
Cardiac Toxicity Associated with Immune Checkpoint Inhibitors: A Systematic Review

 ,
,  , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Cardiotoxicity
3.1. General
3.2. Myocarditis
3.3. Pericarditis
3.4. Takotsubo Cardiomyopathy
3.5. Conduction Diseases
3.6. Myocardial Infarction
4. Treatments
4.1. Ipilimumab
4.2. Pembrolizumab
4.3. Nivolumab
4.4. Atezolizumab
4.5. Durvalumab
5. Antidotes for ICI-Associated Cardiotoxicity
6. Discussion
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ICI | Immune checkpoint inhibitor |
| IRAE | Immune-related adverse event |
| MACE | Major adverse cardiac event |
| CMR | Cardiovascular magnetic resonance imaging |
| NSCLC | Non-small-cell lung cancer |
Appendix A

{kind=link}
{kind=link}
| Study | Sex | Age | Type of Cancer | Cancer Treatment | Type of Cardiotoxicity | Weeks until Presentation | Complaint at Presentation | Antidote |
|---|---|---|---|---|---|---|---|---|
| [38] | M | 76 | Lung cancer | Durvalumab | Myocarditis | 8 weeks | NR | Prednisone |
| [38] | F | 67 | Renal cell carcinoma | Ipilimumab + nivolumab | Myocarditis | 2 weeks | Dyspnea | Dexamethasone |
| [38] | M | 82 | Urothelial carcinoma | Pembrolizumab | Myocarditis | 15 weeks | Chest pain and dyspnea | Methylprednisone and prednisone |
| [19] | M | 70 | Lung cancer | Nivolumab | Acute pericarditis and pericardial effusion | 13 weeks | Pleuritic chest pain | Prednisone |
| [19] | F | 60 | Lung cancer | Nivolumab and THU-decitabine | Acute pericarditis and pericardial effusion | 9 weeks | Pleuritic chest pain, shortness of breath, productive cough | Colchicine and ibuprofen |
| [19] | M | 58 | Non-small cell lung cancer | Nivolumab | Pericardial effusion | 10 weeks | Shortness of breath | Prednisone |
| [19] | M | 60 | Melanoma | Ipilimumab + nivolumab, then nivolumab | Cardiomyopathy | 22 weeks | Chest tightness, decreased exercise tolerance | Prednisone |
| [19] | F | 84 | Lung cancer | Pembrolizumab | Cardiomyopathy | 7 weeks | Shortness of breath | Heart failure treatment |
| [19] | F | 71 | Lung cancer | Durvalumab | Cardiomyopathy and pericardial effusion | 22 weeks | Abdominal pain, shortness of breath on exertion | Prednisone |
| [19] | M | 67 | Melanoma | Ipilimumab | Cardiomyopathy | 17 weeks | Intermittent chest discomfort, shortness of breath on exertion | Carvedilol |
| [19] | F | 80 | Cutaneous squamous cell carcinoma | Pembrolizumab | Myocarditis | 7 weeks | Bilateral eye ptosis, generalized weakness and fatigue | Prednisone |
| [19] | M | 80 | Prostate cancer | Pembrolizumab | Myocarditis | 4 weeks | Right eye ptosis, generalized weakness and fatigue | Prednisone |
| [75] | M | 75 | Myelodysplastic syndrome | Ipilimumab + nivolumab + azacitidine | Pericardial effusion and pleural effusion | 7 weeks | Fever, cough, dyspnea, rash | IVIG, rosuvastatin |
| [75] | M | 78 | Myelodysplastic syndrome | Ipilimumab and azacitidine | Perimyocarditis | 1 week | Fever and pneumonia | IVIG, colchicine, atorvastatin |
| [75] | F | 74 | Melanoma | Ipilimumab and evofosfamide | Paroxysmal atrial fibrillation, sinus tachycardia, myocarditis | 4 weeks | Dyspnea, fever, hypotension, rash | IVIG, colchicine, rosuvastatin, hydroxychloroquine |
| [52] | M | 62 | Hepatocellular carcinoma | Nivolumab | Perimyocarditis, takotsubo syndrome, myocardial infarction | 3 weeks | Chest pain, nausea, and vomiting | Methylprednisolone, prednisone, broad spectrum antibiotics |
| [49] | M | 58 | Non-small cell lung cancer | Nivolumab | Pericarditis | 78 weeks | limb edema | Methylprednisolone, prednisolone, infliximab |
| [76] | F | 58 | Lung cancer | Nivolumab | Pericarditis | 12 weeks | dyspnea and cough | Pericardiocentesis and corticosteroids |
| [76] | M | 65 | Lung cancer | Nivolumab | Pericarditis | 106 weeks | Acute respiratory failure | Corticosteroids and pericardiocentesis |
| [74] | F | 78 | Melanoma | Pembrolizumab | Myocarditis | 6 weeks | Chest pain | Prednisone |
| [74] | F | 55 | Melanoma | Nivolumab, then ipilimumab + nivolumab | Myocarditis | 4 weeks after ipilimumab + nivolumab | Chest pain, fever, and dyspnea | |
| [77] | F | 52 | Non-small cell lung cancer | Ipilimumab + nivolumab | Myocarditis and acute heart failure | 52 weeks | Dyspnea on exertion, chest pain, and lower extremity edema | Methylprednisolone |
| [78] | M | 62 | Lung cancer | Pembrolizumab | Pericarditis | 15 weeks | Shortness of breath | Pericardial window and prednisone |
| [79] | M | 62 | Lung cancer | Nivolumab | Cardiac tamponade | 1 week | Dyspnea | Pericardiocentesis |
| [80] | F | 66 | Lung cancer | Pembrolizumab | Pericardial effusion | 1 week | NR | Pericardiocentesis and prednisone |
| [81] | M | 68 | Melanoma | Ipilimumab + nivolumab | Myocarditis | 6 weeks | Dyspnea, irregular heartbeats, tachycardia | Prednisone and solumedrol |
| [82] | F | 66 | Lung cancer | Nivolumab | Myocarditis | 9 weeks | Chest pain | Methylprednisolone, plasmapheresis, abatacept |
| [83] | F | 71 | Melanoma | Pembrolizumab | Myocarditis and cardiac arrhythmia | 6 weeks | Dyspnea | Methylprednisolone, mycophenolate mofetil, plasmapheresis, rituximab, alemtuzumab |
| [84] | F | 79 | Lung cancer | Pembrolizumab | Pericarditis | 9 weeks | Chest pain | Pyridostigmine and methylprednisolone |
| [25] | M | 72 | Lung cancer | anti-PD-L1 | Pericarditis | 11 weeks | Dyspnea, hypotension, hypoxia | NR |
| [25] | F | 65 | Lung cancer | anti-CTLA-4 and anti-PD-1 | Arrhythmias | 19 weeks | Loss of consciousness and hypotension | Pacemaker |
| [25] | M | 57 | Lung cancer | anti-PD-L1 | Cardiac tamponade | 14 weeks | Dyspnea, orthopnea, bilateral lower extremity edema | NR |
| [85] | M | 80 | Kidney cancer | Nivolumab | Myocarditis and atrial fibrillation | 12 weeks | Severe asthenia | Methylprednisolone |
| [86] | F | 78 | Melanoma | Nivolumab | Myocarditis | 4 weeks | Muscle weakness and dyspnea | Methylprednisolone to pulse steroid |
| [65] | F | 61 | Lung cancer | Atezolizumab | Myocarditis | Less than 1 week | Dyspnea, fatigue | Methylprednisolone and mycophenolate mofetil |
| [87] | F | 55 | Melanoma | Nivolumab | Myocarditis | 6 weeks | Dysphagia, dyspnea, limb weakness | IGI, steroid pulse, plasma exchange |
| [88] | M | 74 | Lung cancer | Nivolumab | Myocardial necrosis | 6 weeks | General malaise, appetite decrease, dyspnea | Catecholamines |
| [89] | F | 76 | T cell lymphoma | Brentuximab and nivolumab | Acute heart failure | 3 weeks | Fatigue, dyspnea, orthopnea | Solumedrol, Impella implant |
| [90] | M | 33 | Hodgkin lymphoma | Nivolumab | Complete heart block, myocarditis | 24 weeks | NR | Mycophenolate mofetil and steroids |
| [91] | M | 73 | Malignant mesothelioma | Pembrolizumab | Myocarditis | 5 weeks | Progressive dyspnea and fatigue | Prednisolone, pacemaker, IGI, and plasmapheresis |
| [91] | M | 89 | Melanoma | Pembrolizumab | Myocarditis | 3 weeks | Weakness, myalgias, and dyspnea | Methylprednisolone, oral prednisone, anti-thymocyte globulin |
| [91] | F | 65 | Lung cancer | Nivolumab | Acute coronary syndrome, acute decompensated heart failure | 1 week | Dyspnea, edema, bradycardia | Methylprednisolone, prednisone, furosemide, anti-thymocyte globulin |
| [91] | M | 67 | Melanoma | Nivolumab | Myocarditis | 9 weeks | Chest pain and palpitations | prednisone, infliximab, oral corticosteroids |
| [92] | M | 42 | Hepatocellular carcinoma | Pembrolizumab | Bradycardia | 18 weeks | Fatigue, dizziness, and anorexia | Cortisone |
| [93] | F | 47 | Melanoma | Ipilimumab + nivolumab, then nivolumab | Heart failure, asymptomatic supraventricular tachycardia | 17 weeks | Dyspnea, tachycardia, and pulmonary edema | Methylprednisolone and infliximab |
| [76] | F | 58 | Lung cancer | Nivolumab | Pericardial effusion | 12 weeks | Dyspnea and cough | Pericardiocentesis and steroids |
| [76] | M | 65 | Lung cancer | Nivolumab | Pericardial effusion | 106 weeks | Acute respiratory failure and fever | Surgical drainage and steroids |
| [94] | M | 70 | Lung cancer | Pembrolizumab | Cardiac tamponade | 9 weeks | Dyspnea and general fatigue | Pericardiocentesis |
| [95] | M | 65 | Lung cancer | Nivolumab | Cardiac tamponade | 8 weeks | Dyspnea | Pericardiocentesis |
| [95] | M | 71 | Lung cancer | Nivolumab | Cardiac tamponade | 6 weeks | Chest pain and dyspnea | Pericardiocentesis |
| [76] | F | 55 | Lung cancer | Nivolumab | Pericardial effusion | 9 weeks | None | None |
| [96] | M | 71 | Lung cancer | Nivolumab | Pericardial effusion | 5 weeks | NR | Pericardiocentesis and pericardial window |
| [97] | M | 79 | Prostate cancer | Nivolumab | Myocarditis | 8 weeks | Blurred vision, pain and stiffness in the upper back | Methylprednisolone, oral prednisone taper |
| [98] | F | 70 | Lung cancer | Nivolumab | Pericardial effusion | Less than 1 week | Chest pain and shortness of breath | Colchicine and prednisone |
| [99] | M | 74 | Lung cancer | Pembrolizumab | Myocarditis and arrhythmia | 8 weeks | Dyspnea on exertion | Prednisone, aspirin, clopidogrel, IV heparin, metoprolol succinate |
| [69] | M | 77 | Melanoma | Ipilimumab | Myocarditis | NR | Malaise, nausea, cough, bradycardia | Methylprednisolone |
| [33] | F | 67 | Multiple myeloma | Pembrolizumab | Myocarditis | 2 weeks | Dyspnea and malaise | Methylprednisolone |
| [100] | M | 52 | Renal cell carcinoma | Ipilimumab + nivolumab | Myocarditis | 6 weeks | None | Beta blocker therapy |
| [101] | M | 67 | Melanoma | Ipilimumab + nivolumab | Acute decompensated heart failure, arrhythmia, chronic heart failure | 2 weeks | Dyspnea and cough | Methylprednisolone, anti-thymocyte globulin, and permanent pacemaker implantation |
| [50] | M | 69 | Lung cancer | Nivolumab | Pericarditis, pericardial tamponade | 73 weeks | Dyspnea, tachycardia, and fever | Prednisone |
| [102] | F | 45 | Melanoma | Ipilimumab + nivolumab | Acute heart failure, Takotsubo-like syndrome | Less than 1 week | NR | Methylprednisolone |
| [102] | M | 77 | Melanoma | Ipilimumab, nivolumab | Takotsubo-like syndrome | 6 weeks | NR | Methylprednisolone |
| [21] | F | 41 | Melanoma | Ipilimumab + nivolumab | Myocarditis | 9 weeks | Dyspnea | Methylprednisolone |
| [103] | M | 60 | Melanoma | Nivolumab | Myocarditis | 39 weeks | Fatigue and fever | Prednisolone, IGI |
| [20] | F | 75 | Extraskeletal myxoid carcinoma | Durvalumab and tremelimumab | Myocarditis, heart failure, complete heart block | 3 weeks | Difficulty ambulating and dyspnea | Methylprednisolone, mycophenolate mofetil |
| [104] | F | 55 | Breast cancer | Pembrolizumab | Pericardial tamponade | 15 weeks | Pericardial chest pain | Anterior pericardectomy, corticosteroids |
| [105] | F | 76 | Lung cancer | Nivolumab | Myocarditis, complete atrioventricular block | 3 weeks | Dyspnea | Methylprednisolone and infliximab |
| [106] | M | 72 | Melanoma | Ipilimumab + nivolumab | Myocarditis | 20 weeks | Dyspnea, leg edema | Prednisolone |
| [107] | M | 73 | Lung cancer | Pembrolizumab | Complete atrioventricular block and myocarditis | 2 weeks | Faintness | Methylprednisolone and temporary pacemaker implantation |
| [108] | M | 43 | Thymoma | Nivolumab | Myocarditis | 1 week | Chest discomfort, fatigue, lower limb myalgias | IGI, methylprednisolone |
| [109] | M | 55 | Lung cancer | Nivolumab | Acute decompensated right-sided heart failure and cardiogenic shock | 1 week | Lethargy and dyspnea | NR |
| [110] | F | 49 | Melanoma | Ipilimumab + nivolumab | Myocarditis | 2 weeks | Atypical chest discomfort at the cardiac apex | Methylprednisolone and IGI |
| [111] | F | 35 | Melanoma | Ipilimumab | Myocarditis | 2 weeks | Progressive dyspnea | Methylprednisolone, IGI, plasma exchanges |
| [112] | M | 61 | Lung cancer | Nivolumab | Acute coronary syndrome | 33 weeks | NR | Corticosteroids |
| [113] | M | 60 | Lung cancer | Nivolumab | Pericarditis | 17 weeks | NR | Pericardiocentesis and methylprednisolone |
| [114] | M | 68 | Histiocytosis and left buttock sarcoma | Anti-PD-L1 and anti-CTLA-4 (unspecified) | Myocarditis and arrhythmia | 2 weeks | Fatigue, general malaise, weakness | Steroids, mycophenolate mofetil, temporary transvenous pacing wire followed by a permanent pacemaker |
| [115] | M | 54 | Lung cancer | Nivolumab | Heart failure | 4 weeks | Dizziness, nausea, loss of consciousness, general paralysis | High dose steroids and a pacemaker |
| [116] | M | 63 | Melanoma | Nivolumab | Atrioventricular block, myocardial infarction | 3 weeks | Dyspnea, dysphagia, worsened muscle pain | Prednisone and antibiotic therapy (sultamicillin), aspirin, and unfractionated heparin |
| [117] | M | 59 | Lung cancer | Nivolumab | Cardiac tamponade | 9 weeks | NR | Pericardiocentesis, prednisone, and anti-tubercular treatment |
| [118] | M | 67 | Lung cancer | Nivolumab | Cardiac tamponade | 15 weeks | Acute respiratory failure | Pericardiocentesis and prednisone |
| [35] | F | 65 | Melanoma | Ipilimumab | Cardiac tamponade | 38 weeks | Shortness of breath and chest discomfort | Pericardiocentesis and methylprednisolone |
| [119] | M | 46 | Small cell lung cancer | Nivolumab | Cardiac tamponade | 9 weeks | NR | Pericardiocentesis |
| [119] | F | 54 | Lung cancer | Nivolumab | Cardiac tamponade | 7 weeks | NR | Pericardiocentesis and prednisone |
| [11] | F | 65 | Melanoma | Ipilimumab + nivolumab | Myocarditis | 2 weeks | Atypical chest pain, dyspnea, fatigue | Methylprednisolone |
| [11] | M | 63 | Melanoma | Ipilimumab + nivolumab | Myocarditis | 2 weeks | Fatigue and myalgias | Methylprednisolone and infliximab |
| [120] | M | 60 | Melanoma | Ipilimumab | Atrial fibrillation | 104 weeks | None | Lisinopril, metoprolol changed to carvedilol |
| [121] | F | 68 | Melanoma | Ipilimumab and nivolumab | Myocarditis | 2 weeks | Right eye ptosis, generalized weakness and fatigue | Steroids |
| [122] | M | 73 | Melanoma | Ipilimumab and nivolumab followed by pembrolizumab | Myocarditis with cardiomyopathy and ventricular arrhythmia | 2 weeks after starting pembrolizumab | NR | Prednisolone |
| [122] | M | 87 | Melanoma | Nivolumab | Asystole | 17 weeks | Cardiac arrest | Prednisolone |
| [122] | M | 77 | Melanoma | Ipilimumab followed by penbrolizumab | Stable angina pectoris | 10 weeks | Stable angina pectoris | None |
| [123] | F | 69 | Melanoma | Nivolumab | Myocarditis | 9 weeks | General malaise and palpitations | Prednisolone |
| [26] | M | 72 | Melanoma | Ipilimumab | Myocarditis | 9 weeks | Dyspnea and anasarca | Corticosteroids |
| [26] | M | 68 | Melanoma | Ipilimumab | Cardiomyopathy | 12 weeks | Dyspnea and lower extremity edema | Diuresis and coronary catheterization |
| [26] | M | 71 | Melanoma | Ipilimumab | Myocardial fibrosis | 6 weeks | No obvious cardiac symptoms | High dose steroids |
| [26] | M | 81 | Melanoma | Ipilimumab | Heart failure, myocarditis | 20 weeks | Progressive subacute dyspnea | Diuretics |
| [26] | M | 23 | Melanoma | Ipilimumab | Myocarditis and heart failure | 30 weeks | Chest pain and cough | Methylprednisolone converted to prednisone |
| [26] | M | 64 | Melanoma | Ipilimumab | Myocarditis | 6 weeks | Fatigue, seizures, and abdominal pain (Yun et al. 2015) | Dopamine and fentanyl |
| [26] | M | 88 | Melanoma | Pembrolizumab | Cardiac arrest | 24 weeks | Myalgia and pain in the shoulder | Corticosteroids |
| [26] | M | 80 | Non-Hodgkin lymphoma | Ipilimumab | Myocarditis | 8 weeks | Dyspnea, edema, and arrhythmia | Methylprednisolone and prednisone |
| [124] | M | 64 | Lung cancer | Nivolumab | Cardiac tamponade | 13 weeks | Pericardial chest pain | Pericardiocentesis and pericardial window |
| [125] | M | 75 | Lung cancer | Nivolumab | Myocarditis | 18 weeks | Acute dyspnea and chest pain | Prednisolone, ACE inhibitor, beta blocker, diuretic therapy |
| [126] | F | 68 | Lung cancer | Nivolumab | Myocarditis and arrhythmia | 3 weeks | Altered mental status, nausea, and vomiting | Methylprednisolone and amiodarone IV |
| [127] | F | 83 | Melanoma | Ipilimumab | Takotsubo cardiomyopathy | 15 weeks | Substernal chest pain and dyspnea | Beta blocker therapy |
| [42] | F | 73 | Melanoma | Pembrolizumab | Acute heart failure | 15 weeks | Progressive dyspnea | AT-2 receptor blocker, beta blocker, spironolactone, and diuretics |
| [128] | M | 59 | Melanoma | Ipilimumab | Acute fibrinous pericarditis | 24 weeks | Chest pain and dyspnea | Methylprednisolone, prednisone, budesonide |
References
- Varricchi, G.; Galdiero, M.R.; Marone, G.; Criscuolo, G.; Triassi, M.; Bonaduce, D.; Marone, G.; Tocchetti, C.G. Cardiotoxicity of immune checkpoint inhibitors. ESMO Open 2017, 2, e000247. Available online: https://pubmed.ncbi.nlm.nih.gov/29104763/ (accessed on 5 July 2021).
- Zhang, B.; Rocci, M.L.; Twomey, J.D. Theme: Identification and Implementation of Predictive Biomarkers for Checkpoint Targeted Immunotherapy Cancer Immunotherapy Update: FDA-Approved Checkpoint Inhibitors and Companion Diagnostics. AAPS J. 2021, 23, 39. [Google Scholar]
- Rowshanravan, B.; Halliday, N.; Sansom, D.M. CTLA-4: A moving target in immunotherapy. Blood Am. Soc. Hematol. 2018, 131, 58–67. Available online: http://ashpublications.org/blood/article-pdf/131/1/58/1367947/blood741033.pdf (accessed on 30 June 2021). [CrossRef]
- Qin, W.; Hu, L.; Zhang, X.; Jiang, S.; Li, J.; Zhang, Z.; Wang, X. The Diverse Function of PD-1/PD-L Pathway Beyond Cancer. Front. Immunol. 2019, 10, 2298. [Google Scholar] [CrossRef]
- Tarrio, M.L.; Grabie, N.; Bu, D.-X.; Sharpe, A.H.; Lichtman, A.H. PD-1 Protects against Inflammation and Myocyte Damage in T Cell-Mediated Myocarditis. J. Immunol. 2012, 188, 4876–4884. Available online: https://pubmed.ncbi.nlm.nih.gov/22491251/ (accessed on 27 June 2021).
- Zhang, L.; Reynolds, K.L.; Lyon, A.R.; Palaskas, N.; Neilan, T.G. The Evolving Immunotherapy Landscape and the Epidemiology, Diagnosis, and Management of Cardiotoxicity. JACC CardioOncol. 2021, 3, 35–47. [Google Scholar] [CrossRef]
- Waliany, S.; Lee, D.; Witteles, R.M.; Neal, J.W.; Nguyen, P.; Davis, M.M.; Salem, J.-E.; Wu, S.M.; Moslehi, J.J.; Zhu, H. Immune Checkpoint Inhibitor Cardiotoxicity: Understanding Basic Mechanisms and Clinical Characteristics and Finding a Cure. Annu. Rev. Pharmacol. Toxicol. 2021, 61, 113–134. [Google Scholar] [CrossRef]
- Michot, J.; Bigenwald, C.; Champiat, S.; Collins, M.; Carbonnel, F.; Postel-Vinay, S.; Berdelou, A.; Varga, A.; Bahleda, R.; Hollebecque, A.; et al. Immune-related adverse events with immune checkpoint blockade: A comprehensive review. Eur. J. Cancer 2016, 54, 139–148. [Google Scholar] [CrossRef]
- Cathcart-Rake, E.J.; Sangaralingham, L.R.; Henk, H.J.; Shah, N.D.; bin Riaz, I.; Mansfield, A.S. A Population-based Study of Immunotherapy-related Toxicities in Lung Cancer. Clin. Lung Cancer 2020, 21, 421–427.e2. [Google Scholar] [CrossRef]
- Puzanov, I.; on behalf of the Society for Immunotherapy of Cancer Toxicity Management Working Group; Diab, A.; Abdallah, K.; Bingham, C.O.; Brogdon, C.; Dadu, R.; Hamad, L.; Kim, S.; Lacouture, M.E.; et al. Managing toxicities associated with immune checkpoint inhibitors: Consensus recommendations from the Society for Immunotherapy of Cancer (SITC) Toxicity Management Working Group. J. Immunother. Cancer 2017, 5, 95. Available online: https://pubmed.ncbi.nlm.nih.gov/29162153/ (accessed on 20 June 2021).
- Johnson, D.B.; Balko, J.M.; Compton, M.L.; Chalkias, S.; Gorham, J.; Xu, Y.; Hicks, M.; Puzanov, I.; Alexander, M.R.; Bloomer, T.L.; et al. Fulminant Myocarditis with Combination Immune Checkpoint Blockade. N. Engl. J. Med. 2016, 375, 1749–1755. Available online: https://pubmed.ncbi.nlm.nih.gov/27806233/ (accessed on 20 June 2021).
- Rubio-Infante, N.; Ramírez-Flores, Y.A.; Castillo, E.C.; Lozano, O.; García-Rivas, G.; Torre-Amione, G. Cardiotoxicity associated with immune checkpoint inhibitor therapy: A meta-analysis. Eur. J. Heart Fail. 2021. Available online: https://pubmed.ncbi.nlm.nih.gov/34196077/ (accessed on 31 June 2021).
- D’Souza, M.; Nielsen, D.; Svane, I.M.; Iversen, K.; Rasmussen, P.V.; Madelaire, C.; Fosbøl, E.; Køber, L.; Gustafsson, F.; Andersson, C.; et al. The risk of cardiac events in patients receiving immune checkpoint inhibitors: A nationwide Danish study. Eur. Heart J. 2021, 42, 1621–1631. Available online: https://pubmed.ncbi.nlm.nih.gov/33291147/ (accessed on 31 June 2021).
- Totzeck, M.; Lutgens, E.; Neilan, T.G. Are we underestimating the potential for cardiotoxicity related to immune checkpoint inhibitors? Eur. Heart J. 2021, 42, 1632–1635. Available online: https://pubmed.ncbi.nlm.nih.gov/33291139/ (accessed on 31 June 2021).
- Michel, L.; Rassaf, T.; Totzeck, M. Cardiotoxicity from immune checkpoint inhibitors. IJC Heart Vasc. 2019, 25, 100420. [Google Scholar] [CrossRef]
- Hu, J.R.; Florido, R.; Lipson, E.J.; Naidoo, J.; Ardehali, R.; Tocchetti, C.G.; Lyon, A.R.; Padera, R.F.; Johnson, D.B.; Moslehi, J. Cardiovascular toxicities associated with immune checkpoint inhibitors. Cardiovasc. Res. 2019, 115, 854–868. Available online: https://pubmed.ncbi.nlm.nih.gov/30715219/ (accessed on 5 June 2021).
- Chen, D.-Y.; Huang, W.-K.; Wu, V.C.-C.; Chang, W.-C.; Chen, J.-S.; Chuang, C.-K.; Chu, P.-H. Cardiovascular toxicity of immune checkpoint inhibitors in cancer patients: A review when cardiology meets immuno-oncology. J. Formos. Med. Assoc. 2020, 119, 1461–1475. [Google Scholar] [CrossRef]
- Escudier, M.; Cautela, J.; Malissen, N.; Ancedy, Y.; Orabona, M.; Pinto, J.; Monestier, S.; Grob, J.J.; Scemama, U.; Jacquier, A.; et al. Clinical features, management, and outcomes of immune checkpoint inhibitor-related cardiotoxicity. Circulation 2017, 136, 2085–2087. Available online: https://pubmed.ncbi.nlm.nih.gov/29158217/ (accessed on 27 June 2021).
- Chahine, J.; Collier, P.; Maroo, A.; Tang, W.W.; Klein, A.L. Myocardial and Pericardial Toxicity Associated With Immune Checkpoint Inhibitors in Cancer Patients. JACC Case Rep. 2020, 2, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, S.S.; Fradley, M.G.; Cohen, J.v.; Nohria, A.; Reynolds, K.L.; Heinzerling, L.M.; Sullivan, R.J.; Damrongwatanasuk, R.; Chen, C.L.; Gupta, D.; et al. Myocarditis in Patients Treated With Immune Checkpoint Inhibitors. J. Am. Coll. Cardiol. 2018, 71, 1755–1764. Available online: https://pubmed.ncbi.nlm.nih.gov/29567210/ (accessed on 27 June 2021).
- Ganatra, S.; Neilan, T.G. Immune Checkpoint Inhibitor-Associated Myocarditis. Oncologist 2018, 23, 879–886. Available online: https://pubmed.ncbi.nlm.nih.gov/29802219/ (accessed on 5 June 2021).
- Sławiński, G.; Wrona, A.; Dabrowska-Kugacka, A.; Raczak, G.; Lewicka, E. Immune checkpoint inhibitors and cardiac toxicity in patients treated for non-small lung cancer: A review. Int. J. Mol. Sci. 2020, 21, 1–19. Available online: https://pubmed.ncbi.nlm.nih.gov/33003425/ (accessed on 5 June 2021).
- Patel, R.P.; Parikh, R.; Gunturu, K.S.; Tariq, R.Z.; Dani, S.S.; Ganatra, S.; Nohria, A. Cardiotoxicity of Immune Checkpoint Inhibitors. Curr. Oncol. Rep. 2021, 23. Available online: https://pubmed.ncbi.nlm.nih.gov/33937956/ (accessed on 5 June 2021).
- Lobenwein, D.; Kocher, F.; Dobner, S.; Gollmann-Tepeköylü, C.; Holfeld, J. Cardiotoxic mechanisms of cancer immunotherapy—A systematic review. Int. J. Cardiol. 2021, 323, 179–187. [Google Scholar] [CrossRef]
- Altan, M.; Toki, M.; Gettinger, S.N.; Carvajal-Hausdorf, D.E.; Zugazagoitia, J.; Sinard, J.H.; Herbst, R.S.; Rimm, D.L. Immune Checkpoint Inhibitor–Associated Pericarditis. J. Thorac. Oncol. 2019, 14, 1102–1108. [Google Scholar] [CrossRef] [PubMed]
- Heinzerling, L.; Ott, P.A.; Hodi, F.S.; Husain, A.N.; Tajmir-Riahi, A.; Tawbi, H.; Pauschinger, M.; Gajewski, T.F.; Lipson, E.J.; Luke, J.J. Cardiotoxicity associated with CTLA4 and PD1 blocking immunotherapy. J. Immunother. Cancer 2016, 4, 50. Available online: https://pubmed.ncbi.nlm.nih.gov/27532025/ (accessed on 5 June 2021).
- Zhou, Y.-W.; Zhu, Y.-J.; Wang, M.-N.; Xie, Y.; Chen, C.-Y.; Zhang, T.; Xia, F.; Ding, Z.-Y.; Liu, J.-Y. Immune Checkpoint Inhibitor-Associated Cardiotoxicity: Current Understanding on Its Mechanism, Diagnosis and Management. Front. Pharmacol. 2019, 10, 1350. [Google Scholar] [CrossRef]
- Baik, A.H.; Oluwole, O.O.; Johnson, D.B.; Shah, N.; Salem, J.-E.; Tsai, K.K.; Moslehi, J.J. Mechanisms of Cardiovascular Toxicities Associated With Immunotherapies. Circ. Res. 2021, 128, 1780–1801. Available online: https://pubmed.ncbi.nlm.nih.gov/33934609/ (accessed on 31 June 2021).
- Tay, W.T.; Fang, Y.-H.; Beh, S.T.; Liu, Y.-W.; Hsu, L.-W.; Yen, C.-J.; Liu, P.-Y. Programmed Cell Death-1: Programmed Cell Death-Ligand 1 Interaction Protects Human Cardiomyocytes Against T-Cell Mediated Inflammation and Apoptosis Response In Vitro. Int. J. Mol. Sci. 2020, 21, 2399. Available online: https://pubmed.ncbi.nlm.nih.gov/32244307/ (accessed on 20 June 2021).
- Quagliariello, V.; Passariello, M.; Rea, D.; Barbieri, A.; Iovine, M.; Bonelli, A.; Caronna, A.; Botti, G.; De Lorenzo, C.; Maurea, N. Evidences of CTLA-4 and PD-1 Blocking Agents-Induced Cardiotoxicity in Cellular and Preclinical Models. J. Pers. Med. 2020, 10, 1–19. Available online: https://pubmed.ncbi.nlm.nih.gov/33086484/ (accessed on 31 June 2021).
- Wang, J.; Okazaki, I.-M.; Yoshida, T.; Chikuma, S.; Kato, Y.; Nakaki, F.; Hiai, H.; Honjo, T.; Okazaki, T. PD-1 deficiency results in the development of fatal myocarditis in MRL mice. Int. Immunol. 2010, 22, 443–452. Available online: https://pubmed.ncbi.nlm.nih.gov/20410257/ (accessed on 20 June 2021).
- Love, V.A.; Grabie, N.; Duramad, P.; Stavrakis, G.; Sharpe, A.; Lichtman, A. CTLA-4 ablation and interleukin-12-driven differentiation synergistically augment cardiac pathogenicity of cytotoxic T lymphocytes. Circ. Res. 2007, 101, 248–257. Available online: https://pubmed.ncbi.nlm.nih.gov/17569889/ (accessed on 27 June 2021).
- Martinez-Calle, N.; Rodriguez-Otero, P.; Villar, S.; Mejías, L.; Melero, I.; Prosper, F.; Marinello, P.; Paiva, B.; Idoate-Gastearena, M.; Miguel, J.S. Anti-PD1 associated fulminant myocarditis after a single pembrolizumab dose: The role of occult pre-existing autoimmunity. Haematologica 2018, 103, e318–e321. Available online: https://europepmc.org/articles/PMC6029537 (accessed on 8 June 2021). [CrossRef]
- Xu, S.; Sharma, U.C.; Tuttle, C.; Pokharel, S. Immune Checkpoint Inhibitors: Cardiotoxicity in Pre-clinical Models and Clinical Studies. Front. Cardiovasc. Med. 2021, 8, 619650. [Google Scholar] [CrossRef]
- Dasanu, C.A.; Jen, T.; Skulski, R. Late-onset pericardial tamponade, bilateral pleural effusions and recurrent immune monoarthritis induced by ipilimumab use for metastatic melanoma. J. Oncol. Pharm. Pract. 2017, 23, 231–234. [Google Scholar] [CrossRef]
- Moslehi, J.J.; Salem, J.E.; Sosman, J.A.; Lebrun-Vignes, B.; Johnson, D.B. Increased reporting of fatal immune checkpoint inhibitor-associated myocarditis. Lancet 2018, 391, 933. Available online: https://pubmed.ncbi.nlm.nih.gov/29536852/ (accessed on 27 June 2021).
- Palaskas, N.; Lopez-Mattei, J.; Durand, J.B.; Iliescu, C.; Deswal, A. Immune Checkpoint Inhibitor Myocarditis: Pathophysiological Characteristics, Diagnosis, and Treatment. J. Am. Hear. Assoc. 2020, 9, e013757. [Google Scholar] [CrossRef] [PubMed]
- Waliany, S.; Neal, J.W.; Reddy, S.; Wakelee, H.; Shah, S.A.; Srinivas, S.; Padda, S.K.; Fan, A.C.; Colevas, A.D.; Wu, S.M.; et al. Myocarditis Surveillance With High-Sensitivity Troponin I During Cancer Treatment With Immune Checkpoint Inhibitors. JACC CardioOncol. 2021, 3, 137–139. Available online: https://pubmed.ncbi.nlm.nih.gov/33796869/ (accessed on 31 June 2021).
- Pirozzi, F.; Poto, R.; Aran, L.; Cuomo, A.; Galdiero, M.R.; Spadaro, G.; Abete, P.; Bonaduce, D.; Marone, G.; Tocchetti, C.G.; et al. Cardiovascular Toxicity of Immune Checkpoint Inhibitors: Clinical Risk Factors. Curr. Oncol. Rep. 2021, 23, 13. Available online: https://pubmed.ncbi.nlm.nih.gov/33415405/ (accessed on 5 June 2021).
- Balanescu, D.V.; Donisan, T.; Palaskas, N.L.; Iliescu, C. Emerging Concerns in Cardio-Oncology: Immune Checkpoint Inhibitor Cardiotoxicity. Am. Coll. Cardiol. 2019. Available online: https://www.acc.org/latest-in-cardiology/articles/2019/06/21/08/45/emerging-concerns-in-cardio-oncology (accessed on 30 June 2021).
- Wang, D.Y.; Okoye, G.; Neilan, T.G.; Johnson, D.B.; Moslehi, J.J. Cardiovascular Toxicities Associated with Cancer Immunotherapies. Curr. Cardiol. Rep. 2017, 19, 21. [Google Scholar] [CrossRef]
- Läubli, H.; Balmelli, C.; Bossard, M.; Pfister, O.; Glatz, K.; Zippelius, A. Acute heart failure due to autoimmune myocarditis under pembrolizumab treatment for metastatic melanoma. J. Immunother. Cancer 2015, 3, 11. Available online: https://pubmed.ncbi.nlm.nih.gov/25901283/ (accessed on 20 June 2021).
- Lal, J.C.; Brown, S.-A.; Collier, P.; Cheng, F. A retrospective analysis of cardiovascular adverse events associated with immune checkpoint inhibitors. Cardio-Oncology 2021, 7, 1–10. Available online: https://pubmed.ncbi.nlm.nih.gov/34049595/ (accessed on 5 June 2021).
- Lyon, A.R.; Yousaf, N.; Battisti, N.M.L.; Moslehi, J.; Larkin, J. Immune checkpoint inhibitors and cardiovascular toxicity. Lancet Oncol. 2018, 19, e447–e458. [Google Scholar] [CrossRef]
- Awadalla, M.; Golden, D.L.A.; Mahmood, S.S.; Alvi, R.M.; Mercaldo, N.D.; Hassan, M.; Banerji, D.; Rokicki, A.; Mulligan, C.; Murphy, S.P.T.; et al. Influenza vaccination and myocarditis among patients receiving immune checkpoint inhibitors. J. Immunother. Cancer 2019, 7, 53. Available online: https://jitc.bmj.com/lookup/doi/10.1186/s40425-019-0535-y (accessed on 27 June 2021). [CrossRef]
- Varricchi, G.; Galdiero, M.R.; Tocchetti, C.G. Cardiac toxicity of immune checkpoint inhibitors: Cardio-oncology meets immunology. Circulation 2017, 136, 1989–1992. Available online: http://ahajournals.org (accessed on 30 June 2021). [CrossRef] [PubMed]
- Gong, J.; Drobni, Z.D.; Zafar, A.; Quinaglia, T.; Hartmann, S.; Gilman, H.K.; Raghu, V.K.; Gongora, C.E.; Sise, M.; Alvi, R.M.; et al. Pericardial disease in patients treated with immune checkpoint inhibitors. J. Immunother. Cancer 2021, 9, e002771. Available online: https://pubmed.ncbi.nlm.nih.gov/34145031/ (accessed on 5 June 2021).
- Salem, J.E.; Manouchehri, A.; Moey, M.; Lebrun-Vignes, B.; Bastarche, L.; Pariente, A.; Gobert, A.; Spano, J.-P.; Balko, J.M.; Bonaca, M.P.; et al. Cardiovascular toxicities associated with immune checkpoint inhibitors: An observational, retrospective, pharmacovigilance study. Lancet Oncol. 2018, 19, 1579–1589. Available online: https://pubmed.ncbi.nlm.nih.gov/30442497/ (accessed on 8 June 2021). [CrossRef]
- Moriyama, S.; Fukata, M.; Tatsumoto, R.; Kono, M. Refractory constrictive pericarditis caused by an immune checkpoint inhibitor properly managed with infliximab: A case report. Eur. Heart J. Case Rep. 2021, 5, ytab002. Available online: https://pubmed.ncbi.nlm.nih.gov/33644656/ (accessed on 5 June 2021).
- De Almeida, D.V.; Gomes, J.R.; Haddad, F.J.; Buzaid, A.C. Immune-mediated Pericarditis With Pericardial Tamponade During Nivolumab Therapy. J. Immunother. 2018, 41, 329–331. [Google Scholar] [CrossRef]
- Yang, S.; Asnani, A. Cardiotoxicities associated with immune checkpoint inhibitors. Curr. Probl. Cancer 2018, 42, 422–432. [Google Scholar] [CrossRef]
- Tan, N.Y.L.; Anavekar, N.S.; Wiley, B.M. Concomitant myopericarditis and takotsubo syndrome following immune checkpoint inhibitor therapy. BMJ Case Rep. 2020, 13, e235265. [Google Scholar] [CrossRef]
- Inno, A.; Maurea, N.; Metro, G.; Carbone, A.; Russo, A.; Gori, S. Immune checkpoint inhibitors-associated pericardial disease: A systematic review of case reports. Cancer Immunol. Immunother. 2021, 70, 3041–3053. Available online: https://pubmed.ncbi.nlm.nih.gov/33877385/ (accessed on 5 June 2021).
- BC Cancer. Ipilimumab. Available online: http://www.bccancer.bc.ca/drug-database-site/Drug%20Index/Ipilimumab_monograph.pdf (accessed on 3 June 2021).
- FDA. Highlights of Prescribing Information: Ipilimumab. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/125377s110lbl.pdf (accessed on 3 June 2021).
- Dolladille, C.; Ederhy, S.; Sassier, M.; Cautela, J.; Thuny, F.; Cohen, A.A.; Fedrizzi, S.; Chrétien, B.; DA Silva, A.; Plane, A.-F.; et al. Immune Checkpoint Inhibitor Rechallenge After Immune-Related Adverse Events in Patients With Cancer. JAMA Oncol. 2020, 6, 865–871. [Google Scholar] [CrossRef]
- BC Cancer. Pembrolizumab. Available online: http://www.bccancer.bc.ca/drug-database-site/Drug%20Index/pembrolizumab_monograph.pdf (accessed on 3 June 2021).
- FDA. Highlights of Prescribing Information: Pembrolizumab. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/125514s096lbl.pdf (accessed on 3 June 2021).
- BC Cancer. Nivolumab. Available online: http://www.bccancer.bc.ca/drug-database-site/Drug%20Index/nivolumab_monograph.pdf (accessed on 3 June 2021).
- FDA. Highlights of Prescribing Information: Nivolumab. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/125554s090lbl.pdf (accessed on 3 June 2021).
- Brahmer, J.R.; Drake, C.G.; Wollner, I.; Powderly, J.D.; Picus, J.; Sharfman, W.H.; Stankevich, E.; Stankevich, A.; Salay, T.M.; McMiller, T.L.; et al. Phase I study of single-agent anti-programmed death-1 (MDX-1106) in refractory solid tumors: Safety, clinical activity, pharmacodynamics, and immunologic correlates. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 3167–3175. Available online: https://pubmed.ncbi.nlm.nih.gov/20516446/ (accessed on 7 June 2021).
- June 25 2020—EPOV Scott Gettinger—The ASCO Post. Available online: https://ascopost.com/issues/june-25-2020/epov-scott-gettinger/ (accessed on 20 June 2021).
- BC Cancer. Atezolizumab. Available online: http://www.bccancer.bc.ca/drug-database-site/Drug%20Index/Atezolizumab_Monograph.pdf (accessed on 6 August 2021).
- FDA. Highlights of Prescribing Information: Atezolizumab. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/761034s033s034s035s036s037s038lbl.pdf (accessed on 6 August 2021).
- Liu, S.-Y.; Huang, W.-C.; Yeh, H.-I.; Ko, C.-C.; Shieh, H.-R.; Hung, C.-L.; Chen, T.-Y.; Chen, Y.-J. Sequential Blockade of PD-1 and PD-L1 Causes Fulminant Cardiotoxicity-From Case Report to Mouse Model Validation. Cancers 2019, 11, 580. Available online: https://pubmed.ncbi.nlm.nih.gov/31022941/ (accessed on 6 August 2021).
- FDA. Highlights of Prescribing Information: Durvalumab. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/761069s002lbl.pdf (accessed on 6 August 2021).
- BC Cancer. Durvalumab. Available online: http://www.bccancer.bc.ca/drug-database-site/Drug%20Index/Durvalumab_monograph.pdf (accessed on 6 August 2021).
- Brahmer, J.R.; Lacchetti, C.; Schneider, B.J.; Atkins, M.B.; Brassil, K.J.; Caterino, J.M.; Chau, L.; Ernstoff, M.S.; Gardner, G.M.; Ginex, P.; et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: American society of clinical oncology clinical practice guideline. J. Clin. Oncol. 2018, 36, 1714–1768. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6481621/ (accessed on 30 June 2021). [CrossRef]
- Samara, Y.; Yu, C.L.; Dasanu, C.A. Acute autoimmune myocarditis and hepatitis due to ipilimumab monotherapy for malignant melanoma. J. Oncol. Pharm. Pract. 2019, 25, 966–968. [Google Scholar] [CrossRef]
- Poto, R.; Marone, G.; Pirozzi, F.; Galdiero, M.R.; Cuomo, A.; Formisano, L.; Bianco, R.; Maria Della Corte, C.; Morgillo, F.; Napolitano, S.; et al. How can we manage the cardiac toxicity of immune checkpoint inhibitors? Expert Opin. Drug Saf. 2021, 20. Available online: https://pubmed.ncbi.nlm.nih.gov/33749484/ (accessed on 30 July 2021).
- Konala, V.M.; Adapa, S.; Aronow, W.S. Immune Checkpoint Inhibitors–Related Cardiotoxicity. Am. J. Ther. 2020, 27, e591–e598. Available online: https://pubmed.ncbi.nlm.nih.gov/31008763/ (accessed on 30 July 2021).
- Spallarossa, P.; Sarocchi, M.; Tini, G.; Arboscello, E.; Toma, M.; Ameri, P.; Porto, I. How to Monitor Cardiac Complications of Immune Checkpoint Inhibitor Therapy. Front. Pharmacol. 2020, 11, 972. Available online: https://pubmed.ncbi.nlm.nih.gov/32676031/ (accessed on 31 July 2021).
- Sarocchi, M.; Grossi, F.; Arboscello, E.; Bellodi, A.; Genova, C.; Bello, M.G.D.; Rijavec, E.; Barletta, G.; Biello, F.; Ghigliotti, G.; et al. Serial Troponin for Early Detection of Nivolumab Cardiotoxicity in Advanced Non-Small Cell Lung Cancer Patients. Oncologist 2018, 23, 936–942. Available online: https://pubmed.ncbi.nlm.nih.gov/29567824/ (accessed on 30 July 2021).
- Shalata, W.; Peled, N.; Gabizon, I.; Abu Saleh, O.; Kian, W.; Yakobson, A. Associated Myocarditis: A Predictive Factor for Response? Case Rep. Oncol. 2020, 13, 550–557. [Google Scholar] [CrossRef]
- Balanescu, D.V.; Donisan, T.; Palaskas, N.; Lopez-Mattei, J.; Kim, P.Y.; Buja, L.M.; McNamara, D.M.; Kobashigawa, J.A.; Durand, J.B.; Iliescu, C.A. Immunomodulatory treatment of immune checkpoint inhibitor-induced myocarditis: Pathway toward precision-based therapy. Cardiovasc. Pathol. 2020, 47, 107211. Available online: https://pubmed.ncbi.nlm.nih.gov/32268262/ (accessed on 31 July 2021).
- Saade, A.; Mansuet-Lupo, A.; Arrondeau, J.; Thibault, C.; Mirabel, M.; Goldwasser, F.; Oudard, S.; Weiss, L. Pericardial effusion under nivolumab: Case-reports and review of the literature. J. Immunother. Cancer 2019, 7, 335. Available online: https://pubmed.ncbi.nlm.nih.gov/31627742/ (accessed on 31 July 2021).
- Al-Obaidi, A.; Parker, N.A.; Choucair, K.; Alderson, J.; Deutsch, J.M. A Case of Acute Heart Failure Following Immunotherapy for Metastatic Lung Cancer. Cureus 2020, 12, e8093. Available online: https://pubmed.ncbi.nlm.nih.gov/32542148/ (accessed on 31 July 2021).
- Khan, A.M.; Munir, A.; Thalody, V.; Munshi, M.K.; Mehdi, S. Cardiac tamponade in a patient with stage IV lung adenocarcinoma treated with pembrolizumab. Immunotherapy 2019, 11, 1533–1540. Available online: https://pubmed.ncbi.nlm.nih.gov/31815569/ (accessed on 31 July 2021).
- Asai, M.; Kato, Y.; Kawai, S.; Watanabe, K.; Yomota, M.; Okuma, Y.; Hosomi, Y.; Hishima, T.; Okamura, T. Management of cardiac tamponade during nivolumab of lung cancer with intrapericardial bleomycin: Case report. Immunotherapy 2019, 11, 467–472. Available online: https://pubmed.ncbi.nlm.nih.gov/30727791/ (accessed on 22 July 2021).
- Atallah-Yunes, S.A.; Kadado, A.J.; Soe, M.H. Pericardial effusion due to pembrolizumab-induced immunotoxicity: A case report and literature review. Curr. Probl. Cancer. 2019, 43, 504–510. Available online: https://pubmed.ncbi.nlm.nih.gov/30685067/ (accessed on 22 July 2021).
- Khoury, Z.H.; Hausner, P.F.; Idzik-Starr, C.L.; Frykenberg, M.R.A.; Brooks, J.K.; Dyalram, D.; Basile, J.R.; Younis, R.H. Combination nivolumab/ipilimumab immunotherapy for melanoma with subsequent unexpected cardiac arrest: A case report and review of literature. J. Immunother. 2019, 42, 313–317. [Google Scholar] [CrossRef]
- Salem, J.E.; Allenbach, Y.; Vozy, A.; Brechot, N.; Johnson, D.B.; Moslehi, J.J.; Kerneis, M. Abatacept for severe immune checkpoint inhibitor-associated myocarditis. N. Engl. J. Med. 2019, 380, 2377–2379. [Google Scholar] [CrossRef]
- Esfahani, K.; Buhlaiga, N.; Thébault, P.; Lapointe, R.; Johnson, N.A.; Miller, W.H. Alemtuzumab for immune-related myocarditis due to PD-1 therapy. N. Engl. J. Med. 2019, 380, 2375–2376. [Google Scholar] [CrossRef]
- Dhenin, A.; Samartzi, V.; Lejeune, S.; Seront, E. Cascade of immunologic adverse events related to pembrolizumab treatment. BMJ Case Rep. 2019, 12, 6. [Google Scholar] [CrossRef]
- Huertas, R.M.; Serrano, C.S.; Perna, C.; Gómez, A.F.; Gordoa, T.A. Cardiac toxicity of immune-checkpoint inhibitors: A clinical case of nivolumab-induced myocarditis and review of the evidence and new challenges. Cancer Manag. Res. 2019, 11, 4541. [Google Scholar] [CrossRef] [Green Version]
- Fazel, M.; Jedlowski, P.M. Severe myositis, myocarditis, and myasthenia gravis with elevated anti-striated muscle antibody following single dose of ipilimumab-nivolumab therapy in a patient with metastatic melanoma. Case Reports Immunol. 2019, 2019, 2539493. [Google Scholar] [CrossRef] [Green Version]
- So, H.; Ikeguchi, R.; Kobayashi, M.; Suzuki, M.; Shimizu, Y.; Kitagawa, K. PD-1 inhibitor-associated severe myasthenia gravis with necrotizing myopathy and myocarditis. J. Neurol. Sci. 2019, 399, 97–100. [Google Scholar] [CrossRef]
- Sakai, T.; Yahagi, K.; Hoshino, T.; Yokota, T.; Tanabe, K.; Mori, M.; Ikeda, S. Nivolumab-induced myocardial necrosis in a patient with lung cancer: A case report. Respir. Med. Case Rep. 2019, 27, 100839. [Google Scholar] [CrossRef]
- Sharma, M.; Suero-Abreu, G.A.; Kim, B. A Case of Acute Heart Failure due to Immune Checkpoint Blocker Nivolumab. Cardiol. Res. 2019, 10, 120–123. [Google Scholar] [CrossRef]
- Charles, J.; Giovannini, D.; Terzi, N.; Schwebel, C.; Sturm, N.; Masson, D.; Leccia, M.T.; Cahn, J.Y.; Manches, O.; Bulabois, C.E.; et al. Multi-organ failure induced by Nivolumab in the context of allo-stem cell transplantation. Exp. Hematol. Oncol. 2019, 8, 8. [Google Scholar] [CrossRef]
- Agrawal, N.; Khunger, A.; Vachhani, P.; Colvin, T.A.; Hattoum, A.; Spangenthal, E.; Curtis, A.B.; Dy, G.K.; Ernstoff, M.S.; Puzanov, I. Cardiac toxicity associated with immune checkpoint inhibitors: Case series and review of the literature. Case Rep. Oncol. 2019, 12, 260–276. [Google Scholar] [CrossRef]
- Hsu, C.Y.; Su, Y.W.; Chen, S.C. Sick sinus syndrome associated with anti-programmed cell death-1. J. Immunother. Cancer 2018, 6, 72. [Google Scholar] [CrossRef] [Green Version]
- Gallegos, C.; Rottmann, D.; Nguyen, V.Q.; Baldassarre, L.A. Myocarditis with checkpoint inhibitor immunotherapy: Case report of late gadolinium enhancement on cardiac magnetic resonance with pathology correlate. Eur. Heart J. Case Rep. 2019, 3, yty149. [Google Scholar] [CrossRef]
- Tachihara, M.; Yamamoto, M.; Yumura, M.; Yoshizaki, A.; Kobayashi, K.; Nishimura, Y. Non-parallel anti-tumour effects of pembrolizumab: A case of cardial tamponade. Respirol. Case Rep. 2019, 7, e00404. [Google Scholar] [CrossRef]
- Yamasaki, M.; Daido, W.; Saito, N.; Funaishi, K.; Okada, T.; Kawamoto, K.; Matsumoto, Y.; Matsumoto, N.; Taniwaki, M.; Ohashi, N.; et al. Pericardial Effusion With Tamponade in Lung Cancer Patients During Treatment With Nivolumab: A Report of Two Cases. Front. Oncol. 2019, 9, 4. [Google Scholar] [CrossRef] [Green Version]
- Vittorio, A.; Sharma, R.; Siejka, D.; Bhattarai, K.; Hardikar, A. Recurrent Pericardial Effusion While Receiving Nivolumab for Metastatic Lung Adenocarcinoma: Case Report and Review of the Literature. Clin. Lung Cancer 2018, 19, e717–e720. [Google Scholar] [CrossRef] [PubMed]
- Monge, C.; Maeng, H.; Brofferio, A.; Apolo, A.B.; Sathya, B.; Arai, A.E.; Gulley, J.L.; Bilusic, M. Myocarditis in a patient treated with Nivolumab and PROSTVAC: A case report. J. Immunother. Cancer 2018, 6, 150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaheen, S.; Mirshahidi, H.; Nagaraj, G.; Hsueh, C.T. Conservative management of nivolumab-induced pericardial effusion: A case report and review of literature. Exp. Hematol. Oncol. 2018, 7, 11. [Google Scholar] [CrossRef] [PubMed]
- Inayat, F.; Masab, M.; Gupta, S.; Ullah, W. New drugs and new toxicities: Pembrolizumab-induced myocarditis. BMJ Case Rep. 2018, 2018, bcr2017223252. [Google Scholar] [CrossRef]
- Thibault, C.; Vano, Y.; Soulat, G.; Mirabel, M. Immune checkpoint inhibitors myocarditis: Not all cases are clinically patent. Eur. Heart J. 2018, 39, 3553. [Google Scholar] [CrossRef]
- Jain, V.; Mohebtash, M.; Rodrigo, M.E.; Ruiz, G.; Atkins, M.B.; Barac, A. Autoimmune myocarditis caused by immune checkpoint inhibitors treated with antithymocyte globulin. J. Immunother. 2018, 41, 332–335. [Google Scholar] [CrossRef]
- Ederhy, S.; Cautela, J.; Ancedy, Y.; Escudier, M.; Thuny, F.; Cohen, A. Takotsubo-Like Syndrome in Cancer Patients Treated With Immune Checkpoint Inhibitors. JACC Cardiovasc. Imaging. 2018, 11, 1187–1190. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, S.; Morimoto, R.; Okumura, T.; Yamashita, Y.; Haga, T.; Kuwayama, T.; Yokoi, T.; Hiraiwa, H.; Kondo, T.; Sugiura, Y.; et al. Late-onset fulminant myocarditis with immune checkpoint inhibitor nivolumab. Can. J. Cardiol. 2018, 34, 812.e1–812.e3. [Google Scholar] [CrossRef] [PubMed]
- Oristrell, G.; Baneras, J.; Ros, J.; Munoz, E. Cardiac tamponade and adrenal insufficiency due to pembrolizumab: A case report. Eur. Heart J. Case Rep. 2018, 2, yty038. [Google Scholar] [CrossRef] [PubMed]
- Frigeri, M.; Meyer, P.; Banfi, C.; Giraud, R.; Hachulla, A.L.; Spoerl, D.; Friedlaender, A.; Pugliesi-Rinaldi, A.; Dietrich, P.Y. Immune checkpoint inhibitor-associated myocarditis: A new challenge for cardiologists. Can. J. Cardiol. 2018, 34, 92.e1–92.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tajmir-Riahi, A.; Bergmann, T.; Schmid, M.; Agaimy, A.; Schuler, G.; Heinzerling, L. Life-threatening autoimmune cardiomyopathy reproducibly induced in a patient by checkpoint inhibitor therapy. J. Immunother. 2018, 41, 35–38. [Google Scholar] [CrossRef]
- Katsume, Y.; Isawa, T.; Toi, Y.; Fukuda, R.; Kondo, Y.; Sugawara, S.; Ootomo, T. Complete atrioventricular block associated with pembrolizumab-induced acute myocarditis: The need for close cardiac monitoring. Intern. Med. 2018, 57, 3157–3162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Q.; Huang, D.S.; Zhang, L.W.; Li, Y.Q.; Wang, H.W.; Liu, H.B. Fatal myocarditis and rhabdomyolysis induced by nivolumab during the treatment of type B3 thymoma. Clin. Toxicol. 2018, 56, 667–671. [Google Scholar] [CrossRef]
- Matson, D.R.; Accola, M.A.; Rehrauer, W.M.; Corliss, R.F. Fatal Myocarditis Following Treatment with the PD-1 Inhibitor Nivolumab. J. Forensic. Sci. 2018, 63, 954–957. [Google Scholar] [CrossRef]
- Norwood, T.G.; Westbrook, B.C.; Johnson, D.B.; Litovsky, S.H.; Terry, N.L.; McKee, S.B.; Gertler, A.S.; Moslehi, J.J.; Conry, R.M. Smoldering myocarditis following immune checkpoint blockade. J. Immunother. Cancer 2017, 5, 91. [Google Scholar] [CrossRef]
- Arangalage, D.; Delyon, J.; Lermuzeaux, M.; Ekpe, K.; Ederhy, S.; Pages, C.; Lebbé, C. Survival after fulminant myocarditis induced by immune-checkpoint inhibitors. Ann. Intern. Med. 2017, 167, 683–684. [Google Scholar] [CrossRef]
- Penel, N.; Cordoba, A.; Mathoulin-Pelissier, S. Lessons from three phase III trials assessing neoadjuvant treatment in sarcoma patients. Ann. Oncol. 2017, 28, 2891–2893. [Google Scholar] [CrossRef]
- Zarogoulidis, P.; Chinelis, P.; Athanasiadou, A.; Tsiouda, T.; Trakada, G.; Kallianos, A.; Veletza, L.; Hatzibougias, D.; Mihalopoulou, E.; Goupou, E.; et al. Possible adverse effects of immunotherapy in non-small cell lung cancer; Treatment and follow-up of three cases. Respir. Med. Case Rep. 2017, 22, 101–105. [Google Scholar] [CrossRef]
- Reddy, N.; Moudgil, R.; Lopez-Mattei, J.C.; Karimzad, K.; Mouhayar, E.N.; Somaiah, N.; Conley, A.P.; Patel, S.; Giza, D.E.; Iliescu, C. Progressive and Reversible Conduction Disease With Checkpoint Inhibitors. Can. J. Cardiol. 2017, 33, 1335.e13–1335.e15. [Google Scholar] [CrossRef] [PubMed]
- Kimura, H.; Tounai, Y.; Nagato, K.; Morimoto, J.I.; Tounai, Y. A case of heart failure after treatment with anti-PD-1 antibody followed by adoptive transfer of cytokine-activated killer cells in a recurrent lung cancer patient. J. Thorac. Oncol. 2017, 12, e128–e130. [Google Scholar] [CrossRef] [PubMed]
- Behling, J.; Kaes, J.; Munzel, T.; Grabbe, S.; Loquai, C. New-onset third-degree atrioventricular block because of autoimmune-induced myositis under treatment with anti-programmed cell death-1 (nivolumab) for metastatic melanoma. Melanoma Res. 2017, 27, 155–158. [Google Scholar] [CrossRef]
- Chu, Y.C.; Fang, K.C.; Chen, H.C.; Yeh, Y.C.; Tseng, C.E.; Chou, T.Y.; Lai, C.L. Pericardial tamponade caused by a hypersensitivity response to tuberculosis reactivation after anti-PD-1 treatment in a patient with advanced pulmonary adenocarcinoma. J. Thorac. Oncol. 2017, 12, e111–e114. [Google Scholar] [CrossRef]
- Kushnir, I.; Wolf, I. Nivolumab-induced pericardial tamponade: A case report and discussion. Cardiology 2017, 136, 49–51. [Google Scholar] [CrossRef]
- Kolla, B.C.; Patel, M.R. Recurrent pleural effusions and cardiac tamponade as possible manifestations of pseudoprogression associated with nivolumab therapy—a report of two cases. J. Immunother. Cancer 2016, 4, 80. [Google Scholar] [CrossRef] [Green Version]
- Roth, M.E.; Muluneh, B.; Jensen, B.C.; Madamanchi, C.; Lee, C.B. Left ventricular dysfunction after treatment with ipilimumab for metastatic Melanoma. Am. J. Ther. 2016, 23, e1925–e1928. [Google Scholar] [CrossRef] [PubMed]
- Mehta, A.; Gupta, A.; Hannallah, F.; Koshy, T.; Reimold, S. Myocarditis as an immune-relatedadverse event with ipilimumab/nivolumab combination therapy for meta-static melanoma. Melanoma Res. 2016, 26, 319–320. [Google Scholar] [CrossRef] [PubMed]
- Zimmer, L.; Goldinger, S.M.; Hofmann, L.; Loquai, C.; Ugurel, S.; Thomas, I.; Schmidgen, M.I.; Gutzmer, R.; Utikal, J.S.; Göppner, D.; et al. Neurological, respiratory, musculoskeletal, cardiac and ocular side-effects of anti-PD-1 therapy. Eur. J. Cancer 2016, 60, 210–225. [Google Scholar] [CrossRef] [PubMed]
- Tadokoro, T.; Keshino, E.; Makiyama, A.; Sasaguri, T.; Ohshima, K.; Katano, H.; Mohri, M. Acute lymphocytic myocarditis with anti-PD-1 antibody nivolumab. Circ. Heart Fail. 2016, 9, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nesfeder, J.; Elsensohn, A.N.; Thind, M.; Lennon, J.; Domsky, S. Pericardial effusion with tamponade physiology induced by nivolumab. Int. J. Cardiol. 2016, 222, 613–614. [Google Scholar] [CrossRef] [PubMed]
- Semper, H.; Muehlberg, F.; Schulz-Menger, J.; Allewelt, M.; Grohé, C. Drug-induced myocarditis after nivolumab treatment in a patient with PDL1-negative squamous cell carcinoma of the lung. Lung Cancer. 2016, 99, 117–119. [Google Scholar] [CrossRef]
- Gibson, R.; Delaune, J.; Szady, A.; Markham, M. Suspected autoimmune myocarditis and cardiac conduction abnormalities with nivolumab therapy for non-small cell lung cancer. BMJ Case Rep. 2016, 2016, bcr2016216228. [Google Scholar] [CrossRef] [PubMed]
- Geisler, B.P.; Raad, R.A.; Esaian, D.; Sharon, E.; Schwartz, D.R. Apical ballooning and cardiomyopathy in a melanoma patient treated with ipilimumab: A case of takotsubo-like syndrome. J. Immunother. Cancer 2015, 3, 4. [Google Scholar] [CrossRef] [Green Version]
- Yun, S.; Vincelette, N.D.; Mansour, I.; Hariri, D.; Motamed, S. Late onset ipilimumab-induced pericarditis and pericardial effusion: A rare but life threatening complication. Case Rep. Oncol. Med. 2015, 2015, 794842. [Google Scholar] [CrossRef]


| Type of Cardiotoxicity | Median Onset | Most Common Symptoms | Diagnosis | Treatment | Sources |
|---|---|---|---|---|---|
| Myocarditis | 65 days | Shortness of breath, palpitations, edema, and fatigue | NT-proBNP, troponin I, endomyocardial biopsy, and CMR | High-dose corticosteroids | [15,16,17,18,19,20,21] |
| Pericarditis | 30 days | Shortness of breath, chest pain | ECG changes, CMR, pericardial effusion, and fluid analysis | Pericardiocentesis, NSAIDs, colchicine, and high-dose corticosteroids | [7,16,22,23,24,25] |
| Takotsubo cardiomyopathy | 15 weeks to 8 months | Unknown | ECG changes, troponin and NT-proBNP | High-dose corticosteroids | [17,23,26] |
| Arrhythmias and conduction disorders | Unknown | Unknown | ECG changes | High-dose corticosteroids, supportive | [17,18,22] |
| Myocardial infarction | Unknown | Chest pain and shortness of breath | ECG changes, troponin, and others | Cardiac catheterization, supportive | [17] |
| Treatment | Ipilimumab | Nivolumab | Pembrolizumab | Ipilimumab + Nivolumab | Durvalumab | Atezolizumab | Unspecified |
|---|---|---|---|---|---|---|---|
| Number of Cases | 18 | 43 | 20 | 17 | 3 | 1 | 5 |
| Average Weeks until Presentation | 18 | 17 | 9 | 10 | 11 | 1 | -- |
| Median Weeks until Presentation | 10 | 9 | 7 | 6 | 8 | 1 | -- |
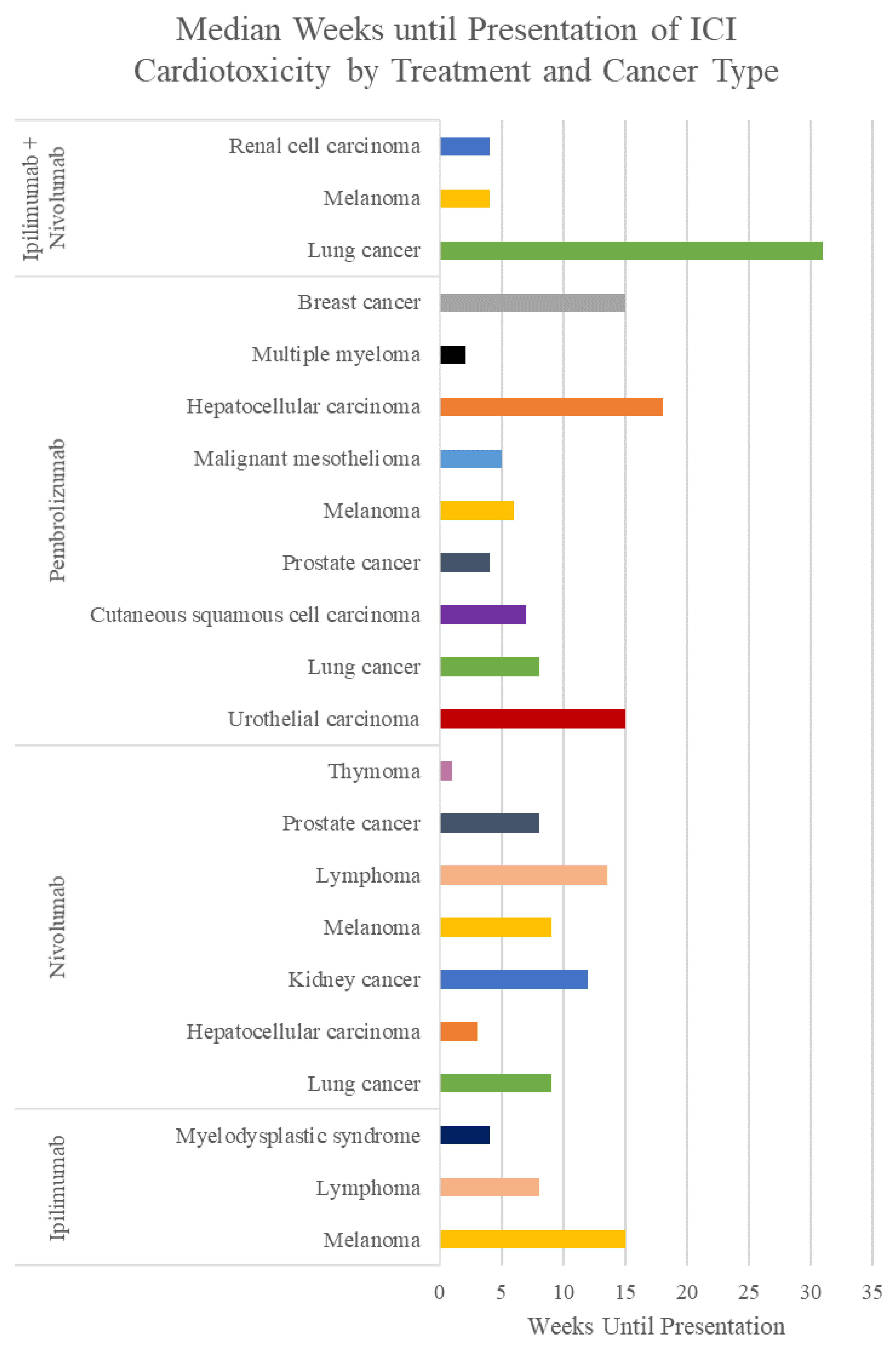
| Treatment | Type of Cancer Treated | Number of Cases | Average Weeks until Presentation | Median Weeks until Presentation |
|---|---|---|---|---|
| Ipilimumab | Melanoma | 13 | 21 | 15 |
| Lymphoma | 1 | 8 | 8 | |
| MDS | 2 | 4 | 4 | |
| Nivolumab | Lung Cancer | 30 | 20 | 9 |
| HCC | 1 | 3 | 3 | |
| Kidney Cancer | 1 | 12 | 12 | |
| Melanoma | 7 | 12 | 9 | |
| Lymphoma | 2 | 14 | 14 | |
| Prostate Cancer | 1 | 8 | 8 | |
| Thymoma | 1 | 1 | 1 | |
| Pembrolizumab | Urothelial Carcinoma | 1 | 15 | 15 |
| Lung Cancer | 7 | 7 | 8 | |
| Cutaneous SCC | 1 | 7 | 7 | |
| Prostate Cancer | 1 | 4 | 4 | |
| Melanoma | 6 | 9 | 6 | |
| Malignant Mesothelioma | 1 | 5 | 5 | |
| HCC | 1 | 18 | 18 | |
| Multiple Myeloma | 1 | 2 | 2 | |
| Breast Cancer | 1 | 15 | 15 | |
| Ipilimumab + Nivolumab | Lung Cancer | 2 | 31 | 31 |
| Melanoma | 13 | 8 | 4 | |
| RCC | 2 | 4 | 4 |
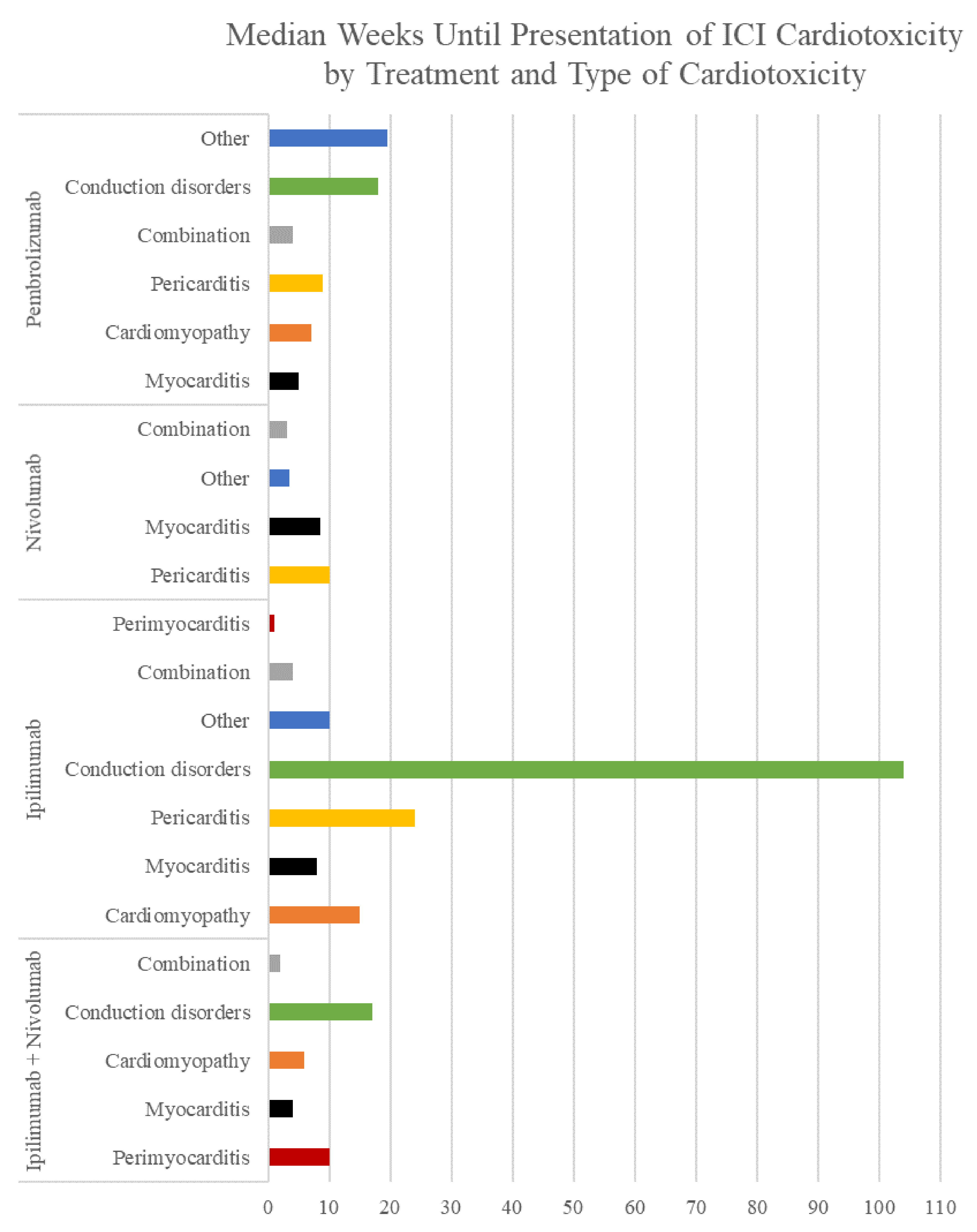
| Treatment | Type of Cardiotoxicity | Number of Cases | Average Weeks until Presentation | Median Weeks until Presentation |
|---|---|---|---|---|
| Ipilimumab + Nivolumab | Perimyocarditis | 1 | 10 | 10 |
| Myocarditis | 11 | 10 | 4 | |
| Cardiomyopathy | 3 | 13 | 6 | |
| Conduction Disorders | 1 | 17 | 17 | |
| Combination | 1 | 2 | 2 | |
| Ipilimumab | Perimyocarditis | 1 | 1 | 1 |
| Myocarditis | 7 | 12 | 8 | |
| Cardiomyopathy | 3 | 15 | 15 | |
| Conduction Disorders | 1 | 104 | 104 | |
| Pericarditis | 3 | 23 | 24 | |
| Combination | 1 | 4 | 4 | |
| Other | 1 | 10 | 10 | |
| Nivolumab | Myocarditis | 10 | 11 | 9 |
| Pericarditis | 21 | 22 | 10 | |
| Combination | 6 | 4 | 3 | |
| Other | 6 | 10 | 4 | |
| Pembrolizumab | Myocarditis | 7 | 6 | 5 |
| Cardiomyopathy | 1 | 7 | 7 | |
| Conduction Disorders | 1 | 18 | 18 | |
| Pericarditis | 5 | 10 | 9 | |
| Combination | 4 | 5 | 4 | |
| Other | 2 | 20 | 20 |
| Drug | First Approved | Cancers Approved for Treatment | Most Common Side Effects |
|---|---|---|---|
| Ipilimumab | 2011 | Melanoma, RCC, CRC, HCC, and NSCLC | Fatigue, diarrhea, pruritis, rash, and colitis |
| Pembrolizumab | 2014 | Melanoma, lung cancer, SCC, lymphomas, urothelial carcinoma, cancers high in MSI, MMR-deficient cancers, gastric cancers, esophageal cancers, cervical cancers, HCC, Merkel cell cancer, RCC, endometrial carcinoma, tumor mutational burden-high cancer, and triple-negative breast cancer | Fatigue, musculoskeletal pain, decreased appetite, diarrhea, rash, fever, cough, constipation, nausea, abdominal pain, and pruritis |
| Nivolumab | 2014 | Melanoma, NSCLC, malignant pleural mesothelioma, RCC, classic Hodgkin lymphoma, HNSCC, urothelial carcinoma, CRC, HCC, and esophageal squamous cell carcinoma | Fatigue, rash, pruritis, and diarrhea |
| Atezolizumab | 2016 | Urothelial carcinoma, NSCLC, triple-negative breast cancer, SCLC, HCC, and melanoma | Fatigue, nausea, vomiting, cough, dyspnea, decreased appetite, alopecia, constipation or diarrhea, headache, and rash |
| Durvalumab | 2017 | Urothelial carcinoma and NSCLC | Fatigue, constipation, UTIs, edema, pneumonitis, dyspnea, rash, cough, and nausea |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shalata, W.; Abu-salman, A.; Steckbeck, R.; Mathew Jacob, B.; Massalha, I.; Yakobson, A. Cardiac Toxicity Associated with Immune Checkpoint Inhibitors: A Systematic Review. Cancers 2021, 13, 5218. https://doi.org/10.3390/cancers13205218
Shalata W, Abu-salman A, Steckbeck R, Mathew Jacob B, Massalha I, Yakobson A. Cardiac Toxicity Associated with Immune Checkpoint Inhibitors: A Systematic Review. Cancers. 2021; 13(20):5218. https://doi.org/10.3390/cancers13205218
Chicago/Turabian StyleShalata, Walid, Amjad Abu-salman, Rachel Steckbeck, Binil Mathew Jacob, Ismaell Massalha, and Alexander Yakobson. 2021. "Cardiac Toxicity Associated with Immune Checkpoint Inhibitors: A Systematic Review" Cancers 13, no. 20: 5218. https://doi.org/10.3390/cancers13205218
APA StyleShalata, W., Abu-salman, A., Steckbeck, R., Mathew Jacob, B., Massalha, I., & Yakobson, A. (2021). Cardiac Toxicity Associated with Immune Checkpoint Inhibitors: A Systematic Review. Cancers, 13(20), 5218. https://doi.org/10.3390/cancers13205218