozzi, A.; Savastano, B.; Petrillo, A.; Diana, A.; Giordano, G.; Troiani, T.; et al. NAB-Paclitaxel and Gemcitabine in Metastatic Pancreatic Ductal Adenocarcinoma (PDAC): From Clinical Trials to Clinical Practice. BMC Cancer 2016, 16, 709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williet, N.; Saint, A.; Pointet, A.-L.; Tougeron, D.; Pernot, S.; Pozet, A.; Bechade, D.; Trouilloud, I.; Lourenco, N.; Hautefeuille, V.; et al. Folfirinox versus Gemcitabine/Nab-Paclitaxel as First-Line Therapy in Patients with Metastatic Pancreatic Cancer: A Comparative Propensity Score Study. Ther. Adv. Gastroenterol. 2019, 12, 1756284819878660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mizusawa, J.; Fukutomi, A.; Katayama, H.; Ishii, H.; Ioka, T.; Okusaka, T.; Ueno, H.; Ueno, M.; Ikeda, M.; Mizuno, N.; et al. Protocol Digest of Randomized Phase II Study of Modified FOLFIRINOX versus Gemcitabine plus Nab-Paclitaxel Combination Therapy for Locally Advanced Pancreatic Cancer: Japan Clinical Oncology Group Study (JCOG1407). Pancreatol. Off. J. Int. Assoc. Pancreatol. IAP Al 2018, 18, 841–845. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.-J. A Phase Ⅲ, Randomized Controlled Study to Evaluate the Efficacy and Safety of the Combination of Nab-Paclitaxel and Gemcitabine Versus mFOLFIRINOX in Treating Patients with Borderline Reseactable and Locally Advanced Pancreatic Cancer. 2020. Available online: https://clinicaltrials.gov/ct2/show/NCT04617821/ (accessed on 4 February 2021).
- Ahmad, S.A.; Duong, M.; Sohal, D.P.S.; Gandhi, N.S.; Beg, M.S.; Wang-Gillam, A.; Wade, J.L.; Chiorean, E.G.; Guthrie, K.A.; Lowy, A.M.; et al. Surgical Outcome Results from SWOG S1505: A Randomized Clinical Trial of MFOLFIRINOX Versus Gemcitabine/Nab-Paclitaxel for Perioperative Treatment of Resectable Pancreatic Ductal Adenocarcinoma. Ann. Surg. 2020, 272, 481–486. [Google Scholar] [CrossRef]
- Hammel, P.; Huguet, F.; van Laethem, J.-L.; Goldstein, D.; Glimelius, B.; Artru, P.; Borbath, I.; Bouché, O.; Shannon, J.; André, T.; et al. Effect of Chemoradiotherapy vs. Chemotherapy on Survival in Patients with Locally Advanced Pancreatic Cancer Controlled After 4 Months of Gemcitabine with or Without Erlotinib: The LAP07 Randomized Clinical Trial. JAMA 2016, 315, 1844–1853. [Google Scholar] [CrossRef]
- Dahan, L.; Phelip, J.-M.; Le Malicot, K.; Williet, N.; Desrame, J.; Volet, J.; Petorin, C.; Malka, D.; Rebischung, C.; Aparicio, T.; et al. FOLFIRINOX until Progression, FOLFIRINOX with Maintenance Treatment, or Sequential Treatment with Gemcitabine and FOLFIRI.3 for First-Line Treatment of Metastatic Pancreatic Cancer: A Randomized Phase II Trial (PRODIGE 35-PANOPTIMOX). J. Clin. Oncol. 2018, 36, e4000. [Google Scholar] [CrossRef]
- Taieb, J.; Prager, G.W.; Melisi, D.; Westphalen, C.B.; D’Esquermes, N.; Ferreras, A.; Carrato, A.; Macarulla, T. First-Line and Second-Line Treatment of Patients with Metastatic Pancreatic Adenocarcinoma in Routine Clinical Practice across Europe: A Retrospective, Observational Chart Review Study. ESMO Open 2020, 5, e000587. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variables | Study Population | Gemcitabine/Nab-Paclitaxel | FOLFIRINOX | p-Value |
|---|---|---|---|---|
| (n = 147) | (n = 60) | (n = 87) | ||
| Country | <0.001 | |||
| France (n = 4) | 98 (66.7%) | 33 (55%) | 65 (74.7%) | |
| Italy (n = 2) | 37 (25.2%) | 27 (45%) | 10 (11.5%) | |
| Bulgaria (n = 1) | 12 (8.2%) | 0 (0%) | 12 (13.8%) | |
| Age, median (IQR) | 66 (59–72) | 71 (63.8–77) | 63 (56–67.5) | <0.001 |
| Age > 70 years, n (%) | 45 (30.6%) | 33 (55%) | 12 (13.8%) | <0.001 |
| Male sex, n (%) | 83 (56.5%) | 31 (51.7%) | 52 (59.8%) | 0.42 |
| Arterial hypertension, n (%) | 51 (34.7%) | 15 (25%) | 36 (41.4%) | 0.48 |
| Diabetes, n (%) | 49 (33.3%) | 24 (40%) | 25 (28.7%) | 0.21 |
| History of myocardial ischemia, n (%) | 11 (7.5%) | 5 (8.3%) | 6 (6.9%) | 0.2 |
| Performance status, n (%) | ||||
| ECOG 0–1 | 133 (95%) | 50 (87.7%) | 83 (100%) | 0.001 |
| ECOG 0 | 73 (49.7%) | 21 (35%) | 52 (59.8%) | <0.001 |
| ECOG 1 | 60 (40.8%) | 29 (48.3%) | 31 (35.6%) | |
| ECOG 2 | 7 (4.8%) | 7 (11.7%) | 0 (0%) | |
| Missing data | 7 (4.8%) | 3 (5%) | 4 (4.6%) | |
| Tumor location, n (%) | ||||
| Head | 106 (72.1%) | 38 (63.3%) | 68 (78.2%) | 0.11 |
| Body | 34 (23.1%) | 19 (31.7%) | 15 (17.2%) | |
| Tail | 7 (4.8%) | 3 (5%) | 4 (4.6%) | |
| Bilirubin, median (IQR) | 12 (6.5–19) | 8.4 (1.2–14) | 15 (9–20.8) | - |
| Albumin, median (IQR) | 36.6 (33–40) | 36.8 (35–40.9) | 36 (33–39.5) | 0.34 |
| CA19-9, median (IQR) | 127 (36.1–471.2) | 83 (18–403.2) | 172 (57.5–535.6) | 0.07 |
| Variables | Study Population Study (n = 147) | Gemcitabine/Nab-Paclitaxel (n = 60) | FOLFIRINOX (n = 87) | p-Value |
|---|---|---|---|---|
| Number of resolved cases, median (IQR) | 9 (5–12) | 12 (9–18) | 8 (5–10) | <0.001 |
| Tumor response (RECIST), n (%) | 31 (21.1%) | 13 (21.7%) | 18 (20.7%) | 1 |
| Management of patients within 4–6 months | ||||
| Best supportive care (in case of disease progression) | 11 (7.5%) | 7 (11.7%) | 1 (1.1%) | 1 |
| Second-line therapy (in case of disease progression) | 25 (17%) | 10 (16.7%) | 15 (17.2%) | 1 |
| Continuation treatment | 28 (19%) | 23 (38.3%) | 5 (5.7%) | <0.001 |
| Maintenance treatment | 7 (4.8%) | 1 (1.7%) | 6 (6.9%) | 0.24 |
| Therapeutic break | 4 (2.4%) | 2 (3.3%) | 2 (2.3%) | 1 |
| Consolidation chemoradiotherapy, n (%) | 51 (34.7%) | 7 (11.7%) | 44 (50.6%) | <0.001 |
| Secondary pancreatic resection, n(%) | 24 (16.3%) | 10 (16.7%) | 14 (16.1%) | 1 |
| Duodenopancreatectomy | 19 (79.2%) | 8 (80%) | 11 (78.6%) | 1 |
| Splenopancreatectomy | 5 (20.8%) | 2 (20%) | 3 (21.4%) | |
| Pathological tumor | 0.81 | |||
| pT0 | 1 (4.5%) | 0 (0%) | 1 (7.7%) | |
| pT2 | 6 (27.3%) | 3 (33.3%) | 3 (23.1%) | |
| pT3 | 12 (54.5%) | 5 (55.6%) | 7 (53.8%) | |
| pT4 | 3 (13.6%) | 1 (11.1%) | 2 (15.4%) | |
| Pathological node | ||||
| pN+ | 11 (50%) | 6 (66.7%) | 5 (38.5%) | 0.49 |
| pN0 | 11 (50%) | 3 (33.3%) | 8 (61.5%) | 0.10 |
| pN1 | 9 (40.9%) | 6 (66.7%) | 3 (23.1%) | |
| pN2 | 2 (9.1%) | 0 (0%) | 2 (15.4%) | |
| Negative resection margin (R0) | 16 (88.9%) | 8 (88.9%) | 12 (92.3%) | 1 |
| Grade 3–4 toxicity, n (%) | 39 (27.6%) | 16 (26.7%) | 23 (28.4%) | 0.97 |
| Neutropenia | 17 (11.6%) | 11 (18.3%) | 6 (6.9%) | 0.062 |
| Anemia | 4 (2.7%) | 4 (6.7%) | 0 (0%) | 0.054 |
| Diarrhea | 4 (2.7%) | 2 (3.3%) | 2 (2.3%) | 1 |
| Vomiting | 4 (2.7%) | 1 (1.7%) | 3 (3.4%) | 0.89 |
| Second line of chemotherapy | 65 (44.2%) | 29 (48.3%) | 36 (41.4%) | 0.51 |
| Gemcitabine | 20 (23%) | |||
| Gemcitabine/nab-paclitaxel | 11 (12.6%) | |||
| FOLFOX or XELOX | 6 (10%) | |||
| FOLFIRI | 15 (25%) | |||
| Nal-IRI (nanoliposomal irinotecan) LV5FU2 | 3 (5%) | |||
| FOLFIRINOX | 2 (3.3%) | |||
| Other | 3 (5.1%) | 5 (5.7%) | ||
| Third line of chemotherapy | 19 (12.9%) | 13 (21.7%) | 6 (6.9%) | 0.02 |
| Prognostic Factor | Univariate Analyses | Multivariate Analyses (Adjusting for Age > 70 Years and ECOG) | ||
|---|---|---|---|---|
| p-Value | HR (95% CI) | p-Value | HR (95% CI) | |
| Country | ||||
| France (n = 98) vs. Bulgaria (n = 12) | 0.6 | 1.19 (0.62–2.30) | ||
| Italy (n = 37) vs. Bulgaria (n = 12) | 0.93 | 1.03 (0.50–2.13) | ||
| Age (years) | 0.6 | 0.99 (0.98–1.01) | ||
| Age > 70 years (n = 45) vs. ≤70 years (n = 102) | 0.83 | 0.96 (0.64–1.43) | 0.12 | 0.55 (0.26–1.16) |
| Sex: male (n = 83) vs. female (n = 64) | 0.58 | 1.1 (0.78–1.57) | ||
| Arterial hypertension: no (n = 64) vs. yes (n = 51) | 0.64 | 1.1 (0.74–1.64) | ||
| Diabetes: no (n = 98) vs. yes (n = 49) | 0.74 | 0.94 (0.65–1.36) | ||
| History of myocardial ischemia: no (n = 105) vs. yes (n = 11) | 0.83 | 0.93 (0.48–1.79) | ||
| Performance status at the baseline: ECOG 1 (n = 60) vs. ECOG 0 (n = 73) | 0.76 | 1.06 (0.73–1.54) | 0.14 | 0.65 (0.36–1.15) |
| ECOG 2 (n = 7) vs. ECOG 0 (n = 73) | 0.18 | 1.72 (0.78–3.78) | 0.24 | 0.27 (0.03–2.38) |
| Abdominal pain: yes (n = 54) vs. no (n = 30) | 0.027 | 1.8 (1.07–3.02) | 0.035 | 2.03 (1.05–3.92) |
| Tumor location: head (n = 106) vs. tail (n = 7) | 0.016 | 0.38 (0.17–0.84) | 0.013 | 0.23 (0.07–0.73) |
| Body (n = 34) vs. tail (n = 7) | 0.011 | 0.33 (0.14–0.78) | 0.003 | 0.13 (0.03–0.5) |
| Tumor size (mm) | 0.4 | 1.01 (0.99–1.02) | ||
| Tumor size > 50 mm (n = 16) vs. ≤50 mm (n = 96) | 0.21 | 1.45 (0.81–2.58) | ||
| Bilirubin (µmol/L) | 0.42 | 1 (1–1.01) | ||
| Albumin (g/L) | 0.89 | 1 (0.98–1.03) | ||
| CA19-9 (UI/L) | 0.28 | 1 (1–1) | ||
| CA19-9 > 200 UI/L (n = 52) vs. ≤200 UI/L (n = 74) | <0.001 | 1.79 (1.22–2.63) | 0.004 | 2.3 (1.3–4.08) |
| Tumor response (RECIST): yes (n = 35) vs. no (n = 110) | 0.16 | 0.74 (0.48–1.12) | ||
| Secondary surgery: yes (n = 24) vs. no (n = 123) | 0.011 | 0.52 (0.32–0.86) | 0.007 | 0.37 (0.18–0.76) |
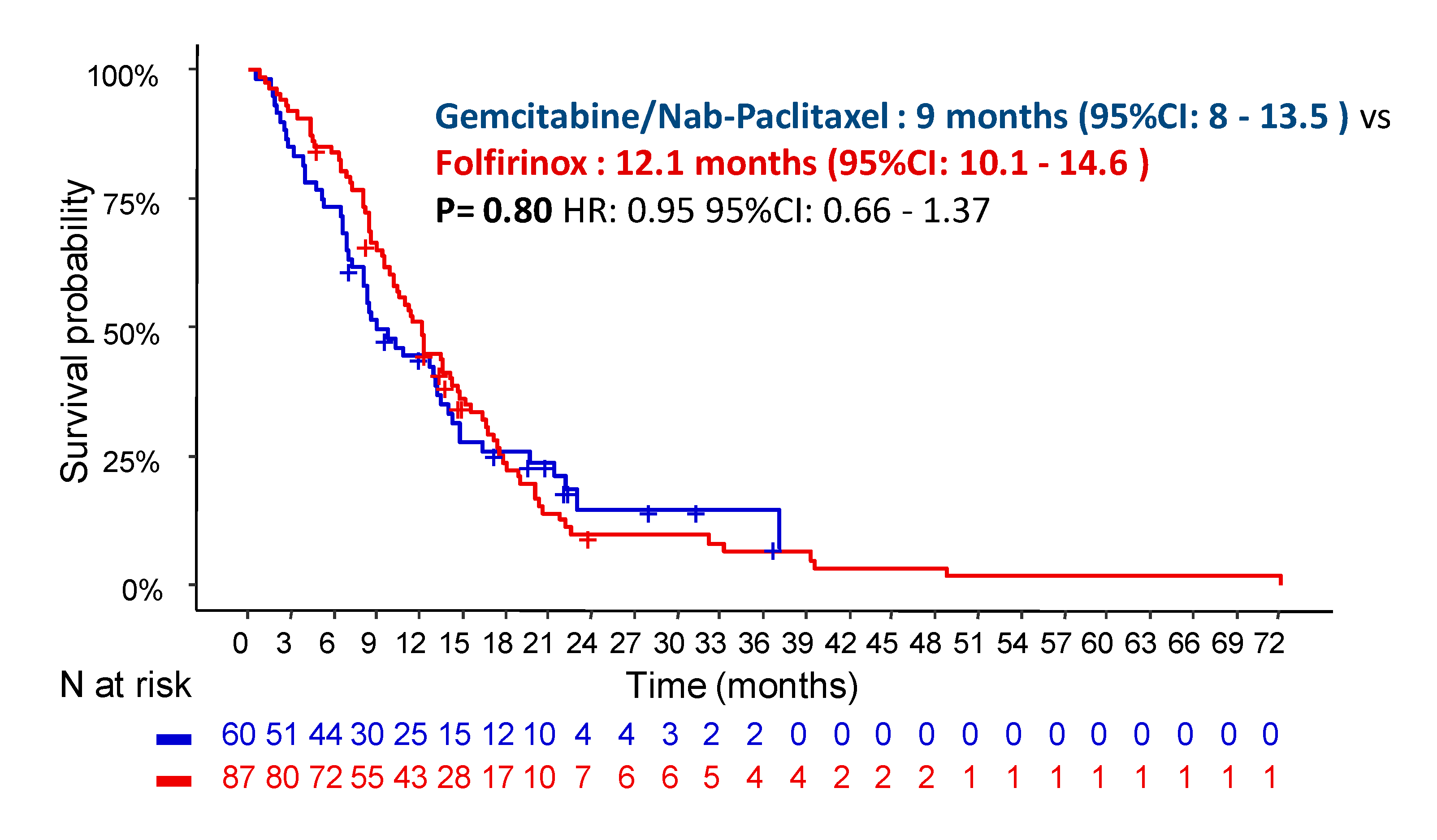
| Chemotherapy regimen: FFX (n = 87) vs. GN (n = 60) | 0.80 | 1.05 (0.73–1.51) | 0.5 | 1.24 (0.66–2.32) |
| Prognostic Factor | Univariate Analyses | Multivariate Analyses (Adjusting for Age > 70 Years and ECOG) | ||
|---|---|---|---|---|
| p-Value | HR (95% CI) | p-Value | HR (95% CI) | |
| Country | ||||
| France (n = 98) vs. Bulgaria (n = 12) | 0.51 | 0.80 (0.41–1.56) | ||
| Italy (n = 37) vs. Bulgaria (n = 12) | 0.64 | 0.84 (0.40–1.74) | ||
| Age (years) | 0.85 | 1 (0.98–1.02) | ||
| Age > 70 years (n = 45) vs. ≤70 years (n = 102) | 0.60 | 1.12 (0.74–1.7) | 0.92 | 1.03 (0.58–1.84) |
| Sex: male (n = 83) vs. female (n = 64) | 0.42 | 1.16 (0.8–1.68) | ||
| Arterial hypertension: no (n = 64) vs. yes (n = 51) | 0.84 | 0.96 (0.64–1.44) | ||
| Diabetes: no (n = 98) vs. yes (n = 49) | 0.9 | 0.98 (0.66–1.44) | ||
| History of myocardial ischemia: no (n = 105) vs. yes (n = 11) | 0.31 | 0.71 (0.36–1.37) | ||
| Performance status at the baseline: ECOG 1 (n = 60) vs. ECOG 0 (n = 73) | 0.54 | 1.13 (0.77–1.66) | 0.21 | 1.33 (0.85–2.08) |
| ECOG 2 (n = 7) vs. ECOG 0 (n = 73) | 0.023 | 2.68 (1.14–6.28) | 0.47 | 1.49 (0.51–4.36) |
| Abdominal pain: yes (n = 54) vs. no (n = 30) | 0.1 | 1.55 (0.91–2.62) | ||
| Tumor location: head (n = 106) vs. tail (n = 7) | 0.042 | 0.42 (0.18–0.97) | 0.1 | 0.45 (0.17–1.16) |
| Body (n = 34) vs. tail (n = 7) | 0.033 | 0.38 (0.16–0.93) | 0.032 | 0.32 (0.11–0.91) |
| Tumor size (mm) | 0.27 | 1.01 (0.99–1.02) | ||
| Tumor size > 50 mm (n = 16) vs. ≤50 mm (n = 96) | 0.26 | 1.38 (0.79–2.42) | ||
| Bilirubin (µmol/L) | 0.4 | 1 (1–1.01) | ||
| Albumin (g/L) | 0.77 | 1 (0.98–1.03) | ||
| CA19-9 (UI/L) | 0.021 | 1 (1–1) | ||
| CA19-9 > 200 UI/L (n = 52) vs. ≤200 UI/L (n = 74) | <0.001 | 1.8 (1.2–2.68) | 0.015 | 1.71 (1.11–2.65) |
| Tumor response (RECIST): yes (n = 35) vs. no (n = 110) | 0.19 | 0.74 (0.48–1.15) | ||
| Secondary surgery: yes (n = 24) vs. no (n = 123) | 0.002 | 0.4 (0.23–0.71) | 0.003 | 0.38 (0.2–0.71) |
| Chemotherapy regimen: FFX (n = 87) vs. GN (n = 60) | 0.70 | 1.08 (0.74–1.57) | 0.60 | 1.15 (0.68–1.94) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Williet, N.; Petrillo, A.; Roth, G.; Ghidini, M.; Petrova, M.; Forestier, J.; Lopez, A.; Thoor, A.; Weislinger, L.; De Vita, F.; et al. Gemcitabine/Nab-Paclitaxel versus FOLFIRINOX in Locally Advanced Pancreatic Cancer: A European Multicenter Study. Cancers 2021, 13, 2797. https://doi.org/10.3390/cancers13112797
Williet N, Petrillo A, Roth G, Ghidini M, Petrova M, Forestier J, Lopez A, Thoor A, Weislinger L, De Vita F, et al. Gemcitabine/Nab-Paclitaxel versus FOLFIRINOX in Locally Advanced Pancreatic Cancer: A European Multicenter Study. Cancers. 2021; 13(11):2797. https://doi.org/10.3390/cancers13112797
Chicago/Turabian StyleWilliet, Nicolas, Angelica Petrillo, Gaël Roth, Michele Ghidini, Mila Petrova, Julien Forestier, Anthony Lopez, Audrey Thoor, Lucie Weislinger, Ferdinando De Vita, and et al. 2021. "Gemcitabine/Nab-Paclitaxel versus FOLFIRINOX in Locally Advanced Pancreatic Cancer: A European Multicenter Study" Cancers 13, no. 11: 2797. https://doi.org/10.3390/cancers13112797
APA StyleWilliet, N., Petrillo, A., Roth, G., Ghidini, M., Petrova, M., Forestier, J., Lopez, A., Thoor, A., Weislinger, L., De Vita, F., Taieb, J., & Phelip, J. M. (2021). Gemcitabine/Nab-Paclitaxel versus FOLFIRINOX in Locally Advanced Pancreatic Cancer: A European Multicenter Study. Cancers, 13(11), 2797. https://doi.org/10.3390/cancers13112797