
A Molecular Signature of Circulating MicroRNA Can Predict Osteolytic Bone Disease in Multiple Myeloma

 , ,
, ,  ,
,  , ,
, ,  ,
,  , and
, and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Biological Material
2.3. miRNA Isolation and First-Strand cDNA Synthesis
2.4. Circulating miRNA Detection Using Quantitative PCR (qPCR)
2.5. Biostatistical Analysis
3. Results
3.1. Baseline Clinical Characteristics of MM Patients
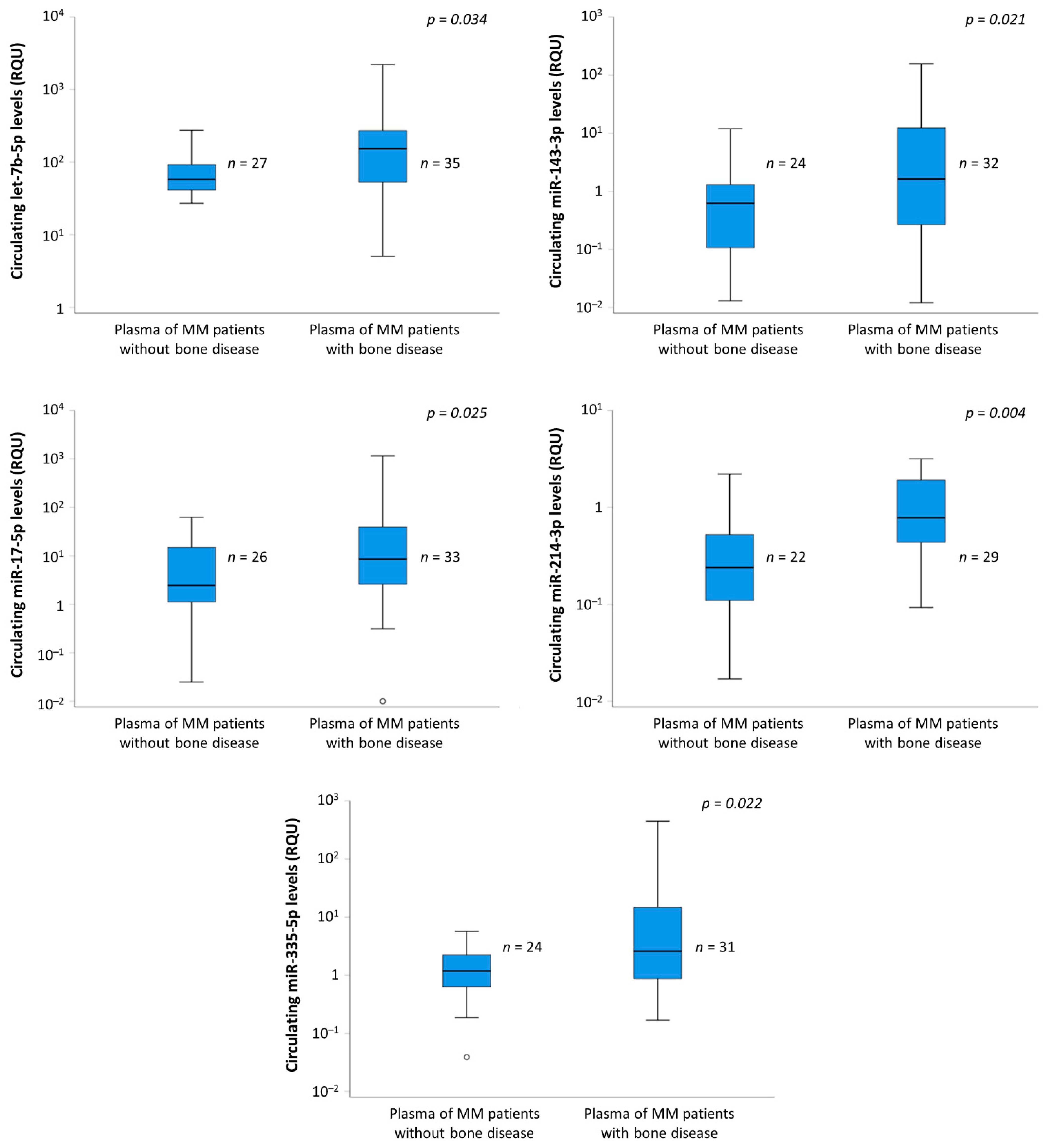
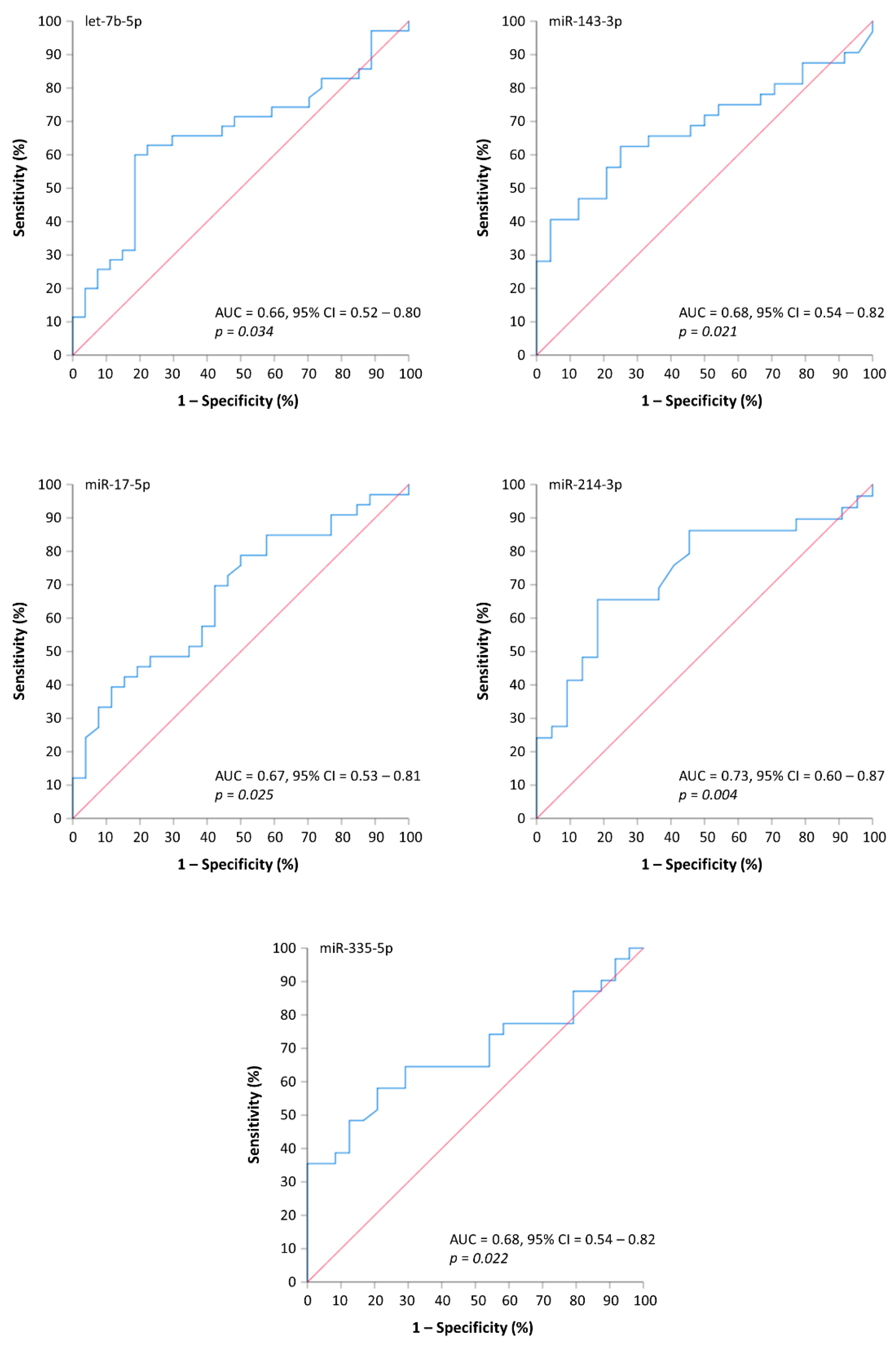
3.2. Circulating miRNAs Can Distinguish MM Patients with Osteolytic Bone Disease
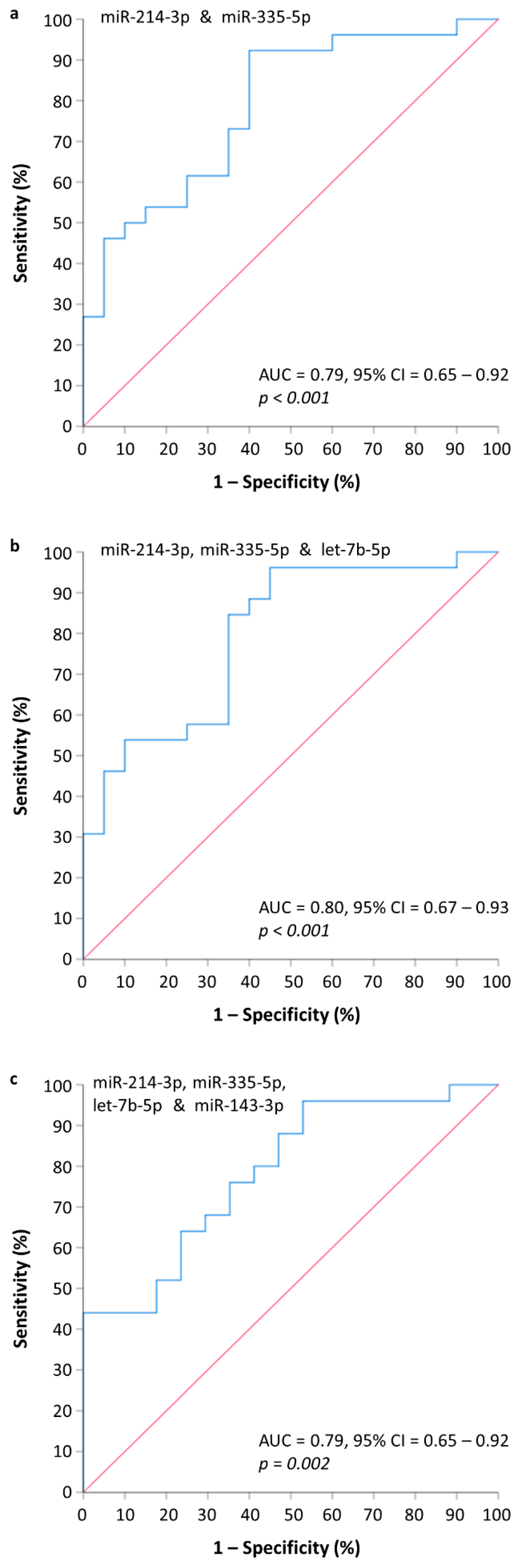
3.3. Construction and Evaluation of an MMBD-Predictive miRNA Model
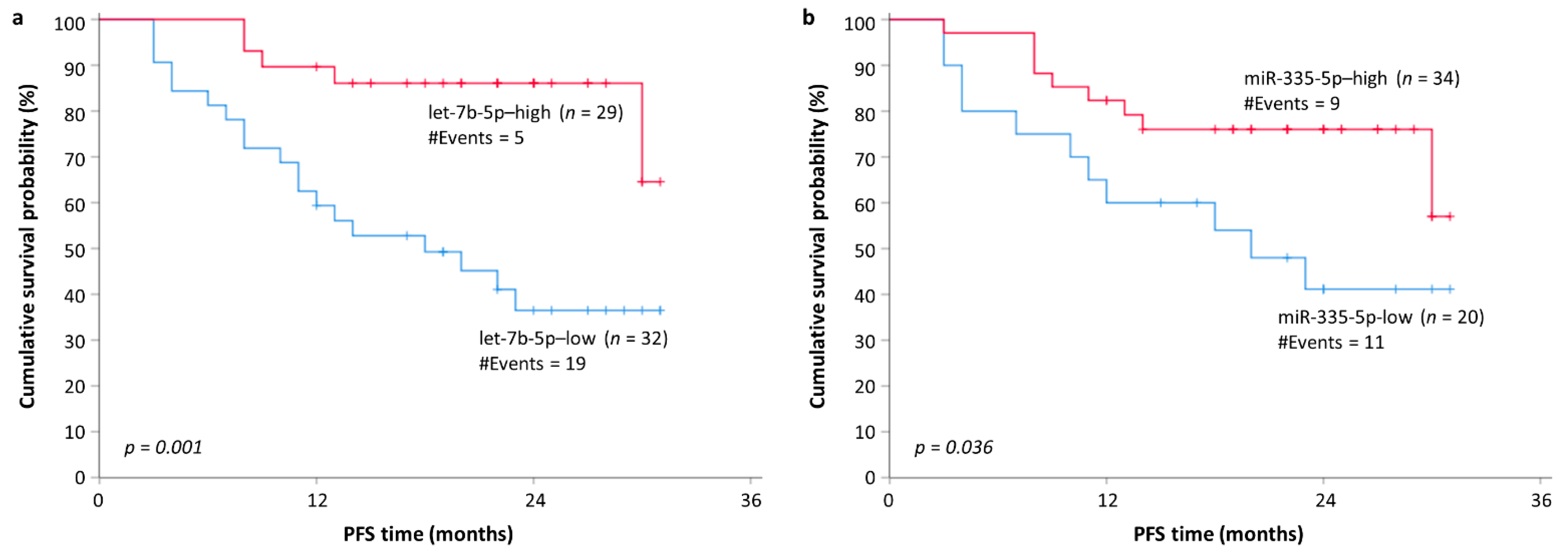
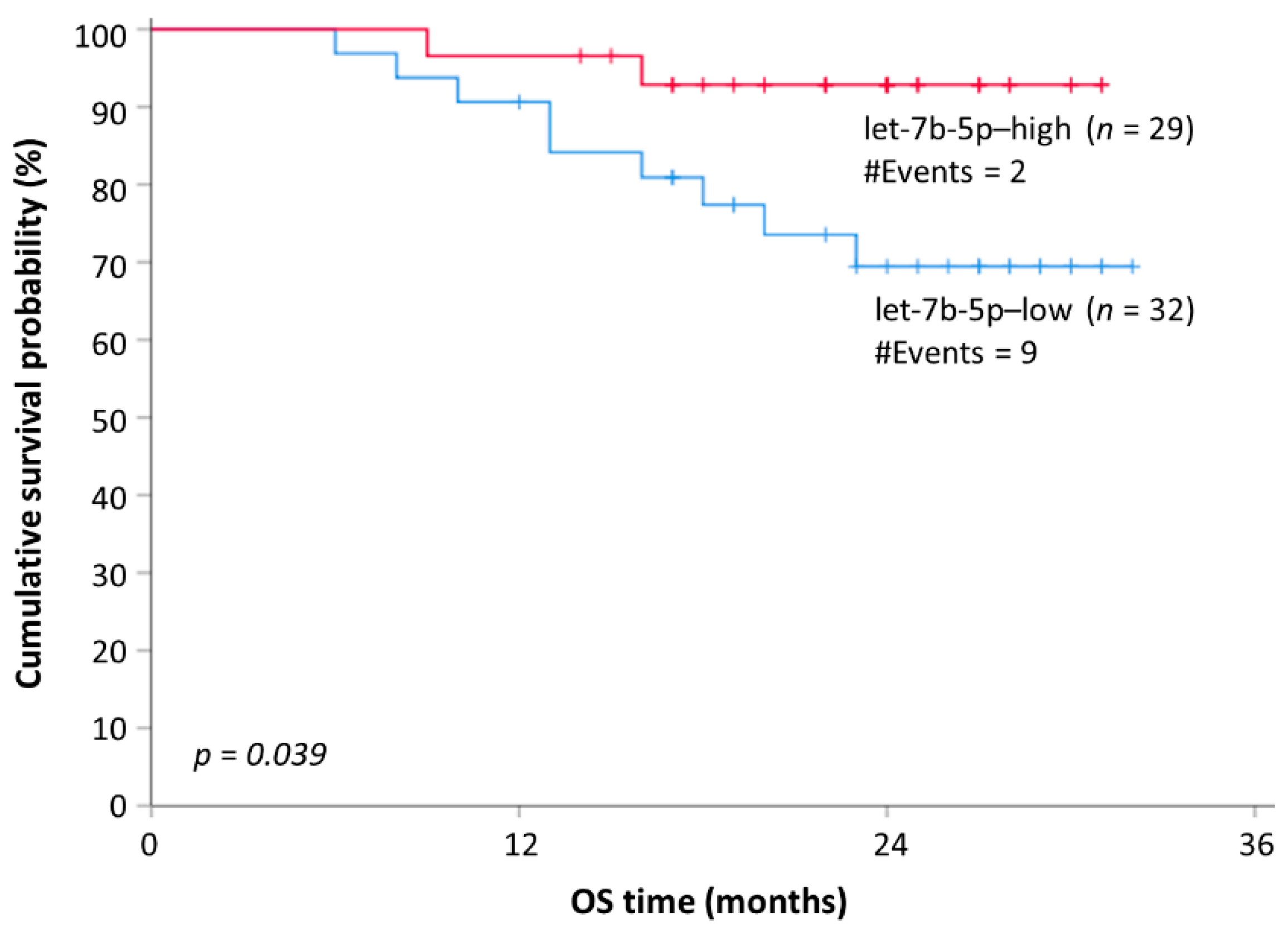
3.4. Evaluating the Prognostic Role of the MMBD-Specific miRNAs in MM
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rajkumar, S.V.; Dimopoulos, M.A.; Palumbo, A.; Blade, J.; Merlini, G.; Mateos, M.V.; Kumar, S.; Hillengass, J.; Kastritis, E.; Richardson, P.; et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014, 15, e538–e548. [Google Scholar] [CrossRef]
- Terpos, E.; Zamagni, E.; Lentzsch, S.; Drake, M.T.; Garcia-Sanz, R.; Abildgaard, N.; Ntanasis-Stathopoulos, I.; Schjesvold, F.; de la Rubia, J.; Kyriakou, C.; et al. Treatment of multiple myeloma-related bone disease: Recommendations from the Bone Working Group of the International Myeloma Working Group. Lancet Oncol. 2021, 22, e119–e130. [Google Scholar] [CrossRef]
- Hillengass, J.; Usmani, S.; Rajkumar, S.V.; Durie, B.G.M.; Mateos, M.V.; Lonial, S.; Joao, C.; Anderson, K.C.; Garcia-Sanz, R.; Riva, E.; et al. International myeloma working group consensus recommendations on imaging in monoclonal plasma cell disorders. Lancet Oncol. 2019, 20, e302–e312. [Google Scholar] [CrossRef]
- Gavriatopoulou, M.; Betaoultadaki, A.; Koutoulidis, V.; Ntanasis-Stathopoulos, I.; Bourgioti, C.; Malandrakis, P.; Fotiou, D.; Migkou, M.; Kanellias, N.; Eleutherakis-Papaiakovou, E.; et al. The Role of Low Dose Whole Body CT in the Detection of Progression of Patients with Smoldering Multiple Myeloma. Blood Cancer J. 2020, 10, 93. [Google Scholar] [CrossRef]
- Xiao, W.; Wang, Y.; Pacios, S.; Li, S.; Graves, D.T. Cellular and Molecular Aspects of Bone Remodeling. Front. Oral Biol. 2016, 18, 9–16. [Google Scholar] [CrossRef]
- Terpos, E.; Ntanasis-Stathopoulos, I.; Gavriatopoulou, M.; Dimopoulos, M.A. Pathogenesis of bone disease in multiple myeloma: From bench to bedside. Blood Cancer J. 2018, 8, 7. [Google Scholar] [CrossRef] [Green Version]
- Terpos, E.; Ntanasis-Stathopoulos, I.; Dimopoulos, M.A. Myeloma bone disease: From biology findings to treatment approaches. Blood 2019, 133, 1534–1539. [Google Scholar] [CrossRef] [Green Version]
- Terpos, E.; Christoulas, D.; Gavriatopoulou, M.; Dimopoulos, M.A. Mechanisms of bone destruction in multiple myeloma. Eur. J. Cancer Care 2017, 26, e12761. [Google Scholar] [CrossRef]
- Gebert, L.F.R.; MacRae, I.J. Regulation of microRNA function in animals. Nat. Rev. Mol. Cell Biol. 2019, 20, 21–37. [Google Scholar] [CrossRef]
- Sul, O.J.; Rajasekaran, M.; Park, H.J.; Suh, J.H.; Choi, H.S. MicroRNA-29b Enhances Osteoclast Survival by Targeting BCL-2-Modifying Factor after Lipopolysaccharide Stimulation. Oxid. Med. Cell. Longev. 2019, 2019, 6018180. [Google Scholar] [CrossRef]
- Wang, X.; Guo, B.; Li, Q.; Peng, J.; Yang, Z.; Wang, A.; Li, D.; Hou, Z.; Lv, K.; Kan, G.; et al. miR-214 targets ATF4 to inhibit bone formation. Nat. Med. 2013, 19, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Katsaraki, K.; Karousi, P.; Artemaki, P.I.; Scorilas, A.; Pappa, V.; Kontos, C.K.; Papageorgiou, S.G. MicroRNAs: Tiny Regulators of Gene Expression with Pivotal Roles in Normal B-Cell Development and B-Cell Chronic Lymphocytic Leukemia. Cancers 2021, 13, 593. [Google Scholar] [CrossRef] [PubMed]
- Pitari, M.R.; Rossi, M.; Amodio, N.; Botta, C.; Morelli, E.; Federico, C.; Gulla, A.; Caracciolo, D.; Di Martino, M.T.; Arbitrio, M.; et al. Inhibition of miR-21 restores RANKL/OPG ratio in multiple myeloma-derived bone marrow stromal cells and impairs the resorbing activity of mature osteoclasts. Oncotarget 2015, 6, 27343–27358. [Google Scholar] [CrossRef] [Green Version]
- Chen, B.; Yang, W.; Zhao, H.; Liu, K.; Deng, A.; Zhang, G.; Pan, K. Abnormal expression of miR-135b-5p in bone tissue of patients with osteoporosis and its role and mechanism in osteoporosis progression. Exp. Ther. Med. 2020, 19, 1042–1050. [Google Scholar] [CrossRef] [Green Version]
- Fan, F.Y.; Deng, R.; Lai, S.H.; Wen, Q.; Zeng, Y.; Gao, L.; Liu, Y.; Kong, P.; Zhong, J.; Su, Y.; et al. Inhibition of microRNA-221-5p induces osteogenic differentiation by directly targeting smad3 in myeloma bone disease mesenchymal stem cells. Oncol. Lett. 2019, 18, 6536–6544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohamad, N.; Nabih, E.S.; Zakaria, Z.M.; Nagaty, M.M.; Metwaly, R.G. Insight into the possible role of miR-214 in primary osteoporosis via osterix. J. Cell Biochem. 2019, 120, 15518–15526. [Google Scholar] [CrossRef]
- Papanota, A.M.; Karousi, P.; Kontos, C.K.; Ntanasis-Stathopoulos, I.; Scorilas, A.; Terpos, E. Multiple Myeloma Bone Disease: Implication of MicroRNAs in Its Molecular Background. Int. J. Mol. Sci. 2021, 22, 2375. [Google Scholar] [CrossRef]
- Weber, J.A.; Baxter, D.H.; Zhang, S.; Huang, D.Y.; Huang, K.H.; Lee, M.J.; Galas, D.J.; Wang, K. The microRNA spectrum in 12 body fluids. Clin. Chem. 2010, 56, 1733–1741. [Google Scholar] [CrossRef]
- Wang, K.; Zhang, S.; Weber, J.; Baxter, D.; Galas, D.J. Export of microRNAs and microRNA-protective protein by mammalian cells. Nucleic Acids Res. 2010, 38, 7248–7259. [Google Scholar] [CrossRef] [Green Version]
- Raposo, G.; Stoorvogel, W. Extracellular vesicles: Exosomes, microvesicles, and friends. J. Cell Biol. 2013, 200, 373–383. [Google Scholar] [CrossRef] [Green Version]
- Artemaki, P.I.; Scorilas, A.; Kontos, C.K. Circular RNAs: A New Piece in the Colorectal Cancer Puzzle. Cancers 2020, 12, 2464. [Google Scholar] [CrossRef]
- Karousi, P.; Artemaki, P.I.; Sotiropoulou, C.D.; Christodoulou, S.; Scorilas, A.; Kontos, C.K. Identification of Two Novel Circular RNAs Deriving from BCL2L12 and Investigation of Their Potential Value as a Molecular Signature in Colorectal Cancer. Int. J. Mol. Sci. 2020, 21, 8867. [Google Scholar] [CrossRef]
- Condrat, C.E.; Thompson, D.C.; Barbu, M.G.; Bugnar, O.L.; Boboc, A.; Cretoiu, D.; Suciu, N.; Cretoiu, S.M.; Voinea, S.C. miRNAs as Biomarkers in Disease: Latest Findings Regarding Their Role in Diagnosis and Prognosis. Cells 2020, 9, 276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawrie, C.H.; Gal, S.; Dunlop, H.M.; Pushkaran, B.; Liggins, A.P.; Pulford, K.; Banham, A.H.; Pezzella, F.; Boultwood, J.; Wainscoat, J.S.; et al. Detection of elevated levels of tumour-associated microRNAs in serum of patients with diffuse large B-cell lymphoma. Br. J. Haematol. 2008, 141, 672–675. [Google Scholar] [CrossRef] [PubMed]
- Artemaki, P.I.; Letsos, P.A.; Zoupa, I.C.; Katsaraki, K.; Karousi, P.; Papageorgiou, S.G.; Pappa, V.; Scorilas, A.; Kontos, C.K. The Multifaceted Role and Utility of MicroRNAs in Indolent B-Cell Non-Hodgkin Lymphomas. Biomedicines 2021, 9, 333. [Google Scholar] [CrossRef] [PubMed]
- Karousi, P.; Katsaraki, K.; Papageorgiou, S.G.; Pappa, V.; Scorilas, A.; Kontos, C.K. Identification of a novel tRNA-derived RNA fragment exhibiting high prognostic potential in chronic lymphocytic leukemia. Hematol. Oncol. 2019, 37, 498–504. [Google Scholar] [CrossRef]
- Katsaraki, K.; Adamopoulos, P.G.; Papageorgiou, S.G.; Pappa, V.; Scorilas, A.; Kontos, C.K. A 3’ tRNA-derived fragment produced by tRNA(LeuAAG) and tRNA(LeuTAG) is associated with poor prognosis in B-cell chronic lymphocytic leukemia, independently of classical prognostic factors. Eur. J. Haematol. 2021, 106, 821–830. [Google Scholar] [CrossRef] [PubMed]
- Karousi, P.; Adamopoulos, P.G.; Papageorgiou, S.G.; Pappa, V.; Scorilas, A.; Kontos, C.K. A novel, mitochondrial, internal tRNA-derived RNA fragment possesses clinical utility as a molecular prognostic biomarker in chronic lymphocytic leukemia. Clin. Biochem. 2020, 85, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Katsaraki, K.; Artemaki, P.I.; Papageorgiou, S.G.; Pappa, V.; Scorilas, A.; Kontos, C.K. Identification of a novel, internal tRNA-derived RNA fragment as a new prognostic and screening biomarker in chronic lymphocytic leukemia, using an innovative quantitative real-time PCR assay. Leuk. Res. 2019, 87, 106234. [Google Scholar] [CrossRef] [PubMed]
- Blondal, T.; Jensby Nielsen, S.; Baker, A.; Andreasen, D.; Mouritzen, P.; Wrang Teilum, M.; Dahlsveen, I.K. Assessing sample and miRNA profile quality in serum and plasma or other biofluids. Methods 2013, 59, S1–S6. [Google Scholar] [CrossRef]
- Artemaki, P.I.; Sklirou, A.D.; Kontos, C.K.; Liosi, A.A.; Gianniou, D.D.; Papadopoulos, I.N.; Trougakos, I.P.; Scorilas, A. High clusterin (CLU) mRNA expression levels in tumors of colorectal cancer patients predict a poor prognostic outcome. Clin. Biochem. 2020, 75, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Kalioraki, M.A.; Artemaki, P.I.; Sklirou, A.D.; Kontos, C.K.; Adamopoulos, P.G.; Papadopoulos, I.N.; Trougakos, I.P.; Scorilas, A. Heat shock protein beta 3 (HSPB3) is an unfavorable molecular biomarker in colorectal adenocarcinoma. Mol. Carcinog. 2020, 59, 116–125. [Google Scholar] [CrossRef]
- Camp, R.L.; Dolled-Filhart, M.; Rimm, D.L. X-tile: A new bio-informatics tool for biomarker assessment and outcome-based cut-point optimization. Clin. Cancer Res. 2004, 10, 7252–7259. [Google Scholar] [CrossRef] [Green Version]
- Artemaki, P.I.; Papatsirou, M.; Boti, M.A.; Adamopoulos, P.G.; Christodoulou, S.; Vassilacopoulou, D.; Scorilas, A.; Kontos, C.K. Revised Exon Structure of l-DOPA Decarboxylase (DDC) Reveals Novel Splice Variants Associated with Colorectal Cancer Progression. Int. J. Mol. Sci. 2020, 21, 8568. [Google Scholar] [CrossRef] [PubMed]
- Papatsirou, M.; Adamopoulos, P.G.; Artemaki, P.I.; Georganti, V.P.; Scorilas, A.; Vassilacopoulou, D.; Kontos, C.K. Next-generation sequencing reveals alternative L-DOPA decarboxylase (DDC) splice variants bearing novel exons, in human hepatocellular and lung cancer cells. Gene 2021, 768, 145262. [Google Scholar] [CrossRef]
- Goossens, N.; Nakagawa, S.; Sun, X.; Hoshida, Y. Cancer biomarker discovery and validation. Transl. Cancer Res. 2015, 4, 256–269. [Google Scholar] [CrossRef] [PubMed]
- Artemaki, P.I.; Kontos, C.K. Editorial for the Special Issue “Molecular Biomarkers in Colorectal Adenocarcinoma”. Int. J. Mol. Sci. 2021, 22, 2052. [Google Scholar] [CrossRef] [PubMed]
- Papatsirou, M.; Artemaki, P.I.; Scorilas, A.; Kontos, C.K. The role of circular RNAs in therapy resistance of patients with solid tumors. Per. Med. 2020, 17, 469–490. [Google Scholar] [CrossRef]
- Peng, Y.; Croce, C.M. The role of MicroRNAs in human cancer. Signal Transduct. Target. Ther. 2016, 1, 15004. [Google Scholar] [CrossRef] [Green Version]
- Califf, R.M. Biomarker definitions and their applications. Exp. Biol. Med. 2018, 243, 213–221. [Google Scholar] [CrossRef]
- Zen, K.; Zhang, C.Y. Circulating microRNAs: A novel class of biomarkers to diagnose and monitor human cancers. Med. Res. Rev. 2012, 32, 326–348. [Google Scholar] [CrossRef]
- Mitchell, P.S.; Parkin, R.K.; Kroh, E.M.; Fritz, B.R.; Wyman, S.K.; Pogosova-Agadjanyan, E.L.; Peterson, A.; Noteboom, J.; O’Briant, K.C.; Allen, A.; et al. Circulating microRNAs as stable blood-based markers for cancer detection. Proc. Natl. Acad. Sci. USA 2008, 105, 10513–10518. [Google Scholar] [CrossRef] [Green Version]
- Xiong, D.D.; Lv, J.; Wei, K.L.; Feng, Z.B.; Chen, J.T.; Liu, K.C.; Chen, G.; Luo, D.Z. A nine-miRNA signature as a potential diagnostic marker for breast carcinoma: An integrated study of 1110 cases. Oncol. Rep. 2017, 37, 3297–3304. [Google Scholar] [CrossRef] [Green Version]
- Zhu, B.; Ju, S.; Chu, H.; Shen, X.; Zhang, Y.; Luo, X.; Cong, H. The potential function of microRNAs as biomarkers and therapeutic targets in multiple myeloma. Oncol. Lett. 2018, 15, 6094–6106. [Google Scholar] [CrossRef]
- Hao, M.; Zang, M.; Zhao, L.; Deng, S.; Xu, Y.; Qi, F.; An, G.; Qin, Y.; Sui, W.; Li, F.; et al. Serum high expression of miR-214 and miR-135b as novel predictor for myeloma bone disease development and prognosis. Oncotarget 2016, 7, 19589–19600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, K.; Lu, J.; Zhao, Y.; Wang, L.; Li, J.; Qi, B.; Li, H.; Ma, C. MicroRNA-214 suppresses osteogenic differentiation of C2C12 myoblast cells by targeting Osterix. Bone 2013, 55, 487–494. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Ge, D.; Cao, X.; Ge, Y.; Chen, H.; Wang, W.; Zhang, H. MiR-214 Attenuates Osteogenic Differentiation of Mesenchymal Stem Cells via Targeting FGFR1. Cell Physiol. Biochem. 2016, 38, 809–820. [Google Scholar] [CrossRef] [PubMed]
- Zhao, C.; Sun, W.; Zhang, P.; Ling, S.; Li, Y.; Zhao, D.; Peng, J.; Wang, A.; Li, Q.; Song, J.; et al. miR-214 promotes osteoclastogenesis by targeting Pten/PI3k/Akt pathway. RNA Biol. 2015, 12, 343–353. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Yan, P.; Wang, J.; Zhang, Y.; Zhang, M.; Wang, Z.; Fu, Q.; Liang, W. Clinical significance of tumor miR-21, miR-221, miR-143, and miR-106a as biomarkers in patients with osteosarcoma. Int. J. Biol. Markers 2019, 34, 184–193. [Google Scholar] [CrossRef]
- Li, E.; Zhang, J.; Yuan, T.; Ma, B. MiR-143 suppresses osteogenic differentiation by targeting Osterix. Mol. Cell Biochem. 2014, 390, 69–74. [Google Scholar] [CrossRef]
- Wang, R.; Zhang, H.; Ding, W.; Fan, Z.; Ji, B.; Ding, C.; Ji, F.; Tang, H. miR-143 promotes angiogenesis and osteoblast differentiation by targeting HDAC7. Cell Death Dis. 2020, 11, 179. [Google Scholar] [CrossRef] [Green Version]
- He, X.; Zhu, L.; An, L.; Zhang, J. MiR-143 Inhibits Osteoclastogenesis by Targeting RANK and NF-kappaB and MAPK Signaling Pathways. Curr. Mol. Pharmacol. 2020, 13, 224–232. [Google Scholar] [CrossRef] [PubMed]
- Ma, W.; Dou, Q.; Ha, X. Let-7a-5p inhibits BMSCs osteogenesis in postmenopausal osteoporosis mice. Biochem. Biophys. Res. Commun. 2019, 510, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Papatsirou, M.; Artemaki, P.I.; Karousi, P.; Scorilas, A.; Kontos, C.K. Circular RNAs: Emerging Regulators of the Major Signaling Pathways Involved in Cancer Progression. Cancers 2021, 13, 2744. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Tu, Q.; Bonewald, L.F.; He, X.; Stein, G.; Lian, J.; Chen, J. Effects of miR-335-5p in modulating osteogenic differentiation by specifically downregulating Wnt antagonist DKK1. J. Bone Miner. Res. 2011, 26, 1953–1963. [Google Scholar] [CrossRef] [Green Version]
- Kocijan, R.; Muschitz, C.; Geiger, E.; Skalicky, S.; Baierl, A.; Dormann, R.; Plachel, F.; Feichtinger, X.; Heimel, P.; Fahrleitner-Pammer, A.; et al. Circulating microRNA Signatures in Patients With Idiopathic and Postmenopausal Osteoporosis and Fragility Fractures. J. Clin. Endocrinol. Metab. 2016, 101, 4125–4134. [Google Scholar] [CrossRef]
- Zarecki, P.; Hackl, M.; Grillari, J.; Debono, M.; Eastell, R. Serum microRNAs as novel biomarkers for osteoporotic vertebral fractures. Bone 2020, 130, 115105. [Google Scholar] [CrossRef]
- Fang, T.; Wu, Q.; Zhou, L.; Mu, S.; Fu, Q. miR-106b-5p and miR-17-5p suppress osteogenic differentiation by targeting Smad5 and inhibit bone formation. Exp. Cell Res. 2016, 347, 74–82. [Google Scholar] [CrossRef]
- Li, H.; Li, T.; Wang, S.; Wei, J.; Fan, J.; Li, J.; Han, Q.; Liao, L.; Shao, C.; Zhao, R.C. miR-17-5p and miR-106a are involved in the balance between osteogenic and adipogenic differentiation of adipose-derived mesenchymal stem cells. Stem Cell Res. 2013, 10, 313–324. [Google Scholar] [CrossRef] [Green Version]
- Wu, M.; Chen, G.; Li, Y.P. TGF-beta and BMP signaling in osteoblast, skeletal development, and bone formation, homeostasis and disease. Bone Res. 2016, 4, 16009. [Google Scholar] [CrossRef]
- Wang, R.; Lu, A.; Liu, W.; Yue, J.; Sun, Q.; Chen, J.; Luan, H.; Zhai, Y.; Li, B.; Jiang, Z.; et al. Searching for valuable differentially expressed miRNAs in postmenopausal osteoporosis by RNA sequencing. J. Obstet. Gynaecol. Res. 2020, 46, 1183–1192. [Google Scholar] [CrossRef]
- Xu, H.; Liu, C.; Zhang, Y.; Guo, X.; Liu, Z.; Luo, Z.; Chang, Y.; Liu, S.; Sun, Z.; Wang, X. Let-7b-5p regulates proliferation and apoptosis in multiple myeloma by targeting IGF1R. Acta Biochim. Biophys. Sin. 2014, 46, 965–972. [Google Scholar] [CrossRef] [Green Version]
- Manier, S.; Powers, J.T.; Sacco, A.; Glavey, S.V.; Huynh, D.; Reagan, M.R.; Salem, K.Z.; Moschetta, M.; Shi, J.; Mishima, Y.; et al. The LIN28B/let-7 axis is a novel therapeutic pathway in multiple myeloma. Leukemia 2017, 31, 853–860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manier, S.; Liu, C.J.; Avet-Loiseau, H.; Park, J.; Shi, J.; Campigotto, F.; Salem, K.Z.; Huynh, D.; Glavey, S.V.; Rivotto, B.; et al. Prognostic role of circulating exosomal miRNAs in multiple myeloma. Blood 2017, 129, 2429–2436. [Google Scholar] [CrossRef] [PubMed]
- Qi, J.; Shi, L.Y.; Wu, Y.; Shen, X.J.; Yuan, J.; Jin, C.J.; Cong, H.; Ju, S.Q. Epigenetic silencing of miR-335 induces migration by targeting insulin-like growth factor-1 receptor in multiple myeloma. Leuk. Lymphoma 2019, 60, 3188–3198. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Median (Range) |
|---|---|
| Age (years) | 62 (35–90) |
| OS 1 (months) | 24 (6–32) |
| PFS 2 (months) | 20 (3–31) |
| Number of Patients (%) | |
| Gender | |
| Male | 35 (56.5%) |
| Female | 27 (43.5%) |
| MM type | |
| IgA | 17 (27.5%) |
| IgG | 35 (56.5%) |
| IgD | 2 (3.2%) |
| κLC | 2 (3.2%) |
| λLC | 2 (3.2%) |
| NSMM 3 | 4 (6.4%) |
| ISS 4 | |
| I | 23 (37.1%) |
| II | 15 (24.2%) |
| III | 23 (37.1%) |
| Unavailable data | 1 (1.6%) |
| Revised ISS 4 (R-ISS) | |
| I | 18 (29.0%) |
| II | 25 (40.3%) |
| III | 12 (19.4%) |
| Unavailable data | 7 (11.3%) |
| B2M 5 | |
| ≤5.5 mg/L | 39 (62.9%) |
| >5.5 mg/L | 23 (37.1%) |
| LDH 6 | |
| Normal (≤225 U/L) | 49 (79.0%) |
| Elevated (>225 U/L) | 13 (21.0%) |
| ALP 7 | |
| Normal (≤129 U/L) | 59 (95.2%) |
| Elevated (>129 U/L) | 3 (4.8%) |
| Primary treatment of MM | |
| Bortezomib-based | 60 (96.8%) |
| IMiD-based 8 | 2 (3.2%) |
| HDM-ASCT 9 | |
| Yes | 38 (61.3%) |
| No | 24 (38.7%) |
| MMBD 10 | |
| Yes | 35 (56.5%) |
| No | 27 (43.5%) |
| SREs 11 (out of the 35 MMBD cases) | |
| Yes | 20 (57.1%) |
| No | 15 (42.9%) |
| BP 12 treatment | |
| Yes | 35 (56.5%) |
| No | 23 (37.0%) |
| Unavailable data | 4 (6.5%) |
| Covariate | OR 1 | 95% CI 2 | p Value 3 | BCa Bootstrap 95% CI 2 | Bootstrap p Value 3 |
|---|---|---|---|---|---|
| let-7b-5p levels | 3.13 | 1.04–9.44 | 0.043 | 1.86–14.30 | 0.044 |
| miR-143-3p levels | 1.86 | 1.07–3.23 | 0.029 | 1.14–4.13 | 0.020 |
| miR-17-5p levels | 1.89 | 1.01–3.54 | 0.048 | 1.07–4.62 | 0.052 |
| miR-214-3p levels | 3.07 | 1.15–8.21 | 0.025 | 1.28–20.49 | 0.032 |
| miR-335-5p levels | 3.24 | 1.23–8.51 | 0.017 | 1.57–10.70 | 0.004 |
| Variable (Tested vs. Control) | HR 1 | 95% CI 2 | p Value 3 | BCa Bootstrap 95% CI 2 | Bootstrap p Value 3 | |
|---|---|---|---|---|---|---|
| Univariate analysis | Age | 1.02 | 0.98–1.06 | 0.26 | 0.82–2.01 | 0.30 |
| R-ISS 4 | 1.58 | 0.89–2.83 | 0.12 | 0.93–2.88 | 0.097 | |
| B2M 5 (>5.5 mg/L vs. ≤5.5 mg/L) | 2.18 | 0.98–4.88 | 0.056 | 1.00–5.21 | 0.045 | |
| LDH 6 (elevated vs. normal) | 1.21 | 0.48–3.10 | 0.69 | 0.37–3.00 | 0.70 | |
| let-7b-5p (high vs. low) | 0.22 | 0.081–0.59 | 0.003 | 0.074–0.52 | 0.004 | |
| miR-335-5p (high vs. low) | 0.41 | 0.17–0.98 | 0.044 | 0.15–0.97 | 0.027 | |
| Multivariate analysis 7 | Age | 1.02 | 0.98–1.07 | 0.38 | 0.97–1.10 | 0.49 |
| R-ISS 4 | 1.23 | 0.42–3.54 | 0.71 | 0.32–5.64 | 0.70 | |
| B2M 5 (>5.5 mg/L vs. ≤5.5 mg/L) | 1.11 | 0.23–5.26 | 0.90 | 0.12–8.33 | 0.91 | |
| LDH 6 (elevated vs. normal) | 0.59 | 0.17–2.00 | 0.40 | 0.15–1.75 | 0.40 | |
| let-7b-5p (high vs. low) | 0.25 | 0.078–0.82 | 0.022 | 0.082–0.51 | 0.011 | |
| Age | 1.04 | 0.98–1.09 | 0.21 | 0.96–1.17 | 0.27 | |
| R-ISS 4 | 1.06 | 0.33–3.33 | 0.93 | 0.20–6.55 | 0.93 | |
| B2M 5 (>5.5 mg/L vs. ≤5.5 mg/L) | 2.61 | 0.51–13.29 | 0.25 | 0.26–34.81 | 0.30 | |
| LDH 6 (elevated vs. normal) | 0.67 | 0.19–2.43 | 0.56 | 0.13–2.31 | 0.54 | |
| miR-335-5p (high vs. low) | 0.31 | 0.11–0.85 | 0.024 | 0.098–0.55 | 0.021 |
| Variable (Tested vs. Control) | HR 1 | 95% CI 2 | p Value 3 | BCa Bootstrap 95% CI 2 | Bootstrap p Value 3 |
|---|---|---|---|---|---|
| Age | 1.02 | 0.97–1.08 | 0.46 | 0.97–1.08 | 0.38 |
| R-ISS 4 | 2.98 | 1.13–7.86 | 0.028 | 1.54–8.76 | 0.002 |
| B2M 5 (>5.5 mg/L vs. ≤5.5 mg/L) | 3.43 | 1.00–4.88 | 0.049 | 0.96–16.44 | 0.017 |
| LDH 6 (elevated vs. normal) | 2.04 | 0.59–6.98 | 0.26 | 0.40–7.31 | 0.21 |
| let-7b-5p (high vs. low) | 0.23 | 0.049–1.060 | 0.059 | 0.014–0.75 | 0.025 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papanota, A.-M.; Tsiakanikas, P.; Kontos, C.K.; Malandrakis, P.; Liacos, C.-I.; Ntanasis-Stathopoulos, I.; Kanellias, N.; Gavriatopoulou, M.; Kastritis, E.; Avgeris, M.; et al. A Molecular Signature of Circulating MicroRNA Can Predict Osteolytic Bone Disease in Multiple Myeloma. Cancers 2021, 13, 3877. https://doi.org/10.3390/cancers13153877
Papanota A-M, Tsiakanikas P, Kontos CK, Malandrakis P, Liacos C-I, Ntanasis-Stathopoulos I, Kanellias N, Gavriatopoulou M, Kastritis E, Avgeris M, et al. A Molecular Signature of Circulating MicroRNA Can Predict Osteolytic Bone Disease in Multiple Myeloma. Cancers. 2021; 13(15):3877. https://doi.org/10.3390/cancers13153877
Chicago/Turabian StylePapanota, Aristea-Maria, Panagiotis Tsiakanikas, Christos K. Kontos, Panagiotis Malandrakis, Christine-Ivy Liacos, Ioannis Ntanasis-Stathopoulos, Nikolaos Kanellias, Maria Gavriatopoulou, Efstathios Kastritis, Margaritis Avgeris, and et al. 2021. "A Molecular Signature of Circulating MicroRNA Can Predict Osteolytic Bone Disease in Multiple Myeloma" Cancers 13, no. 15: 3877. https://doi.org/10.3390/cancers13153877
APA StylePapanota, A. -M., Tsiakanikas, P., Kontos, C. K., Malandrakis, P., Liacos, C. -I., Ntanasis-Stathopoulos, I., Kanellias, N., Gavriatopoulou, M., Kastritis, E., Avgeris, M., Dimopoulos, M. -A., Scorilas, A., & Terpos, E. (2021). A Molecular Signature of Circulating MicroRNA Can Predict Osteolytic Bone Disease in Multiple Myeloma. Cancers, 13(15), 3877. https://doi.org/10.3390/cancers13153877