
Oncologic Imaging of the Lymphatic System: Current Perspective with Multi-Modality Imaging and New Horizon

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
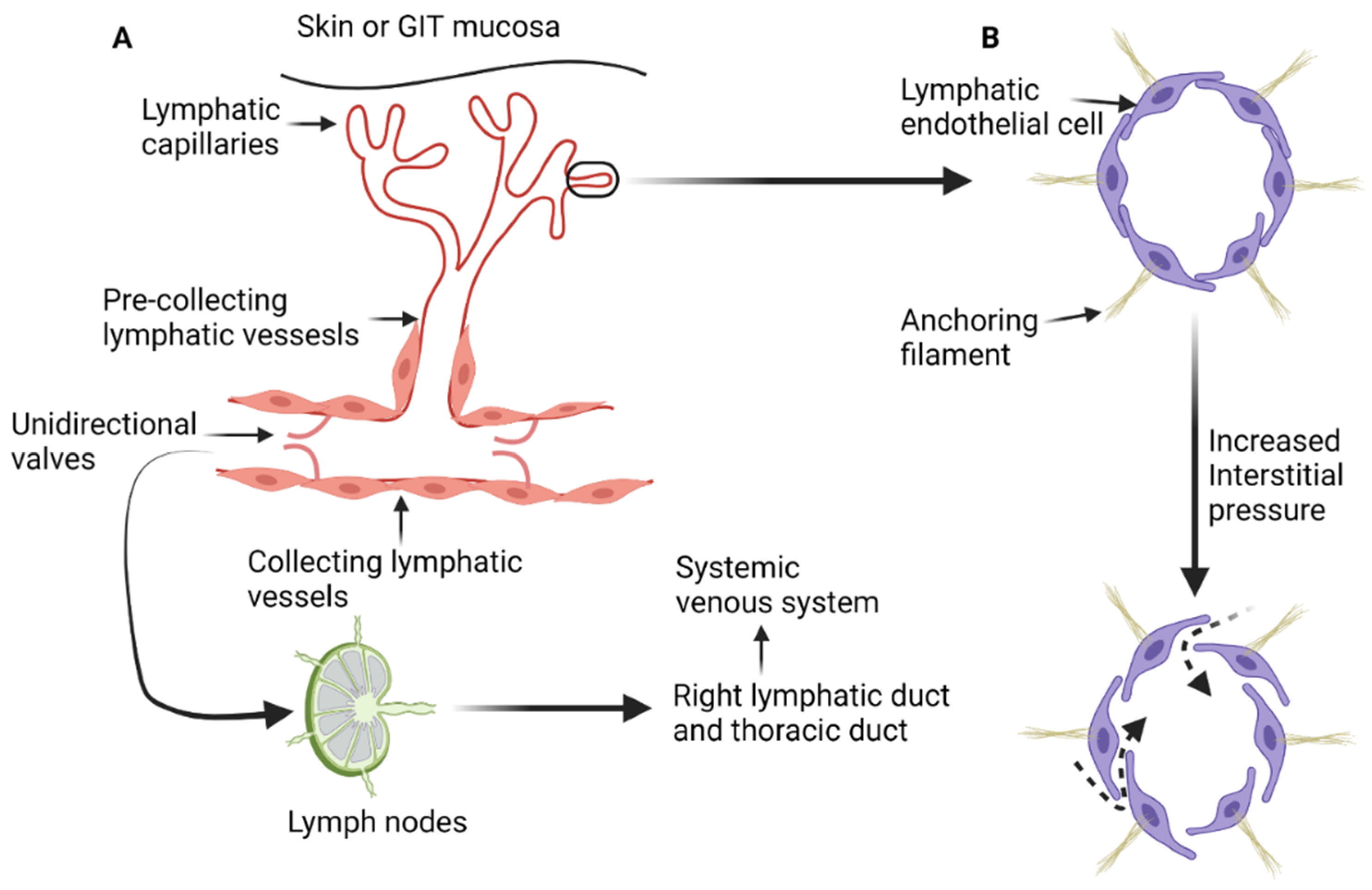
2. Microscopic Anatomy and Physiology of the Lymphatic System
2.1. Lymphatic Anatomy of the Abdomen, Pelvis and Lower Extremities
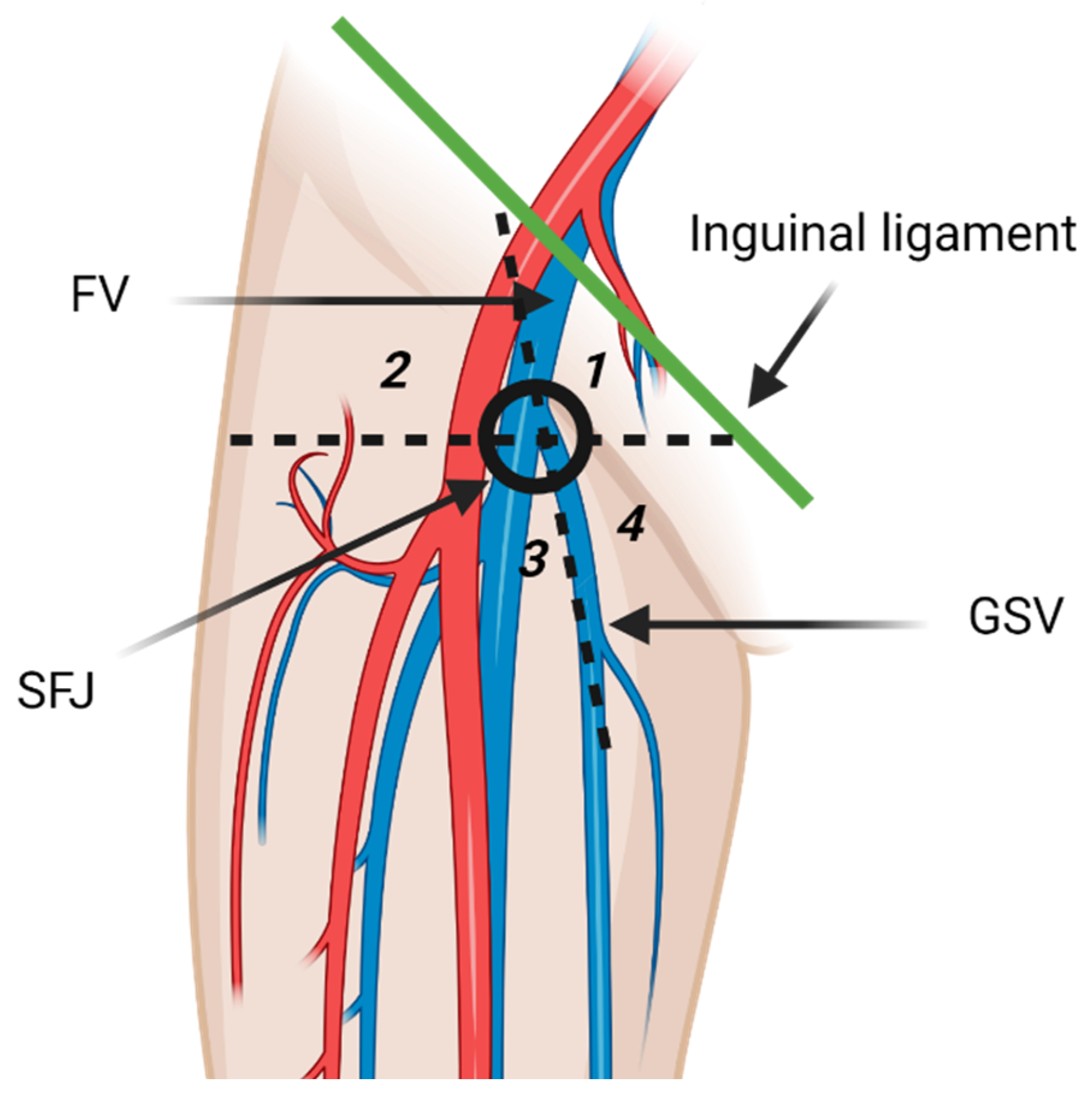
2.1.1. Inguinal and Popliteal Lymph Nodes and Lower Extremity Lymphatic Drainage Pathways
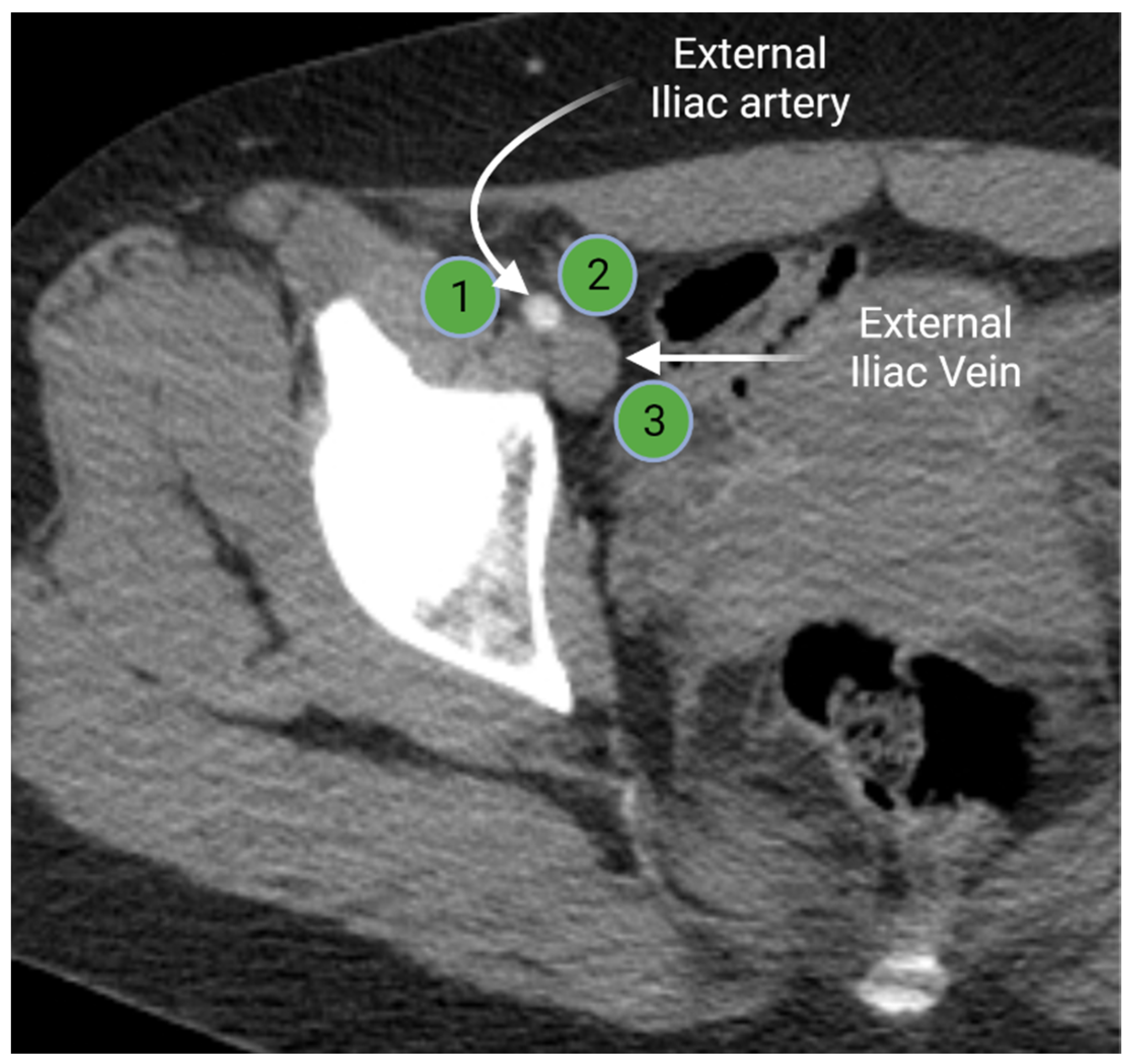
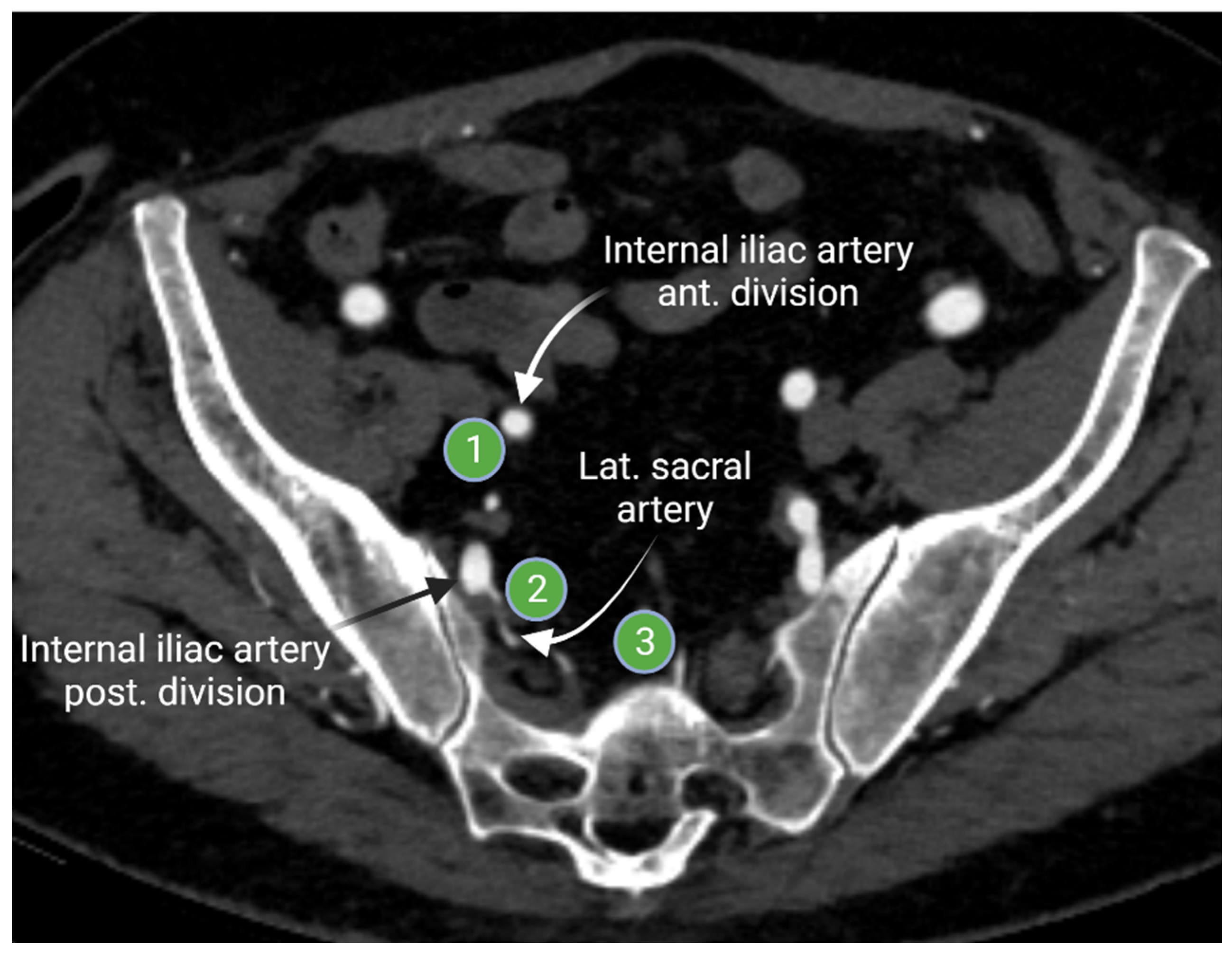
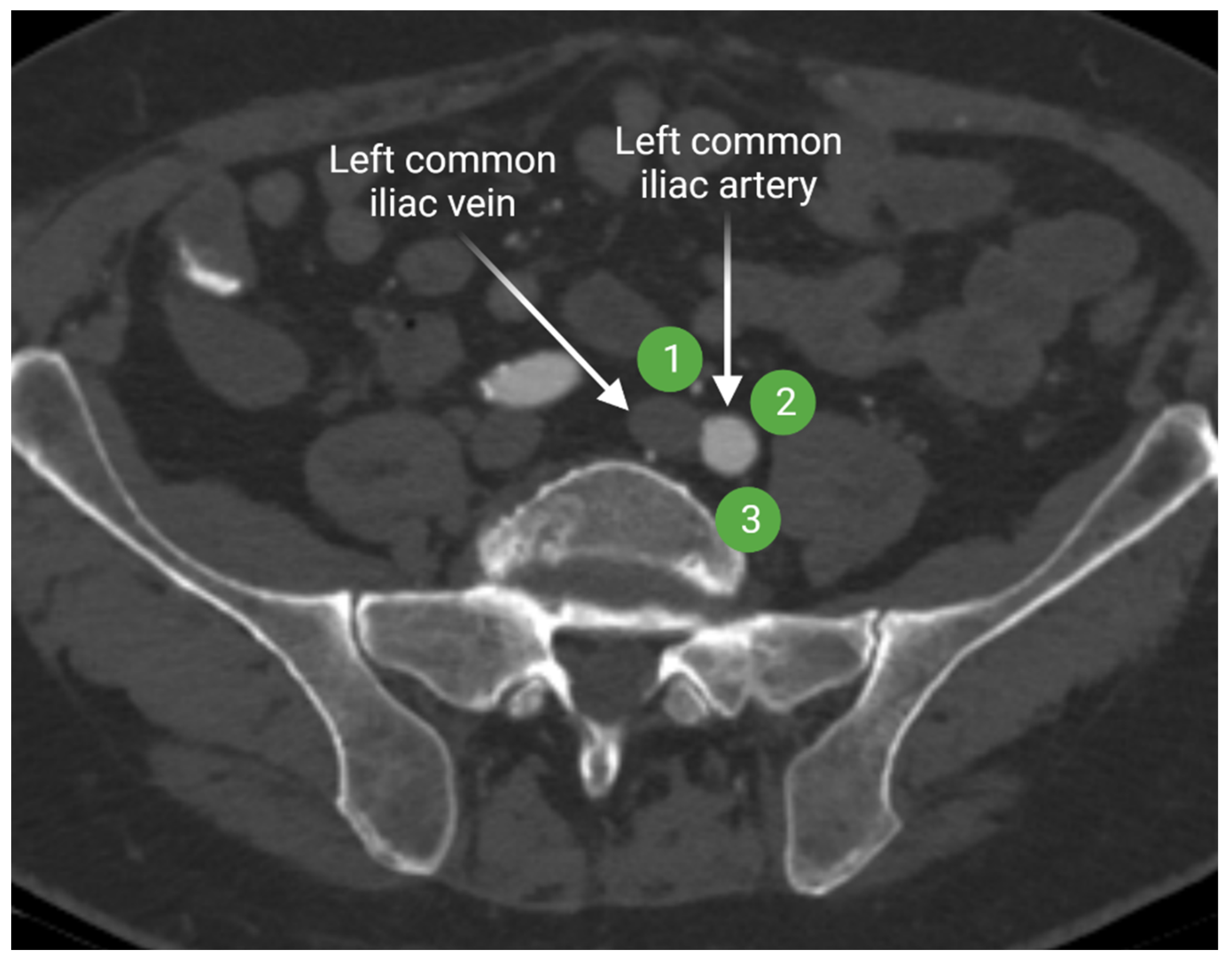
2.1.2. Iliac Lymph Nodes Anatomy
2.1.3. Peri-Aortic Lymph Node Anatomy
2.1.4. Anatomy of the Visceral/Digestive Lymph Nodes
3. Lymphatic Spread of Cancer
4. Radiologic Evaluation of the Lymphatic System in Cancer Patients
4.1. Cross-Sectional Evaluation of the Lymphatic System
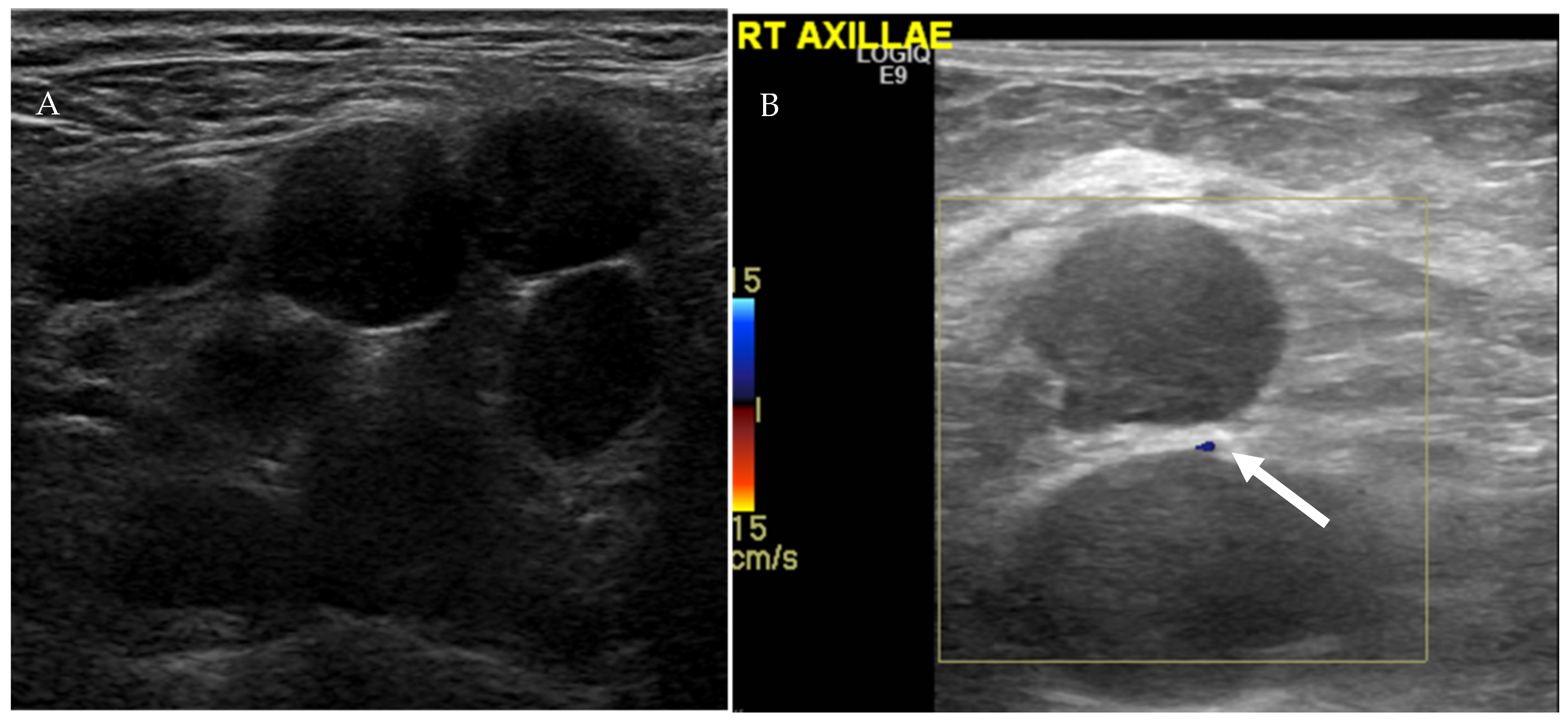
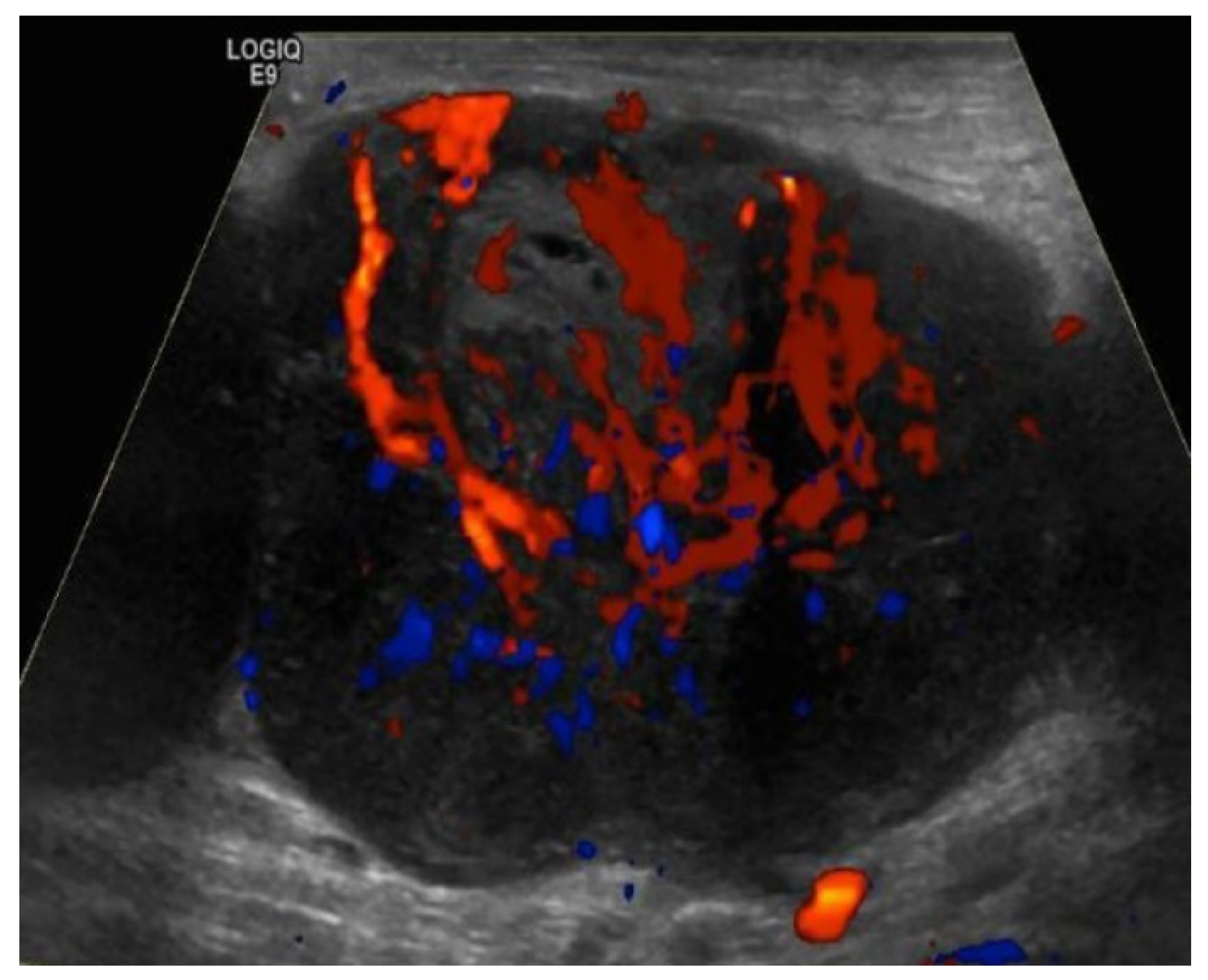
4.1.1. Ultrasound Evaluation of the Lymphatic System
4.1.2. Computed Tomography (CT) and Conventional Magnetic Resonance Imaging (MRI) of the Lymphatic System
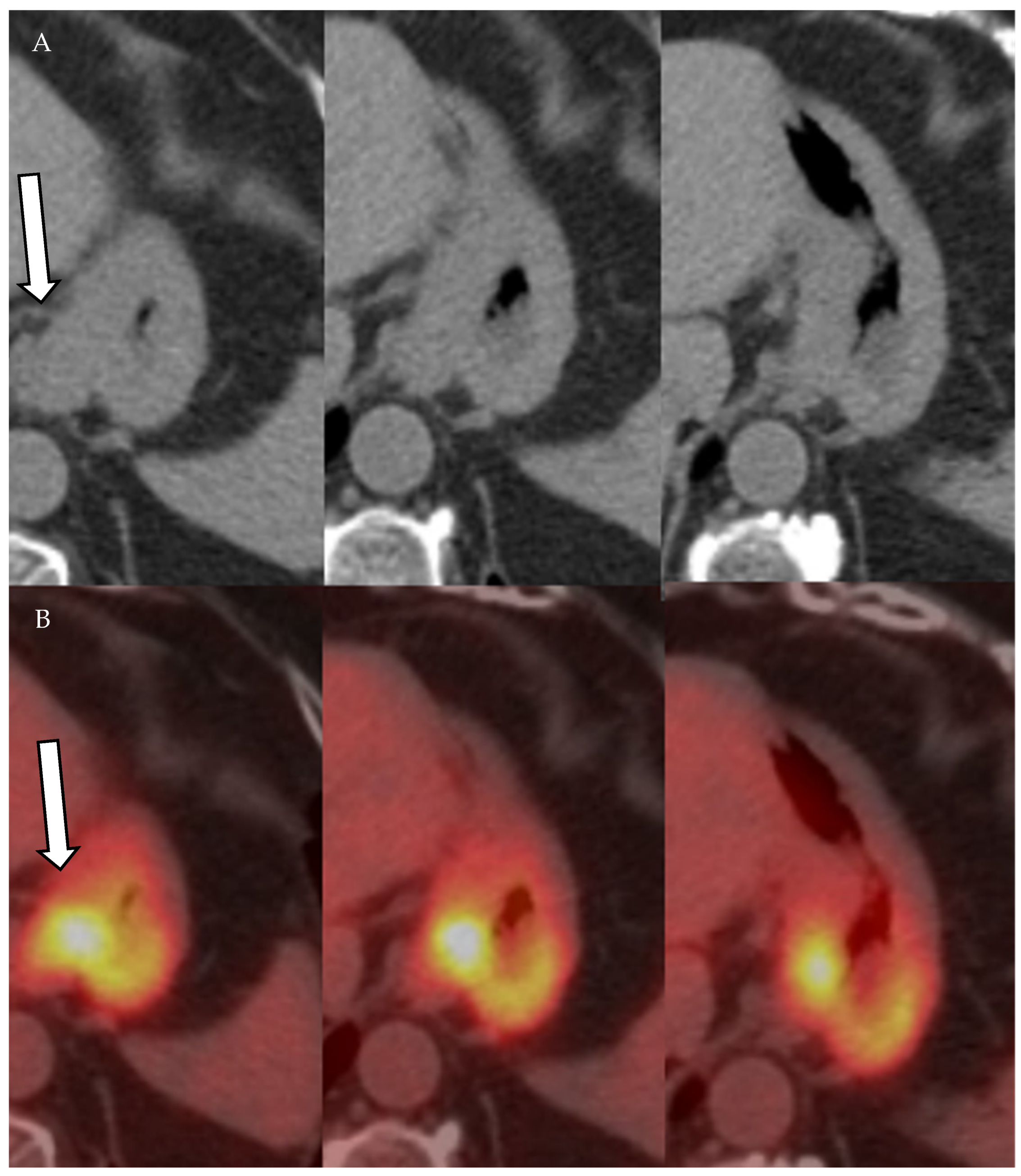
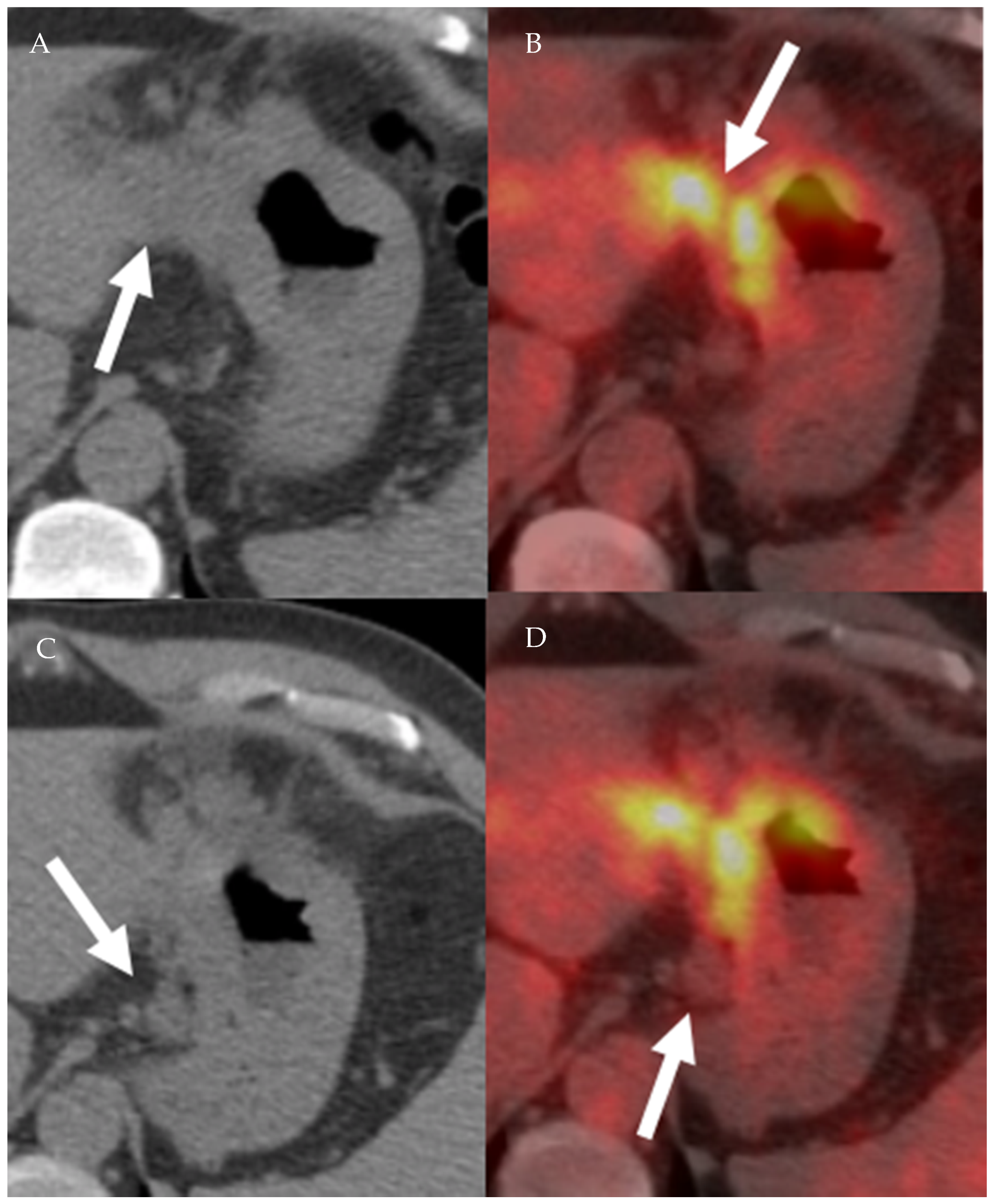
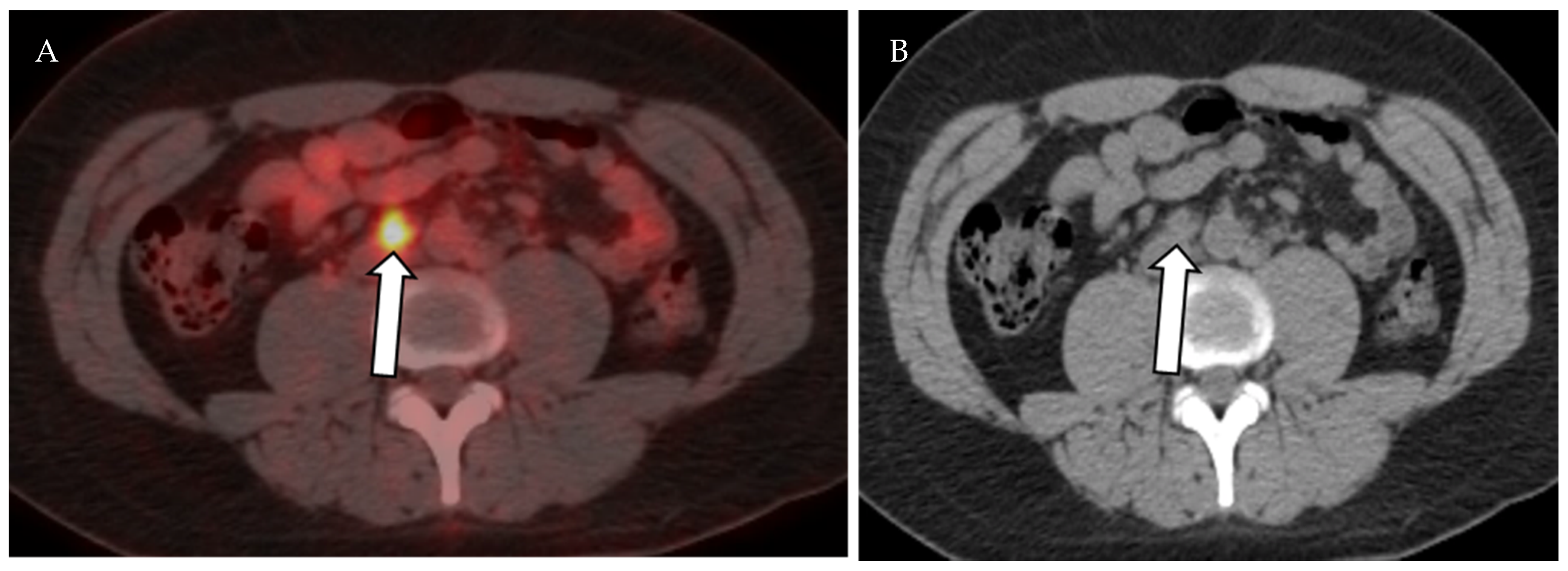
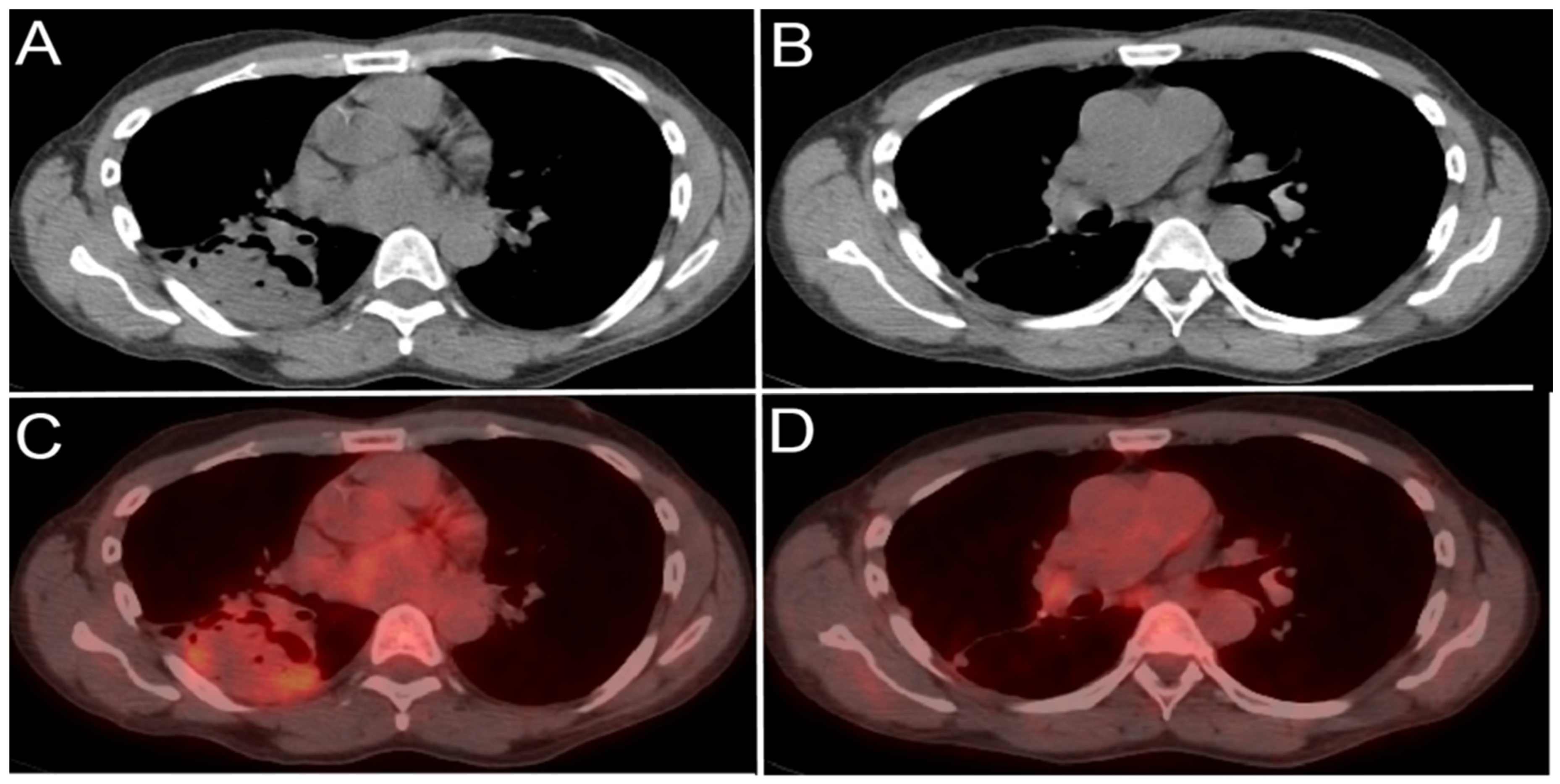
4.1.3. Positron Emission Tomography (PET) and Positron Emission Tomography-Computed Tomography (PET-CT)
4.2. Vascular Imaging of the Lymphatic System
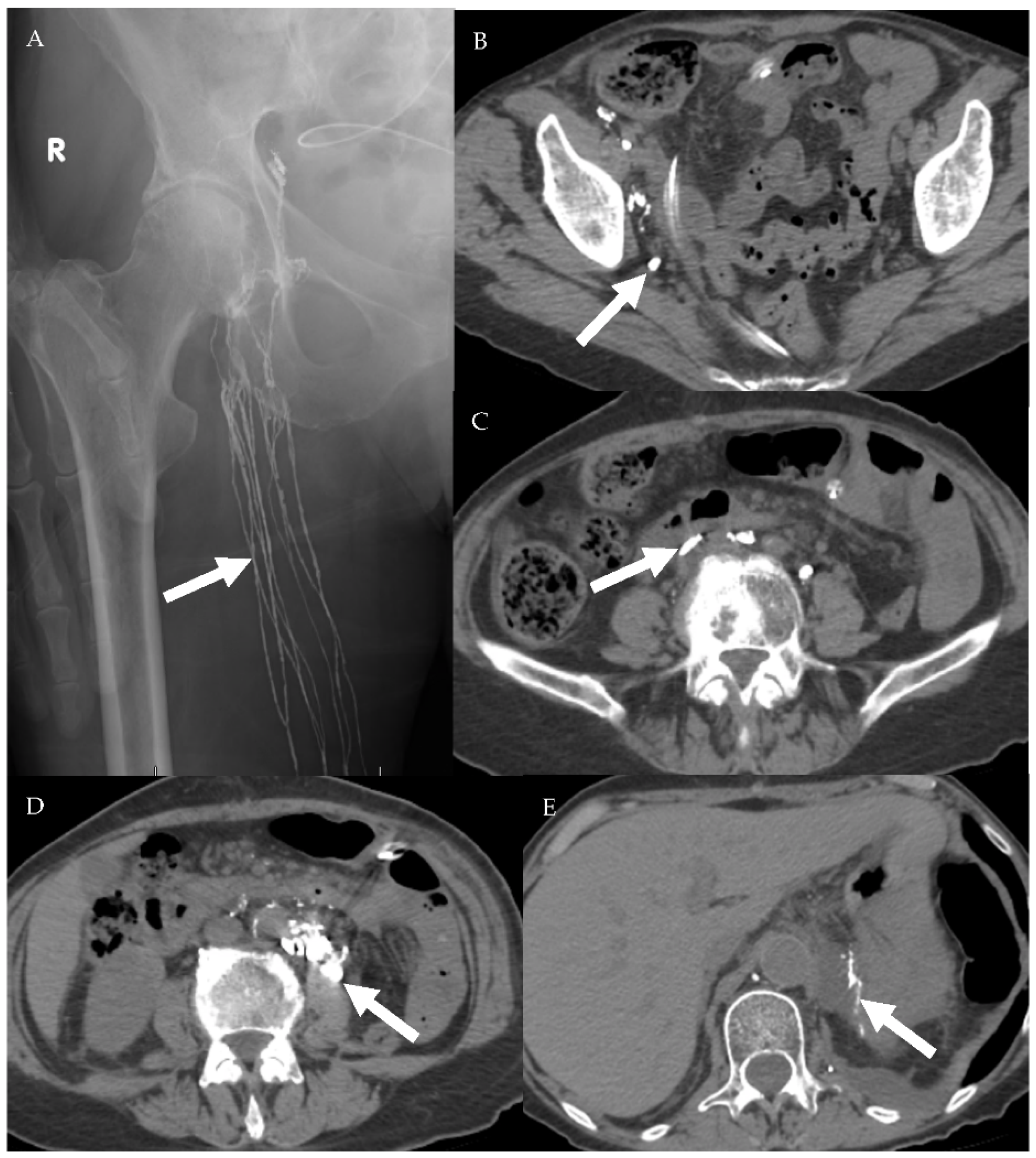
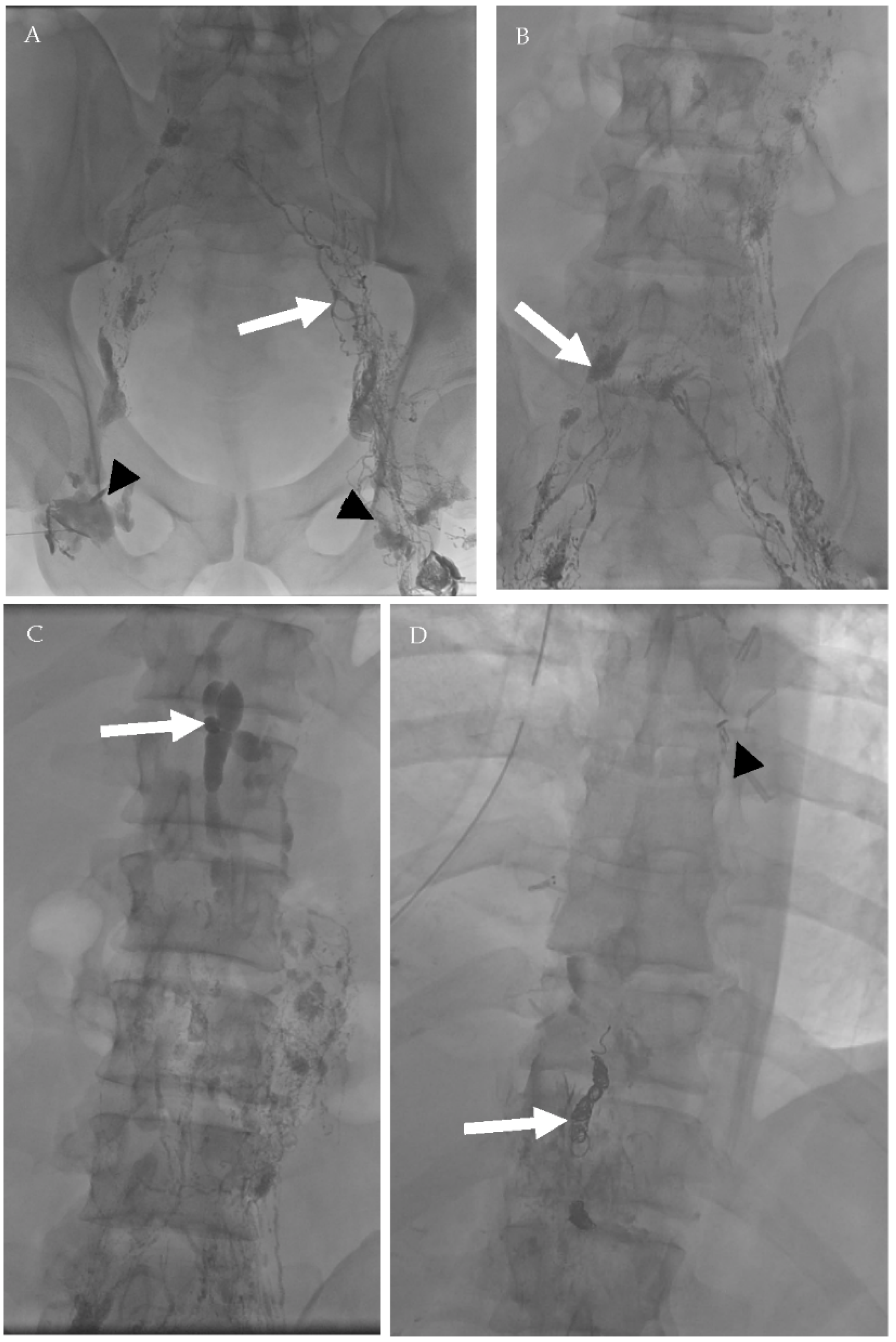
4.2.1. Conventional Lymphangiography (CL)
4.2.2. Magnetic Resonance Lymphangiogram (MRL)
4.2.3. Ultrasmall Superparamagnetic Particles of Iron Oxide (USPIO) MRL
4.3. Sentinel Lymph Node (SNL) Imaging
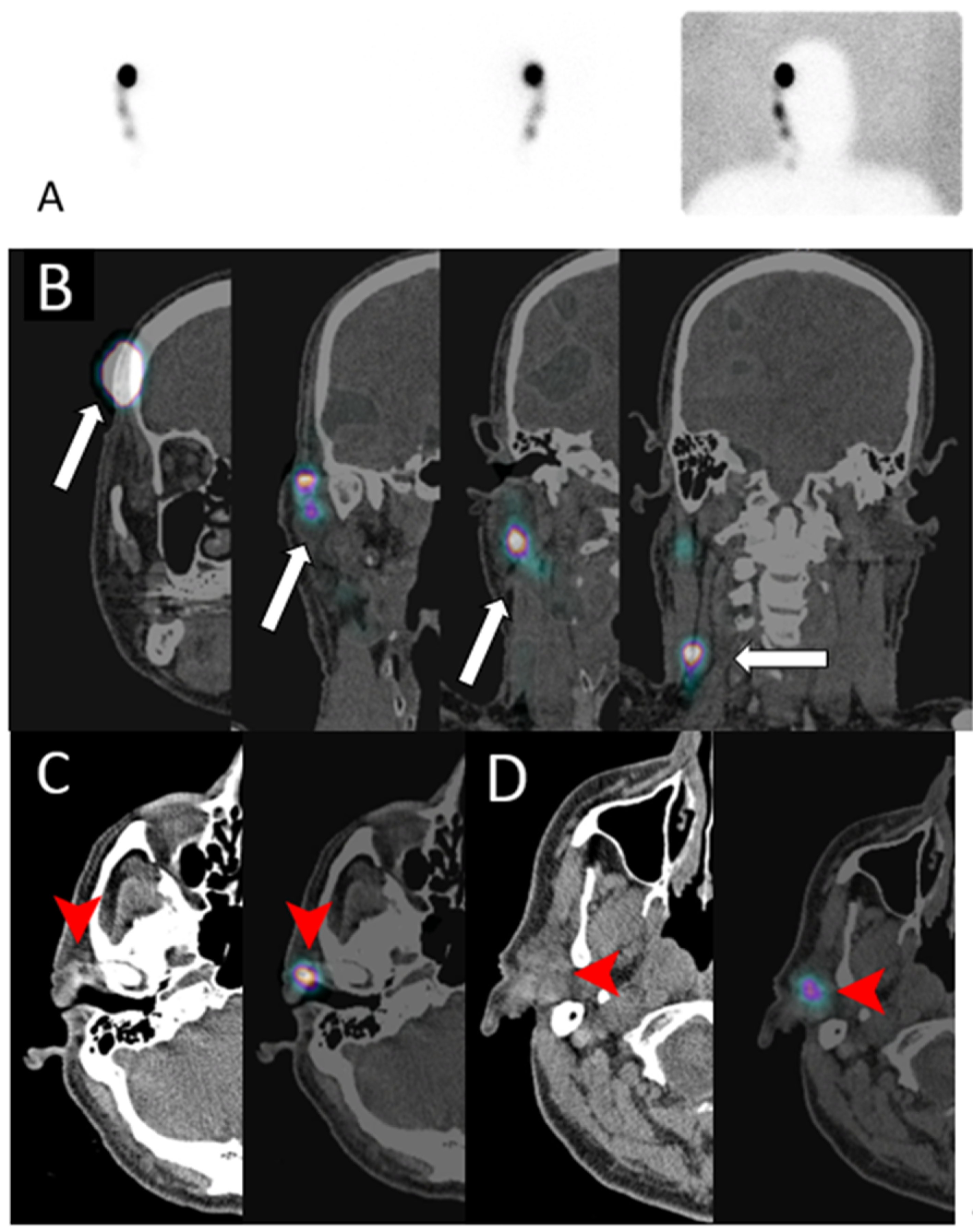
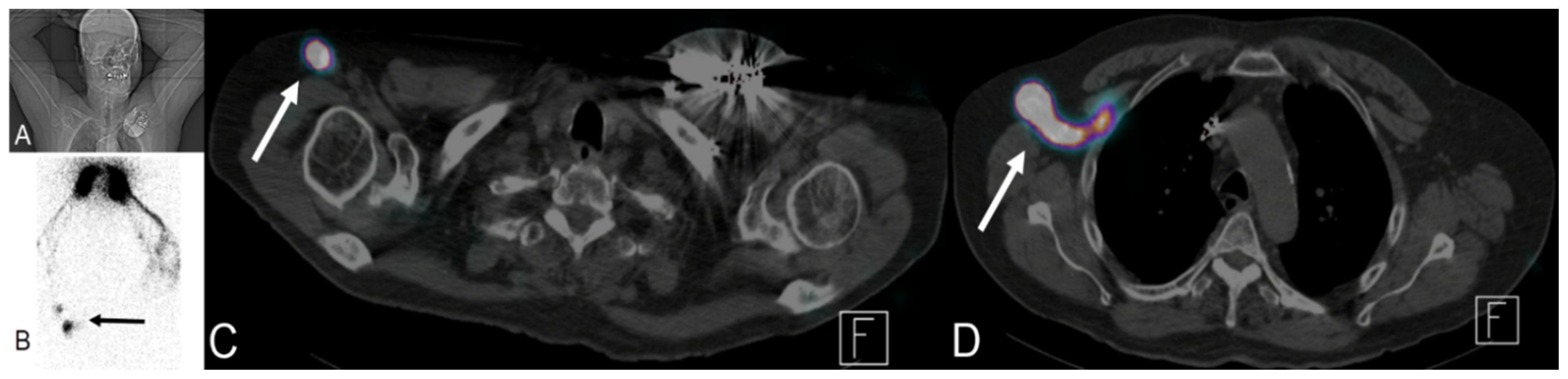
Lymphoscintigraphy
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Al-Kofahi, M.; Yun, J.W.; Minagar, A.; Alexander, J.S. Anatomy and roles of lymphatics in inflammatory diseases. Clin. Exp. Neuroimmunol. 2017, 8, 199–214. [Google Scholar] [CrossRef] [Green Version]
- Scaglioni, M.F.; Suami, H. Anatomy of the Lymphatic System and the Lymphosome Concept with Reference to Lymphedema. Semin. Plast. Surg. 2018, 32, 5–11. [Google Scholar] [CrossRef]
- Hsu, M.C.; Itkin, M. Lymphatic Anatomy. Tech. Vasc. Interv. Radiol. 2016, 19, 247–254. [Google Scholar] [CrossRef]
- Tammela, T.; Alitalo, K. Lymphangiogenesis: Molecular Mechanisms and Future Promise. Cell 2010, 140, 460–476. [Google Scholar] [CrossRef] [Green Version]
- Dellinger, M.T.; Witte, M.H. Lymphangiogenesis, lymphatic systemomics, and cancer: Context, advances and unanswered questions. Clin. Exp. Metastasis 2018, 35, 419–424. [Google Scholar] [CrossRef] [Green Version]
- Mandriota, S.J.; Jussila, L.; Jeltsch, M.; Compagni, A.; Baetens, D.; Prevo, R.; Banerji, S.; Huarte, J.; Montesano, R.; Jackson, D.G.; et al. Vascular endothelial growth factor-C-mediated lymphangiogenesis promotes tumour metastasis. EMBO J. 2001, 20, 672–682. [Google Scholar] [CrossRef] [Green Version]
- Stacker, S.A.; Caesar, C.; Baldwin, M.E.; Thornton, G.E.; Williams, R.A.; Prevo, R.; Jackson, D.G.; Nishikawa, S.-I.; Kubo, H.; Achen, M.G. VEGF-D promotes the metastatic spread of tumor cells via the lymphatics. Nat. Med. 2001, 7, 186–191. [Google Scholar] [CrossRef]
- Clément, O.; Luciani, A. Imaging the lymphatic system: Possibilities and clinical applications. Eur. Radiol. 2004, 14, 1498–1507. [Google Scholar] [CrossRef]
- Barrett, T.; Choyke, P.L.; Kobayashi, H. Imaging of the lymphatic system: New horizons. Contrast Media Mol. Imaging 2006, 1, 230–245. [Google Scholar] [CrossRef] [PubMed]
- Munn, L.L.; Padera, T.P. Imaging the lymphatic system. Microvasc. Res. 2014, 96, 55–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baluk, P.; Fuxe, J.; Hashizume, H.; Romano, T.; Lashnits, E.; Butz, S.; Vestweber, D.; Corada, M.; Molendini, C.; Dejana, E.; et al. Functionally specialized junctions between endothelial cells of lymphatic vessels. J. Exp. Med. 2007, 204, 2349–2362. [Google Scholar] [CrossRef]
- Schulte-Merker, S.; Sabine, A.; Petrova, T.V. Lymphatic vascular morphogenesis in development, physiology, and disease. J. Cell Biol. 2011, 193, 607–618. [Google Scholar] [CrossRef] [Green Version]
- Shinaoka, A.; Koshimune, S.; Suami, H.; Yamada, K.; Kumagishi, K.; Boyages, J.; Kimata, Y.; Ohtsuka, A. Lower-Limb Lymphatic Drainage Pathways and Lymph Nodes: A CT Lymphangiography Cadaver Study. Radiology 2020, 294, 223–229. [Google Scholar] [CrossRef]
- Yamazaki, S.; Suami, H.; Imanishi, N.; Aiso, S.; Yamada, M.; Jinzaki, M.; Kuribayashi, S.; Chang, D.W.; Kishi, K. Three-dimensional demonstration of the lymphatic system in the lower extremities with multi-detector-row computed tomography: A study in a cadaver model. Clin. Anat. 2013, 26, 258–266. [Google Scholar] [CrossRef]
- McMahon, C.J.; Rofsky, N.M.; Pedrosa, I. Lymphatic Metastases from Pelvic Tumors: Anatomic Classification, Characterization, and Staging. Radiology 2010, 254, 31–46. [Google Scholar] [CrossRef]
- Park, J.M.; Charnsangavej, C.; Yoshimitsu, K.; Herron, D.H.; Robinson, T.J.; Wallace, S. Pathways of nodal metastasis from pelvic tumors: CT demonstration. Radiographics 1994, 14, 1309–1321. [Google Scholar] [CrossRef] [Green Version]
- Lengelé, B.; Nyssen-Behets, C.; Scalliet, P. Anatomical bases for the radiological delineation of lymph node areas. Upper limbs, chest and abdomen. Radiother. Oncol. 2007, 84, 335–347. [Google Scholar] [CrossRef]
- Chavhan, G.B.; Amaral, J.G.; Temple, M.; Itkin, M. MR Lymphangiography in Children: Technique and Potential Applications. Radiographics 2017, 37, 1775–1790. [Google Scholar] [CrossRef] [Green Version]
- Skobe, M.; Hawighorst, T.; Jackson, D.G.; Prevo, R.; Janes, L.; Velasco, P.; Riccardi, L.; Alitalo, K.; Claffey, K.; Detmar, M. Induction of tumor lymphangiogenesis by VEGF-C promotes breast cancer metastasis. Nat. Med. 2001, 7, 192–198. [Google Scholar] [CrossRef]
- Prativadi, R.; Dahiya, N.; Kamaya, A.; Bhatt, S. Chapter 5 Ultrasound Characteristics of Benign vs Malignant Cervical Lymph Nodes. Semin. Ultrasound CT MRI 2017, 38, 506–515. [Google Scholar] [CrossRef]
- Wang, B.; Zhang, M.K.; Zhou, M.P.; Liu, Y.; Li, N.; Liu, G.; Wang, Z.L. Logistic Regression Analysis of Conventional Ultrasound, and Contrast-Enhanced Ultrasound Characteristics. J. Ultrasound Med. 2021. [Google Scholar] [CrossRef]
- Dudea, S.M.; Lenghel, M.; Botar-Jid, C.; Vasilescu, D.; Duma, M. Ultrasonography of superficial lymph nodes: Benign vs. malignant. Med. Ultrason. 2012, 14, 294–306. [Google Scholar]
- Vassallo, P.; Wernecke, K.; Roos, N.; E Peters, P. Differentiation of benign from malignant superficial lymphadenopathy: The role of high-resolution US. Radiology 1992, 183, 215–220. [Google Scholar] [CrossRef]
- Ahuja, A.; Ying, M. Sonographic evaluation of cervical lymphadenopathy: Is power Doppler sonography routinely indicated? Ultrasound Med. Biol. 2003, 29, 353–359. [Google Scholar] [CrossRef]
- Ahuja, A.T. Ultrasound of malignant cervical lymph nodes. Cancer Imaging 2008, 8, 48–56. [Google Scholar] [CrossRef] [Green Version]
- Rubaltelli, L.; Khadivi, Y.; Tregnaghi, A.; Stramare, R.; Ferro, F.; Borsato, S.; Fiocco, U.; Adami, F.; Rossi, C.R. Evaluation of lymph node perfusion using continuous mode harmonic ultrasonography with a second-generation contrast agent. J. Ultrasound Med. 2004, 23, 829–836. [Google Scholar] [CrossRef]
- Cui, X.-W. New ultrasound techniques for lymph node evaluation. World J. Gastroenterol. 2013, 19, 4850–4860. [Google Scholar] [CrossRef] [PubMed]
- Rubaltelli, L.; Beltrame, V.; Tregnaghi, A.; Scagliori, E.; Frigo, A.C.; Stramare, R. Contrast-Enhanced Ultrasound for Characterizing Lymph Nodes With Focal Cortical Thickening in Patients With Cutaneous Melanoma. Am. J. Roentgenol. 2011, 196, W8–W12. [Google Scholar] [CrossRef]
- Wan, C.F.; Du, J.; Fang, H.; Li, F.H.; Zhu, J.S.; Liu, Q. Enhancement Patterns and Parameters of Breast Cancers at Contrast-enhanced US: Correlation with Prognostic Factors. Radiology 2012, 262, 450–459. [Google Scholar] [CrossRef]
- Yu, M.; Liu, Q.; Song, H.-P.; Han, Z.-H.; Su, H.-L.; He, G.-B.; Zhou, X.-D. Clinical Application of Contrast-Enhanced Ultrasonography in Diagnosis of Superficial Lymphadenopathy. J. Ultrasound Med. 2010, 29, 735–740. [Google Scholar] [CrossRef]
- Ouyang, Q.; Chen, L.; Zhao, H.; Xu, R.; Lin, Q. Detecting Metastasis of Lymph Nodes and Predicting Aggressiveness in Patients With Breast Carcinomas. J. Ultrasound Med. 2010, 29, 343–352. [Google Scholar] [CrossRef]
- Chen, L.; Chen, L.; Liu, J.; Wang, B.; Zhang, H. Value of Qualitative and Quantitative Contrast-Enhanced Ultrasound Analysis in Preoperative Diagnosis of Cervical Lymph Node Metastasis From Papillary Thyroid Carcinoma. J. Ultrasound Med. 2020, 39, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Nakase, K.; Yamamoto, K.; Hiasa, A.; Tawara, I.; Yamaguchi, M.; Shiku, H. Contrast-enhanced ultrasound examination of lymph nodes in different types of lymphoma. Cancer Detect. Prev. 2006, 30, 188–191. [Google Scholar] [CrossRef] [PubMed]
- Ahuja, A.T.; Ying, M. Sonographic Evaluation of Cervical Lymph Nodes. Am. J. Roentgenol. 2005, 184, 1691–1699. [Google Scholar] [CrossRef]
- Luciani, A.; Itti, E.; Rahmouni, A.; Meignan, M.; Clement, O. Lymph node imaging: Basic principles. Eur. J. Radiol. 2006, 58, 338–344. [Google Scholar] [CrossRef]
- Grey, A.; Carrington, B.; Hulse, P.; Swindell, R.; Yates, W. Magnetic Resonance Appearance of Normal Inguinal Nodes. Clin. Radiol. 2000, 55, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Brown, G.; Richards, C.J.; Bourne, M.W.; Newcombe, R.G.; Radcliffe, A.G.; Dallimore, N.S.; Williams, G.T. Morphologic Predictors of Lymph Node Status in Rectal Cancer with Use of High-Spatial-Resolution MR Imaging with Histopathologic Comparison. Radiology 2003, 227, 371–377. [Google Scholar] [CrossRef]
- Fukuda, H.; Nakagawa, T.; Shibuya, H. Metastases to pelvic lymph nodes from carcinoma in the pelvic cavity: Diagnosis using thin-section CT. Clin. Radiol. 1999, 54, 237–242. [Google Scholar] [CrossRef]
- Oyen, R.H.; Van Poppel, H.P.; E Ameye, F.; A Van De Voorde, W.; Baert, A.L.; Baert, L.V. Lymph node staging of localized prostatic carcinoma with CT and CT-guided fine-needle aspiration biopsy: Prospective study of 285 patients. Radiology 1994, 190, 315–322. [Google Scholar] [CrossRef]
- Hilton, S.; Herr, H.W.; Teitcher, J.B.; Begg, C.B.; Castéllino, R.A. CT detection of retroperitoneal lymph node metastases in patients with clinical stage I testicular nonseminomatous germ cell cancer: Assessment of size and distribution criteria. Am. J. Roentgenol. 1997, 169, 521–525. [Google Scholar] [CrossRef] [Green Version]
- Vinnicombe, S.; Norman, A.R.; Nicolson, V.; Husband, J.E. Normal pelvic lymph nodes: Evaluation with CT after bipedal lymphangiography. Radiology 1995, 194, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Mittra, E.; Quon, A. Positron Emission Tomography/Computed Tomography: The Current Technology and Applications. Radiol. Clin. N. Am. 2009, 47, 147–160. [Google Scholar] [CrossRef]
- Vallabhajosula, S. 18F-Labeled Positron Emission Tomographic Radiopharmaceuticals in Oncology: An Overview of Radiochemistry and Mechanisms of Tumor Localization. Semin. Nucl. Med. 2007, 37, 400–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, B.; Gao, S.; Li, S. A Comprehensive Comparison of CT, MRI, Positron Emission Tomography or Positron Emission Tomogra-phy/CT, and Diffusion Weighted Imaging-MRI for Detecting the Lymph Nodes Metastases in Patients with Cervical Cancer: A Me-ta-Analysis Based on 67 Studies. Gynecol. Obstet. Investig. 2017, 82, 209–222. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.J.; Ju, W.; Myung, S.-K.; Kim, Y. Diagnostic performance of computer tomography, magnetic resonance imaging, and positron emission tomography or positron emission tomography/computer tomography for detection of metastatic lymph nodes in patients with cervical cancer: Meta-analysis. Cancer Sci. 2010, 101, 1471–1479. [Google Scholar] [CrossRef]
- Riegger, C.; Koeninger, A.; Hartung, V.; Otterbach, F.; Kimmig, R.; Forsting, M.; Bockisch, A.; Antoch, G.; Heusner, T.A. Comparison of the Diagnostic Value of FDG-PET/CT and Axillary Ultrasound for the Detection of Lymph Node Metastases in Breast Cancer Patients. Acta Radiol. 2012, 53, 1092–1098. [Google Scholar] [CrossRef] [PubMed]
- Cochet, A.; Dygai-Cochet, I.; Riedinger, J.-M.; Humbert, O.; Berriolo-Riedinger, A.; Toubeau, M.; Guiu, S.; Coutant, C.; Coudert, B.; Fumoleau, P.; et al. 18F-FDG PET/CT provides powerful prognostic stratification in the primary staging of large breast cancer when compared with conventional explorations. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 428–437. [Google Scholar] [CrossRef]
- Itkin, M.; Kucharczuk, J.C.; Kwak, A.; Trerotola, S.O.; Kaiser, L.R. Nonoperative thoracic duct embolization for traumatic thoracic duct leak: Experience in 109 patients. J. Thorac. Cardiovasc. Surg. 2010, 139, 584–590. [Google Scholar] [CrossRef] [Green Version]
- Cope, C.; Kaiser, L.R. Management of unremitting chylothorax by percutaneous embolization and blockage of retroperitoneal lym-phatic vessels in 42 patients. J. Vasc. Interv. Radiol. 2002, 13, 1139–1148. [Google Scholar] [CrossRef]
- Nadolski, G.J.; Itkin, M. Feasibility of Ultrasound-guided Intranodal Lymphangiogram for Thoracic Duct Embolization. J. Vasc. Interv. Radiol. 2012, 23, 613–616. [Google Scholar] [CrossRef]
- Rajebi, M.R.; Chaudry, G.; Padua, H.M.; Dillon, B.; Yilmaz, S.; Arnold, R.W.; Landrigan-Ossar, M.F.; Alomari, A.I. Intranodal Lymphangiography: Feasibility and Preliminary Experience in Children. J. Vasc. Interv. Radiol. 2011, 22, 1300–1305. [Google Scholar] [CrossRef]
- Von Eschenbach, A.C.; Jing, B.S.; Wallace, S. Lymphangiography in genitourinary cancer. Urol. Clin. N. Am. 1985, 12, 715–723. [Google Scholar] [CrossRef]
- Litwin, S.B.; Fraley, E.E.; Clouse, M.E.; Ulfelder, H. Lymphography in Patients with Pelvic Cancer. Obstet. Gynecol. 1964, 24, 809–816. [Google Scholar]
- Lang, J.H. Lymphangiography in ovarian cancer. Zhonghua Fu Chan Ke Za Zhi 1989, 24, 29–31. [Google Scholar] [PubMed]
- Baz, A.A.; Hassan, T.; Atta, A.; El Kholy, M.S. Role of contrast enhanced MRI lymphangiography in evaluation of lower extremity lymphatic vessels for patients with primary lymphedema. Egypt. J. Radiol. Nucl. Med. 2018, 49, 776–781. [Google Scholar] [CrossRef]
- Mazzei, F.G.; Gentili, F.; Guerrini, S.; Squitieri, N.C.; Guerrieri, D.; Gennaro, P.; Scialpi, M.; Volterrani, L.; Mazzei, M.A. MR Lymphangiography: A Practical Guide to Perform It and a Brief Review of the Literature from a Technical Point of View. BioMed. Res. Int. 2017, 2017, 2598358. [Google Scholar] [CrossRef]
- Derhy, S.; El Mouhadi, S.; Monnier-Cholley, L.; Menu, Y.; Becker, C.; Arrivé, L. Noncontrast Magnetic Resonance Lymphography. J. Reconstr. Microsurg. 2015, 32, 80–86. [Google Scholar] [CrossRef] [Green Version]
- Arrivé, L.; Derhy, S.; Dahan, B.; El Mouhadi, S.; Monnier-Cholley, L.; Menu, Y.; Becker, C. Primary lower limb lymphoedema: Classification with non-contrast MR lymphography. Eur. Radiol. 2018, 28, 291–300. [Google Scholar] [CrossRef] [PubMed]
- Bellin, M.F.; Lebleu, L.; Meric, J.B. Evaluation of retroperitoneal and pelvic lymph node metastases with MRI and MR lymphan-giography. Abdom Imaging 2003, 28, 155–163. [Google Scholar] [CrossRef]
- Harisinghani, M.G.; Barentsz, J.; Hahn, P.F.; Deserno, W.M.; Tabatabaei, S.; Van De Kaa, C.H.; De La Rosette, J.; Weissleder, R. Noninvasive Detection of Clinically Occult Lymph-Node Metastases in Prostate Cancer. N. Engl. J. Med. 2003, 348, 2491–2499. [Google Scholar] [CrossRef] [Green Version]
- Weissleder, R.; Elizondo, G.; Wittenberg, J.; Rabito, C.A.; Bengele, H.H.; Josephson, L. Ultrasmall superparamagnetic iron oxide: Characterization of a new class of contrast agents for MR imaging. Radiology 1990, 175, 489–493. [Google Scholar] [CrossRef]
- Guimaraes, R.; Clement, O.; Bittoun, J.; Carnot, F.; Frija, G. MR lymphography with superparamagnetic iron nanoparticles in rats: Pathologic basis for contrast enhancement. Am. J. Roentgenol. 1994, 162, 201–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anzai, Y.; Blackwell, K.E.; Hirschowitz, S.L.; Rogers, J.W.; Sato, Y.; Yuh, W.T.; Runge, V.M.; Morris, M.R.; McLachlan, S.J.; Lufkin, R.B. Initial clinical experience with dextran-coated superparamagnetic iron oxide for detection of lymph node metastases in patients with head and neck cancer. Radiology 1994, 192, 709–715. [Google Scholar] [CrossRef] [PubMed]
- Pannu, H.K.; Wang, K.-P.; Borman, T.L.; Bluemke, D.A. MR imaging of mediastinal lymph nodes: Evaluation using a superparamagnetic contrast agent. J. Magn. Reson. Imaging 2000, 12, 899–904. [Google Scholar] [CrossRef]
- Morton, D.L.; Wen, D.-R.; Wong, J.H.; Economou, J.S.; Cagle, L.A.; Storm, F.K.; Foshag, L.J.; Cochran, A.J. Technical Details of Intraoperative Lymphatic Mapping for Early Stage Melanoma. Arch. Surg. 1992, 127, 392–399. [Google Scholar] [CrossRef]
- Morton, D.L.; Wen, D.R.; Foshag, L.J.; Essner, R.; Cochran, A. Intraoperative lymphatic mapping and selective cervical lymphadenectomy for early-stage melanomas of the head and neck. J. Clin. Oncol. 1993, 11, 1751–1756. [Google Scholar] [CrossRef]
- Albertini, J.J.; Lyman, G.H.; Cox, C.; Yeatman, T.; Balducci, L.; Ku, N.; Shivers, S.; Berman, C.; Wells, K.; Rapaport, D.; et al. Lymphatic mapping and sentinel node biopsy in the patient with breast cancer. JAMA 1996, 276, 1818–1822. [Google Scholar] [CrossRef] [PubMed]
- Intenzo, C.M.; Truluck, C.A.; Kushen, M.C.; Kim, S.M.; Berger, A.; Kairys, J.C. Lymphoscintigraphy in Cutaneous Melanoma: An Updated Total Body Atlas of Sentinel Node Mapping. Radiographics 2009, 29, 1125–1135. [Google Scholar] [CrossRef] [PubMed]
- Uren, R.F.; Howman-Giles, R.; Chung, D.; Thompson, J.F. Imaging Sentinel Lymph Nodes. Cancer J. 2015, 21, 25–32. [Google Scholar] [CrossRef]
- Olmos, R.A.V.; Hoefnagel, C.A.; Nieweg, O.E.; Jansen, L.; Rutgers, E.J.; Borger, J.; Horenblas, S.; Kroon, B.B. Lymphoscintigraphy in oncology: A rediscovered challenge. Eur. J. Nucl. Med. Mol. Imaging 1999, 26 (Suppl. 4), S2–S10. [Google Scholar] [CrossRef]
- Maza, S.; Valencia, R.; Geworski, L.; Sandrock, D.; Zander, A.; Audring, H.; Dräger, E.; Winter, H.; Sterry, W.; Munz, D.L. Influence of fast lymphatic drainage on metastatic spread in cutaneous malignant melanoma: A prospective feasibility study. Eur. J. Nucl. Med. Mol. Imaging 2003, 30, 538–544. [Google Scholar] [CrossRef]
- Cammilleri, S.; Jacob, T.; Rojat-Habib, M.C.; Hesse, S.; Berthet, B.; Giorgi, R.; Bonerandi, J.J.; Mundler, O. High negative predictive value of slow lymphatic drainage on metastatic node spread detection in malignant limb and trunk cutaneous melanoma. Bull Cancer 2004, 91, 10225–10228. [Google Scholar]
- Fujiwara, M.; Sawada, M.; Kasuya, A.; Matsushita, Y.; Yamada, M.; Fukamizu, H.; Magata, Y.; Tokura, Y.; Sakahara, H. Measurement of cutaneous lymphatic flow rates in patients with skin cancer: Area extraction method. J. Dermatol. 2014, 41, 498–504. [Google Scholar] [CrossRef] [Green Version]
- Smith, G.; Thrams, A.; Voslar, A. Impact of metastatic disease on transit time in sentinel node lymphoscintigraphy. J. Nucl. Med. 2021, 62 (Suppl. 1), 159. [Google Scholar]
- Collarino, A.; Fuoco, V.; Garganese, G.; Bouda, L.M.P.A.-; Perotti, G.; Manca, G.; Vidal-Sicart, S.; Giammarile, F.; De Geus-Oei, L.-F.; Scambia, G.; et al. Lymphoscintigraphy and sentinel lymph node biopsy in vulvar carcinoma: Update from a European expert panel. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1261–1274. [Google Scholar] [CrossRef]
- Skanjeti, A.; Dhomps, A.; Paschetta, C.; Tordo, J.; Bolton, R.C.D.; Giammarile, F. Lymphoscintigraphy for Sentinel Node Mapping in Head and Neck Cancer. Semin. Nucl. Med. 2021, 51, 39–49. [Google Scholar] [CrossRef]
- Giammarile, F.; Bozkurt, M.F.; Cibula, D.; Pahisa, J.; Oyen, W.J.; Paredes, P.; Olmos, R.V.; Sicart, S.V. The EANM clinical and technical guidelines for lymphoscintigraphy and sentinel node localization in gynaecological cancers. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 1463–1477. [Google Scholar] [CrossRef] [PubMed]
- Catarci, M.; Zaraca, F.; Angeloni, R.; Mancini, B.; de Filippo, M.G.; Massa, R.; Carboni, M.; Pasquini, G. Preoperative lymphoscintigraphy and sentinel lymph node biopsy in papillary thyroid cancer. A pilot study. J. Surg. Oncol. 2001, 77, 21–24. [Google Scholar] [CrossRef] [PubMed]
- Wawroschek, F.; Vogt, H.; Wengenmair, H.; Weckermann, D.; Hamm, M.; Keil, M.; Graf, G.; Heidenreich, P.; Harzmann, R. Prostate Lymphoscintigraphy and Radio-Guided Surgery for Sentinel Lymph Node Identification in Prostate Cancer. Urol. Int. 2003, 70, 303–310. [Google Scholar] [CrossRef] [Green Version]
- Bats, A.-S.; Frati, A.; Mathevet, P.; Orliaguet, I.; Querleu, D.; Zerdoud, S.; Leblanc, E.; Gauthier, H.; Uzan, C.; Deandreis, D.; et al. Contribution of lymphoscintigraphy to intraoperative sentinel lymph node detection in early cervical cancer: Analysis of the prospective multicenter SENTICOL cohort. Gynecol. Oncol. 2015, 137, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Quartuccio, N.; Garau, M.L.; Arnone, A.; Pappalardo, M.; Rubello, D.; Arnone, G.; Manca, G. Comparison of 99m TC-Labeled Colloid SPECT/CT and Planar Lymphoscintigraphy in Sentinel Lymph Node Detection in Patients with Melanoma: A Meta-Analysis. J. Clin. Med. 2020, 9, 1680. [Google Scholar] [CrossRef] [PubMed]
- Kwak, J.J.; Kesner, A.L.; Gleisner, A.; Jensen, A.; Friedman, C.; McCarter, M.D.; Koo, P.J.; Morgan, R.; Kounalakis, N. Utility of Quantitative SPECT/CT Lymphoscintigraphy in Guiding Sentinel Lymph Node Biopsy in Head and Neck Melanoma. Ann. Surg. Oncol. 2019, 27, 1432–1438. [Google Scholar] [CrossRef] [PubMed]
- Chahid, Y.; Qiu, X.; van de Garde, E.M.W.; Verberne, H.J.; Booij, J. Risk factors for nonvisualization of the sentinel lymph node on lymphoscintigraphy in breast cancer patients. EJNMMI Res. 2021, 11, 54. [Google Scholar] [CrossRef] [PubMed]



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| US Criteria | Benign Lymph Node | Malignant Lymph Node |
|---|---|---|
| Size | <1 cm in short axis | ≥1 cm in short axis |
| Shape | Oval or elliptical | Round |
| Border | Indistinct | Sharp |
| Echogenicity | Hypoechoic | Very hypoechoic |
| Hilum | Maintained fatty hilum | Absent fatty hilum |
| Vascularity | Avascular or hilar vascularity | Peripheral or mixed |
| Resistive index | Low | High |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elshikh, M.; Moawad, A.W.; Salem, U.; Klimkowski, S.P.; Hassan, T.; Rao Korivi, B.; Jensen, C.T.; Javadi, S.; Elsayes, K.M. Oncologic Imaging of the Lymphatic System: Current Perspective with Multi-Modality Imaging and New Horizon. Cancers 2021, 13, 4554. https://doi.org/10.3390/cancers13184554
Elshikh M, Moawad AW, Salem U, Klimkowski SP, Hassan T, Rao Korivi B, Jensen CT, Javadi S, Elsayes KM. Oncologic Imaging of the Lymphatic System: Current Perspective with Multi-Modality Imaging and New Horizon. Cancers. 2021; 13(18):4554. https://doi.org/10.3390/cancers13184554
Chicago/Turabian StyleElshikh, Mohamed, Ahmed W Moawad, Usama Salem, Sergio P Klimkowski, Talaat Hassan, Brinda Rao Korivi, Corey T Jensen, Sanaz Javadi, and Khaled M Elsayes. 2021. "Oncologic Imaging of the Lymphatic System: Current Perspective with Multi-Modality Imaging and New Horizon" Cancers 13, no. 18: 4554. https://doi.org/10.3390/cancers13184554
APA StyleElshikh, M., Moawad, A. W., Salem, U., Klimkowski, S. P., Hassan, T., Rao Korivi, B., Jensen, C. T., Javadi, S., & Elsayes, K. M. (2021). Oncologic Imaging of the Lymphatic System: Current Perspective with Multi-Modality Imaging and New Horizon. Cancers, 13(18), 4554. https://doi.org/10.3390/cancers13184554