
Basosquamous Carcinoma: A Commentary


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Background and Definition
3.2. Epidemiology
3.3. Clinical and Demographic Characteristics
3.4. Diagnosis of Basosquamous Carcinoma
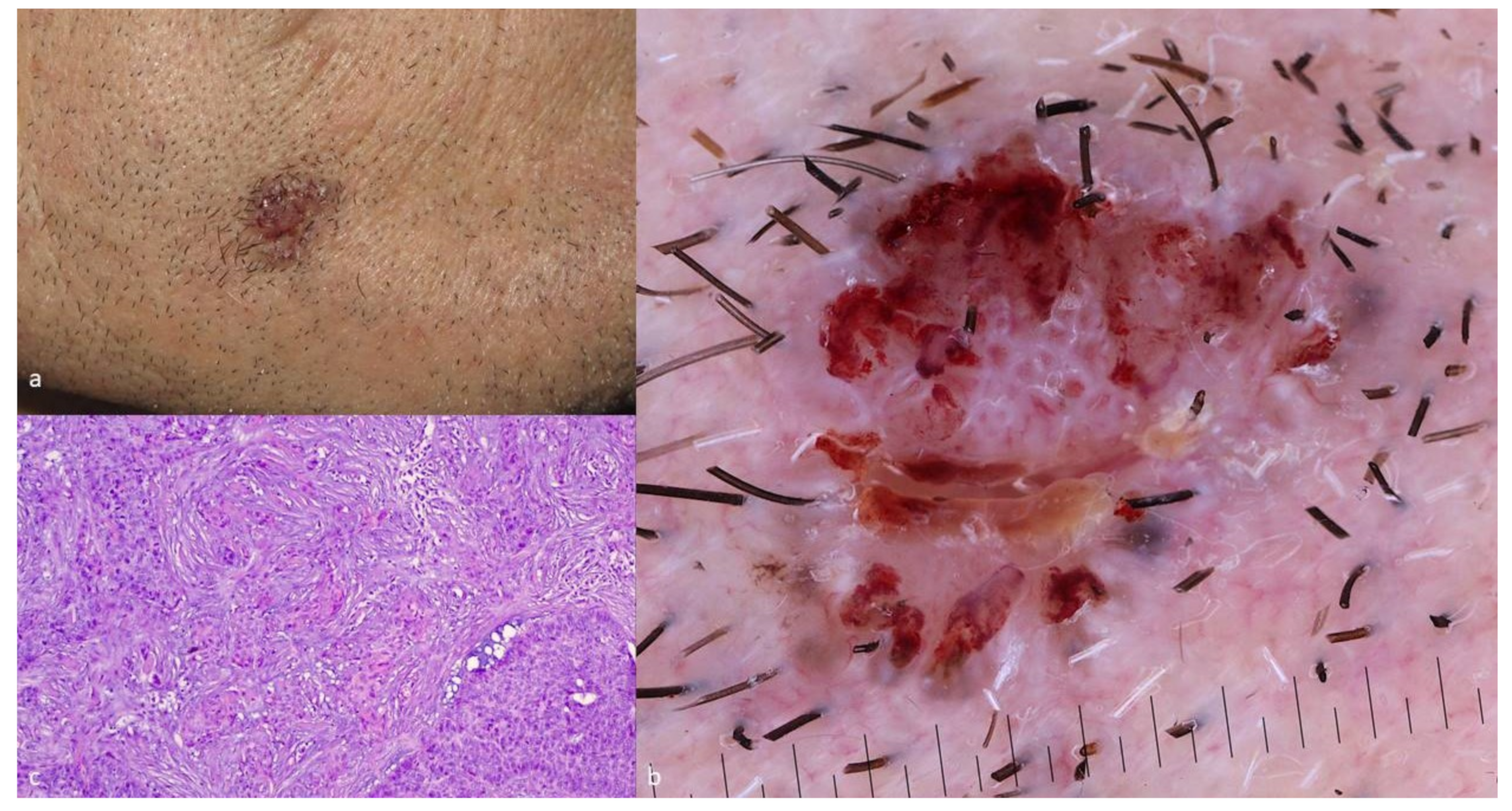
3.4.1. Dermoscopy of BSC
3.4.2. Histopathologic Features of BSC
3.4.3. Immunohistologic Features of BSC
3.5. Genetics and Pathogenesis
3.6. Biologic Behavior and Prognosis
3.7. Therapeutic Options and Management of BSC
3.7.1. Wide Surgical Excision
3.7.2. Mohs’ Micrographic Surgery (MMS)
3.7.3. Sentinel Lymph Node Biopsy (SLNB)
3.7.4. Radiotherapy–Chemotherapy
3.7.5. New Emerging Therapies
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- De Stefano, A.; Dispenza, F.; Petrucci, A.G.; Citraro, L.; Croce, A. Features of biopsy in diagnosis of metatypical basal cell carcinoma (basosquamous carcinoma) of head and neck. Otolaryngol. Pol. 2012, 66, 419–423. [Google Scholar] [CrossRef]
- Tan, C.Z.; Rieger, K.E.; Sarin, K.Y. Basosquamous carcinoma: Controversy, advances, and future directions. Dermatol. Surg. 2017, 43, 23–31. [Google Scholar] [CrossRef]
- MacCormac, H. The relation of rodent ulcer to squamous cell carcinoma of the skin. Arch. Middlesex. Hosp. 1910, 19, 172–183. [Google Scholar] [CrossRef]
- Hamilton, M. Basal squamous cell epithelioma. Arch. Dermatol. Syph. 1928, 18, 50–73. [Google Scholar] [CrossRef]
- Garcia, C.; Poletti, E.; Crowson, A.N. Basosquamous carcinoma. J. Am. Acad. Dermatol. 2009, 60, 137–143. [Google Scholar] [CrossRef]
- Bowman, P.H.; Ratz, J.L.; Knoepp, T.G.; Barnes, C.J.; Finlay, R.E. Basosquamous carcinoma. Dermatol. Surg. 2003, 29, 830–832. [Google Scholar] [CrossRef] [PubMed]
- Ciążyńska, M.; Sławińska, M.; Kamińska-Winciorek, G.; Lange, D.; Lewandowski, B.; Reich, A.; Pabianek, M.; Szczepaniak, K.; Hankiewicz, A.; Ułańska, M.; et al. Clinical and epidemiological analysis of basosquamous carcinoma: Results of the multicenter study. Sci. Rep. 2020, 10, 1–8. [Google Scholar] [CrossRef]
- Burston, J.; Clay, R.D. THE PROBLEMS OF HISTOLOGICAL DIAGNOSIS IN BASO-SQUAMOUS CELL CARCINOMA OF THE SKIN. J. Clin. Pathol. 1959, 12, 73–79. [Google Scholar] [CrossRef] [Green Version]
- de Faria, J. Basal cell carcinoma of the skin with areas of squamous cell carcinoma: A basosquamous cell carcinoma? J. Clin. Pathol. 1985, 38, 1273–1277. [Google Scholar] [CrossRef] [Green Version]
- Tarallo, M.; Cigna, E.; Frati, R.; Delfino, S.; Innocenzi, D.; Fama, U.; Corbianco, A.; Scuderi, N. Metatypical basal cell carcinoma: A clinical review. J. Exp. Clin. Cancer Res. 2008, 27, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shukla, S.; Khachemoune, A. Reappraising basosquamous carcinoma: A summary of histologic features, diagnosis, and treatment. Arch. Dermatol. Res. 2020, 312, 605–609. [Google Scholar] [CrossRef]
- Oldbury, J.W.; Wain, R.; Abas, S.; Dobson, C.M.; Iyer, S.S. Basosquamous Carcinoma: A Single Centre Clinicopathological Evaluation and Proposal of an Evidence-Based Protocol. J. Ski. Cancer 2018, 2018, 1–7. [Google Scholar] [CrossRef]
- LeBoit, P.E.; International Agency for Research on Cancer; World Health Organization; International Academy of Pathology; European Organization for Research on Treatment of Cancer; UniversitätsSpital Zürich. Pathology and Genetics of Skin Tumours; IARC Press: Lyon, France, 2006. [Google Scholar]
- Wermker, K.; Roknic, N.; Goessling, K.; Klein, M.; Schulze, H.-J.; Hallermann, C. Basosquamous Carcinoma of the Head and Neck: Clinical and Histologic Characteristics and Their Impact on Disease Progression. Neoplasia 2015, 17, 301–305. [Google Scholar] [CrossRef] [Green Version]
- Gualdi, G.; Soglia, S.; Fusano, M.; Monari, P.; Giuliani, F.; Porreca, A.; Di Nicola, M.; Calzavara-Pinton, P.; Amerio, P. Characterization of Basosquamous Carcinoma. A distinct type of keratinizing tumour. Acta Derm. Venereol. 2021, 101, adv00353. [Google Scholar] [CrossRef] [PubMed]
- Schuller, D.E.; Berg, J.W.; Sherman, G.; Krause, C.J. Cutaneous Basosquamous Carcinoma of the Head and Neck: A Comparative Analysis. Otolaryngol. Neck Surg. 1979, 87, 420–427. [Google Scholar] [CrossRef]
- Martin, R.C.; Edwards, M.J.; Cawte, T.G.; Sewell, C.L.; McMasters, K.M. Basosquamous carcinoma: Analysis of prognostic factors influencing recurrence. Cancer 2000, 88, 1365–1369. [Google Scholar] [CrossRef]
- Volkenstein, S.; Wohlschlaeger, J.; Liebau, J.; Arens, A.; Lehnerdt, G.; Jahnke, K.; Neumann, A. Basosquamous carcinoma-A rare but aggressive skin malignancy. J. Plast. Reconstr. Aesthetic Surg. 2010, 63, e304–e306. [Google Scholar] [CrossRef] [PubMed]
- Borel, D.M. Cutaneous basosquamous carcinoma. Review of the literature and report of 35 cases. Arch. Pathol. 1973, 95, 293–297. [Google Scholar] [PubMed]
- Mougel, F.; Kanitakis, J.; Faure, M.; Euvrard, S. Basosquamous cell carcinoma in organ transplant patients: A clinicopathologic study. J. Am. Acad. Dermatol. 2012, 66, e151–e157. [Google Scholar] [CrossRef]
- Betti, R.; Crosti, C.; Ghiozzi, S.; Cerri, A.; Moneghini, L.; Menni, S. Basosquamous cell carcinoma: A survey of 76 patients and a comparative analysis of basal cell carcinomas and squamous cell carcinomas. Eur. J. Dermatol. EJD 2013, 23, 83–86. [Google Scholar] [CrossRef]
- Giacomel, J.; Lallas, A.; Argenziano, G.; Reggiani, C.; Piana, S.; Apalla, Z.; Ferrara, G.; Moscarella, E.; Longo, C.; Zalaudek, I. Dermoscopy of basosquamous carcinoma. Br. J. Dermatol. 2013, 169, 358–364. [Google Scholar] [CrossRef] [PubMed]
- Akay, B.N.; Saral, S.; Heper, A.O.; Erdem, C.; Rosendahl, C. Basosquamous carcinoma: Dermoscopic clues to diagnosis. J. Dermatol. 2016, 44, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Leibovitch, I.; Huilgol, S.C.; Selva, D.; Richards, S.; Paver, R. Basosquamous carcinoma: Treatment with Mohs micrographic surgery. Cancer 2005, 104, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Costantino, D.; Lowe, L.; Brown, D.L. Basosquamous carcinoma—an under-recognized, high-risk cutaneous neoplasm: Case study and review of the literature. J. Plast. Reconstr. Aesthetic Surg. 2006, 59, 424–428. [Google Scholar] [CrossRef]
- Anand, R.L.; Collins, D.; Chapman, A. Basosquamous carcinoma: Appearance and reality. Oxf. Med. Case Rep. 2017, 2017, omw095. [Google Scholar] [CrossRef] [Green Version]
- Jankovic, I.; Kovacevic, P.; Visnjic, M.; Jankovic, D.; Binic, I.; Jankovic, A.; Ilic, I. Application of sentinel lymph node biopsy in cutaneous basosquamous carcinoma. Ann. Dermatol. 2011, 23 Suppl. 1, S123–S126. [Google Scholar] [CrossRef] [Green Version]
- Malloney, M.L. What is basosquamous carcinoma? Dermatol. Surg. 2000, 26, 505–506. [Google Scholar] [CrossRef]
- Jones, M.S.; Helm, K.F.; Maloney, M.E. The Immunohistochemical Characteristics of the Basosquamous Cell Carcinoma. Dermatol. Surg. 1997, 23, 181–184. [Google Scholar] [CrossRef]
- Chiang, A.; Tan, C.Z.; Kuonen, F.; Hodgkinson, L.M.; Chiang, F.; Cho, R.J.; South, A.P.; Tang, J.Y.; Chang, A.L.S.; Rieger, K.E. Genetic mutations underlying phenotypic plasticity in basosquamous carcinoma. J. Investig. Dermatol. 2019, 139, 2263–2271.e5. [Google Scholar] [CrossRef]
- Apalla, Z.; Papageorgiou, C.; Lallas, A.; Sotiriou, E.; Lazaridou, E.; Vakirlis, E.; Kyrgidis, A.; Ioannides, D. Spotlight on vismodegib in the treatment of basal cell carcinoma: An evidence-based review of its place in therapy. Clin. Cosmet. Investig. Dermatol. 2017, ume 10, 171–177. [Google Scholar] [CrossRef] [Green Version]
- Marzuka, A.G.; Book, S.E. Basal Cell Carcinoma: Pathogenesis, Epidemiology, Clinical Features, Diagnosis, Histopathology, and Management. Yale J. Boil. Med. 2015, 88, 167–179. [Google Scholar]
- Bonilla, X.; Parmentier, L.; King, B.; Bezrukov, F.; Kaya, G.; Zoete, V.; Seplyarskiy, V.B.; Sharpe, H.J.; McKee, T.; Letourneau, A.; et al. Genomic analysis identifies new drivers and progression pathways in skin basal cell carcinoma. Nat. Genet. 2016, 48, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Jayaraman, S.S.; Rayhan, D.J.; Hazany, S.; Kolodney, M.S. Mutational landscape of basal cell carcinomas by whole-exome sequencing. J. Invest. Dermatol. 2014, 134, 213–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cammareri, P.; Rose, A.M.; Vincent, D.F.; Wang, J.; Nagano, A.; Libertini, S.; Ridgway, R.A.; Athineos, D.; Coates, P.J.; McHugh, A.; et al. Inactivation of TGFbeta receptors in stem cells drives cutaneous squamous cell carcinoma. Nat. Commun. 2016, 7, 12493. [Google Scholar] [CrossRef]
- South, A.P.; Purdie, K.J.; Watt, S.A.; Haldenby, S.; Breems, N.Y.D.; Dimon, M.; Arron, S.; Kluk, M.J.; Aster, J.C.; McHugh, A.; et al. NOTCH1 Mutations Occur Early during Cutaneous Squamous Cell Carcinogenesis. J. Investig. Dermatol. 2014, 134, 2630–2638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pickering, C.R.; Zhou, J.H.; Lee, J.J.; Drummond, J.A.; Peng, S.A.; Saade, R.E.; Tsai, K.Y.; Curry, J.L.; Tetzlaff, M.T.; Lai, S.Y.; et al. Mutational Landscape of Aggressive Cutaneous Squamous Cell Carcinoma. Clin. Cancer Res. 2014, 20, 6582–6592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwaederle, M.; Elkin, S.K.; Tomson, B.N.; Carter, J.L.; Kurzrock, R. Squamousness: Next-generation sequencing reveals shared molecular features across squamous tumor types. Cell Cycle 2015, 14, 2355–2361. [Google Scholar] [CrossRef] [PubMed]
- Tarapore, E.; Atwood, S.X. Defining the genetics of Basoaquamous Carcinoma. J. Invest. Dermatol. 2019, 139, 2258–2260. [Google Scholar] [CrossRef] [PubMed]
- Zhu, G.A.; Danial, C.; Liu, A.; Li, S.; Chang, A.L.S. Overall and progression-free survival in metastatic basosquamous cancer: A case series. J. Am. Acad. Dermatol. 2014, 70, 1145–1146. [Google Scholar] [CrossRef]
- Alam, M.; Desai, S.; Nodzenski, M.; Dubina, M.; Kim, N.; Martini, M.; Fife, D.; Reid, D.; Pirigyi, M.; Poon, E.; et al. Active ascertainment of recurrence rate after treatment of primary basal cell carcinoma (BCC). J. Am. Acad. Dermatol. 2015, 73, 323–325. [Google Scholar] [CrossRef] [Green Version]
- Belkin, D.; Carucci, J.A. Mohs Surgery for Squamous Cell Carcinoma. Dermatol. Clin. 2011, 29, 161–174. [Google Scholar] [CrossRef] [PubMed]
- Kececi, Y.; Argon, A.; Kebat, T.; Sir, E.; Gungor, M.; Vardar, E. Basosquamous carcinoma: Is it an aggressive tumor? J. Plas. Surg. Hand Surg. 2015, 49, 107–111. [Google Scholar] [CrossRef]
- Skaria, A. Recurrence of Basosquamous Carcinoma after Mohs Micrographic Surgery. Dermatology 2010, 221, 352–355. [Google Scholar] [CrossRef]
- Allen, K.J.; Cappel, M.A.; Killian, J.M.; Brewer, J.D. Basosquamous carcinoma and metatypical basal cell carcinoma: A review of treatment with Mohs micrographic surgery. Int. J. Dermatol. 2014, 53, 1395–1403. [Google Scholar] [CrossRef]
- Kagakia, D.; Zapandioti, P.; Tryspiannis, G.; Grekou, A.; Tsoutsos, D. Sentinel lymph node metastasis in primary cutaneous basosquamous carcinoma. A cross-sectional study. J. Surg. Oncol. 2018, 117, 1752–1758. [Google Scholar] [CrossRef] [PubMed]
- Deganello, A.; Gitti, G.; Struijs, B.; Paiar, F.; Gallo, O. Palliative combined treatment for unresectable cutaneous basosquamous cell carcinoma of the head and neck. Acta Otorhinolaryngol. Ital. 2013, 33, 353–356. [Google Scholar] [PubMed]
- Farmer, E.R.; Helwig, E.B. Metastatic basal cell carcinoma: A clinicopathologic study of seventeen cases. Cancer 1980, 46, 748–757. [Google Scholar] [CrossRef]
- Mohan, S.V.; Chang, J.; Li, S.; Henry, S.; Wood, D.J.; Chang, A.L.S. Increased risk of cutaneous squamous cell carcinoma after vismodegib therapy for basal cell carcinoma. JAMA Dermatol. 2016, 152, 527–532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puig, S.; Sampogna, F.; Tejera-Vaquerizo, A. Study on the risk of cutaneous squamous cell carcinoma after vismodegib therapy for basal cell carcinoma: Not a case-control study. JAMA Dermatol. 2016, 152, 1172–1173. [Google Scholar] [CrossRef] [PubMed]
- Bhutani, T.; Abrouk, M.; Sima, C.S.; Sadetsky, N.; Hou, J.; Caro, I.; Chren, M.-M.; Arron, S. Risk of cutaneous squamous cell carcinoma after treatment of basal cell carcinoma with vismodegib. J. Am. Acad. Dermatol. 2017, 77, 713–718. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, A.A.; Aldahan, A.S.; Hughes, O.B.; Shah, V.V.; Strasswimmer, J. Hedgehog pathway inhibitor therapy for locally advanced and metastatic basal cell carcinoma: A systematic review and pooled analysis of interventional studies. JAMA Dermatol. 2016, 152, 816–824. [Google Scholar] [CrossRef] [Green Version]
- McGrane, J.; Carswell, S.; Talbot, T. Metastatic spinal cord compression from basal cell carcinoma of the skin treated with surgical decompression and vismodegib: Case report and review of Hedgehog signalling pathway inhibition in advanced basal cell carcinoma. Clin. Exp. Dermatol. 2017, 42, 80–83. [Google Scholar] [CrossRef] [PubMed]
- Apalla, Z.; Giakouvis, V.; Gavros, Z.; Lazaridou, E.; Sotiriou, E.; Bobos, M.; Vakirlis, E.; Ioannides, D.; Lallas, A. Complete response of locally advanced basosquamous carcinoma to vismodegib in two patients. Eur. J. Dermatol. EJD 2019, 29, 102–104. [Google Scholar] [PubMed]
- Sahuquillo-Torralba, A.; Llavador-Ros, M.; Caballero-Daroqui, J.; Botella-Estrada, R. Complete response of a locally advanced basosquamous carcinoma with vismodegib treatment. Indian J. Dermatol. Venereol. Leprol. 2019, 85, 549–552. [Google Scholar] [CrossRef]
- Shalhout, S.Z.; Emerick, K.S.; Kaufman, H.L.; Miller, D.M. Immunotherapy for Non-melanoma Skin Cancer. Curr. Oncol. Rep. 2021, 23, 1–10. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| BCCs | SCCs | BSCs |
|---|---|---|
| PTCH | HRAS | PTCH |
| SMO | TGFBR1 | SMO |
| PTEN | TGFBR2 | MYCN |
| MYCN | NOTCH1 | PPP6C |
| PPP6C | NOTCH2 | GRIN2A |
| GRIN2A | CASP8 | CSMD3 |
| GLI1 | CDKN2A | DCC |
| CSMD3 | NOTCH3 | PREX2 |
| DCC | KRAS | APC |
| PREX2 | NRAS | PTEN |
| APC | PDK1 | PIK3CA |
| BAP1 | ARIDIA | |
| AJUBA | ||
| KMT2D | ||
| CDH1 |
| Source | Study Design | Number of Patients | Results |
|---|---|---|---|
| McGrane J. et al. [53] | Case report | 1 | Marked improvement, stable after 28 months |
| Apalla Z. et al. [54] | Case series | 2 | Complete clinical response with long-term follow up (12 and 18 months, respectively |
| Sahuquillo-Torralba A. et al. [55] | Case report | 1 | Complete response after 7 months |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fotiadou, C.; Apalla, Z.; Lazaridou, E. Basosquamous Carcinoma: A Commentary. Cancers 2021, 13, 6146. https://doi.org/10.3390/cancers13236146
Fotiadou C, Apalla Z, Lazaridou E. Basosquamous Carcinoma: A Commentary. Cancers. 2021; 13(23):6146. https://doi.org/10.3390/cancers13236146
Chicago/Turabian StyleFotiadou, Christina, Zoe Apalla, and Elizabeth Lazaridou. 2021. "Basosquamous Carcinoma: A Commentary" Cancers 13, no. 23: 6146. https://doi.org/10.3390/cancers13236146
APA StyleFotiadou, C., Apalla, Z., & Lazaridou, E. (2021). Basosquamous Carcinoma: A Commentary. Cancers, 13(23), 6146. https://doi.org/10.3390/cancers13236146