
Deep Learning Fast Screening Approach on Cytological Whole Slides for Thyroid Cancer Diagnosis

 , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. The Dataset
2.2. Methods
2.2.1. Whole Slide Image Processing
2.2.2. Proposed Convolution Network Architecture
2.2.3. Implementation details
3. Results
3.1. Evaluation Metrics
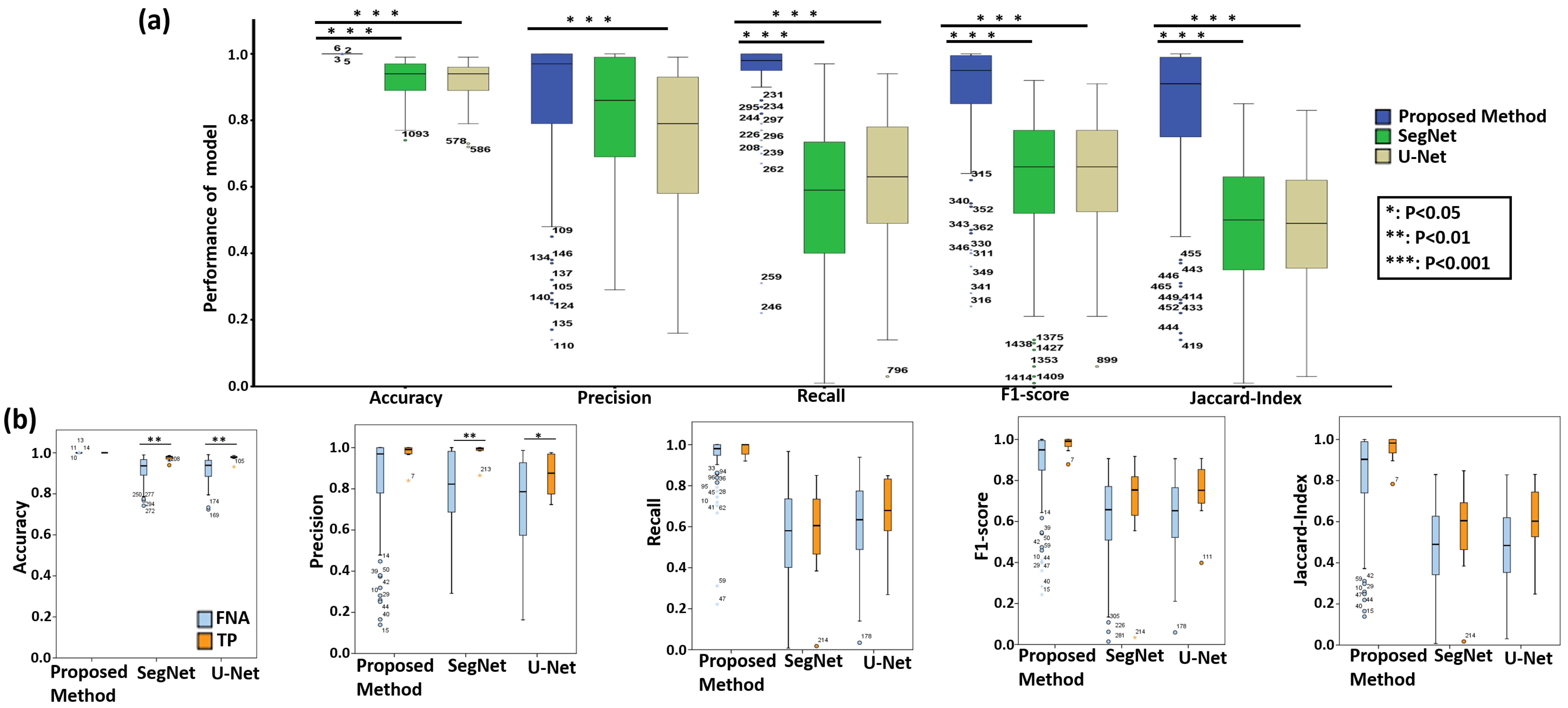
3.2. Quantitative Evaluation with Statistical Analysis
3.3. Run Time Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 145–164. [Google Scholar] [CrossRef] [Green Version]
- Bai, Y.; Kakudo, K.; Jung, C.K. Updates in the pathologic classification of thyroid neoplasms: A review of the world health organization classification. Endocrinol. Metab. 2020, 35, 696. [Google Scholar] [CrossRef] [PubMed]
- Limaiem, F.; Rehman, A.; Mazzoni, T. Cancer, Papillary Thyroid Carcinoma (PTC); StatPearls: Treasure Island, FL, USA, 2020. [Google Scholar]
- Kini, S.; Miller, J.; Hamburger, J.; Smith, M. Cytopathology of papillary carcinoma of the thyroid by fine needle aspiration. Acta Cytol. 1980, 24, 511–521. [Google Scholar]
- Akhtar, M.; Ali, M.A.; Huq, M.; Bakry, M. Fxine-needle aspiration biopsy of papillary thyroid carcinoma: Cytologic, histologic, and ultrastructural correlations. Diagn. Cytopathol. 1991, 7, 373–379. [Google Scholar] [CrossRef]
- Sidawy, M.K.; Vecchio, D.M.D.; Knoll, S.M. Fine-needle aspiration of thyroid nodules: Correlation between cytology and histology and evaluation of discrepant cases. Cancer Cytopathol. Interdiscip. Int. J. Am. Cancer Soc. 1997, 81, 253–259. [Google Scholar] [CrossRef]
- Cibas, E.S.; Ali, S.Z. The 2017 Bethesda system for reporting thyroid cytopathology. Thyroid 2017, 27, 1341–1346. [Google Scholar] [CrossRef]
- Kini, S. Guides to clinical aspiration biopsy: Thyroid. In Thyroid Adequacy Criteria and Thinprep; Igaku-Shoin: New York, NY, USA, 1996. [Google Scholar]
- Kumar, S.; Singh, N.; Siddaraju, N. “Cellular swirls” and similar structures on fine needle aspiration cytology as diagnostic clues to papillary thyroid carcinoma: A report of 4 cases. Acta Cytol. 2010, 54, 939–942. [Google Scholar]
- Mukhopadhyay, S.; Feldman, M.D.; Abels, E.; Ashfaq, R.; Beltaifa, S.; Cacciabeve, N.G.; Cathro, H.P.; Cheng, L.; Cooper, K.; Dickey, G.E.; et al. Whole slide imaging versus microscopy for primary diagnosis in surgical pathology: A multicenter blinded randomized noninferiority study of 1992 cases (pivotal study). Am. J. Surg. Pathol. 2018, 42, 39. [Google Scholar] [CrossRef]
- Yu, K.H.; Beam, A.L.; Kohane, I.S. Artificial intelligence in healthcare. Nat. Biomed. Eng. 2018, 2, 719–731. [Google Scholar] [CrossRef]
- Syrykh, C.; Abreu, A.; Amara, N.; Siegfried, A.; Maisongrosse, V.; Frenois, F.X.; Martin, L.; Rossi, C.; Laurent, C.; Brousset, P. Accurate diagnosis of lymphoma on whole-slide histopathology images using deep learning. NPJ Digit. Med. 2020, 3, 1–8. [Google Scholar] [CrossRef]
- De Fauw, J.; Ledsam, J.R.; Romera-Paredes, B.; Nikolov, S.; Tomasev, N.; Blackwell, S.; Askham, H.; Glorot, X.; O’Donoghue, B.; Visentin, D.; et al. Clinically applicable deep learning for diagnosis and referral in retinal disease. Nat. Med. 2018, 24, 1342–1350. [Google Scholar] [CrossRef]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Correction: Corrigendum: Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 546, 686. [Google Scholar] [CrossRef]
- Chen, P.J.; Lin, M.C.; Lai, M.J.; Lin, J.C.; Lu, H.H.S.; Tseng, V.S. Accurate classification of diminutive colorectal polyps using computer-aided analysis. Gastroenterology 2018, 154, 568–575. [Google Scholar] [CrossRef]
- Hannun, A.Y.; Rajpurkar, P.; Haghpanahi, M.; Tison, G.H.; Bourn, C.; Turakhia, M.P.; Ng, A.Y. Cardiologist-level arrhythmia detection and classification in ambulatory electrocardiograms using a deep neural network. Nat. Med. 2019, 25, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Titano, J.J.; Badgeley, M.; Schefflein, J.; Pain, M.; Su, A.; Cai, M.; Swinburne, N.; Zech, J.; Kim, J.; Bederson, J.; et al. Automated deep-neural-network surveillance of cranial images for acute neurologic events. Nat. Med. 2018, 24, 1337–1341. [Google Scholar] [CrossRef]
- Durstewitz, D.; Koppe, G.; Meyer-Lindenberg, A. Deep neural networks in psychiatry. Mol. Psychiatry 2019, 24, 1583–1598. [Google Scholar] [CrossRef]
- Lee, H.; Yune, S.; Mansouri, M.; Kim, M.; Tajmir, S.H.; Guerrier, C.E.; Ebert, S.A.; Pomerantz, S.R.; Romero, J.M.; Kamalian, S.; et al. An explainable deep-learning algorithm for the detection of acute intracranial haemorrhage from small datasets. Nat. Biomed. Eng. 2019, 3, 173–182. [Google Scholar] [CrossRef]
- Hazlett, H.C.; Gu, H.; Munsell, B.C.; Kim, S.H.; Styner, M.; Wolff, J.J.; Elison, J.T.; Swanson, M.R.; Zhu, H.; Botteron, K.N.; et al. Early brain development in infants at high risk for autism spectrum disorder. Nature 2017, 542, 348–351. [Google Scholar] [CrossRef]
- Courtiol, P.; Maussion, C.; Moarii, M.; Pronier, E.; Pilcer, S.; Sefta, M.; Manceron, P.; Toldo, S.; Zaslavskiy, M.; Le Stang, N.; et al. Deep learning-based classification of mesothelioma improves prediction of patient outcome. Nat. Med. 2019, 25, 1519–1525. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Tsuzuki, T.; Akatsuka, J.; Ueki, M.; Morikawa, H.; Numata, Y.; Takahara, T.; Tsuyuki, T.; Tsutsumi, K.; Nakazawa, R.; et al. Automated acquisition of explainable knowledge from unannotated histopathology images. Nat. Commun. 2019, 10, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Chen, P.; McGough, M.; Xing, F.; Wang, C.; Bui, M.; Xie, Y.; Sapkota, M.; Cui, L.; Dhillon, J.; et al. Pathologist-level interpretable whole-slide cancer diagnosis with deep learning. Nat. Mach. Intell. 2019, 1, 236–245. [Google Scholar] [CrossRef]
- Sanyal, P.; Mukherjee, T.; Barui, S.; Das, A.; Gangopadhyay, P. Artificial intelligence in cytopathology: A neural network to identify papillary carcinoma on thyroid fine-needle aspiration cytology smears. J. Pathol. Inform. 2018, 9, 43. [Google Scholar] [PubMed]
- Ke, W.; Wang, Y.; Wan, P.; Liu, W.; Li, H. An Ultrasonic Image Recognition Method for Papillary Thyroid Carcinoma Based on Depth Convolution Neural Network. In International Conference on Neural Information Processing; Springer: Berlin/Heidelberg, Germany, 2017; pp. 82–91. [Google Scholar]
- Ren, S.; He, K.; Girshick, R.; Sun, J. Faster R-CNN: Towards Real-Time Object Detection with Region Proposal Networks. IEEE Trans. Pattern Anal. Mach. Intell. 2017, 39, 1137–1149. [Google Scholar] [CrossRef] [Green Version]
- Falk, T.; Mai, D.; Bensch, R.; Çiçek, Ö.; Abdulkadir, A.; Marrakchi, Y.; Böhm, A.; Deubner, J.; Jäckel, Z.; Seiwald, K.; et al. U-Net: Deep learning for cell counting, detection, and morphometry. Nat. Methods 2019, 16, 67–70. [Google Scholar] [CrossRef]
- Badrinarayanan, V.; Kendall, A.; Cipolla, R. Segnet: A deep convolutional encoder-decoder architecture for image segmentation. IEEE Trans. Pattern Anal. Mach. Intell. 2017, 39, 2481–2495. [Google Scholar] [CrossRef]
- Shelhamer, E.; Long, J.; Darrell, T. Fully convolutional networks for semantic segmentation. IEEE Trans. Pattern Anal. Mach. Intell. 2017, 39, 640–651. [Google Scholar] [CrossRef]
- Signaevsky, M.; Prastawa, M.; Farrell, K.; Tabish, N.; Baldwin, E.; Han, N.; Iida, M.A.; Koll, J.; Bryce, C.; Purohit, D.; et al. Artificial intelligence in neuropathology: Deep learning-based assessment of tauopathy. Lab. Investig. 2019, 99, 1019. [Google Scholar] [CrossRef] [PubMed]
- Naylor, P.; Laé, M.; Reyal, F.; Walter, T. Segmentation of nuclei in histopathology images by deep regression of the distance map. IEEE Trans. Med. Imaging 2018, 38, 448–459. [Google Scholar] [CrossRef]
- Zhu, R.; Sui, D.; Qin, H.; Hao, A. An extended type cell detection and counting method based on FCN. In Proceedings of the 2017 IEEE 17th International Conference on Bioinformatics and Bioengineering (BIBE), Washington, DC, USA, 23–25 October 2017; pp. 51–56. [Google Scholar]
- Gupta, D.; Jhunjhunu Wala, R.; Juston, M.; MC, J. Image Segmentation Keras: Implementation of Segnet, FCN, UNet, PSPNet and Other Models in Keras. Available online: https://github.com/divamgupta/image-segmentation-keras (accessed on 15 October 2020).
- Steiner, D.F.; MacDonald, R.; Liu, Y.; Truszkowski, P.; Hipp, J.D.; Gammage, C.; Thng, F.; Peng, L.; Stumpe, M.C. Impact of deep learning assistance on the histopathologic review of lymph nodes for metastatic breast cancer. Am. J. Surg. Pathol. 2018, 42, 1636. [Google Scholar] [CrossRef]
- Sakamoto, T.; Furukawa, T.; Lami, K.; Pham, H.H.N.; Uegami, W.; Kuroda, K.; Kawai, M.; Sakanashi, H.; Cooper, L.A.D.; Bychkov, A.; et al. A narrative review of digital pathology and artificial intelligence: Focusing on lung cancer. Transl. Lung Cancer Res. 2020, 9, 2255. [Google Scholar] [CrossRef] [PubMed]
- Bera, K.; Schalper, K.A.; Rimm, D.L.; Velcheti, V.; Madabhushi, A. Artificial intelligence in digital pathology—New tools for diagnosis and precision oncology. Nat. Rev. Clin. Oncol. 2019, 16, 703–715. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Layer | Features (Train) | Features (Inference) | Kernel Size | Stride |
|---|---|---|---|---|
| Input | 512 × 512 × 3 | 512 × 512 × 3 | - | - |
| Padding | 712 × 712 × 3 | 712 × 712 × 3 | - | - |
| Conv1_1 + relu1_1 | 710 × 710 × 64 | 710 × 710 × 64 | 3 × 3 | 1 |
| Conv1_2 + relu1_2 | 710 × 710 × 64 | 710 × 710 × 64 | 3 × 3 | 1 |
| Pool1 | 355 × 355 × 64 | 355 × 355 × 64 | 2 × 2 | 2 |
| Conv2_1 + relu2_1 | 355 × 355 × 128 | 355 × 355 × 128 | 3 × 3 | 1 |
| Conv2_2 + relu2_2 | 355 × 355 × 128 | 355 × 355 × 128 | 3 × 3 | 1 |
| Pool2 | 178 × 178 × 128 | 178 × 178 × 128 | 2 × 2 | 2 |
| Conv3_1 + relu3_1 | 178 × 178 × 256 | 178 × 178 × 256 | 3 × 3 | 1 |
| Conv3_2 + relu3_2 | 178 × 178 × 256 | 178 × 178 × 256 | 3 × 3 | 1 |
| Conv3_3 + relu3_3 | 178 × 178 × 256 | 178 × 178 × 256 | 3 × 3 | 1 |
| Pool3 | 89 × 89 × 256 | 89 × 89 × 256 | 2 × 2 | 2 |
| Conv4_1 + relu4_1 | 89 × 89 × 512 | 89 × 89 × 512 | 3 × 3 | 1 |
| Conv4_2 + relu4_2 | 89 × 89 × 512 | 89 × 89 × 512 | 3 × 3 | 1 |
| Conv4_3 + relu4_3 | 89 × 89 × 512 | 89 × 89 × 512 | 3 × 3 | 1 |
| Pool4 | 45 × 45 × 512 | 45 × 45 × 512 | 2 × 2 | 2 |
| Conv5_1 + relu5_1 | 45 × 45 × 512 | 45 × 45 × 512 | 3 × 3 | 1 |
| Conv5_2 + relu5_2 | 45 × 45 × 512 | 45 × 45 × 512 | 3 × 3 | 1 |
| Conv5_3 + relu5_3 | 45 × 45 × 512 | 45 × 45 × 512 | 3 × 3 | 1 |
| Pool5 | 23 × 23 × 512 | 23 × 23 × 512 | 2 × 2 | 2 |
| Conv6 + relu6 + Drop6 | 17 × 17 × 4096 | 17 × 17 × 4096 | 7 × 7 | 1 |
| Conv7 + relu7 + Drop7 | 17 × 17 × 4096 | 17 × 17 × 4096 | 1 × 1 | 1 |
| Conv8 | 17 × 17 × 3 | 17 × 17 × 3 | 1 × 1 | 1 |
| Deconv9 | 576 × 576 × 3 | 576 × 576 × 3 | 64 × 64 | 32 |
| Cropping | 512 × 512 × 3 | 512 × 512 × 3 | - | - |
| Output Class Map | 512 × 512 × 1 | 512 × 512 × 1 | - | - |
| Proposed Method | U-Net [27] | SegNet [28] | |||||||
|---|---|---|---|---|---|---|---|---|---|
| All | FNA | TP | All | FNA | TP | All | FNA | TP | |
| Accuracy | 0.99 | 0.99 | 0.99 | 0.92 | 0.92 | 0.98 | 0.92 | 0.92 | 0.97 |
| Precision | 0.86 | 0.85 | 0.97 | 0.74 | 0.73 | 0.87 | 0.81 | 0.80 | 0.98 |
| Recall | 0.94 | 0.94 | 0.98 | 0.61 | 0.61 | 0.66 | 0.56 | 0.56 | 0.55 |
| F1-score | 0.88 | 0.87 | 0.98 | 0.64 | 0.63 | 0.74 | 0.62 | 0.61 | 0.67 |
| Jaccard-Index | 0.82 | 0.80 | 0.96 | 0.49 | 0.48 | 0.60 | 0.48 | 0.47 | 0.54 |
| Measurement | (I) Method | (J) Method | Mean Diff. (I–J) | Std. Error | Sig. | 95% C.I. | |
|---|---|---|---|---|---|---|---|
| Lo. Bound | Up. Bound | ||||||
| Accuracy | Proposed Method | U-Net | 0.0784732 * | 0.0068 | 0.0651 | 0.0918 | |
| SegNet | 0.0761947 * | 0.0068 | 0.0629 | 0.0895 | |||
| Precision | Proposed Method | U-Net | 0.1187516 * | 0.0289 | 0.0620 | 0.1755 | |
| SegNet | 0.0452 | 0.0289 | 0.1180 | −0.0116 | 0.1020 | ||
| Recall | Proposed Method | U-Net | 0.3336451 * | 0.0271 | 0.2803 | 0.3870 | |
| SegNet | 0.3856975 * | 0.0271 | 0.3323 | 0.4391 | |||
| F1-score | Proposed Method | U-Net | 0.2392282 * | 0.0266 | 0.1868 | 0.2916 | |
| SegNet | 0.2578479 * | 0.0266 | 0.2055 | 0.3102 | |||
| Jaccard Index | Proposed Method | U-Net | 0.3238887 * | 0.0290 | 0.2668 | 0.3809 | |
| SegNet | 0.3391651 * | 0.0290 | 0.2821 | 0.3962 | |||
| Method | CPU | RAM | GPU | Time (min) * |
|---|---|---|---|---|
| Proposed Method | Intel Xeon Gold 6134 CPU @ 3.20GHz × 16 | 128 GB | 4 × GeForce GTX 1080 Ti | 0.4 |
| Proposed Method | Intel Xeon CPU E5-2650 v2 @ 2.60GHz × 16 | 32 GB | 1 × GeForce GTX 1080 Ti | 1.7 |
| U-Net [27] | Intel Xeon CPU E5-2650 v2 @ 2.60GHz × 16 | 32 GB | 1 × GeForce GTX 1080 Ti | 13.2 |
| SegNet [28] | Intel Xeon CPU E5-2650 v2 @ 2.60GHz × 16 | 32 GB | 1 × GeForce GTX 1080 Ti | 15.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, Y.-J.; Chao, T.-K.; Khalil, M.-A.; Lee, Y.-C.; Hong, D.-Z.; Wu, J.-J.; Wang, C.-W. Deep Learning Fast Screening Approach on Cytological Whole Slides for Thyroid Cancer Diagnosis. Cancers 2021, 13, 3891. https://doi.org/10.3390/cancers13153891
Lin Y-J, Chao T-K, Khalil M-A, Lee Y-C, Hong D-Z, Wu J-J, Wang C-W. Deep Learning Fast Screening Approach on Cytological Whole Slides for Thyroid Cancer Diagnosis. Cancers. 2021; 13(15):3891. https://doi.org/10.3390/cancers13153891
Chicago/Turabian StyleLin, Yi-Jia, Tai-Kuang Chao, Muhammad-Adil Khalil, Yu-Ching Lee, Ding-Zhi Hong, Jia-Jhen Wu, and Ching-Wei Wang. 2021. "Deep Learning Fast Screening Approach on Cytological Whole Slides for Thyroid Cancer Diagnosis" Cancers 13, no. 15: 3891. https://doi.org/10.3390/cancers13153891
APA StyleLin, Y. -J., Chao, T. -K., Khalil, M. -A., Lee, Y. -C., Hong, D. -Z., Wu, J. -J., & Wang, C. -W. (2021). Deep Learning Fast Screening Approach on Cytological Whole Slides for Thyroid Cancer Diagnosis. Cancers, 13(15), 3891. https://doi.org/10.3390/cancers13153891