
Pretreatment Plasma IL-6 and YKL-40 and Overall Survival after Surgery for Metastatic Bone Disease of the Extremities

 ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Clinical Variables
2.2. Statistical Analysis
3. Results
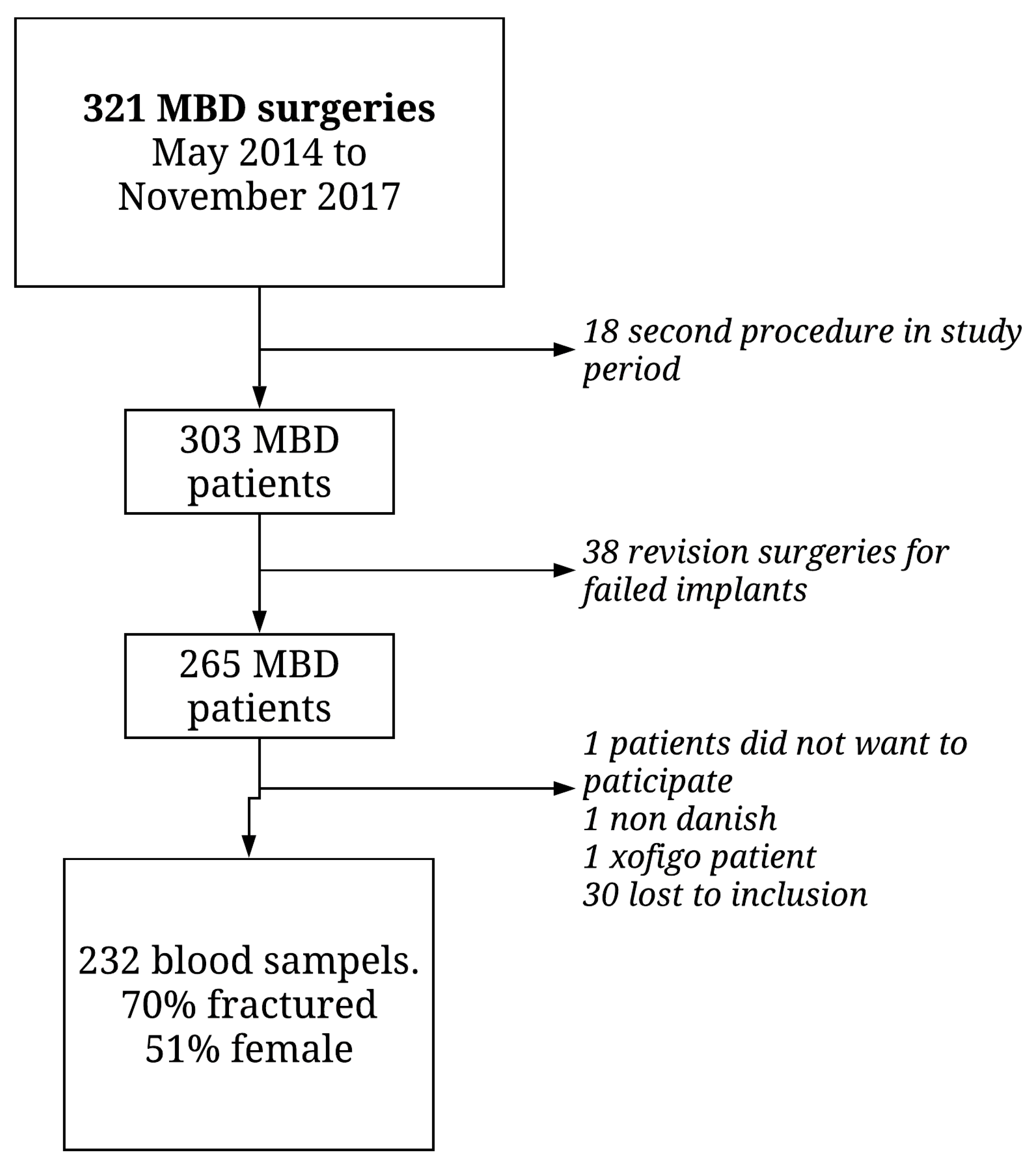
3.1. Clinical Characteristics
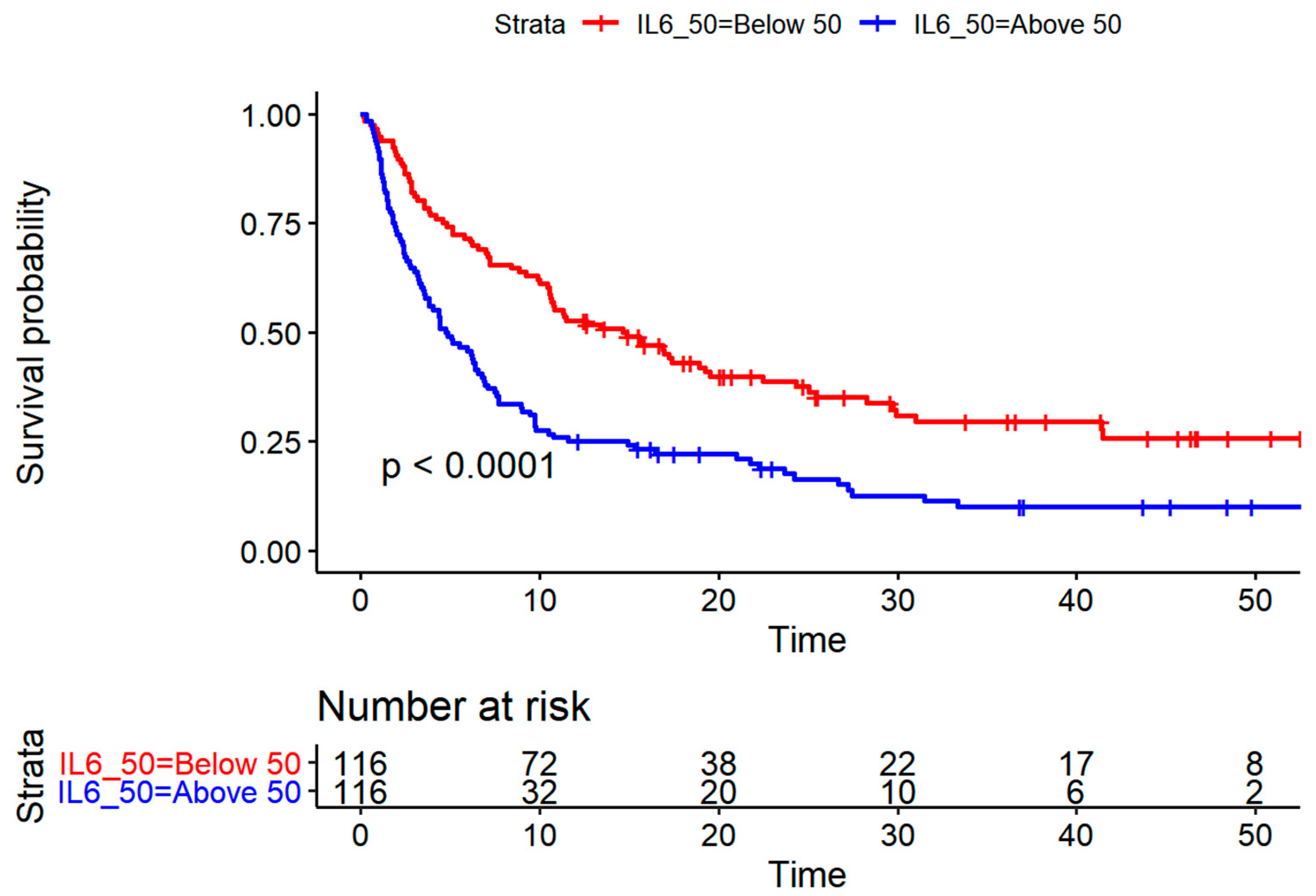
3.2. Plasma IL-6 and YKL-40 and Overall Survival
3.2.1. Univariate Analysis
3.2.2. Multivariate Analysis
4. Discussion
4.1. Limitations
4.2. Inflammatory Response
4.3. Performance Status and Comorbidity
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Steensma, M.; Healey, J.H. Trends in the surgical treatment of pathologic proximal femur fractures among Musculoskeletal Tumor Society members. Clin. Orthop. Relat. Res. 2013, 471, 2000–2006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorensen, M.S.; Gerds, T.A.; Hindso, K.; Petersen, M.M. Prediction of survival after surgery due to skeletal metastases in the extremities. Bone Jt. J. 2016, 98, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Forsberg, J.A.; Sjoberg, D.; Chen, Q.R.; Vickers, A.; Healey, J.H. Treating metastatic disease: Which survival model is best suited for the clinic? Clin. Orthop. Relat. Res. 2013, 471, 843–850. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katagiri, H.; Okada, R.; Takagi, T.; Takahashi, M.; Murata, H.; Harada, H.; Nishimura, T.; Asakura, H.; Ogawa, H. New prognostic factors and scoring system for patients with skeletal metastasis. Cancer Med. 2014, 3, 1359–1367. [Google Scholar] [CrossRef]
- Willeumier, J.J.; van der Linden, Y.M.; van der Wal, C.; Jutte, P.C.; van der Velden, J.M.; Smolle, M.A.; van der Zwaal, P.; Koper, P.; Bakri, L.; de Pree, I.; et al. An Easy-to-Use Prognostic Model for Survival Estimation for Patients with Symptomatic Long Bone Metastases. J. Bone Jt. Surg. Am. 2018, 100, 196–204. [Google Scholar] [CrossRef]
- Johansen, J.S.; Schultz, N.A.; Jensen, B.V. Plasma YKL-40: A potential new cancer biomarker? Future Oncol. 2009, 5, 1065–1082. [Google Scholar] [CrossRef]
- Simpson, R.J.; Hammacher, A.; Smith, D.K.; Matthews, J.M.; Ward, L.D. Interleukin-6: Structure-function relationships. Protein. Sci. 1997, 6, 929–955. [Google Scholar] [CrossRef]
- Brabek, J.; Jakubek, M.; Vellieux, F.; Novotny, J.; Kolar, M.; Lacina, L.; Szabo, P.; Strnadova, K.; Rosel, D.; Dvorankova, B.; et al. Interleukin-6: Molecule in the Intersection of Cancer, Ageing and COVID-19. Int. J. Mol. Sci. 2020, 21, 7937. [Google Scholar] [CrossRef]
- Zhao, T.; Su, Z.; Li, Y.; Zhang, X.; You, Q. Chitinase-3 like-protein-1 function and its role in diseases. Signal. Transduct. Target. Ther. 2020, 5, 201. [Google Scholar] [CrossRef]
- Yeo, I.J.; Lee, C.K.; Han, S.B.; Yun, J.; Hong, J.T. Roles of chitinase 3-like 1 in the development of cancer, neurodegenerative diseases, and inflammatory diseases. Pharmacol. Ther. 2019, 203, 107394. [Google Scholar] [CrossRef]
- Libreros, S.; Iragavarapu-Charyulu, V. YKL-40/CHI3L1 drives inflammation on the road of tumor progression. J. Leukoc Biol. 2015, 98, 931–936. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Zhang, S.; Wang, Q.; Zhang, X. Tumor-recruited M2 macrophages promote gastric and breast cancer metastasis via M2 macrophage-secreted CHI3L1 protein. J. Hematol. Oncol. 2017, 10, 36. [Google Scholar] [CrossRef] [Green Version]
- Larionova, I.; Tuguzbaeva, G.; Ponomaryova, A.; Stakheyeva, M.; Cherdyntseva, N.; Pavlov, V.; Choinzonov, E.; Kzhyshkowska, J. Tumor-Associated Macrophages in Human Breast, Colorectal, Lung, Ovarian and Prostate Cancers. Front. Oncol. 2020, 10, 566511. [Google Scholar] [CrossRef]
- Vainer, N.; Dehlendorff, C.; Johansen, J.S. Systematic literature review of IL-6 as a biomarker or treatment target in patients with gastric, bile duct, pancreatic and colorectal cancer. Oncotarget 2018, 9, 29820–29841. [Google Scholar] [CrossRef] [Green Version]
- Bian, B.; Li, L.; Yang, J.; Liu, Y.; Xie, G.; Zheng, Y.; Zeng, L.; Zeng, J.; Shen, L. Prognostic value of YKL-40 in solid tumors: A meta-analysis of 41 cohort studies. Cancer Cell Int. 2019, 19, 259. [Google Scholar] [CrossRef] [Green Version]
- Sorensen, M.S.; Hovgaard, T.B.; Hindso, K.; Petersen, M.M. Prognostic value of biochemical variables for survival after surgery for metastatic bone disease of the extremities. J. Surg. Oncol. 2017, 115, 442–448. [Google Scholar] [CrossRef]
- Sørensen, M.S.; Hindsø, K.; Horstmann, P.F.; Troelsen, A.; Dalsgaard, S.; Fog, T.; Zimnicki, T.; Petersen, M.M. Incidence of surgical interventions for metastatic bone disease in the extremities: A population-based cohort study. Acta Oncol. 2019, in press. [Google Scholar]
- Karnofsky, D.A.; Abelmann, W.H.; Craver, L.F.; Burchenal, J.H. The use of nitrogen mustards in the palliative treatment of carcinoma. Cancer 1948, 1, 634–656. [Google Scholar] [CrossRef]
- Wolters, U.; Wolf, T.; Stutzer, H.; Schroder, T. ASA classification and perioperative variables as predictors of postoperative outcome. Br. J. Anaesth. 1996, 77, 217–222. [Google Scholar] [CrossRef]
- Knudsen, L.S.; Christensen, I.J.; Lottenburger, T.; Svendsen, M.N.; Nielsen, H.J.; Nielsen, L.; Horslev-Petersen, K.; Jensen, J.E.; Kollerup, G.; Johansen, J.S. Pre-analytical and biological variability in circulating interleukin 6 in healthy subjects and patients with rheumatoid arthritis. Biomarkers 2008, 13, 59–78. [Google Scholar] [CrossRef]
- Bojesen, S.E.; Johansen, J.S.; Nordestgaard, B.G. Plasma YKL-40 levels in healthy subjects from the general population. Clin. Chim. Acta 2011, 412, 709–712. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, M.S.; Hindso, K.; Hovgaard, T.B.; Petersen, M.M. Extent of Surgery Does Not Influence 30-Day Mortality in Surgery for Metastatic Bone Disease: An Observational Study of a Historical Cohort. Medicine 2016, 95, e3354. [Google Scholar] [CrossRef] [PubMed]
- Ganapathi, M.K.; May, L.T.; Schultz, D.; Brabenec, A.; Weinstein, J.; Sehgal, P.B.; Kushner, I. Role of interleukin-6 in regulating synthesis of C-reactive protein and serum amyloid A in human hepatoma cell lines. Biochem. Biophys. Res. Commun. 1988, 157, 271–277. [Google Scholar] [CrossRef]
- Tsiridis, E.; Upadhyay, N.; Giannoudis, P. Molecular aspects of fracture healing: Which are the important molecules? Injury 2007, 38 (Suppl. 1), S11–S25. [Google Scholar] [CrossRef]
- Pal, M.; Febbraio, M.A.; Whitham, M. From cytokine to myokine: The emerging role of interleukin-6 in metabolic regulation. Immunol. Cell Biol. 2014, 92, 331–339. [Google Scholar] [CrossRef]
- Varady, N.H.; Ameen, B.T.; Chen, A.F. Is Delayed Time to Surgery Associated with Increased Short-term Complications in Patients with Pathologic Hip Fractures? Clin. Orthop. Relat. Res. 2020, 478, 607–615. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Median (IQR) or n (%) |
|---|---|
| Age, years | 66 (58, 74) |
| Female gender | 114 (49.1%) |
| Cancer: | |
| Slow growing | 73 (31.6%) |
| Moderate growing | 61 (26.4%) |
| Fast growing | 97 (42.0%) |
| Cancer type (5 most comment) | |
| Breast | 50 (22%) |
| Lung | 46 (20%) |
| Renal | 34 (15%) |
| Prostate | 25 (11%) |
| Myeloma | 23 (10%) |
| Hemoglobin, mmol/L | 7.20 mmol/L (6.50, 8.03) |
| Leucocyte count × 109 | 7.90 (5.70, 10.20) |
| Neutrophil count × 109 | 5.80 (4.00, 7.50) |
| C-reactive protein, mg/L | 29 (7, 67) |
| Alkaline phosphatase, U/L | 116 (79, 169) |
| YKL-40, µg/L | 131.00 (68, 262) |
| IL-6, ng/L | 11.75 ng/L (4.57, 27.60) |
| Fracture | 163 (70.3%) |
| Karnofsky < 70 | 94 (40.9%) |
| ASA group 3 + 4 | 131 (56.7%) |
| Ischemic heart disease (EF < 45%) | 16 (6.9%) |
| Diabetes | 29 (12.5%) |
| Multiple metastatic lesions (visceral + bone) | 190 (81.9%) |
| Visceral metastases present | 107 (46.1%) |
| Lower extremity | 190 (81.9%) |
| Plasma YKL-40 | Plasma IL-6 | |||
|---|---|---|---|---|
| Median (µg/L) (IQR) | p-Value * | Median (ng/L)(IQR) | p-Value * | |
| Solitary lesion (n = 42) | 81 (50, 156) | 0.002 | 7.65 (2.23, 20.30) | 0.011 |
| Multiple lesions (n = 190) | 143 (74, 290) | 12.85 (5.30, 29.28) | ||
| ASA 1 + 2 (n = 100) | 89 (51, 197) | <0.001 | 9.05 (3.20, 22.60) | 0.005 |
| ASA 3 + 4 (n = 131) | 155 (84, 296) | 16.60 (6.20, 29.10) | ||
| Slow growing cancer (n = 73) | 116 (60, 206) | 0.078 | 7.10 (2.90, 15.40) | <0.001 |
| Moderate growing cancer (n = 61) | 138 (69, 316) | 20.80 (6.20, 31.80) | ||
| Fast growing cancer (n = 97) | 144 (77, 291) | 12.90 (6.10, 27.50) | ||
| Variable | Type | HR | 2.5% | 97.5% | p | Reference |
|---|---|---|---|---|---|---|
| Age | Cat. | 1.38 | 1.02 | 1.85 | 0.03 | <66 year |
| Gender | Cat | 1.22 | 0.91 | 1.64 | 0.19 | Female |
| Moderate growing cancer | Cat | 1.28 | 0.84 | 1.94 | <0.01 | Slow growing cancer |
| Fast growing cancer | Cat | 3.14 | 2.17 | 4.53 | <0.001 | Slow growing cancer |
| Hemoglobin | Cont | 0.34 | 0.19 | 0.62 | <0.01 | |
| Leucocytes | Cont | 1.43 | 1.11 | 1.83 | <0.01 | |
| Neutrophils | Cont | 1.34 | 1.08 | 1.65 | 0.01 | |
| CRP | Cont | 1.20 | 1.12 | 1.29 | <0.01 | |
| Alkaline Phosphatase | Cont | 1.28 | 1.11 | 1.48 | <0.01 | |
| YKL-40 | Cont | 1.25 | 1.15 | 1.37 | <0.01 | |
| Age-adjusted YKL-40 (>median) | Cat | 1.59 | 1.10 | 2.32 | 0.01 | 89 µg/L |
| IL-6 | Cont | 1.26 | 1.16 | 1.37 | <0.01 | |
| IL-6 (> median) | Cat | 1.99 | 1.47 | 2.68 | <0.01 | 11.8 ng/L |
| Fracture | Cat | 1.92 | 1.37 | 2.71 | <0.01 | Impending fracture |
| Karnofsky score | Cat | 2.61 | 1.92 | 3.56 | <0.01 | Below 70 |
| ASA | Cat | 2.30 | 1.68 | 3.16 | <0.01 | 1 + 2 |
| Ischemic heart disease | Cat | 1.29 | 0.75 | 2.24 | 0.37 | EF < 45% |
| Diabetes | Cat | 0.97 | 0.62 | 1.52 | 0.89 | No |
| Multiple metastatic sites | Cat | 3.21 | 1.98 | 5.21 | <0.01 | None |
| Visceral metastasis | Cat | 2.48 | 1.83 | 3.35 | <0.01 | None |
| Lower extremity | Cat | 1.48 | 0.99 | 2.22 | 0.05 | Upper extremity |
| Variable | Category | HR | 2.5% | 97.5% | p | Reference |
|---|---|---|---|---|---|---|
| Age above 66 years | Categorical | 1.22 | 0.86 | 1.72 | 0.27 | <66 year |
| Moderate growing cancer | Categorical | 1.21 | 0.75 | 1.96 | 0.44 | Female |
| Fast growing cancer | Categorical | 2.80 | 1.80 | 4.37 | <0.01 | Slow growing cancer |
| Hemoglobin (mmol/l) | Continuous | 0.74 | 0.32 | 1.67 | 0.46 | Slow growing cancer |
| Leucocyte count | Continuous | 1.00 | 0.34 | 2.98 | 1.00 | |
| Neutrophile count | Continuous | 1.31 | 0.51 | 3.34 | 0.57 | |
| C-reactive protein (mg/L) | Continuous | 0.99 | 0.88 | 1.12 | 0.86 | |
| Alkaline Phosphatase (U/L) | Continuous | 0.94 | 0.78 | 1.14 | 0.55 | |
| YKL-40 (µg/L) | Continuous | 0.94 | 0.82 | 1.08 | 0.39 | |
| IL-6 (ng/L) | Continuous | 1.24 | 1.08 | 1.43 | <0.01 | |
| Fracture | Categorical | 1.69 | 1.12 | 2.55 | 0.01 | Impending |
| Karnofsky score | Categorical | 2.22 | 1.51 | 3.26 | 0.00 | Below 70 |
| ASA classification | Categorical | 1.11 | 0.76 | 1.62 | 0.60 | 1 + 2 |
| Multiple metastatic lesions | Categorical | 2.86 | 1.59 | 5.16 | <0.01 | No |
| Visceral metastasis present | Categorical | 1.56 | 1.07 | 2.27 | 0.02 | None |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sørensen, M.S.; Colding-Rasmussen, T.; Horstmann, P.F.; Hindsø, K.; Dehlendorff, C.; Johansen, J.S.; Petersen, M.M. Pretreatment Plasma IL-6 and YKL-40 and Overall Survival after Surgery for Metastatic Bone Disease of the Extremities. Cancers 2021, 13, 2833. https://doi.org/10.3390/cancers13112833
Sørensen MS, Colding-Rasmussen T, Horstmann PF, Hindsø K, Dehlendorff C, Johansen JS, Petersen MM. Pretreatment Plasma IL-6 and YKL-40 and Overall Survival after Surgery for Metastatic Bone Disease of the Extremities. Cancers. 2021; 13(11):2833. https://doi.org/10.3390/cancers13112833
Chicago/Turabian StyleSørensen, Michala Skovlund, Thomas Colding-Rasmussen, Peter Frederik Horstmann, Klaus Hindsø, Christian Dehlendorff, Julia Sidenius Johansen, and Michael Mørk Petersen. 2021. "Pretreatment Plasma IL-6 and YKL-40 and Overall Survival after Surgery for Metastatic Bone Disease of the Extremities" Cancers 13, no. 11: 2833. https://doi.org/10.3390/cancers13112833
APA StyleSørensen, M. S., Colding-Rasmussen, T., Horstmann, P. F., Hindsø, K., Dehlendorff, C., Johansen, J. S., & Petersen, M. M. (2021). Pretreatment Plasma IL-6 and YKL-40 and Overall Survival after Surgery for Metastatic Bone Disease of the Extremities. Cancers, 13(11), 2833. https://doi.org/10.3390/cancers13112833