
MRI-Determined Psoas Muscle Fat Infiltration Correlates with Severity of Weight Loss during Cancer Cachexia


 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Subjects
2.2. Anthropometric Measurements
2.3. MRI Measurements
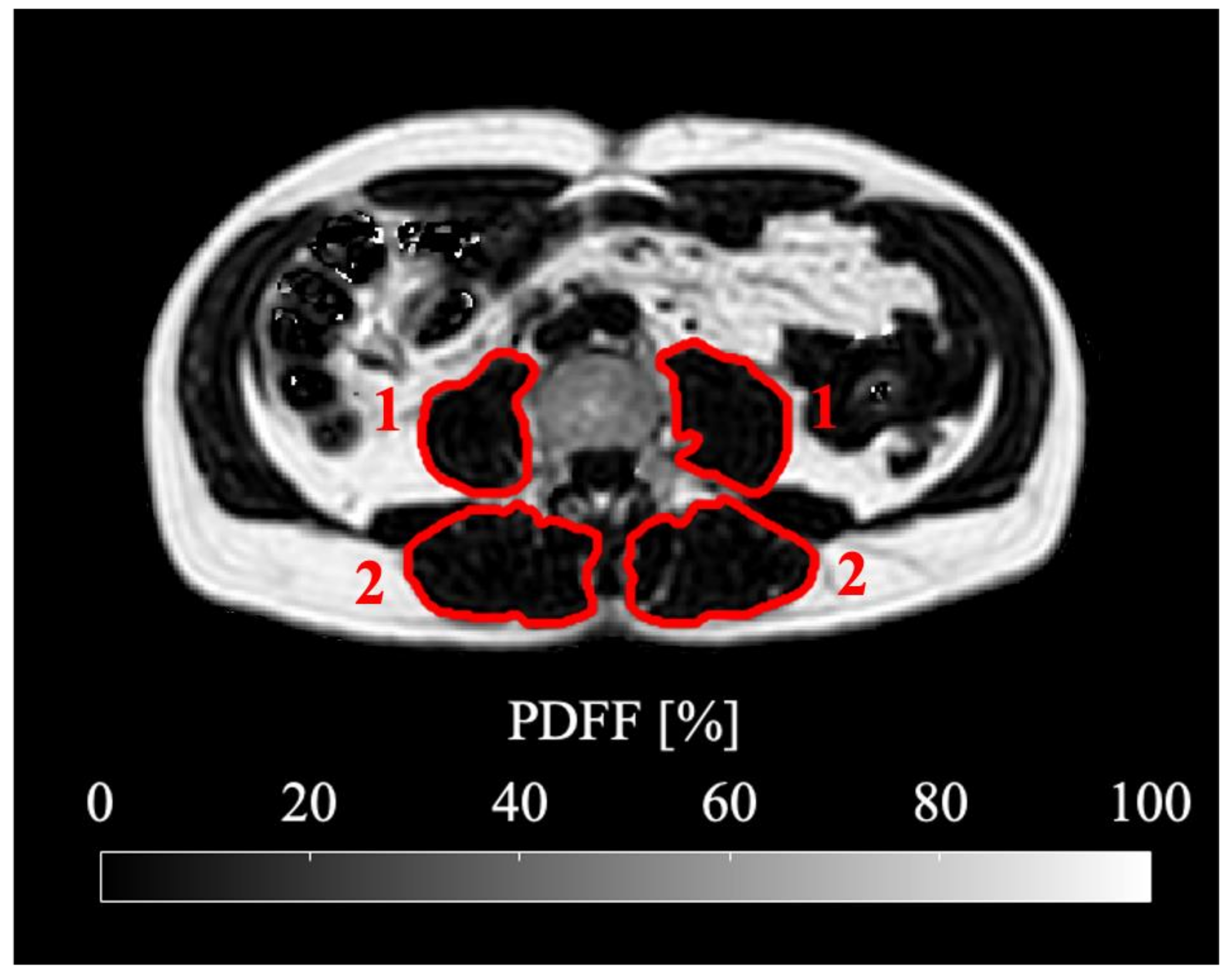
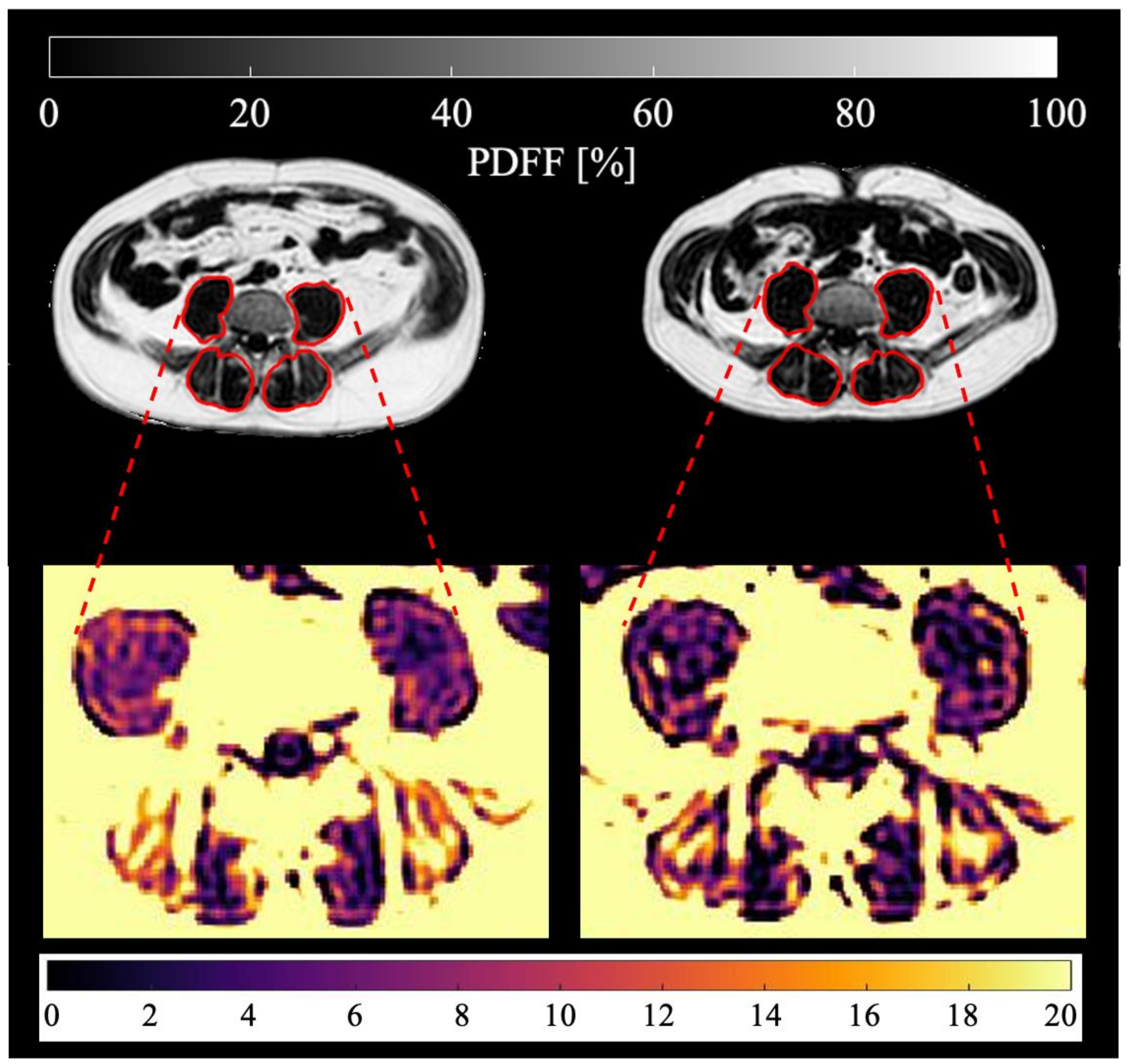
2.4. Skeletal Muscle Segmentation
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Cohort
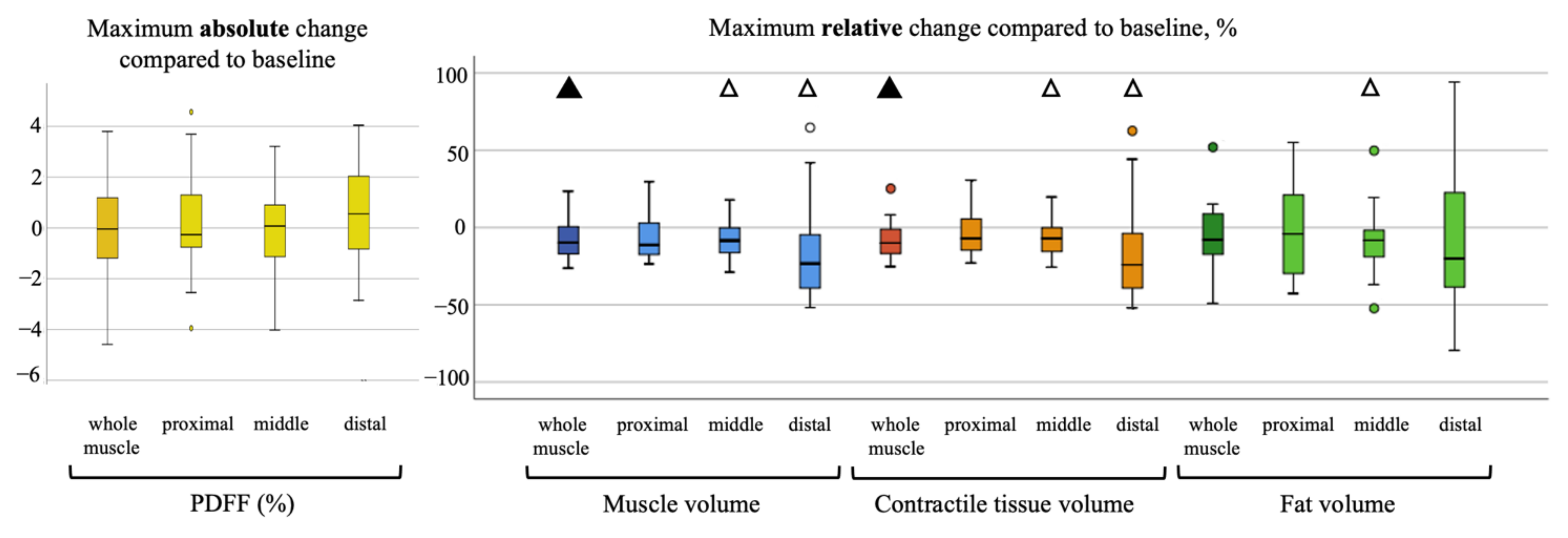
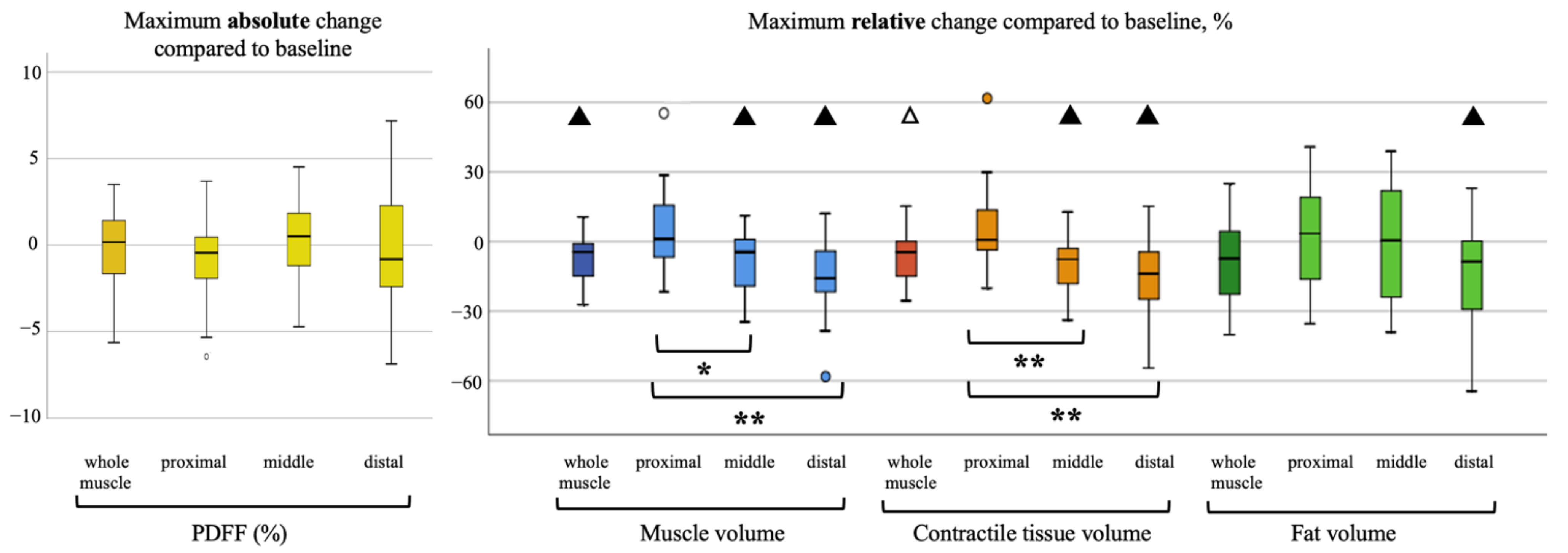
3.2. Longitudinal Analysis
3.3. Correlation Analysis
4. Discussion
4.1. Regional Analysis of Psoas and Erector Spinae Muscle
4.2. Muscle PDFF as a Predictive Marker
4.3. Clinical Implications
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baracos, V.E.; Martin, L.; Korc, M.; Guttridge, D.C.; Fearon, K.C.H. Cancer-associated cachexia. Nat. Rev. Dis. Primers 2018, 4, 17105. [Google Scholar] [CrossRef]
- Tisdale, M.J. Cachexia in cancer patients. Nat. Rev. Cancer 2002, 2, 862–871. [Google Scholar] [CrossRef]
- Fox, K.M.; Brooks, J.M.; Gandra, S.R.; Markus, R.; Chiou, C.F. Estimation of Cachexia among Cancer Patients Based on Four Definitions. J. Oncol. 2009, 2009, 693458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Haehling, S.; Anker, S.D. Cachexia as a major underestimated and unmet medical need: Facts and numbers. J. Cachexia Sarcopenia Muscle 2010, 1, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loberg, R.D.; Bradley, D.A.; Tomlins, S.A.; Chinnaiyan, A.M.; Pienta, K.J. The Lethal Phenotype of Cancer: The Molecular Basis of Death Due to Malignancy. CA A Cancer J. Clin. 2007, 57, 225–241. [Google Scholar] [CrossRef] [Green Version]
- Dewys, W.D.; Begg, C.; Lavin, P.T.; Band, P.R.; Bennett, J.M.; Bertino, J.R.; Cohen, M.H.; Douglass, H.O.; Engstrom, P.F.; Ezdinli, E.Z.; et al. Prognostic effect of weight loss prior tochemotherapy in cancer patients. Am. J. Med. 1980, 69, 491–497. [Google Scholar] [CrossRef]
- Laviano, A.; Meguid, M.M. Nutritional issues in cancer management. Nutrition 1996, 12, 358–371. [Google Scholar] [CrossRef]
- Fearon, K.; Strasser, F.; Anker, S.D.; Bosaeus, I.; Bruera, E.; Fainsinger, R.L.; Jatoi, A.; Loprinzi, C.; MacDonald, N.; Mantovani, G.; et al. Definition and classification of cancer cachexia: An international consensus. Lancet Oncol. 2011, 12, 489–495. [Google Scholar] [CrossRef]
- Hurria, A.; Gupta, S.; Zauderer, M.; Zuckerman, E.L.; Cohen, H.J.; Muss, H.; Rodin, M.; Panageas, K.S.; Holland, J.C.; Saltz, L.; et al. Developing a cancer-specific geriatric assessment. Cancer 2005, 104, 1998–2005. [Google Scholar] [CrossRef] [PubMed]
- Viganò, A.; Morais, J.A. The elderly patient with cancer: A holistic view. Nutrition 2015, 31, 587–589. [Google Scholar] [CrossRef]
- Soubeyran, P.; Fonck, M.; Blanc-Bisson, C.; Blanc, J.-F.; Ceccaldi, J.; Mertens, C.; Imbert, Y.; Cany, L.; Vogt, L.; Dauba, J.; et al. Predictors of Early Death Risk in Older Patients Treated With First-Line Chemotherapy for Cancer. J. Clin. Oncol. 2012, 30, 1829–1834. [Google Scholar] [CrossRef]
- Martin, A.; Freyssenet, D. Phenotypic features of cancer cachexia-related loss of skeletal muscle mass and function: Lessons from human and animal studies. J. Cachexia Sarcopenia Muscle 2021, 12, 252–273. [Google Scholar] [CrossRef]
- Argilés, J.M.; Busquets, S.; López-Soriano, F.J. Cytokines in the pathogenesis of cancer cachexia. Curr. Opin. Clin. Nutr. Metab. Care 2003, 6, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, J.A.; Pothuraju, R.; Jain, M.; Batra, S.K.; Nasser, M.W. Advances in cancer cachexia: Intersection between affected organs, mediators, and pharmacological interventions. Biochim. Et Biophys. Acta (BBA) Rev. Cancer 2020, 1873, 188359. [Google Scholar] [CrossRef]
- Boettcher, M.; Machann, J.; Stefan, N.; Thamer, C.; Häring, H.-U.; Claussen, C.D.; Fritsche, A.; Schick, F. Intermuscular adipose tissue (IMAT): Association with other adipose tissue compartments and insulin sensitivity. J. Magn. Reson. Imaging 2009, 29, 1340–1345. [Google Scholar] [CrossRef] [PubMed]
- Song, M.-Y.; Ruts, E.; Kim, J.; Janumala, I.; Heymsfield, S.; Gallagher, D. Sarcopenia and increased adipose tissue infiltration of muscle in elderly African American women. Am. J. Clin. Nutr. 2004, 79, 874–880. [Google Scholar] [CrossRef] [PubMed]
- Hooijmans, M.T.; Niks, E.H.; Burakiewicz, J.; Anastasopoulos, C.; van den Berg, S.I.; van Zwet, E.; Webb, A.G.; Verschuuren, J.J.G.M.; Kan, H.E. Non-uniform muscle fat replacement along the proximodistal axis in Duchenne muscular dystrophy. Neuromuscul. Disord. 2017, 27, 458–464. [Google Scholar] [CrossRef]
- Bhullar, A.S.; Anoveros-Barrera, A.; Dunichand-Hoedl, A.; Martins, K.; Bigam, D.; Khadaroo, R.G.; McMullen, T.; Bathe, O.F.; Putman, C.T.; Clandinin, M.T.; et al. Lipid is heterogeneously distributed in muscle and associates with low radiodensity in cancer patients. J. Cachexia Sarcopenia Muscle 2020, 11, 735–747. [Google Scholar] [CrossRef] [PubMed]
- Adam, R.A.; Adam, Y.G. Malignant ascites: Past, present, and future. J. Am. Coll. Surg. 2004, 198, 999–1011. [Google Scholar] [CrossRef] [PubMed]
- Bar-Sela, G.; Omer, A.; Flechter, E.; Zalman, D. Treatment of Lower Extremity Edema by Subcutaneous Drainage in Palliative Care of Advanced Cancer Patients. Am. J. Hosp. Palliat. Med. 2010, 27, 272–275. [Google Scholar] [CrossRef]
- Baracos, V.E.; Reiman, T.; Mourtzakis, M.; Gioulbasanis, I.; Antoun, S. Body composition in patients with non−small cell lung cancer: A contemporary view of cancer cachexia with the use of computed tomography image analysis. Am. J. Clin. Nutr. 2010, 91, 1133S–1137S. [Google Scholar] [CrossRef] [Green Version]
- Faron, A.; Luetkens, J.A.; Schmeel, F.C.; Kuetting, D.L.R.; Thomas, D.; Sprinkart, A.M. Quantification of fat and skeletal muscle tissue at abdominal computed tomography: Associations between single-slice measurements and total compartment volumes. Abdom. Radiol. 2019, 44, 1907–1916. [Google Scholar] [CrossRef]
- Burakiewicz, J.; Sinclair, C.D.; Fischer, D.; Walter, G.A.; Kan, H.E.; Hollingsworth, K.G. Quantifying fat replacement of muscle by quantitative MRI in muscular dystrophy. J. Neurol. 2017, 264, 2053–2067. [Google Scholar] [CrossRef] [Green Version]
- Karampinos, D.C.; Baum, T.; Nardo, L.; Alizai, H.; Yu, H.; Carballido-Gamio, J.; Yap, S.P.; Shimakawa, A.; Link, T.M.; Majumdar, S. Characterization of the regional distribution of skeletal muscle adipose tissue in type 2 diabetes using chemical shift-based water/fat separation. J. Magn. Reson. Imaging 2012, 35, 899–907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reeder, S.B.; Cruite, I.; Hamilton, G.; Sirlin, C.B. Quantitative assessment of liver fat with magnetic resonance imaging and spectroscopy. J. Magn. Reson. Imaging 2011, 34, 729–749. [Google Scholar] [CrossRef] [PubMed]
- Reeder, S.B.; Hu, H.H.; Sirlin, C.B. Proton density fat-fraction: A standardized mr-based biomarker of tissue fat concentration. J. Magn. Reson. Imaging 2012, 36, 1011–1014. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.H.; Branca, R.T.; Hernando, D.; Karampinos, D.C.; Machann, J.; McKenzie, C.A.; Wu, H.H.; Yokoo, T.; Velan, S.S. Magnetic resonance imaging of obesity and metabolic disorders: Summary from the 2019 ISMRM Workshop. Magn. Reson. Med. 2020, 83, 1565–1576. [Google Scholar] [CrossRef] [PubMed]
- Yushkevich, P.A.; Piven, J.; Hazlett, H.C.; Smith, R.G.; Ho, S.; Gee, J.C.; Gerig, G. User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. NeuroImage 2006, 31, 1116–1128. [Google Scholar] [CrossRef] [Green Version]
- Aust, S.; Knogler, T.; Pils, D.; Obermayr, E.; Reinthaller, A.; Zahn, L.; Radlgruber, I.; Mayerhoefer, M.E.; Grimm, C.; Polterauer, S. Skeletal muscle depletion and markers for cancer cachexia are strong prognostic factors in epithelial ovarian cancer. PLoS ONE 2015, 10, e0140403. [Google Scholar] [CrossRef] [PubMed]
- van Dijk, D.P.J.; Bakers, F.C.H.; Sanduleanu, S.; Vaes, R.D.W.; Rensen, S.S.; Dejong, C.H.C.; Beets-Tan, R.G.H.; Damink, S.W.M.O. Myosteatosis predicts survival after surgery for periampullary cancer: A novel method using mri. HPB 2018, 20, 715–720. [Google Scholar] [CrossRef] [Green Version]
- Wallengren, O.; Iresjö, B.-M.; Lundholm, K.; Bosaeus, I. Loss of muscle mass in the end of life in patients with advanced cancer. Supportive Care Cancer 2015, 23, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Jackson, W.; Alexander, N.; Schipper, M.; Fig, L.; Feng, F.; Jolly, S. Characterization of changes in total body composition for patients with head and neck cancer undergoing chemoradiotherapy using dual-energy x-ray absorptiometry. Head Neck 2014, 36, 1356–1362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levine, J.A.; Abboud, L.; Barry, M.; Reed, J.E.; Sheedy, P.F.; Jensen, M.D. Measuring leg muscle and fat mass in humans: Comparison of CT and dual-energy X-ray absorptiometry. J. Appl. Physiol. 2000, 88, 452–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maden-Wilkinson, T.; Degens, H.; Jones, D.; McPhee, J. Comparison of MRI and DXA to measure muscle size and age-related atrophy in thigh muscles. J. Musculoskelet. Neuronal Interact. 2013, 13, 320–328. [Google Scholar]
- Clark, R.V.; Walker, A.C.; O’Connor-Semmes, R.L.; Leonard, M.S.; Miller, R.R.; Stimpson, S.A.; Turner, S.M.; Ravussin, E.; Cefalu, W.T.; Hellerstein, M.K. Total body skeletal muscle mass: Estimation by creatine (methyl-d3) dilution in humans. J. Appl. Physiol. 2014, 116, 1605–1613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heymsfield, S.B.; Adamek, M.; Gonzalez, M.C.; Jia, G.; Thomas, D.M. Assessing skeletal muscle mass: Historical overview and state of the art. J. Cachexia Sarcopenia Muscle 2014, 5, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Correa-de-Araujo, R.; Addison, O.; Miljkovic, I.; Goodpaster, B.H.; Bergman, B.C.; Clark, R.V.; Elena, J.W.; Esser, K.A.; Ferrucci, L.; Harris-Love, M.O. Myosteatosis in the context of skeletal muscle function deficit: An interdisciplinary workshop at the national institute on aging. Front. Physiol. 2020, 11, 963. [Google Scholar] [CrossRef] [PubMed]
- Moon, J.; Stout, J.; Smith-Ryan, A.; Kendall, K.; Fukuda, D.; Cramer, J.; Moon, S. Tracking fat-free mass changes in elderly men and women using single-frequency bioimpedance and dual-energy X-ray absorptiometry: A four-compartment model comparison. Eur. J. Clin. Nutr. 2013, 67, S40–S46. [Google Scholar] [CrossRef] [PubMed]
- St-Onge, M.-P.; Wang, Z.; Horlick, M.; Wang, J.; Heymsfield, S.B. Dual-energy X-ray absorptiometry lean soft tissue hydration: Independent contributions of intra-and extracellular water. Am. J. Physiol.-Endocrinol. Metab. 2004, 287, E842–E847. [Google Scholar] [CrossRef]
- Burian, E.; Syvari, J.; Holzapfel, C.; Drabsch, T.; Kirschke, J.S.; Rummeny, E.J.; Zimmer, C.; Hauner, H.; Karampinos, D.C.; Baum, T.; et al. Gender- and Age-Related Changes in Trunk Muscle Composition Using Chemical Shift Encoding-Based Water(-)Fat MRI. Nutrients 2018, 10, 1972. [Google Scholar] [CrossRef] [Green Version]
- Jones, K.I.; Doleman, B.; Scott, S.; Lund, J.N.; Williams, J.P. Simple psoas cross-sectional area measurement is a quick and easy method to assess sarcopenia and predicts major surgical complications. Colorectal Dis. 2015, 17, O20–O26. [Google Scholar] [CrossRef] [Green Version]
- Zargar, H.; Almassi, N.; Kovac, E.; Ercole, C.; Remer, E.; Rini, B.; Stephenson, A.; Garcia, J.A.; Grivas, P. Change in Psoas Muscle Volume as a Predictor of Outcomes in Patients Treated with Chemotherapy and Radical Cystectomy for Muscle-Invasive Bladder Cancer. Bladder Cancer 2017, 3, 57–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baracos, V.E. Psoas as a sentinel muscle for sarcopenia: A flawed premise. J. Cachexia Sarcopenia Muscle 2017, 8, 527–528. [Google Scholar] [CrossRef]
- Rutten, I.J.G.; Ubachs, J.; Kruitwagen, R.; Beets-Tan, R.G.H.; Olde Damink, S.W.M.; Van Gorp, T. Psoas muscle area is not representative of total skeletal muscle area in the assessment of sarcopenia in ovarian cancer. J. Cachexia Sarcopenia Muscle 2017, 8, 630–638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prado, C.M.; Lieffers, J.R.; McCargar, L.J.; Reiman, T.; Sawyer, M.B.; Martin, L.; Baracos, V.E. Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: A population-based study. Lancet Oncol. 2008, 9, 629–635. [Google Scholar] [CrossRef]
- Tan, B.H.L.; Birdsell, L.A.; Martin, L.; Baracos, V.E.; Fearon, K.C.H. Sarcopenia in an Overweight or Obese Patient Is an Adverse Prognostic Factor in Pancreatic Cancer. Clin. Cancer Res. 2009, 15, 6973–6979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yip, C.; Dinkel, C.; Mahajan, A.; Siddique, M.; Cook, G.J.; Goh, V. Imaging body composition in cancer patients: Visceral obesity, sarcopenia and sarcopenic obesity may impact on clinical outcome. Insights Imaging 2015, 6, 489–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosaeus, I. Nutritional support in multimodal therapy for cancer cachexia. Supportive Care Cancer 2008, 16, 447. [Google Scholar] [CrossRef]
- Lundholm, K.; Daneryd, P.; Körner, U.; Hyltander, A.; Bosaeus, I. Evidence that long-term COX-treatment improves energy homeostasis and body composition in cancer patients with progressive cachexia. Int. J. Oncol. 2004, 24, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Monk, J.P.; Phillips, G.; Waite, R.; Kuhn, J.; Schaaf, L.J.; Otterson, G.A.; Guttridge, D.; Rhoades, C.; Shah, M.; Criswell, T.; et al. Assessment of Tumor Necrosis Factor Alpha Blockade As an Intervention to Improve Tolerability of Dose-Intensive Chemotherapy in Cancer Patients. J. Clin. Oncol. 2006, 24, 1852–1859. [Google Scholar] [CrossRef] [PubMed]
- Aapro, M.; Arends, J.; Bozzetti, F.; Fearon, K.; Grunberg, S.M.; Herrstedt, J.; Hopkinson, J.; Jacquelin-Ravel, N.; Jatoi, A.; Kaasa, S.; et al. Early recognition of malnutrition and cachexia in the cancer patient: A position paper of a European School of Oncology Task Force. Ann. Oncol. 2014, 25, 1492–1499. [Google Scholar] [CrossRef] [PubMed]
- Moreira-Pais, A.; Ferreira, R.; Gil da Costa, R. Platinum-induced muscle wasting in cancer chemotherapy: Mechanisms and potential targets for therapeutic intervention. Life Sci. 2018, 208, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Damrauer, J.S.; Stadler, M.E.; Acharyya, S.; Baldwin, A.S.; Couch, M.E.; Guttridge, D.C. Chemotherapy-induced muscle wasting: Association with NF-κB and cancer cachexia. Eur. J. Transl. Myol. 2018, 28, 7590. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TR | 7 ms |
| TE1/ΔTE | TE1 = 1.14 ms/ΔTE = 0.8 ms |
| Flip angle | 3° |
| Bandwidth | 2342.5 Hz/pixel |
| Acquisition matrix size | 116 × 155 |
| Field of view (FOV) | 350 × 467 × 102 mm3 |
| Acquisition voxel size | 3 × 3 × 6 mm3 |
| Slices | 17 |
| SENSE reduction factor | 2.2 × 1.2 |
| Number of averages | 1 |
| Scan time | 8 s |
| Muscle Measurements | Muscle Section | M. Erector Spinae, n = 55 | M. Psoas, n = 56 |
|---|---|---|---|
| Mean (SD, Range) | Mean (SD, Range) | ||
| PDFF, % | total muscle | 15.5 (*, 7.1–39.7) | 9.7 (*, 5.6–22.9) |
| proximal | 14.1 (6.6, 4.1–39.1) | 11.2 (3.8, 5.4–21.9) | |
| middle | 15.2 (6.8, 5.9–37.8) | 10.0 (3.5, 5.3–22.9) | |
| distal | 22.5 (7.9, 8.1–43.9) | 9.5 (4.0, 3.6–27.7) | |
| Muscle volume, mL | total muscle | 804.7 (*, 394.0–1588.9) | 294.1 (115.3, 108.0–601.5) |
| proximal | 214.0 (65.9, 93.9–371.5) | 75.0 (28.6, 33.3–151.1) | |
| middle | 418.5 (136.7, 189.3–799.7) | 166.7 (63.4, 59.3–335.8) | |
| distal | 212.7 (93.0, 71.6–565.2) | 52.4 (41.7, 10.5–202.7) | |
| Fat volume, mL | total muscle | 124.7 (*, 58.9–583.3) | 28.5 (11.1, 10.5–59.4) |
| proximal | 29.6 (17.4, 8.2–117.2) | 8.1 (3.4, 2.5–19.0) | |
| middle | 62.6 (41.0, 24.5–296.6) | 15.8 (5.8, 5.1–30.6) | |
| distal | 46.4 (25.7, 19.2–169.5) | 4.7 (4.8, 1.1–32.0) | |
| Contractile tissue volume, mL | total muscle | 706.6 (243.4, 307.2–1454.5) | 265.6 (108.9, 93.9–567.1) |
| proximal | 184.5 (60.9, 85.0–333.4) | 66.9 (26.8, 29.6–138.4) | |
| middle | 355.9 (121.8, 152.1–737.3) | 151.0 (60.0, 52.0–309.7) | |
| distal | 166.3 (79.1, 49.5–464.7) | 47.7 (37.7, 9.3–171.7) |
| Muscle Measurements | Muscle Section | Correlation Analysis, r (p) | |||
|---|---|---|---|---|---|
| M. Erector Spinae, n = 21 | M. Psoas, n = 22 | ||||
| Maximum absolute BMI change, kg/m2 | Correlation with age as control variable | Maximum absolute BMI change, kg/m2 | Correlation with age as control variable | ||
| PDFF, % | total muscle | −0.12 (0.59) | −0.31 (0.18) | −0.29 (0.19) | −0.52 (0.02) |
| proximal | −0.29 (0.21) | −0.42 (0.07) | −0.30 (0.18) | −0.44 (<0.05) | |
| middle | −0.18 (0.44) | −0.31 (0.19) | −0.28 (0.21) | −0.40 (0.08) | |
| distal | 0.08 (0.74) | −0.02 (0.93) | −0.24 (0.29) | −0.36 (0.11) | |
| Muscle volume, mL | total muscle | −0.41 (0.06) | −0.39 (0.09) | −0.25 (0.27) | −0.21 (0.36) |
| proximal | −0.11 (0.64) | −0.14 (0.54) | −0.23 (0.30) | −0.08 (0.72) | |
| middle | −0.43 (<0.05) | −0.43 (0.05) | −0.06 (0.78) | −0.04 (0.88) | |
| distal | −0.44 (0.04) | −0.45 (0.04) | −0.44 (0.04) | −0.36 (0.11) | |
| Fat volume, mL | total muscle | −0.35 (0.12) | −0.46 (0.04) | −0.52 (0.02) | −0.55 (0.01) |
| proximal | −0.49 (0.02) | −0.57 (<0.01) | −0.44 (0.04) | −0.53 (0.01) | |
| middle | −0.36 (0.10) | −0.45 (0.04) | −0.33 (0.13) | −0.36 (0.11) | |
| distal | −0.16 (0.48) | −0.24 (0.30) | −0.56 (<0.01) | −0.40 (0.07) | |
| Contractile tissue volume, mL | total muscle | −0.34 (0.13) | −0.30 (0.20) | −0.22 (0.34) | −0.17 (0.46) |
| proximal | −0.10 (0.67) | −0.04 (0.85) | −0.20 (0.38) | −0.04 (0.88) | |
| middle | −0.38 (0.08) | −0.35 (0.12) | −0.07 (0.75) | −0.01 (0.99) | |
| distal | −0.46 (0.03) | −0.44 (<0.05) | −0.44 (0.04) | −0.35 (0.12) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patzelt, L.; Junker, D.; Syväri, J.; Burian, E.; Wu, M.; Prokopchuk, O.; Nitsche, U.; Makowski, M.R.; Braren, R.F.; Herzig, S.; et al. MRI-Determined Psoas Muscle Fat Infiltration Correlates with Severity of Weight Loss during Cancer Cachexia. Cancers 2021, 13, 4433. https://doi.org/10.3390/cancers13174433
Patzelt L, Junker D, Syväri J, Burian E, Wu M, Prokopchuk O, Nitsche U, Makowski MR, Braren RF, Herzig S, et al. MRI-Determined Psoas Muscle Fat Infiltration Correlates with Severity of Weight Loss during Cancer Cachexia. Cancers. 2021; 13(17):4433. https://doi.org/10.3390/cancers13174433
Chicago/Turabian StylePatzelt, Lisa, Daniela Junker, Jan Syväri, Egon Burian, Mingming Wu, Olga Prokopchuk, Ulrich Nitsche, Marcus R. Makowski, Rickmer F. Braren, Stephan Herzig, and et al. 2021. "MRI-Determined Psoas Muscle Fat Infiltration Correlates with Severity of Weight Loss during Cancer Cachexia" Cancers 13, no. 17: 4433. https://doi.org/10.3390/cancers13174433
APA StylePatzelt, L., Junker, D., Syväri, J., Burian, E., Wu, M., Prokopchuk, O., Nitsche, U., Makowski, M. R., Braren, R. F., Herzig, S., Diaz, M. B., & Karampinos, D. C. (2021). MRI-Determined Psoas Muscle Fat Infiltration Correlates with Severity of Weight Loss during Cancer Cachexia. Cancers, 13(17), 4433. https://doi.org/10.3390/cancers13174433