The Prognostic Value of Lymph Node Involvement after Neoadjuvant Chemotherapy Is Different among Breast Cancer Subtypes

 ,
,  ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Baseline Patients’ and Tumors’ Characteristics
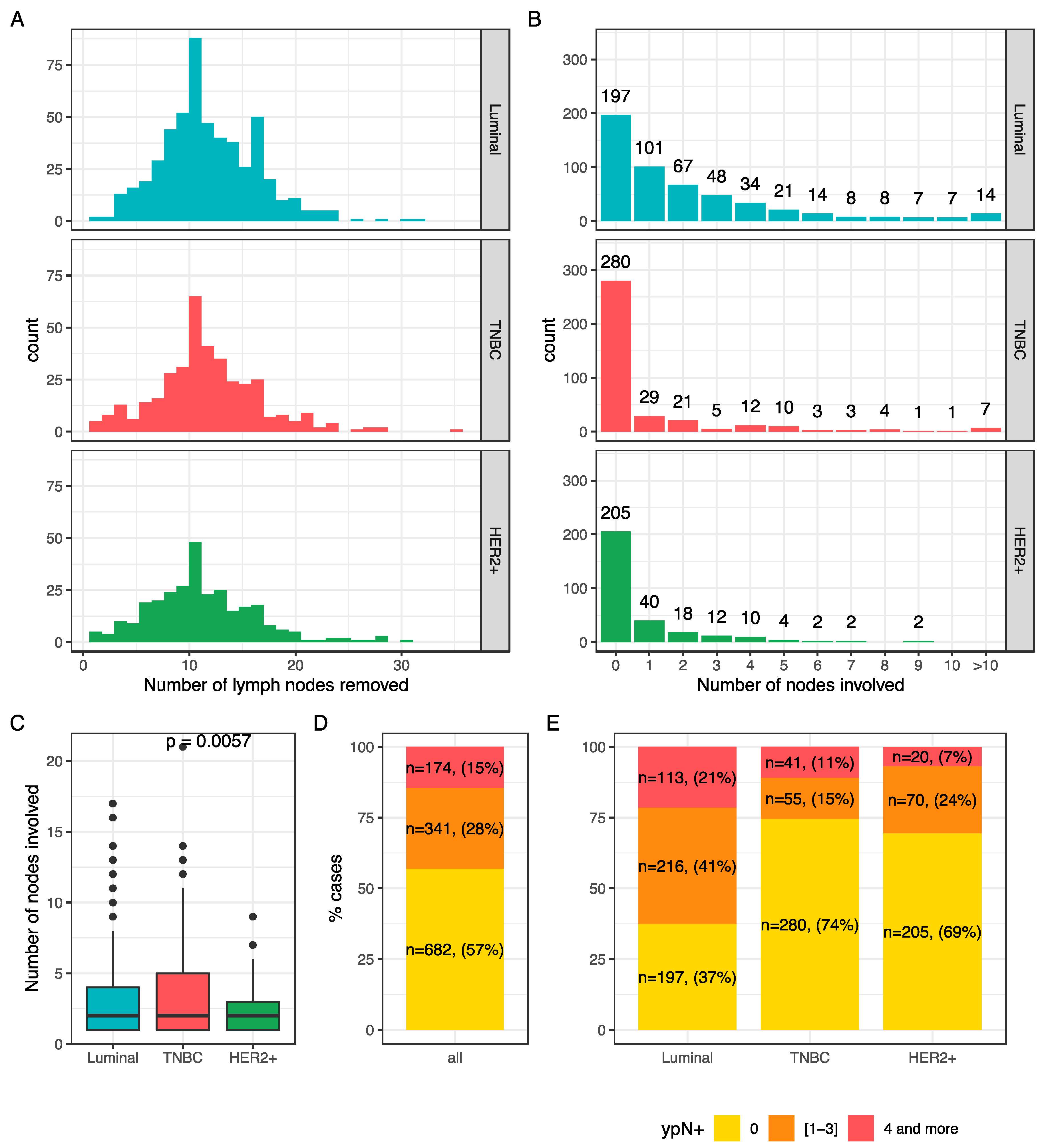
2.2. Association Between Post-NAC Involvement and Tumor Characteristics
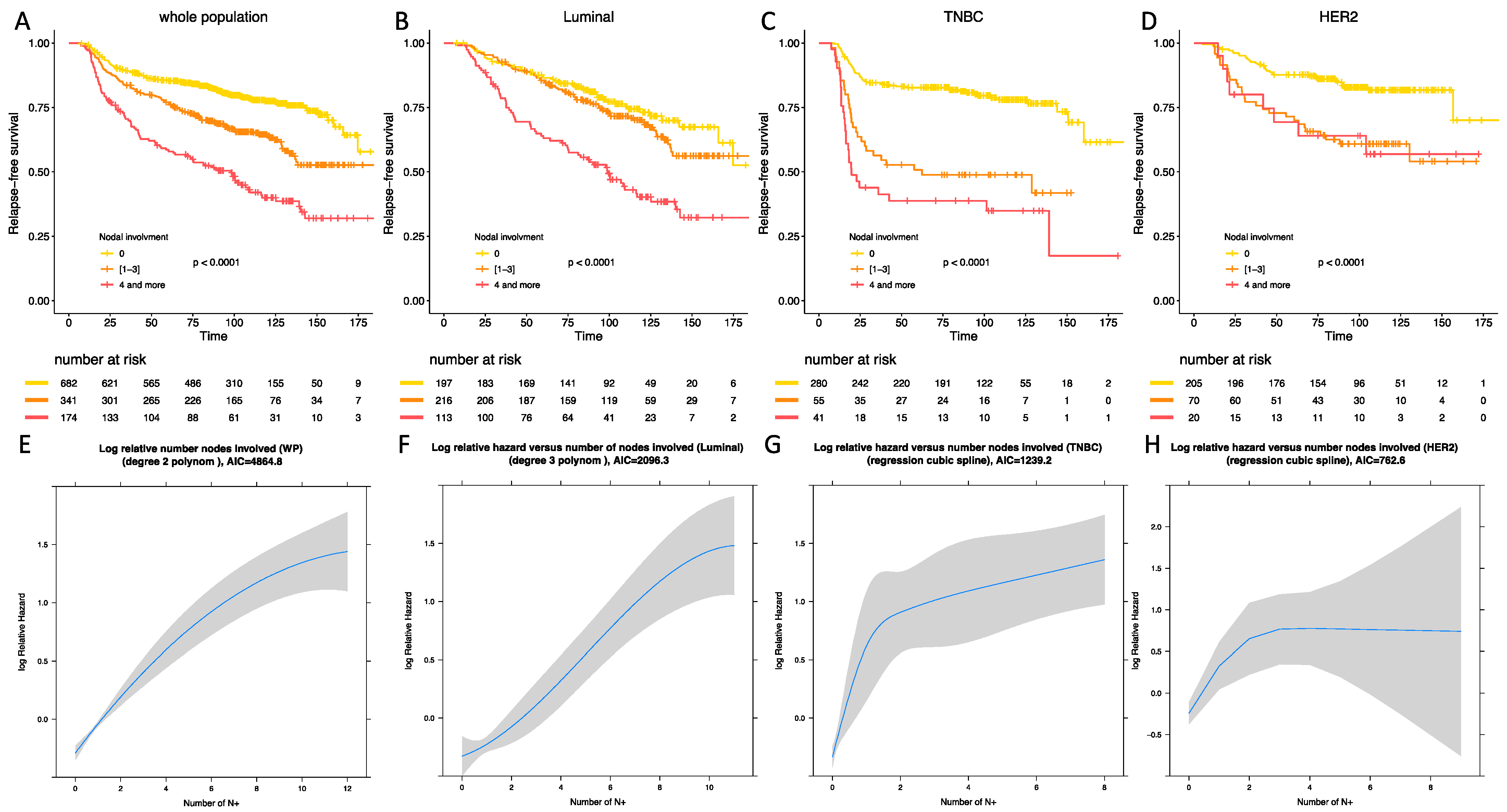
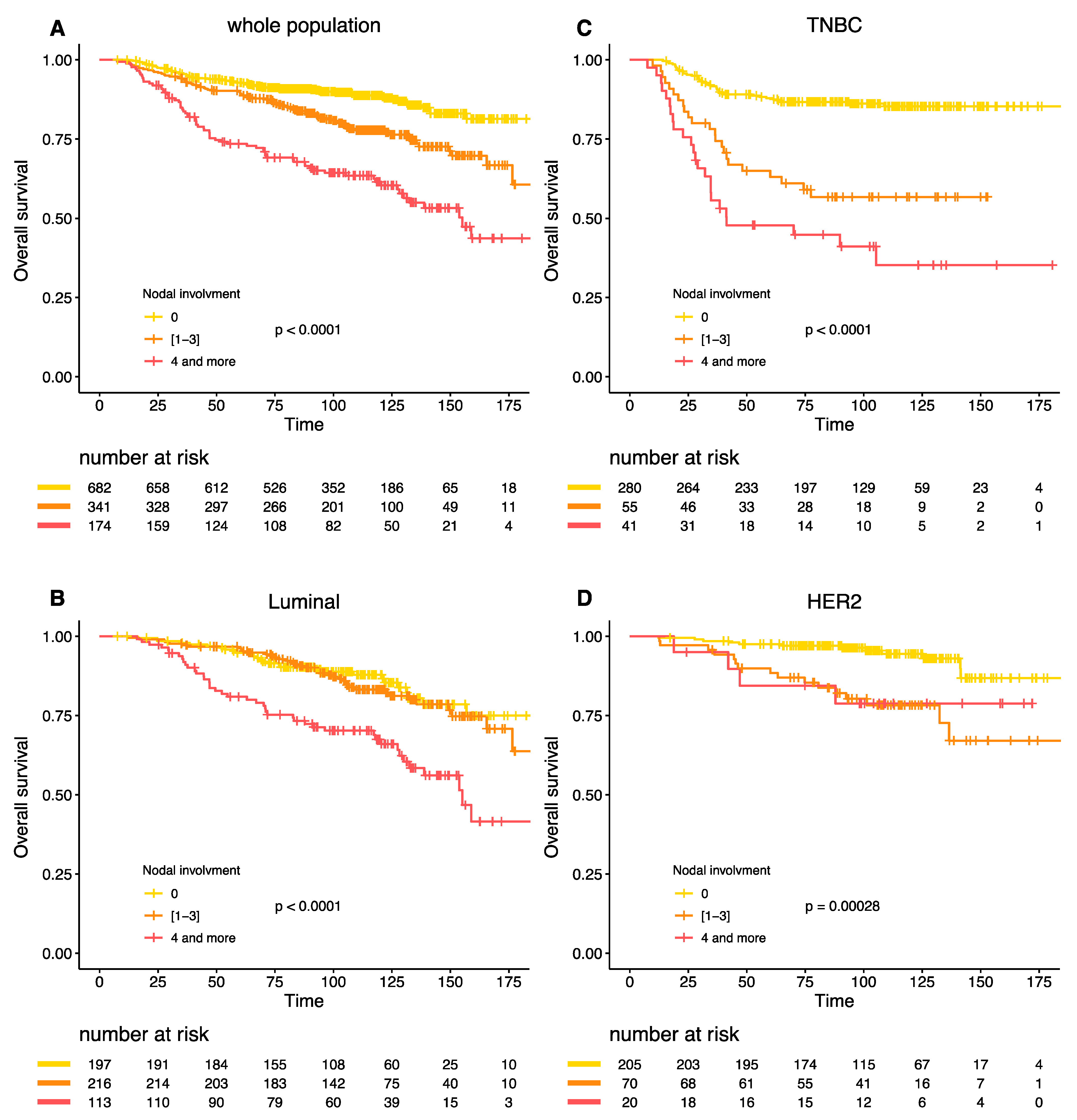
2.3. Survival Analyses
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Tumor Samples and Pathological Review
4.2.1. BC Subtypes
4.2.2. Post-NAC Nodal Involvement (ypN)
4.2.3. Residual Cancer Burden Index (RCB)
4.2.4. TILs and LVI
4.3. Study Endpoints
4.4. Statistical Analysis
4.5. Linearity and Interaction Tests
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Masuda, N.; Lee, S.J. Adjuvant Capecitabine for Breast Cancer after Preoperative Chemotherapy. N. Engl. J. Med. 2017, 376, 2147–2159. [Google Scholar] [CrossRef]
- Von Minckwitz, G.; Huang, C.S. Trastuzumab Emtansine for Residual Invasive HER2-Positive Breast Cancer. N. Engl. J. Med. 2019, 380, 617–628. [Google Scholar] [CrossRef] [PubMed]
- Fitzgibbons, P.L.; Page, D.L. Prognostic factors in breast cancer. College of American Pathologists Consensus Statement 1999. Arch. Pathol. Lab. Med. 2000, 124, 966–978. [Google Scholar] [PubMed]
- Shek, L.L.; Godolphin, W. Model for breast cancer survival: Relative prognostic roles of axillary nodal status, TNM stage, estrogen receptor concentration, and tumor necrosis. Cancer Res. 1988, 48, 5565–5569. [Google Scholar] [PubMed]
- Saez, R.A.; McGuire, W.L.; Clark, G.M. Prognostic factors in breast cancer. Semin. Surg. Oncol. 1989, 5, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Carter, C.L.; Allen, C.; Henson, D.E. Relation of tumor size, lymph node status, and survival in 24,740 breast cancer cases. Cancer 1989, 63, 181–187. [Google Scholar] [CrossRef]
- McCready, D.R.; Hortobagyi, G.N. The prognostic significance of lymph node metastases after preoperative chemotherapy for locally advanced breast cancer. Arch. Surg. 1989, 124, 21–25. [Google Scholar] [CrossRef]
- Kuerer, H.M.; Sahin, A.A. Incidence and Impact of Documented Eradication of Breast Cancer Axillary Lymph Node Metastases Before Surgery in Patients Treated with Neoadjuvant Chemotherapy. Ann. Surg. 1999, 230, 72. [Google Scholar] [CrossRef]
- Pierga, J.Y.; Mouret, E. Prognostic value of persistent node involvement after neoadjuvant chemotherapy in patients with operable breast cancer. Br. J. Cancer 2000, 83, 1480–1487. [Google Scholar] [CrossRef]
- Mougalian, S.S.; Hernandez, M. Ten-Year Outcomes of Patients with Breast Cancer with Cytologically Confirmed Axillary Lymph Node Metastases and Pathologic Complete Response After Primary Systemic Chemotherapy. JAMA Oncol. 2016, 2, 508–516. [Google Scholar] [CrossRef]
- Symmans, W.F.; Wei, C. Long-Term Prognostic Risk After Neoadjuvant Chemotherapy Associated with Residual Cancer Burden and Breast Cancer Subtype. J. Clin. Oncol. 2017, 35, 1049–1060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rouzier, R.; Extra, J.M. Incidence and prognostic significance of complete axillary downstaging after primary chemotherapy in breast cancer patients with T1 to T3 tumors and cytologically proven axillary metastatic lymph nodes. J. Clin. Oncol. 2002, 20, 1304–1310. [Google Scholar] [CrossRef] [PubMed]
- Hennessy, B.T.; Hortobagyi, G.N. Outcome after pathologic complete eradication of cytologically proven breast cancer axillary node metastases following primary chemotherapy. J. Clin. Oncol. 2005, 23, 9304–9311. [Google Scholar] [CrossRef] [PubMed]
- Federal Register: Pathological Complete Response in Neoadjuvant Treatment of High-Risk Early-Stage Breast Cancer: Use as an Endpoint to Support Accelerated Approval. Guidance for Industry. Available online: https://www.federalregister.gov/documents/2014/10/07/2014-23845/pathological-complete-response-in-neoadjuvant-treatment-of-high-risk-early-stage-breast-cancer-use (accessed on 1 November 2020).
- Houssami, N.; Macaskill, P.; von Minckwitz, G.; Marinovich, M.L.; Mamounas, E. Meta-analysis of the association of breast cancer subtype and pathologic complete response to neoadjuvant chemotherapy. Eur. J. Cancer 2012, 48, 3342–3354. [Google Scholar] [CrossRef] [PubMed]
- Von Minckwitz, G.; Untch, M. Definition and impact of pathologic complete response on prognosis after neoadjuvant chemotherapy in various intrinsic breast cancer subtypes. J. Clin. Oncol. 2012, 30, 1796–1804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cortazar, P.; Zhang, L.; Untch, M. Pathological complete response and long-term clinical benefit in breast cancer: The CTNeoBC pooled analysis. Lancet 2014, 384, 164–172. [Google Scholar] [CrossRef] [Green Version]
- Dominici, L.S.; Negron, G. Cytologically proven axillary lymph node metastases are eradicated in patients receiving preoperative chemotherapy with concurrent trastuzumab for HER2-positive breast cancer. Cancer 2010, 116, 2884–2889. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.C.; Zhang, Y.F. Axillary lymph node status, adjusted for pathologic complete response in breast and axilla after neoadjuvant chemotherapy, predicts differential disease-free survival in breast cancer. Curr. Oncol. 2013, 20, e180–e192. [Google Scholar] [CrossRef] [Green Version]
- Boughey, J.C.; McCall, L.M. Tumor biology correlates with rates of breast-conserving surgery and pathologic complete response after neoadjuvant chemotherapy for breast cancer: Findings from the ACOSOG Z1071 (Alliance) prospective multicenter clinical trial. Ann. Surg. 2014, 260, 608–616. [Google Scholar] [CrossRef] [Green Version]
- Mamtani, A.; Barrio, A.V. How Often Does Neoadjuvant Chemotherapy Avoid Axillary Dissection in Patients with Histologically Confirmed Nodal Metastases: Results of a Prospective Study. Ann. Surg. Oncol. 2016, 23, 3467–3474. [Google Scholar] [CrossRef] [Green Version]
- Fayanju, O.M.; Ren, Y. The Clinical Significance of Breast-only and Node-only Pathologic Complete Response (pCR) after Neoadjuvant Chemotherapy (NACT): A Review of 20,000 Breast Cancer Patients in the National Cancer Data Base (NCDB). Ann. Surg. 2018, 268, 591–601. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Park, H.S. Prognostic Nomogram for Prediction of Axillary Pathologic Complete Response After Neoadjuvant Chemotherapy in Cytologically Proven Node-Positive Breast Cancer. Medicine 2015, 94, e1720. [Google Scholar] [CrossRef] [PubMed]
- AL-Tweigeri, T.; AlSayed, A. A multicenter prospective phase II trial of neoadjuvant epirubicin, cyclophosphamide, and 5-fluorouracil (FEC100) followed by cisplatin–docetaxel with or without trastuzumab in locally advanced breast cancer. Cancer Chemother. Pharmacol. 2016, 77, 147–153. [Google Scholar] [CrossRef]
- Boland, M.R.; McVeigh, T.P. Impact of receptor phenotype on nodal burden in patients with breast cancer who have undergone neoadjuvant chemotherapy. BJS Open 2017, 1, 39–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sueta, A.; Yamamoto, Y. Clinical significance of pretherapeutic Ki67 as a predictive parameter for response to neoadjuvant chemotherapy in breast cancer: Is it equally useful across tumor subtypes? Surgery 2014, 155, 927–935. [Google Scholar] [CrossRef] [PubMed]
- Ohno, S.; Chow, L.W.C. Randomized trial of preoperative docetaxel with or without capecitabine after 4 cycles of 5-fluorouracil– epirubicin–cyclophosphamide (FEC) in early-stage breast cancer: Exploratory analyses identify Ki67 as a predictive biomarker for response to neoadjuvant chemotherapy. Breast Cancer Res. Treat. 2013, 142, 69–80. [Google Scholar] [PubMed] [Green Version]
- Andre, F.; Arnedos, M.; Goubar, A.; Ghouadni, A.; Delaloge, S. Ki67-no evidence for its use in node-positive breast cancer. Nat. Rev. Clin. Oncol. 2015, 12, 296–301. [Google Scholar] [CrossRef]
- Sotiriou, C.; Pusztai, L. Gene-expression signatures in breast cancer. N. Engl. J. Med. 2009, 360, 790–800. [Google Scholar] [CrossRef] [Green Version]
- Albain, K.S.; Barlow, W.E. Prognostic and predictive value of the 21-gene recurrence score assay in postmenopausal women with node-positive, oestrogen-receptor-positive breast cancer on chemotherapy: A retrospective analysis of a randomised trial. Lancet Oncol. 2010, 11, 55–65. [Google Scholar] [CrossRef] [Green Version]
- Dowsett, M.; Cuzick, J. Prediction of risk of distant recurrence using the 21-gene recurrence score in node-negative and node-positive postmenopausal patients with breast cancer treated with anastrozole or tamoxifen: A TransATAC study. J. Clin. Oncol. 2010, 28, 1829–1834. [Google Scholar] [CrossRef] [Green Version]
- ClinicalTrials.Gov: National Cancer Institute (NCI). A Phase III, Randomized Clinical Trial of Standard Adjuvant Endocrine Therapy +/− Chemotherapy in Patients with 1-3 Positive Nodes, Hormone Receptor-Positive and HER2-Negative Breast Cancer with Recurrence Score (RS) of 25 or Less. RxPONDER: A Clinical Trial Rx for Positive Node, Endocrine Responsive Breast Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT01272037 (accessed on 4 November 2020).
- Bonsang-Kitzis, H.; Chaltier, E. Beyond Axillary Lymph Node Metastasis, BMI and Menopausal Status Are Prognostic Determinants for Triple-Negative Breast Cancer Treated by Neoadjuvant Chemotherapy. PLoS ONE 2015, 10, e0144359. [Google Scholar] [CrossRef] [PubMed]
- Hamy, A.-S.; Lam, G.T.; Laas, E. Lymphovascular invasion after neoadjuvant chemotherapy is strongly associated with poor prognosis in breast carcinoma. Breast Cancer Res. Treat. 2018, 169, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Symmans, W.F.; Peintinger, F. Measurement of residual breast cancer burden to predict survival after neoadjuvant chemotherapy. J. Clin. Oncol. 2007, 25, 4414–4422. [Google Scholar] [CrossRef] [PubMed]
- ClinicalTrials.Gov: AstraZeneca. A Randomised, Double-blind, Parallel Group, Placebo-controlled Multi-centre Phase III Study to Assess the Efficacy and Safety of Olaparib Versus Placebo as Adjuvant Treatment in Patients with gBRCA1/2 Mutations and High Risk HER2 Negative Primary Breast Cancer Who Have Completed Definitive Local Treatment and Neoadjuvant or Adjuvant Chemotherapy. Available online: https://clinicaltrials.gov/ct2/show/NCT02032823 (accessed on 16 November 2020).
- ClinicalTrials.Gov: M.D. Anderson Cancer Center. Triple-Negative First-Line Study: Neoadjuvant Trial of Nab-Paclitaxel and MPDL3280A, a PDL-1 Inhibitor in Patients with Triple Negative Breast Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT02530489 (accessed on 16 November 2020).
- ClinicalTrials.Gov: German Breast Group. Phase III Study Evaluating Palbociclib (PD-0332991), a Cyclin-Dependent Kinase (CDK) 4/6 Inhibitor in Patients with Hormone-receptor-positive, HER2-normal Primary Breast Cancer with High Relapse Risk After Neoadjuvant Chemotherapy ‘PENELOPEB’. Available online: https://clinicaltrials.gov/ct2/show/NCT01864746 (accessed on 16 November 2020).
- ClinicalTrials.Gov: Cancer Insight, LLC. Phase II Trial of Combination Immunotherapy with Nelipepimut-S + GM-CSF (NeuVaxTM) and Trastuzumab in High-risk HER2+ Breast Cancer Patients. Available online: https://clinicaltrials.gov/ct2/show/NCT02297698 (accessed on 16 November 2020).
- Grandal, B.; Evrevin, C. Impact of BRCA Mutation Status on Tumor Infiltrating Lymphocytes (TILs), Response to Treatment, and Prognosis in Breast Cancer Patients Treated with Neoadjuvant Chemotherapy. Cancers 2020, 12, 3681. [Google Scholar] [CrossRef]
- Hamy, A.S.; Bonsang-Kitzis, H. Interaction between Molecular Subtypes and Stromal Immune Infiltration before and after Treatment in Breast Cancer Patients Treated with Neoadjuvant Chemotherapy. Clin. Cancer Res. 2019, 25, 6731–6741. [Google Scholar] [CrossRef] [Green Version]
- Hamy, A.S.; Pierga, J.Y. Stromal lymphocyte infiltration after neoadjuvant chemotherapy is associated with aggressive residual disease and lower disease-free survival in HER2-positive breast cancer. Ann. Oncol. 2017, 28, 2233–2240. [Google Scholar] [CrossRef]
- Hamy, A.S.; Darrigues, L. Prognostic value of the Residual Cancer Burden index according to breast cancer subtype: Validation on a cohort of BC patients treated by neoadjuvant chemotherapy. PLoS ONE 2020, 15, e0234191. [Google Scholar] [CrossRef]
- Harvey, J.M.; Clark, G.M.; Osborne, C.K.; Allred, D.C. Estrogen receptor status by immunohistochemistry is superior to the ligand-binding assay for predicting response to adjuvant endocrine therapy in breast cancer. J. Clin. Oncol. 1999, 17, 1474–1481. [Google Scholar] [CrossRef]
- Wolff, A.C.; Hammond, M.E. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2 testing in breast cancer. Arch. Pathol. Lab. Med. 2007, 131, 18–43. [Google Scholar] [CrossRef] [Green Version]
- Salgado, R.; Denkert, C. The evaluation of tumor-infiltrating lymphocytes (TILs) in breast cancer: Recommendations by an International TILs Working Group 2014. Ann. Oncol. 2015, 26, 259–271. [Google Scholar] [CrossRef]
- Dieci, M.V.; Radosevic-Robin, N. Update on tumor-infiltrating lymphocytes (TILs) in breast cancer, including recommendations to assess TILs in residual disease after neoadjuvant therapy and in carcinoma in situ: A report of the International Immuno-Oncology Biomarker Working Group on Breast Cancer. Semin. Cancer Biol. 2018, 52, 16–25. [Google Scholar] [PubMed]
- Harrell, F. Regression Modeling Strategies: With Applications to Linear Models, Logistic Regression, and Survival Analysis; Springer: New York, NY, USA, 2001. [Google Scholar]
- Selvin, S. Statistical Analysis of Epidemiologic Data. Statistical Analysis of Epidemiologic Data; Oxford University Press: Oxford, UK, 2004. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Class | All | Node Negative | Node Positive | p |
|---|---|---|---|---|---|
| n | 1197 (100%) | 682 (57%) | 515 (43%) | ||
| Age median | 48.5 (10.1) | 48.0 (10.4) | 49.3 (9.6) | 0.027 | |
| Age class | [0–50) | 678 (56.6) | 399 (58.5) | 279 (54.2) | 0.279 |
| [50–60) | 352 (29.4) | 189 (27.7) | 163 (31.7) | ||
| 60+ | 167 (14.0) | 94 (13.8) | 73 (14.2) | ||
| Menopausal status | Premenopausal | 746 (62.8) | 432 (63.9) | 314 (61.3) | 0.396 |
| Postmenopausal | 442 (37.2) | 244 (36.1) | 198 (38.7) | ||
| BMI | 18.5–24.9 | 680 (57.1) | 401 (59.1) | 279 (54.5) | 0.302 |
| <18.5 | 48 (4.0) | 26 (3.8) | 22 (4.3) | ||
| 25–29.9 | 304 (25.5) | 160 (23.6) | 144 (28.1) | ||
| >=30 | 159 (13.4) | 92 (13.5) | 67 (13.1) | ||
| Smoking status | No | 719 (75.6) | 428 (76.4) | 291 (74.4) | 0.528 |
| Yes | 232 (24.4) | 132 (23.6) | 100 (25.6) | ||
| BRCA mutation genes | BRCA1 | 31 (11.7) | 24 (13.7) | 7 (7.8) | 0.404 |
| BRCA2 | 14 (5.3) | 10 (5.7) | 4 (4.4) | ||
| others | 1 (0.4) | 1 (0.6) | 0 (0.0) | ||
| No | 219 (82.6) | 140 (80.0) | 79 (87.8) | ||
| Clinical T stage (TNM) | T0-T1 | 70 (5.9) | 41 (6.0) | 29 (5.6) | 0.001 |
| T2 | 797 (66.6) | 483 (70.8) | 314 (61.1) | ||
| T3-T4 | 329 (27.5) | 158 (23.2) | 171 (33.3) | ||
| Clinical N stage (TNM) | N0 | 525 (43.9) | 372 (54.5) | 153 (29.8) | <0.001 |
| N1-N2-N3 | 671 (56.1) | 310 (45.5) | 361 (70.2) | ||
| BC subtype | Luminal | 526 (43.9) | 197 (28.9) | 329 (63.9) | <0.001 |
| TNBC | 376 (31.4) | 280 (41.1) | 96 (18.6) | ||
| HER2+ | 295 (24.6) | 205 (30.1) | 90 (17.5) | ||
| ER status | Negative | 544 (45.4) | 399 (58.5) | 145 (28.2) | <0.001 |
| Positive | 653 (54.6) | 283 (41.5) | 370 (71.8) | ||
| PR status | Negative | 680 (57.9) | 450 (66.8) | 230 (46.0) | <0.001 |
| Positive | 494 (42.1) | 224 (33.2) | 270 (54.0) | ||
| Her2 status | Negative | 902 (75.4) | 477 (69.9) | 425 (82.5) | <0.001 |
| Positive | 295 (24.6) | 205 (30.1) | 90 (17.5) | ||
| Histological type | NST | 1060 (93.5) | 617 (96.0) | 443 (90.2) | <0.001 |
| Others | 74 (6.5) | 26 (4.0) | 48 (9.8) | ||
| KI67 | [0–10) | 65 (11.2) | 25 (7.9) | 40 (15.0) | 0.001 |
| [10–20) | 110 (18.9) | 49 (15.6) | 61 (22.9) | ||
| ≥20 | 406 (69.9) | 241 (76.5) | 165 (62.0) | ||
| Mitotic index | ≤22 | 20.8 (19.2) | 24.1 (20.2) | 16.3 (16.9) | <0.001 |
| >22 | 61.3 (18.2) | 61.0 (19.2) | 61.8 (16.4) | ||
| SBR grade | Grade I-II | 477 (41.3) | 200 (30.4) | 277 (55.7) | <0.001 |
| Grade III | 678 (58.7) | 458 (69.6) | 220 (44.3) | ||
| LVI | No | 267 (61.0) | 158 (69.9) | 109 (51.4) | <0.001 |
| Yes | 171 (39.0) | 68 (30.1) | 103 (48.6) | ||
| DCIS component | No | 601 (60.7) | 385 (66.3) | 216 (52.8) | <0.001 |
| Yes | 389 (39.3) | 196 (33.7) | 193 (47.2) | ||
| Stromal TIL levels (%) | 24.0 (19.9) | 26.9 (21.7) | 19.3 (15.6) | <0.001 | |
| Intra Tumoral TIL levels (%) | 11.2 (12.3) | 12.4 (13.1) | 9.3 (10.6) | 0.001 | |
| CT regimen (NAC) | anthra-taxanes | 841 (70.6) | 507 (74.7) | 334 (65.1) | <0.001 |
| anthra | 235 (19.7) | 105 (15.5) | 130 (25.3) | ||
| taxanes | 25 (2.1) | 13 (1.9) | 12 (2.3) | ||
| others | 91 (7.6) | 54 (8.0) | 37 (7.2) | ||
| Adjuvant chemotherapy | No | 1000 (83.5) | 661 (96.9) | 339 (65.8) | <0.001 |
| Yes | 197 (16.5) | 21 (3.1) | 176 (34.2) | ||
| 5FU and Vinorelbine | 144 (73.1) | 8 (38.1) | 136 (77.3) | <0.001 | |
| Others | 53 (26.9) | 13 (61.9) | 40 (22.7) | ||
| Adjuvant Anti HER2 therapy | No | 166 (39.2) | 18 (9) | 148 (66.1) | <0.001 |
| Yes | 258 (60.8) | 182 (91) | 76 (33.9) | ||
| Radiotherapy | No | 22 (1.8) | 15 (2.2) | 7 (1.4) | 0.393 |
| Yes | 1175 (98.2) | 667 (97.8) | 508 (98.6) | ||
| Infraclavicular Radiotherapy | No | 203 (17.3) | 161 (24.3) | 42 (8.3) | <0.001 |
| Yes | 969 (82.7) | 503 (75.7) | 466 (91.7) | ||
| Sus-clavicular Radiotherapy | No | 121 (10.3) | 113 (17) | 8 (1.6) | <0.001 |
| Yes | 1051 (89.7) | 551 (83) | 500 (98.4) | ||
| Axillar Radiotherapy | No | 947 (80.8) | 623 (93.8) | 324 (63.8) | <0.001 |
| Yes | 225 (19.2) | 41 (6.2) | 184 (36.2) | ||
| Endocrine therapy | No | 544 (45.4) | 404 (59.2) | 140 (27.2) | <0.001 |
| Yes | 653 (54.6) | 278 (40.8) | 375 (72.8) | ||
| Type of endocrine therapy | Tamoxifen | 397 (33.3) | 178 (26.3) | 219 (42.5) | <0.001 |
| Aromatase inhibitor | 217 (18.2) | 82 (12.1) | 135 (26.2) | ||
| Tamoxifen + Agonist | 12 (1) | 5 (0.7) | 7 (1.4) | ||
| Aromatase inh + Ag | 6 (0.5) | 3 (0.4) | 3 (0.6) | ||
| Others | 20 (1.7) | 9 (1.3) | 11 (2.1) | ||
| Characteristics | Class | Post-NAC Node Involvement (ypN) | p | ||
|---|---|---|---|---|---|
| 0 | 1–3 | 4 and More | |||
| n | 682 | 341 | 174 | ||
| Pathological complete response | No pCR | 396 (58.3) | 340 (100.0) | 173 (100.0) | <0.001 |
| pCR | 283 (41.7) | 0 (0.0) | 0 (0.0) | ||
| Post-NAC LVI | No | 318 (78.3) | 156 (55.5) | 56 (38.6) | <0.001 |
| Yes | 88 (21.7) | 125 (44.5) | 89 (61.4) | ||
| RCB index (continuous) | 1.0 (0.9) | 3.0 (0.8) | 3.6 (0.7) | <0.001 | |
| RCB class | RCB-0 | 200 (45.1) | 0 (0.0) | 0 (0.0) | <0.001 |
| RCB-I | 53 (12.0) | 12 (6.4) | 0 (0.0) | ||
| RCB-II | 188 (42.4) | 101 (53.7) | 20 (24.1) | ||
| RCB-III | 2 (0.5) | 75 (39.9) | 63 (75.9) | ||
| Stromal TIL levels (%) (post-NAC) | 12.8 (13.1) | 13.6 (12.3) | 12.6 (12.1) | 0.750 | |
| IT TIL levels (%) (post-NAC) | 7.2 (8.2) | 6.9 (8.0) | 5.7 (5.4) | 0.289 | |
| Mitotic index (post-NAC) | 18.9 (30.9) | 12.6 (23.0) | 16.9 (34.8) | 0.103 | |
| Tumor cellularity (post-NAC) | 19.6 (26.7) | 35.9 (25.5) | 36.5 (24.5) | <0.001 | |
| Univariate | Multivariate | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Category | n | Events | HR | 95% CI | p * | p | HR | 95% CI | p |
| Pre-NAC parameters | ||||||||||
| Age | [0–50) | 678 | 210 | 1 | 0.716 | |||||
| [50–60) | 352 | 106 | 0.97 | [0.77–1.22] | ||||||
| 60+ | 167 | 55 | 1.11 | [0.82–1.49] | ||||||
| Menopausal status | Pre | 746 | 232 | 1 | 0.87 | |||||
| Post | 442 | 135 | 0.98 | [0.79–1.21] | ||||||
| BMI | 18.5–24.9 | 680 | 193 | 1 | 0.009 | 1 | ||||
| <18.5 | 48 | 15 | 1.13 | [0.67–1.91] | 0.651 | 1.13 | [0.66–1.91] | 0.66 | ||
| 25–29.9 | 304 | 96 | 1.15 | [0.9–1.47] | 0.255 | 1.06 | [0.83–1.36] | 0.624 | ||
| >= 30 | 159 | 66 | 1.63 | [1.23–2.15] | <0.001 | 1.52 | [1.15–2.02] | 0.003 | ||
| Smoking status | No | 721 | 221 | 1 | 0.924 | |||||
| Yes | 233 | 70 | 0.99 | [0.75–1.29] | ||||||
| BRCA mutation genes | BRCA1 | 31 | 9 | 1 | 0.991 | |||||
| BRCA2 | 14 | 4 | 0.91 | [0.28–2.96] | ||||||
| others | 1 | 0 | ||||||||
| No | 220 | 59 | 0.89 | [0.44–1.79] | ||||||
| Clinical T stage (TNM) | T0-T1 | 70 | 18 | 1 | <0.001 | 1 | ||||
| T2 | 797 | 223 | 1.1 | [0.68–1.78] | 0.703 | 1.25 | [0.77–2.03] | 0.371 | ||
| T3-T4 | 329 | 129 | 1.79 | [1.09–2.93] | 0.021 | 1.69 | [1.02–2.78] | 0.04 | ||
| Clinical N stage (TNM) | N0 | 525 | 148 | 1 | 0.032 | |||||
| N1-N2-N3 | 671 | 223 | 1.26 | [1.02–1.55] | ||||||
| BC subtype | Luminal | 526 | 184 | 1 | 0.025 | 1 | ||||
| TNBC | 376 | 116 | 1.05 | [0.83–1.33] | 0.668 | 1.66 | [1.29–2.15] | <0.001 | ||
| HER2 + | 295 | 71 | 0.72 | [0.54–0.94] | 0.017 | 1.04 | [0.78–1.39] | 0.785 | ||
| ER status | Negative | 544 | 158 | 1 | 0.953 | |||||
| Positive | 653 | 213 | 0.99 | [0.81–1.22] | ||||||
| PR status | Negative | 680 | 208 | 1 | 0.288 | |||||
| Positive | 494 | 152 | 0.89 | [0.72–1.1] | ||||||
| Her2 status | Negative | 902 | 300 | 1 | 0.007 | |||||
| Positive | 295 | 71 | 0.7 | [0.54–0.91] | ||||||
| Histological type | NST | 1060 | 317 | 1 | 0.106 | |||||
| Others | 74 | 30 | 1.36 | [0.94–1.98] | ||||||
| KI67 | [0–10) | 65 | 21 | 1 | 0.494 | |||||
| [10–20) | 110 | 38 | 1.07 | [0.63–1.82] | ||||||
| ≥20 | 406 | 144 | 1.25 | [0.79–1.98] | ||||||
| SBR grade | Grade I-II | 477 | 170 | 1 | 0.11 | |||||
| Grade III | 678 | 188 | 0.84 | [0.69–1.04] | ||||||
| LVI | No | 267 | 98 | 1 | 0.63 | |||||
| Yes | 171 | 66 | 1.08 | [0.79–1.48] | ||||||
| DCIS component | No | 604 | 165 | 1 | 0.11 | |||||
| Yes | 389 | 135 | 1.2 | [0.96–1.51] | ||||||
| CT regimen (NAC) | anthra-taxanes | 845 | 234 | 1 | 0.017 | |||||
| anthra | 235 | 97 | 1.37 | [1.07–1.74] | 0.011 | |||||
| taxanes | 25 | 4 | 0.59 | [0.22–1.59] | 0.3 | |||||
| others | 91 | 36 | 1.42 | [1–2.02] | 0.052 | |||||
| Post-NAC parameters | ||||||||||
| pCR | No pCR | 911 | 332 | 1 | <0.001 | |||||
| pCR | 285 | 39 | 0.35 | [0.25–0.49] | <0.001 | |||||
| Post-NAC LVI | No | 531 | 143 | 1 | <0.001 | |||||
| Yes | 302 | 144 | 2 | [1.59–2.52] | <0.001 | |||||
| ypN | 0 | 682 | 144 | 1 | <0.001 | 1 | - | - | ||
| [1,2,3] | 341 | 127 | 1.8 | [1.42–2.28] | <0.001 | 2.06 | [1.59–2.66] | <0.001 | ||
| 4 and more | 174 | 100 | 3.35 | [2.59–4.32] | <0.001 | 3.6 | [2.73–4.75] | <0.001 | ||
| RCB class | RCB-0 | 202 | 23 | 1 | <0.001 | |||||
| RCB-I | 65 | 7 | 0.98 | [0.42–2.29] | 0.965 | |||||
| RCB-II | 309 | 102 | 3.24 | [2.06–5.09] | <0.001 | |||||
| RCB-III | 141 | 72 | 5.56 | [3.47–8.89] | <0.001 | |||||
| Study | Study Population | Study Design | Number of Patients | Median f-u (mo.) | Post-C Nodal Involvement WP (n, %) | Post-NAC Nodal Involvement According to BC Subtype (n, %) | 5 Years RFS WP (HR) | Interaction Test ypN/BC Subtype | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | HR+/HER2- (%) | TNBC (%) | HER2+ (%) | HR+/HER2- (%) | TNBC (%) | HER2+ (%) | |||||||
| McReady (1989) Archives of Surgery | T3-T4, N2-N3 BC | RA | 136 | - | - | - | 56 | None (n = 34, 25%) 1–3 (n = 43, 32%) 4–10 (n = 35, 26%) >10 (n = 24, 17%) | - | - | - | - | - |
| Kuerer (1998) The American Journal of Surgery | IIA, IIB, IIIA, IIIB, IV BC | CT | 165 | - | - | - | 35 | None (n = 49, 30%) 1–3 (n = 51, 31%) 4–10 (n = 43, 27%) >10 (n = 20, 12%) | - | - | - | - | - |
| Kuerer (1999) Annals of Surgery | N+ IIA, IIB, IIIA, IIIB, IV BC | CT | 191 | - | - | - | 61 | None (n = 43, 23%) ≥1 (n = 148, 77%) | - | - | - | - | - |
| Pierga (2000) British Journal of Cancer | T2–T3, N0–N1 BC | RA | 487 | - | - | - | 84 | None (n = 223, 45.8%) 1–3 (n = 159, 32.6%) 4–7 (n = 72, 14.8%) ≥8 (n = 34, 7%) | - | - | - | 1 1.6 [1.2–2.3] 2.3 [1.5–3.4] 6.3 [4.1–9.7] | - |
| Rouzier (2002) JCO | T1-T3 N+ BC | RA | 152 | - | - | - | 75 | ypN0 (n = 35, 23%) ypN+ (n = 117, 77%) | - | - | - | 1 3.4 [2–5.9] | - |
| Hennessy (2005) JCO | stage II/III N+ BC | CT | 403 | - | - | - | 64 | ypN0 (n = 89, 22%) ypN+ (n = 314, 78%) | - | - | - | - | - |
| Dominici (2010) Cancer | T1-T4 N+ BC | RA | 109 | 0 | 0 | 109 | 29 | ypN0 (n = 81, 74%) ypN+ (n = 28, 26%) | - | - | 74% 26% | - | - |
| Zhang (2013) Curr. Oncol. | stage II/III | RA | 301 | 145 (48.2%) | 55 (18.3%) | 101 (33.6%) | 36.2 | ypN0 pCR (n = 75, 24.9%) ypN0 non pCR (n = 103, 34.2%) ypN1 (n = 72, 23.9%) ypN2 (n = 35, 11.6%) ypN3 (n = 16, 5.3%) | 11.7% 34.5% 31.7% 17.2% 4.8% | 25.4% 43.6% 18.2% 5.5% 7.3% | 43.5% 28.7% 15.8% 6.9% 5% | 0.07 0.53 1 5.51 3.8 | - |
| Boughey (2014) Ann Surg | T1-T4 N1-2 M0 BC | CT | 694 | 317 45.7%) | 170 (24.5%) | 207 29.8%) | - | ypN0 (n = 285, 41.1%) ypN1 (n = 241, 34.7%) ypN2 (n = 129, 18.6%) ypN3 (n = 39, 5.6%) | 21.1% 43% 27.4% 9.5% | 49.4% 32.4% 15.3% 2.9% | 64.7% 25.6% 7.7% 1.9% | - | - |
| Kim (2015) Medicine (Baltimore) | T1-T4 N1-3 M0 BC | RA | 415 | 245 (59%) | 93 (22.4%) | 77 (18.6%) | - | ypN0 (n = 159, 38.3%) ypN+ (n = 256, 61.7%) | 29% 71% | 53.8% 46.2% | 49.4% 50.6% | - | - |
| Bonsang-Kitzis (2015) PLoS One | T1-T3 N1-3 M0 BC | RA | 326 | - | 326 (100%) | - | 52 | ypN0 (n = 245, 75%) ypN+ (n = 81, 25%) | - | 75% 25% | - | 1 3.48 [2.08–5.84] | - |
| Mougalian (2016) JAMA Oncology | Stage II/III N+ BC | RA | 1600 | 719 (53.42%) | 289 (21.47%) | 338 (25.1%) | 79 | ypN0 (n = 454, 28.4%) ypN+ (n = 1146, 71.6%) | 16.4% 83.6% | 40.8% 59.2% | 47.3% 52.7% | 1 3.1 [2.3–4.15] * | - |
| Mamtani (2016) Ann Surg Oncol | Stage II/III N+ BC | CT | 195 | 73 (37.4%) | 55 (28.2%) | 67 (34.4%) | - | ypN0 (n = 96, 49%) | 21% | 47% | 82% | - | - |
| Al-Tweigeri (2016) Cancer Chemot Parmacol | T2–T4, N0–N2 M0 BC | CT | 80 | 38 (47.5%) | 13 (16.5%) | 29 (36%) | 43 | ypN0 (n = 51, 63.7%) | 50% | 73% | 79% | - | - |
| Diego (2016) Ann Surg Oncol | Stage II/III N+ BC | RA | 30 | 2 (7%) | 12 (36%) | 16 (57%) | - | ypN0 (n = 19, 63%) | 0% | 67% | 69% | - | - |
| Boland (2017) BJS Open | T1-T4 N+ BC | RA | 284 | 154 (54.2%) | 30 (10%) | 102 (35.9%) | 0 (n = 105, 37%) 1 (n = 41, 14.4%) 2–4 (n = 63, 22.2%) 5–10 (n = 43, 15.1%) >10 (n = 29, 10.2%) | 22.7% 14.9% 26.6% 20.8% 14.3% | 50% 6.6% 16.7% 10% 13.3% | 54% 15.7% 16.7% 7.8% 2.9% | - | - | |
| Our study (2020) | T1-T3 NxM0 BC | RA | 1197 | 526 (43.9%) | 376 (31.4%) | 295 (24.6%) | 110.5 | 0 (n = 682, 57%) 1–3 (n = 341, 28%) ≥4 (n = 174, 15%) | 37% 41% 21% | 74% 15% 11% | 69% 24% 7% | 1 1.79 [1.41–2.28] 3.3 [2.56–4.27] ** | Pinteraction = 0.004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laot, L.; Laas, E.; Girard, N.; Dumas, E.; Daoud, E.; Grandal, B.; Pierga, J.-Y.; Coussy, F.; Kirova, Y.; El-Alam, E.; et al. The Prognostic Value of Lymph Node Involvement after Neoadjuvant Chemotherapy Is Different among Breast Cancer Subtypes. Cancers 2021, 13, 171. https://doi.org/10.3390/cancers13020171
Laot L, Laas E, Girard N, Dumas E, Daoud E, Grandal B, Pierga J-Y, Coussy F, Kirova Y, El-Alam E, et al. The Prognostic Value of Lymph Node Involvement after Neoadjuvant Chemotherapy Is Different among Breast Cancer Subtypes. Cancers. 2021; 13(2):171. https://doi.org/10.3390/cancers13020171
Chicago/Turabian StyleLaot, Lucie, Enora Laas, Noemie Girard, Elise Dumas, Eric Daoud, Beatriz Grandal, Jean-Yves Pierga, Florence Coussy, Youlia Kirova, Elsy El-Alam, and et al. 2021. "The Prognostic Value of Lymph Node Involvement after Neoadjuvant Chemotherapy Is Different among Breast Cancer Subtypes" Cancers 13, no. 2: 171. https://doi.org/10.3390/cancers13020171
APA StyleLaot, L., Laas, E., Girard, N., Dumas, E., Daoud, E., Grandal, B., Pierga, J. -Y., Coussy, F., Kirova, Y., El-Alam, E., Bataillon, G., Lae, M., Llouquet, F., Reyal, F., & Hamy, A. -S. (2021). The Prognostic Value of Lymph Node Involvement after Neoadjuvant Chemotherapy Is Different among Breast Cancer Subtypes. Cancers, 13(2), 171. https://doi.org/10.3390/cancers13020171