
Efficacy and Safety of Auricular Acupuncture for the Treatment of Insomnia in Breast Cancer Survivors: A Randomized Controlled Trial

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Randomization
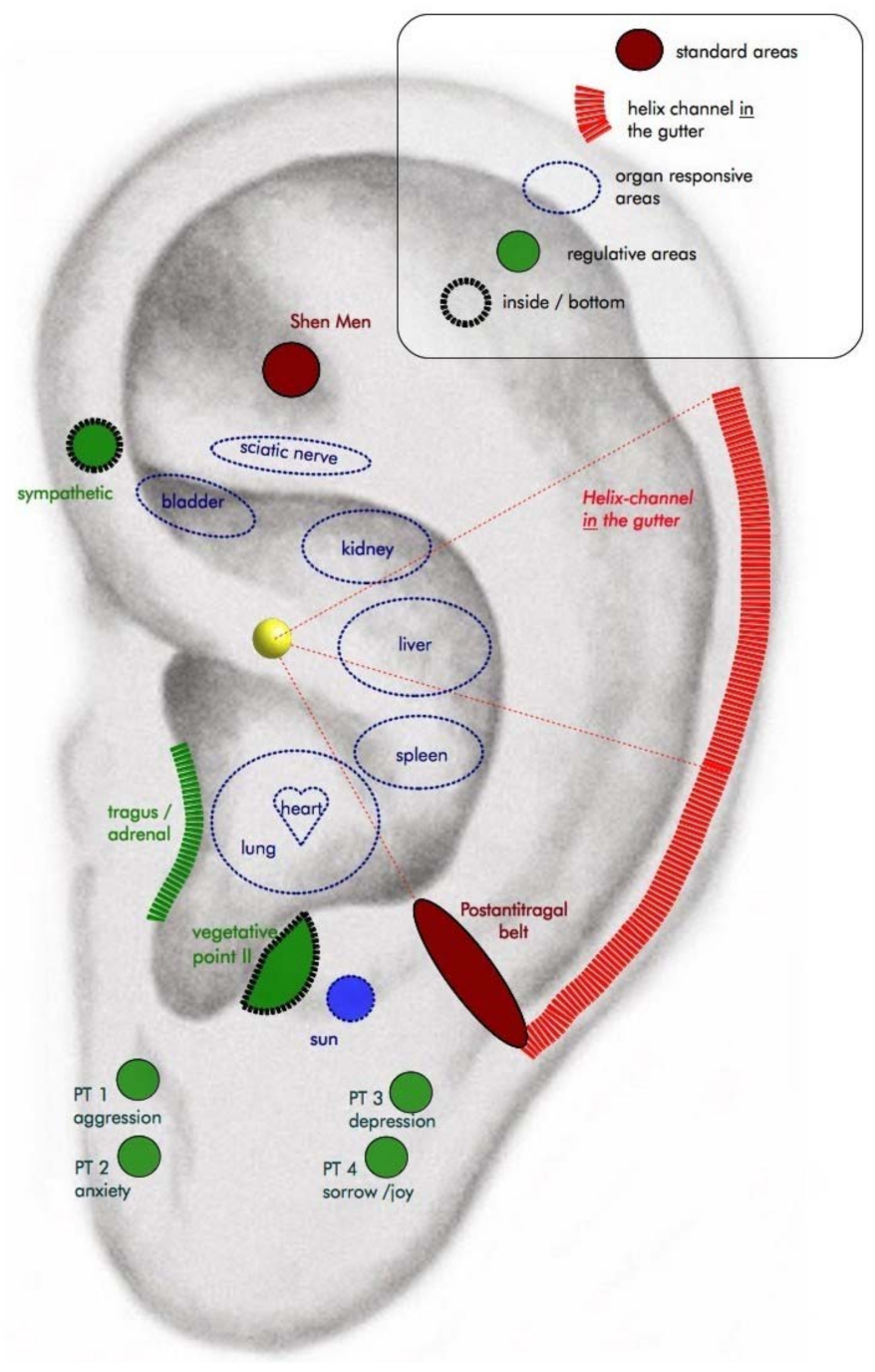
2.3. Interventions
2.4. Measures
2.5. Primary Outcome
Sleep Quality at Week 5
2.6. Secondary Outcomes
2.6.1. Sleep Quality
2.6.2. IL-6 Plasma Levels
2.6.3. Anxiety and Depressive Symptoms
2.6.4. Quality of Life and Fatigue
2.6.5. Stress
2.6.6. Treatment Expectation at Week 0
2.7. Adverse Events
2.8. Sample Size Calculation
2.9. Statistical Analysis
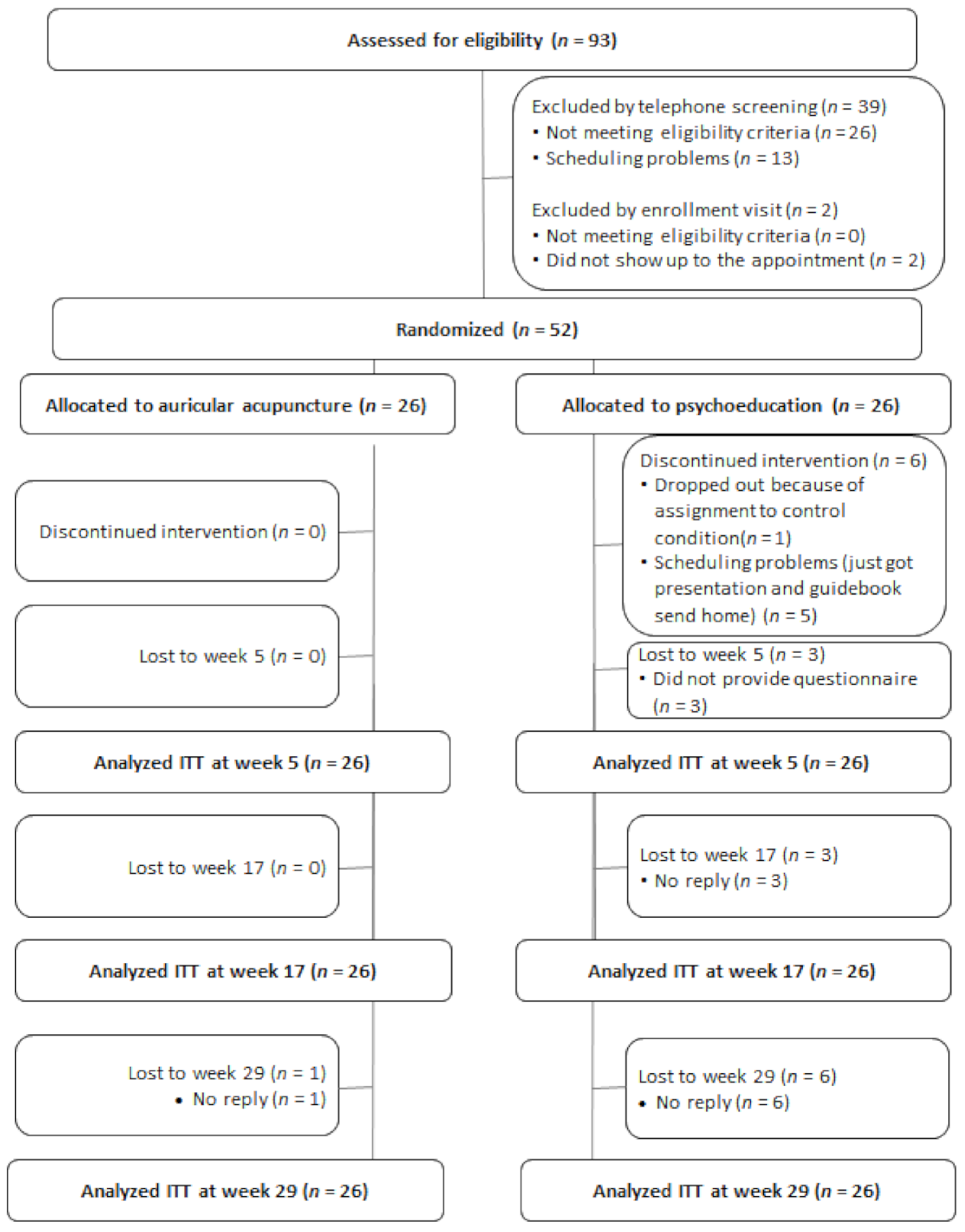
3. Results
3.1. Participant Characteristics
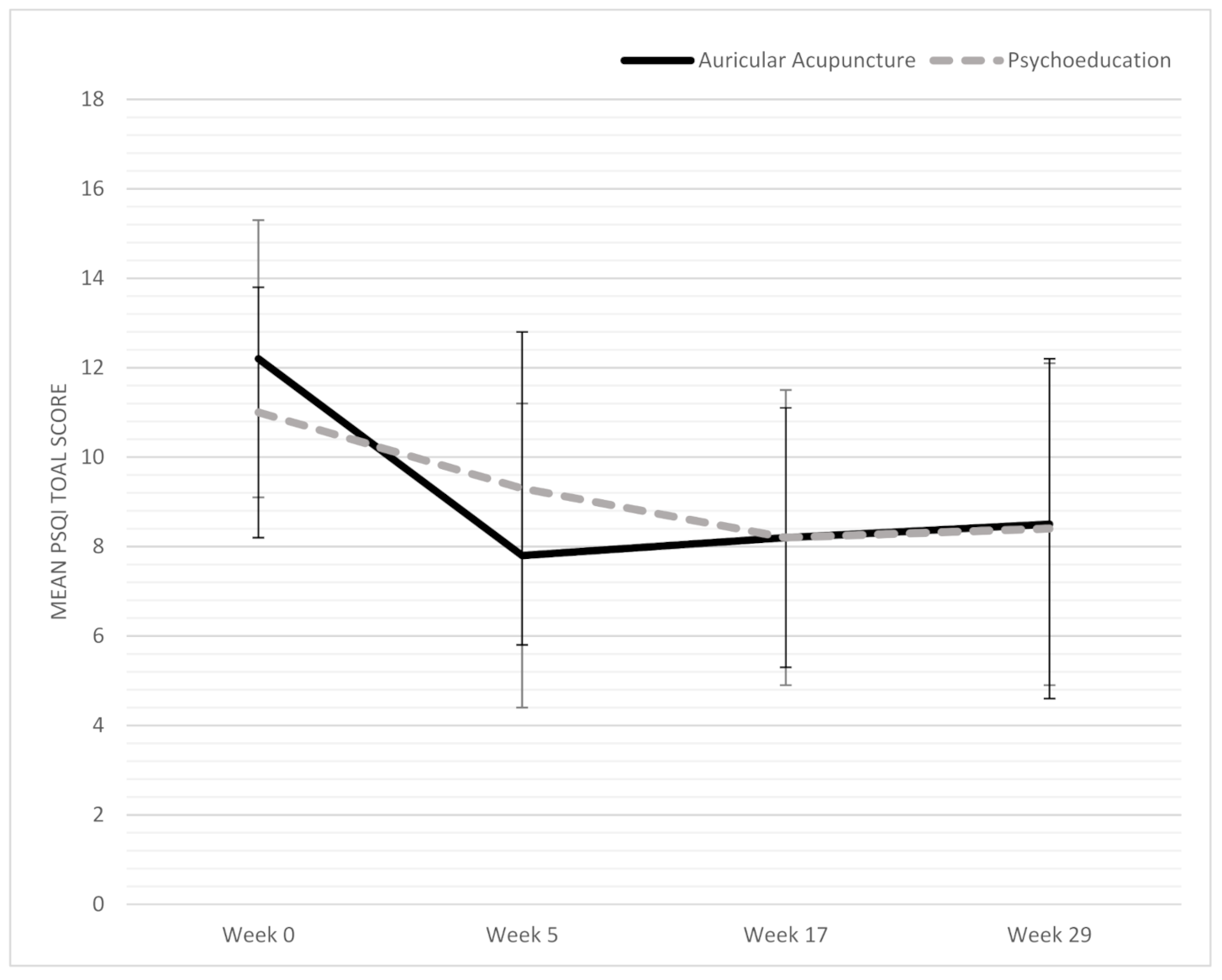
3.2. Primary Outcome
3.3. Secondary Outcomes
3.4. Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Gesellschaft der Epidemiologischen Krebsregister in Deutschland e V. Krebs in Deutschland 2015/2016, 12th ed.; Robert Koch Institute: Berlin, Germany, 2019. [Google Scholar]
- Schmidt, M.E.; Wiskemann, J.; Steindorf, K. Quality of life, problems, and needs of disease-free breast cancer survivors 5 years after diagnosis. Qual. Life Res. 2018, 27, 2077–2086. [Google Scholar] [CrossRef]
- Haidinger, R.; Bauerfeind, I. Long-Term Side Effects of Adjuvant Therapy in Primary Breast Cancer Patients: Results of a Web-Based Survey. Breast Care 2019, 14, 111–116. [Google Scholar] [CrossRef]
- Savard, J.; Ivers, H.; Villa, J.; Caplette-Gingras, A.; Morin, C.M. Natural course of insomnia comorbid with cancer: An 18-month longitudinal study. J. Clin. Oncol. 2011, 29, 3580–3586. [Google Scholar] [CrossRef]
- Fiorentino, L.; Ancoli-Israel, S. Insomnia and its treatment in women with breast cancer. Sleep Med. Rev. 2006, 10, 419–429. [Google Scholar] [CrossRef] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Pub: Washington, DC, USA, 2013. [Google Scholar]
- Stepanski, E.J.; Walker, M.S.; Schwartzberg, L.S.; Blakely, L.J.; Ong, J.C.; Houts, A.C. The relation of trouble sleeping, depressed mood, pain, and fatigue in patients with cancer. J. Clin. Sleep Med. 2009, 5, 132–136. [Google Scholar] [CrossRef] [Green Version]
- Fleming, L.; Gillespie, S.; Espie, C.A. The development and impact of insomnia on cancer survivors: A qualitative analysis. Psychooncology 2010, 19, 991–996. [Google Scholar] [CrossRef]
- Trudel-Fitzgerald, C.; Zhou, E.S.; Poole, E.M.; Zhang, X.; Michels, K.B.; Eliassen, A.H.; Chen, W.Y.; Holmes, M.D.; Tworoger, S.S.; Schernhammer, E.S. Sleep and survival among women with breast cancer: 30 years of follow-up within the Nurses’ Health Study. Br. J. Cancer 2017, 116, 1239–1246. [Google Scholar] [CrossRef] [Green Version]
- Bach, L.; Kalder, M.; Kostev, K. Depression and sleep disorders are associated with early mortality in women with breast cancer in the United Kingdom. J. Psychiatr. Res. 2020. [Google Scholar] [CrossRef]
- Irwin, M.R. Why sleep is important for health: A psychoneuroimmunology perspective. Annu. Rev. Psychol. 2015, 66, 143–172. [Google Scholar] [CrossRef] [Green Version]
- Irwin, M.R.; Olmstead, R.E.; Ganz, P.A.; Haque, R. Sleep disturbance, inflammation and depression risk in cancer survivors. Brain Behav. Immun. 2013, 30, S58–S67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haspel, J.A.; Anafi, R.; Brown, M.K.; Cermakian, N.; Depner, C.; Desplats, P.; Gelman, A.E.; Haack, M.; Jelic, S.; Kim, B.S.; et al. Perfect timing: Circadian rhythms, sleep, and immunity—An NIH workshop summary. JCI Insight 2020, 5, e131487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koffel, E.; Bramoweth, A.D.; Ulmer, C.S. Increasing access to and utilization of cognitive behavioral therapy for insomnia (CBT-I): A narrative review. J. Gen. Intern. Med. 2018, 33, 955–962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slade, A.N.; Waters, M.R.; Serrano, N.A. Long-term sleep disturbance and prescription sleep aid use among cancer survivors in the United States. Supportive Care Cancer 2020, 28, 551–560. [Google Scholar] [CrossRef]
- Baglioni, C.; Altena, E.; Bjorvatn, B.; Blom, K.; Bothelius, K.; Devoto, A.; Espie, C.A.; Frase, L.; Gavriloff, D.; Tuuliki, H.; et al. The European Academy for Cognitive Behavioural Therapy for Insomnia: An initiative of the European Insomnia Network to promote implementation and dissemination of treatment. J. Sleep Res. 2019, 29, e12967. [Google Scholar] [CrossRef] [PubMed]
- Mysliwiec, V.; Martin, J.L.; Ulmer, C.S.; Chowdhuri, S.; Brock, M.S.; Spevak, C.; Sall, J. The Management of Chronic Insomnia Disorder and Obstructive Sleep Apnea: Synopsis of the 2019 U.S. Department of Veterans Affairs and U.S. Department of Defense Clinical Practice Guidelines. Ann. Intern. Med. 2020, 172, 325–336. [Google Scholar] [CrossRef] [Green Version]
- Riemann, D.; Baglioni, C.; Bassetti, C.; Bjorvatn, B.; Groselj, L.D.; Ellis, J.G.; Espie, C.A.; Garcia-Borreguero, D.; Gjerstad, M.; Goncalves, M.; et al. European guideline for the diagnosis and treatment of insomnia. J. Sleep Res. 2017, 26, 675–700. [Google Scholar] [CrossRef]
- Kvale, E.A.; Shuster, J.L. Sleep disturbance in supportive care of cancer: A review. J. Palliat. Med. 2006, 9, 437–450. [Google Scholar] [CrossRef]
- Murphy, C.C.; Fullington, H.M.; Alvarez, C.A.; Betts, A.C.; Lee, S.J.C.; Haggstrom, D.A.; Halm, E.A. Polypharmacy and patterns of prescription medication use among cancer survivors. Cancer 2018, 124, 2850–2857. [Google Scholar] [CrossRef]
- Matthews, E.E.; Schmiege, S.J.; Cook, P.F.; Berger, A.M.; Aloia, M.S. Adherence to cognitive behavioral therapy for insomnia (CBTI) among women following primary breast cancer treatment: A pilot study. Behav. Sleep Med. 2012, 10, 217–229. [Google Scholar] [CrossRef]
- Quintiliani, M.I.; Imperatori, C.; Testani, E.; Losurdo, A.; Tamburello, S.; Contardi, A.; Della Marca, G.; Farina, B. Usefulness of psychoeducational intervention in chronic insomnia: An actigraphic study. J. Ment. Health 2020, 29, 20–26. [Google Scholar] [CrossRef]
- Romero, S.A.D.; Jiang, E.; Bussell, J.; Eriksen, W.; Duhamel, K.N.; Barg, F.K.; Mao, J.J. What makes one respond to acupuncture for insomnia? Perspectives of cancer survivors. Palliat. Supportive Care 2019, 18, 301–306. [Google Scholar] [CrossRef]
- Zia, F.Z.; Olaku, O.; Bao, T.; Berger, A.; Deng, G.; Fan, A.Y.; Garcia, M.K.; Herman, P.M.; Kaptchuk, T.J.; Ladas, E.J.; et al. The National Cancer Institute’s Conference on Acupuncture for Symptom Management in Oncology: State of the Science, Evidence, and Research Gaps. J. Natl. Cancer Inst. Monogr. 2017, 2017. [Google Scholar] [CrossRef] [Green Version]
- Tan, J.Y.; Molassiotis, A.; Wang, T.; Suen, L.K. Adverse events of auricular therapy: A systematic review. Evid. Based Complement. Alternat. Med. 2014, 2014, 506758. [Google Scholar] [CrossRef] [PubMed]
- Choi, T.Y.; Kim, J.I.; Lim, H.J.; Lee, M.S. Acupuncture for Managing Cancer-Related Insomnia: A Systematic Review of Randomized Clinical Trials. Integr. Cancer Ther. 2017, 16, 135–146. [Google Scholar] [CrossRef] [Green Version]
- Kuo, H.C.; Tsao, Y.; Tu, H.Y.; Dai, Z.H.; Creedy, D.K. Pilot randomized controlled trial of auricular point acupressure for sleep disturbances in women with ovarian cancer. Res. Nurs. Health 2018, 41, 469–479. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. NCI Dictionary of Cancer Terms. Available online: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/793175#:~:text=A%20type%20of%20acupuncture%20in,Also%20called%20ear%20acupuncture (accessed on 2 June 2020).
- Romoli, M.; Allais, G.; Airola, G.; Benedetto, C.; Mana, O.; Giacobbe, M.; Pugliese, A.M.; Battistella, G.; Fornari, E. Ear acupuncture and fMRI: A pilot study for assessing the specificity of auricular points. Neurol. Sci. 2014, 35 (Suppl. 1), 189–193. [Google Scholar] [CrossRef]
- Hou, P.W.; Hsu, H.C.; Lin, Y.W.; Tang, N.Y.; Cheng, C.Y.; Hsieh, C.L. The History, Mechanism, and Clinical Application of Auricular Therapy in Traditional Chinese Medicine. Evid. Based Complement. Alternat. Med. 2015, 2015, 495684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nielsen, A.; Gereau, S.; Tick, H. Risks and Safety of Extended Auricular Therapy: A Review of Reviews and Case Reports of Adverse Events. Pain Med. 2020, 21, 1276–1293. [Google Scholar] [CrossRef]
- Yang, Y.; Wen, J.; Hong, J. The Effects of Auricular Therapy for Cancer Pain: A Systematic Review and Meta-Analysis. Evid. Based Complement. Alternat. Med. 2020, 2020, 1618767. [Google Scholar] [CrossRef]
- Mao, J.J.; Liou, K.T.; Baser, R.E.; Bao, T.; Panageas, K.S.; Romero, S.A.D.; Li, Q.S.; Gallagher, R.M.; Kantoff, P.W. Effectiveness of Electroacupuncture or Auricular Acupuncture vs Usual Care for Chronic Musculoskeletal Pain Among Cancer Survivors: The PEACE Randomized Clinical Trial. JAMA Oncol. 2021, 7, 720–727. [Google Scholar] [CrossRef]
- Shin, J.; Park, H. Effects of Auricular Acupressure on Constipation in Patients With Breast Cancer Receiving Chemotherapy: A Randomized Control Trial. West. J. Nurs. Res. 2018, 40, 67–832. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Qi, D.; Gong, L.; Qu, H.; Xu, B.; Wen, X.; Li, J.; Xu, J. Effect of auricular points treatment combined with acupoints application in patients with constipation after lung cancer surgery. J. Cancer Res. Ther. 2017, 13, 844–848. [Google Scholar] [PubMed]
- Chen, C.Y.; Lin, X.X.; Wang, X. Efficacy of Non-Invasive Auricular Acupressure for Treating Constipation in Leukemia Patients Undergoing Chemotherapy: A Systematic Review. Complement. Med. Res. 2018, 25, 406–412. [Google Scholar] [CrossRef]
- Colagiuri, B.; Smith, C.A. A systematic review of the effect of expectancy on treatment responses to acupuncture. Evid. Based Complement. Alternat. Med. 2012, 2012, 857804. [Google Scholar] [CrossRef]
- Association, W.M. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. Int. J. Surg. 2011, 9, 672–677. [Google Scholar] [CrossRef] [Green Version]
- Ioannidis, J.P.; Evans, S.J.; Gøtzsche, P.C.; O’neill, R.T.; Altman, D.G.; Schulz, K.; Moher, D. Better reporting of harms in randomized trials: An extension of the CONSORT statement. Ann. Intern. Med. 2004, 141, 781–788. [Google Scholar] [CrossRef] [PubMed]
- Saghaei, M. Random allocation software for parallel group randomized trials. BMC Med. Res. Methodol. 2004, 4, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riemann, D.; Baum, E.; Cohrs, S.; Crönlein, T.; Hajak, G.; Hertenstein, E.; Klose, P.; Langhorst, J.; Mayer, G.; Nissen, C. S3-Leitlinie nicht erholsamer schlaf/schlafstörungen. Somnologie 2017, 21, 2–44. [Google Scholar] [CrossRef]
- Riemann, D. Ratgeber Schlafstörungen: Informationen für Betroffene und Angehörige; Hogrefe Verlag: Göttingen, Germany, 2016; Volume 33. [Google Scholar]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Carpenter, J.S.; Andrykowski, M.A. Psychometric evaluation of the Pittsburgh sleep quality index. J. Psychosom. Res. 1998, 45, 5–13. [Google Scholar] [CrossRef]
- Hughes, C.M.; McCullough, C.A.; Bradbury, I.; Boyde, C.; Hume, D.; Yuan, J.; Quinn, F.; McDonough, S.M. Acupuncture and reflexology for insomnia: A feasibility study. Acupunct. Med. 2009, 27, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Backhaus, J.; Junghanns, K.; Broocks, A.; Riemann, D.; Hohagen, F. Test–retest reliability and validity of the Pittsburgh Sleep Quality Index in primary insomnia. J. Psychosom. Res. 2002, 53, 737–740. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Herrmann, C. International experiences with the Hospital Anxiety and Depression Scale-a review of validation data and clinical results. J. Psychosom. Res. 1997, 42, 17–41. [Google Scholar] [CrossRef]
- Annunziata, M.A.; Muzzatti, B.; Bidoli, E.; Flaiban, C.; Bomben, F.; Piccinin, M.; Gipponi, K.M.; Mariutti, G.; Busato, S.; Mella, S. Hospital Anxiety and Depression Scale (HADS) accuracy in cancer patients. Supportive Care Cancer 2019, 28, 1–6. [Google Scholar] [CrossRef]
- Brady, M.J.; Cella, D.F.; Mo, F.; Bonomi, A.E.; Tulsky, D.S.; Lloyd, S.R.; Deasy, S.; Cobleigh, M.; Shiomoto, G. Reliability and validity of the Functional Assessment of Cancer Therapy-Breast quality-of-life instrument. J. Clin. Oncol. 1997, 15, 974–986. [Google Scholar] [CrossRef]
- Yellen, S.B.; Cella, D.F.; Webster, K.; Blendowski, C.; Kaplan, E. Measuring fatigue and other anemia-related symptoms with the Functional Assessment of Cancer Therapy (FACT) measurement system. J. Pain Symptom Manag. 1997, 13, 63–74. [Google Scholar] [CrossRef]
- Winstead-Fry, P.; Schultz, A. Psychometric analysis of the functional assessment of cancer therapy-general (FACT-G) scale in a rural sample. Cancer Interdiscip. Int. J. Am. Cancer Soc. 1997, 79, 2446–2452. [Google Scholar] [CrossRef]
- Webster, K.; Cella, D.; Yost, K. The Functional Assessment of Chronic Illness Therapy (FACIT) Measurement System: Properties, applications, and interpretation. Health Qual. Life Outcomes 2003, 1, 79. [Google Scholar] [CrossRef] [Green Version]
- Eton, D.T.; Cella, D.; Yost, K.J.; Yount, S.E.; Peterman, A.H.; Neuberg, D.S.; Sledge, G.W.; Wood, W.C. A combination of distribution- and anchor-based approaches determined minimally important differences (MIDs) for four endpoints in a breast cancer scale. J. Clin. Epidemiol. 2004, 57, 898–910. [Google Scholar] [CrossRef]
- Cella, D.; Eton, D.T.; Lai, J.S.; Peterman, A.H.; Merkel, D.E. Combining anchor and distribution-based methods to derive minimal clinically important differences on the Functional Assessment of Cancer Therapy (FACT) anemia and fatigue scales. J. Pain Symptom Manag. 2002, 24, 547–561. [Google Scholar] [CrossRef]
- Patrick, D.L.; Gagnon, D.D.; Zagari, M.J.; Mathijs, R.; Sweetenham, J. Assessing the clinical significance of health-related quality of life (HrQOL) improvements in anaemic cancer patients receiving epoetin alfa. Eur. J. Cancer 2003, 39, 335–345. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Klein, E.M.; Brähler, E.; Dreier, M.; Reinecke, L.; Müller, K.W.; Schmutzer, G.; Wölfling, K.; Beutel, M.E. The German version of the Perceived Stress Scale—psychometric characteristics in a representative German community sample. BMC Psychiatry 2016, 16, 159. [Google Scholar] [CrossRef] [Green Version]
- Edwards, I.R.; Aronson, J.K. Adverse drug reactions: Definitions, diagnosis, and management. Lancet 2000, 356, 1255–1259. [Google Scholar] [CrossRef]
- U.S. Food & Drug Administration. Safety. Available online: https://www.fda.gov/safety/reporting-serious-problems-fda/what-serious-adverse-event (accessed on 31 January 2020).
- Mao, J.J.; Farrar, J.T.; Bruner, D.; Zee, J.; Bowman, M.; Seluzicki, C.; DeMichele, A.; Xie, S.X. Electroacupuncture for fatigue, sleep, and psychological distress in breast cancer patients with aromatase inhibitor-related arthralgia: A randomized trial. Cancer 2014, 120, 3744–3751. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988; p. 22. [Google Scholar]
- Garland, S.N.; Xie, S.X.; DuHamel, K.; Bao, T.; Li, Q.; Barg, F.K.; Song, S.; Kantoff, P.; Gehrman, P.; Mao, J.J. Acupuncture Versus Cognitive Behavioral Therapy for Insomnia in Cancer Survivors: A Randomized Clinical Trial. J. Natl. Cancer Inst. 2019, 111, 1323–1331. [Google Scholar] [CrossRef]
- Garland, S.N.; Xie, S.X.; Li, Q.; Seluzicki, C.; Basal, C.; Mao, J.J. Comparative effectiveness of electro-acupuncture versus gabapentin for sleep disturbances in breast cancer survivors with hot flashes: A randomized trial. Menopause 2017, 24, 517–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergdahl, L.; Broman, J.E.; Berman, A.H.; Haglund, K.; von Knorring, L.; Markstrom, A. Auricular Acupuncture and Cognitive Behavioural Therapy for Insomnia: A Randomised Controlled Study. Sleep Disord. 2016, 2016, 7057282. [Google Scholar] [CrossRef] [Green Version]
- Culpepper, L. Insomnia: A primary care perspective. J. Clin. Psychiatry 2005, 66 (Suppl. 9), 14–17. [Google Scholar] [PubMed]
- Butt, M.F.; Albusoda, A.; Farmer, A.D.; Aziz, Q. The anatomical basis for transcutaneous auricular vagus nerve stimulation. J. Anat. 2020, 236, 588–611. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.H.; Yang, M.H.; Zhang, G.Z.; Wang, X.X.; Li, B.; Li, M.; Woelfer, M.; Walter, M.; Wang, L. Neural networks and the anti-inflammatory effect of transcutaneous auricular vagus nerve stimulation in depression. J. Neuroinflamm. 2020, 17, 54. [Google Scholar] [CrossRef] [PubMed]
- Bower, J.E.; Ganz, P.A.; Irwin, M.R.; Kwan, L.; Breen, E.C.; Cole, S.W. Inflammation and behavioral symptoms after breast cancer treatment: Do fatigue, depression, and sleep disturbance share a common underlying mechanism? J. Clin. Oncol. 2011, 29, 3517–3522. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
| Characteristics | Auricular Acupuncture (n = 26) | Psychoeducation (n = 26) | Total (n= 52) |
|---|---|---|---|
| Age (years) | 56.58 ± 7.9 | 54.8 ± 8.3 | 55.73 ± 8.1 |
| Weight (kg) | 74.46 ± 14.9 | 72.7 ± 14.3 | 73.6 ± 14.5 |
| Height (m) | 1.7 ± 0.1 | 1.69 ± 0.1 | 1.7 ± 0.1 |
| Time since diagnosis (months) | 53.8 ± 35.2 | 57.8 ± 44.7 | 55.8 ± 39.9 |
| Children | 1.7 ± 1.0 | 1.3 ± 1.2 | 1.5 ± 1.1 |
| Marital status n (%) | |||
| Single/living alone | 3 (11.5%) | 3 (11.5%) | 6 (11.5%) |
| Living with partner | 1 (3.8%) | 2 (7.7%) | 3 (5.8%) |
| Married | 19 (73.1%) | 19 (73%) | 38 (73.1%) |
| Divorced | 1 (3.8%) | 1 (3.8%) | 2 (3.8%) |
| Widowed | 2 (7.7%) | 1 (3.8%) | 3 (5.8%) |
| Education n (%) | |||
| Secondary modern school (“Hauptschule”) qualification | 2 (7.7%) | 2 (7.7%) | 4 (7.7%) |
| High school (“Realschule”) qualification | 8 (30.8%) | 6 (23.1%) | 14 (26.9%) |
| A level (“Abitur”) (without subsequent studies/with uncompleted studies) | 1 (3.8%) | 6 (23.1%) | 7 (13.5%) |
| University/college degree | 15 (57.7%) | 12 (46.2%) | 27 (51.9%) |
| Employment n (%) | |||
| Yes (full-time/part-time/training/retraining/sick leave currently under 6 months) | 16 (61.5%) | 18 (69.2%) | 34 (65.4%) |
| No (housewife/unemployed /sick leave longer than 6 months) | 2 (7.7%) | 6 (23.1%) | 8 (15.4%) |
| Retired | 8 (30.8%) | 2 (7.7%) | 10 (19.2%) |
| TNM Stage * n (%) | |||
| I | 11 (42.3%) | 13 (50%) | 24 (46.2%) |
| II | 10 (38.5%) | 9 (34.6%) | 19 (36.5%) |
| III | 4 (15.4%) | 4 (15.4%) | 8 (15.4%) |
| Tumor biology n (%) | |||
| Hormone-receptor-positive | 22 (84.6%) | 18 (69.2%) | 40 (76.9%) |
| Triple-positive | 0 (0%) | 4 (15.4%) | 4 (7.7%) |
| ER-positive and HER2-positive | 1 (3.8%) | 3 (11.5%) | 4 (7.7%) |
| Triple-negative | 3 (11.5%) | 1 (3.8%) | 4 (7.7%) |
| Prior chemotherapy n (%) | 19 (73.1%) | 14 (53.8%) | 33 (63.5%) |
| Prior radiation therapy n (%) | 23 (88.5%) | 21 (80.8%) | 44 (84.6%) |
| Prior operation n (%) | 26 (100%) | 24 (92.3%) | 50 (96.2%) |
| Current antihormonal therapy n (%) | 20 (76.9%) | 17 (65.4%) | 37 (71.2%) |
| Treatment expectancy ** | 7.81 ± 1.81 | 4.22 ± 2.96 | 6.02 ± 3.03 |
| Variable | Effect: Mean ± SD | Time × Group Interaction Effect | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Auricular Acupuncture, n = 26 | Psychoeducation, n = 26 | Week 5 | Week 17 | Week 29 | ||||||||||
| Week 0 | Week 5 | Week 17 | Week 29 | Week 0 | Week 5 | Week 17 | Week 29 | p | η2p | p | η2p | p | η2p | |
| PSQI | 12.2 ± 3.1 | 7.8 ± 3.4 | 8.2 ± 3.4 | 8.5 ± 3.6 | 11.0 ± 2.8 | 9.3 ± 3.5 | 8.2 ± 2.9 | 8.4 ± 3.8 | 0.031 | 0.094 | 0.141 | 0.045 | 0.133 | 0.046 |
| PSS | 20.2 ± 4.8 | 16.9 ± 4.0 | 18.0 ± 4.5 | 19.3 ± 4.6 | 18.0 ± 5.5 | 18.3 ± 5.8 | 18.4 ± 5.8 | 19.0 ± 5.3 | 0.030 | 0.094 | 0.079 | 0.063 | 0.902 | 0.000 |
| FACT-B | 92.2 ± 15.1 | 103.4 ± 12.7 | 97.5 ± 17.9 | 96.1 ± 17.9 | 96.3 ± 17.0 | 99.2 ± 17.2 | 96.9 ± 18.1 | 95.7 ± 19.9 | 0.158 | 0.041 | 0.494 | 0.010 | 0.700 | 0.003 |
| FACIT-F | 31.3 ± 10.5 | 40.6 ± 5.8 | 36.2 ± 11.7 | 35.3 ± 9.3 | 33.1 ± 10.8 | 34.3 ± 11.3 | 36.3 ± 10.3 | 34.3 ± 12.1 | 0.006 | 0.148 | 0.617 | 0.005 | 0.201 | 0.034 |
| HADS-A | 9.5 ± 4.2 | 6.0 ± 3.5 | 7.2 ± 4.0 | 7.5 ± 3.4 | 8.0 ± 4.3 | 7.8 ± 4.3 | 7.7 ± 4.0 | 8.4 ± 4.5 | 0.001 | 0.192 | 0.473 | 0.011 | 0.192 | 0.035 |
| HADS-D | 5.6 ± 3.5 | 3.4 ± 2.4 | 5.0 ± 3.5 | 5.0 ± 3.3 | 5.0 ± 4.2 | 5.3 ± 3.9 | 5.1 ± 3.9 | 5.6 ± 4.2 | 0.272 | 0.025 | 0.093 | 0.058 | 0.148 | 0.043 |
| Interleukin 6 | 2.5 ± 2.2 | 2.2 ± 2.3 | * | * | 1.8 ± 2.5 | 1.4 ± 0.9 | * | * | 0.205 | 0.033 | * | * | * | * |
| Adverse Event | Auricular Acupuncture | Psychoeducation | |
|---|---|---|---|
| Non-Serious | Non-Serious | ||
| Total | Intervention-Related | ||
| Bruising | 9 | 9 | 0 |
| Pain | 4 | 2 | 0 |
| Pressure sensitivity | 3 | 3 | 0 |
| Hot flushes | 6 | 6 | 0 |
| Insatiable hunger/attacks of hunger/ravenous hunger | 7 | 7 | 0 |
| Restless legs syndrome | 1 | 0 | 0 |
| Flatulence/diarrhea | 2 | 1 | 0 |
| Cephalgia/tension headache | 2 | 0 | 0 |
| Fatigue | 3 | 3 | 0 |
| Sweats | 1 | 0 | 0 |
| Increased cramp tendency in the legs and thighs | 2 | 0 | 0 |
| Migraine attack | 1 | 0 | 0 |
| Swollen hand | 1 | 0 | 0 |
| Dental root inflammation | 1 | 0 | 0 |
| Lumbago | 1 | 0 | 0 |
| Abdominal discomfort | 2 | 0 | 0 |
| Xerostomia | 1 | 0 | 0 |
| Dysgeusia | 1 | 0 | 0 |
| Dull feeling in the head | 1 | 1 | 0 |
| Unrest | 1 | 1 | 0 |
| Itching on the ear | 1 | 1 | 0 |
| Heavy eyelids | 4 | 4 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Höxtermann, M.D.; Buner, K.; Haller, H.; Kohl, W.; Dobos, G.; Reinisch, M.; Kümmel, S.; Cramer, H.; Voiss, P. Efficacy and Safety of Auricular Acupuncture for the Treatment of Insomnia in Breast Cancer Survivors: A Randomized Controlled Trial. Cancers 2021, 13, 4082. https://doi.org/10.3390/cancers13164082
Höxtermann MD, Buner K, Haller H, Kohl W, Dobos G, Reinisch M, Kümmel S, Cramer H, Voiss P. Efficacy and Safety of Auricular Acupuncture for the Treatment of Insomnia in Breast Cancer Survivors: A Randomized Controlled Trial. Cancers. 2021; 13(16):4082. https://doi.org/10.3390/cancers13164082
Chicago/Turabian StyleHöxtermann, Melanie D., Katja Buner, Heidemarie Haller, Wiebke Kohl, Gustav Dobos, Mattea Reinisch, Sherko Kümmel, Holger Cramer, and Petra Voiss. 2021. "Efficacy and Safety of Auricular Acupuncture for the Treatment of Insomnia in Breast Cancer Survivors: A Randomized Controlled Trial" Cancers 13, no. 16: 4082. https://doi.org/10.3390/cancers13164082
APA StyleHöxtermann, M. D., Buner, K., Haller, H., Kohl, W., Dobos, G., Reinisch, M., Kümmel, S., Cramer, H., & Voiss, P. (2021). Efficacy and Safety of Auricular Acupuncture for the Treatment of Insomnia in Breast Cancer Survivors: A Randomized Controlled Trial. Cancers, 13(16), 4082. https://doi.org/10.3390/cancers13164082