
Prediction of Clinically Significant Cancer Using Radiomics Features of Pre-Biopsy of Multiparametric MRI in Men Suspected of Prostate Cancer

 , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Method
2.1. Target Population
2.2. MultiParametric MRI (mpMRI) Image Acquisition
2.3. Radiomic Feature Analysis
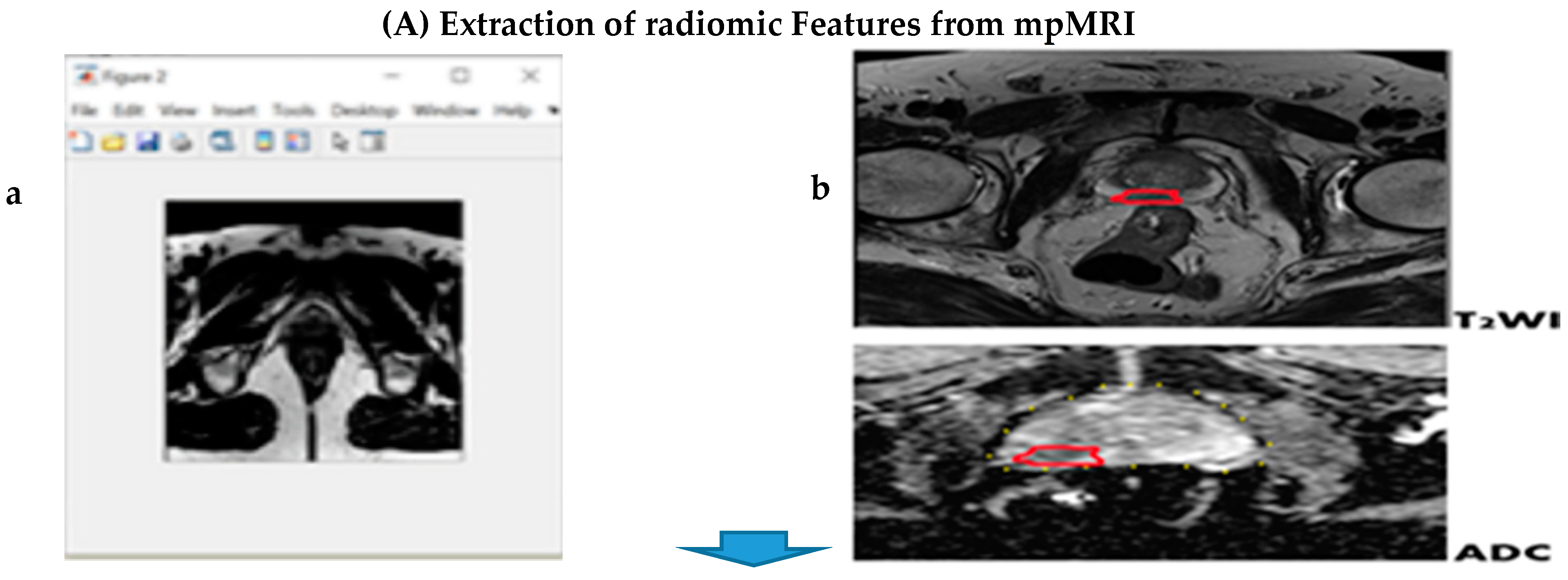
2.4. Segmentation
2.5. Feature Extraction and Selection
2.6. Histological Gleason Score
2.7. Statistical Analysis
3. Results
3.1. Patients Summary
3.2. Correlation Analysis
3.3. Significant Features
3.4. Predictive Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [Green Version]
- Hoffman, R.M.; Gilliland, F.D.; Adams-Cameron, M.; Hunt, W.C.; Key, C.R. Prostate-specific antigen testing accuracy in community practice. BMC Fam. Pract. 2002, 3, 19. [Google Scholar] [CrossRef] [Green Version]
- Simpkin, A.J.; Rooshenas, L.; Wade, J.; Donovan, J.L.; Lane, J.A.; Martin, R.M.; Metcalfe, C.; Albertsen, P.C.; Hamdy, F.C.; Holmberg, L.; et al. Development, Validation and Evaluation of an Instrument for Active Monitoring of Men with Clinically Localised Prostate Cancer: Systematic Review, Cohort Studies and Qualitative Study. Health Serv. Deliv. Res. 2015, 3. [Google Scholar] [CrossRef]
- Welch, H.G.; Schwartz, L.M.; Woloshin, S. Prostate-specific antigen levels in the United States: Implications of various definitions for abnormal. J. Natl. Cancer Inst. 2005, 97, 1132–1137. [Google Scholar] [CrossRef]
- Narain, V.; Bianco, F.J., Jr.; Grignon, D.J.; Sakr, W.A.; Pontes, J.E.; Wood, D.P., Jr. How accurately does prostate biopsy Gleason score predict pathologic findings and disease free survival? Prostate 2001, 49, 185–190. [Google Scholar] [CrossRef]
- Melia, J.; Moseley, R.; Ball, R.Y.; Griffiths, D.F.R.; Grigor, K.; Harnden, P.; Parkinson, M.C. A UK-based investigation of inter-and intra-observer reproducibility of Gleason grading of prostatic biopsies. Histopathology 2006, 48, 644–654. [Google Scholar] [CrossRef] [PubMed]
- Short, E.; Warren, A.Y.; Varma, M. Gleason grading of prostate cancer: A pragmatic approach. Diagn. Histopathol. 2019, 25, 371–378. [Google Scholar] [CrossRef] [Green Version]
- Hu, J.C.; Gu, X.; Lipsitz, S.R.; Barry, M.J.; D’Amico, A.V.; Weinberg, A.C.; Keating, N.L. Comparative effectiveness of minimally invasive vs open radical prostatectomy. JAMA 2009, 302, 1557–1564. [Google Scholar] [CrossRef] [PubMed]
- Bjurlin, M.A.; Wysock, J.S.; Taneja, S.S. Optimization of prostate biopsy: Review of technique and complications. Urol. Clin. 2014, 41, 299–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lojanapiwat, B.; Anutrakulchai, W.; Chongruksut, W.; Udomphot, C. Correlation and diagnostic performance of the prostate-specific antigen level with the diagnosis, aggressiveness, and bone metastasis of prostate cancer in clinical practice. Prostate Int. 2014, 2, 133–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, B.; Cheng, J.; Guo, D.; He, X.; Luo, Y.; Zeng, Y.; Li, C. Prediction of prostate cancer aggressiveness with a combination of radiomics and machine learning-based analysis of dynamic contrast-enhanced MRI. Clin. Radiol. 2019, 74, 896.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinreb, J.C.; Barentsz, J.O.; Choyke, P.L.; Cornud, F.; Haider, M.A.; Macura, K.J.; A Margolis, D.J.; Schnall, M.D.; Shtern, F.; Tempany, C.M.; et al. PI-RADS Prostate Imaging–Reporting and Data System: 2015, Version 2. Eur. Urol. 2016, 69, 16–40. [Google Scholar] [CrossRef]
- Mehralivand, S.; Shih, J.H.; Rais-Bahrami, S.; Oto, A.; Bednarova, S.; Nix, J.W.; Thomas, J.V.; Gordetsky, J.B.; Gaur, S.; Harmon, S.A.; et al. A Magnetic Resonance Imaging–Based Prediction Model for Prostate Biopsy Risk Stratification. JAMA Oncol. 2018, 4, 678–685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donati, O.F.; Afaq, A.; Vargas, H.A.; Mazaheri, Y.; Zheng, J.; Moskowitz, C.S.; Hricak, H.; Akin, O. Prostate MRI: Evaluating tumor volume and apparent diffusion coefficient as surrogate biomarkers for predicting tumor Gleason score. Clin. Cancer Res. 2014, 20, 3705–3711. [Google Scholar] [CrossRef] [Green Version]
- Fehr, D.; Veeraraghavan, H.; Wibmer, A.; Gondo, T.; Matsumoto, K.; Vargas, H.A.; Sala, E.; Hricak, H.; Deasy, J.O. Automatic classification of prostate cancer Gleason scores from multiparametric magnetic resonance images. Proc. Natl. Acad. Sci. USA 2015, 112, E6265–E6273. [Google Scholar] [CrossRef] [Green Version]
- Alexandratou, E.; Yova, D.; Gorpas, D.; Maragos, P.; Agrogiannis, G.; Kavantzas, N. Texture analysis of tissues in Gleason grading of prostate cancer. In Imaging, Manipulation, and Analysis of Biomolecules, Cells, and Tissues VI; International Society for Optics and Photonics: Bellingham, WA, USA, 2008; p. 685904. [Google Scholar]
- Chaddad, A.; Niazi, T.; Probst, S.; Bladou, F.; Anidjar, M.; Bahoric, B. Predicting Gleason Score of Prostate Cancer Patients Using Radiomic Analysis. Front. Oncol. 2018, 8, 630. [Google Scholar] [CrossRef] [Green Version]
- Nketiah, G.; Elschot, M.; Kim, E.; Teruel, J.R.; Scheenen, T.W.; Bathen, T.F.; Selnæs, K.M. T2-weighted MRI-derived textural features reflect prostate cancer aggressiveness: Preliminary results. Eur. Radiol. 2017, 27, 3050–3059. [Google Scholar] [CrossRef]
- Ploussard, G.; Epstein, J.I.; Montironi, R.; Carroll, P.R.; Wirth, M.; Grimm, M.O.; Bjartell, A.S.; Montorsi, F.; Freedland, S.J.; Erbersdobler, A.; et al. The contemporary concept of significant versus insignificant prostate cancer. Eur. Urol. 2011, 60, 291–303. [Google Scholar] [CrossRef] [Green Version]
- Alqahtani, S.; Wei, C.; Zhang, Y.; Szewczyk-Bieda, M.; Wilson, J.; Huang, Z.; Nabi, G. Prediction of prostate cancer Gleason score upgrading from biopsy to radical prostatectomy using pre-biopsy multiparametric MRI PIRADS scoring system. Sci. Rep. 2020, 10, 7722. [Google Scholar] [CrossRef]
- Sheikh, N.; Wei, C.; Szewczyk-Bieda, M.; Campbell, A.; Memon, S.; Lang, S.; Nabi, G. Combined T2 and diffusion-weighted MR imaging with template prostate biopsies in men suspected with prostate cancer but negative transrectal ultrasound-guided biopsies. World J. Urol. 2017, 35, 213–220. [Google Scholar] [CrossRef] [Green Version]
- Wei, C.; Jin, B.; Szewczyk-Bieda, M.; Gandy, S.; Lang, S.; Zhang, Y.; Huang, Z.; Nabi, G. Quantitative parameters in dynamic contrast-enhanced magnetic resonance imaging for the detection and characterization of prostate cancer. Oncotarget 2018, 9, 15997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Epstein, J.I.; Allsbrook, W.C., Jr.; Amin, M.B.; Egevad, L.L.; ISUP Grading Committee. The 2005 International Society of Urological Pathology (ISUP) consensus conference on Gleason grading of prostatic carcinoma. Am. J. Surg. Pathol. 2005, 29, 1228–1242. [Google Scholar]
- Epstein, J.I.; Egevad, L.; Amin, M.B.; Delahunt, B.; Srigley, J.R.; Humphrey, P.A. The 2014 International Society of Urological Pathology (ISUP) consensus conference on Gleason grading of prostatic carcinoma. Am. J. Surg. Pathol. 2016, 40, 244–252. [Google Scholar] [CrossRef]
- Nketiah, G.A.; Elschot, M.; Scheenen, T.W.; Maas, M.C.; Bathen, T.F.; Selnæs, K.M. Utility of T 2-weighted MRI texture analysis in assessment of peripheral zone prostate cancer aggressiveness: A single-arm, multicenter study. Sci. Rep. 2021, 11, 1–13. [Google Scholar]
- Chen, T.; Li, M.; Gu, Y.; Zhang, Y.; Yang, S.; Wei, C.; Wu, J.; Li, X.; Zhao, W.; Shen, J. Prostate cancer differentiation and aggressiveness: Assessment with a radiomic-based model vs. PI-RADS v2. J. Magn. Reson. Imaging 2019, 49, 875–884. [Google Scholar] [CrossRef] [Green Version]
- Barucci, A.; Bastiani, P.; Carpi, R.; Fondelli, S.; Giannetti, A.; Olmastroni, M.; Pini, R.; Ratto, F.; Rucco, M.; Zatelli, G.; et al. Prostate cancer Radiomics using multiparametric MR imaging: An exploratory study. Phys. Medica Eur. J. Med. Phys. 2018, 56, 246. [Google Scholar] [CrossRef]
- Woźnicki, P.; Westhoff, N.; Huber, T.; Riffel, P.; Froelich, M.F.; Gresser, E.; von Hardenberg, J.; Mühlberg, A.; Michel, M.S.; Schoenberg, S.O.; et al. Multiparametric MRI for prostate cancer characterization: Combined use of radiomics model with PI-RADS and clinical parameters. Cancers 2020, 12, 1767. [Google Scholar] [CrossRef]
- Hectors, S.J.; Cherny, M.; Yadav, K.K.; Beksaç, A.T.; Thulasidass, H.; Lewis, S.; Davicioni, E.; Wang, P.; Tewari, A.K.; Taouli, B. Radiomics features measured with multiparametric magnetic resonance imaging predict prostate cancer aggressiveness. J. Urol. 2019, 202, 498–505. [Google Scholar] [CrossRef]
- Haralick, R.M.; Shanmugam, K.; Dinstein, I. Textural Features for Image Classification. IEEE Trans. Syst. Man Cybern. 1973, 6, 610–621. [Google Scholar] [CrossRef] [Green Version]
- Slaoui, H.; Neuzillet, Y.; Ghoneim, T.; Rouanne, M.; Abdou, A.; Lugagne-Delpon, P.M.; Scherrer, A.; Radulescu, C.; Delancourt, C.; Molinie, V.; et al. Gleason score within prostate abnormal areas defined by multiparametric magnetic resonance imaging did not vary according to the PIRADS score. Urol. Int. 2017, 99, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Algohary, A.; Viswanath, S.; Shiradkar, R.; Ghose, S.; Pahwa, S.; Moses, D.; Jambor, I.; Shnier, R.; Böhm, M.; Haynes, A.M.; et al. Radiomic features on MRI enable risk categorization of prostate cancer patients on active surveillance: Preliminary findings. J. Magn. Reson. Imaging 2018, 48, 818–828. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Weng, Z.; Xu, H.; Zhang, Z.; Miao, H.; Chen, W.; Liu, Z.; Zhang, X.; Wang, M.; Xu, X.; et al. Support Vector Machines (SVM) classification of prostate cancer Gleason score in central gland using multiparametric magnetic resonance images: A cross-validated study. Eur. J. Radiol. 2018, 98, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Chitalia, R.D.; Kontos, D. Role of texture analysis in breast MRI as a cancer biomarker: A review. J. Magn. Reson. Imaging 2019, 49, 927–938. [Google Scholar] [CrossRef]
- Li, M.; Yang, L.; Yue, Y.; Xu, J.; Huang, C.; Song, B. Use of Radiomics to Improve Diagnostic Performance of PI-RADS v2.1 in Prostate Cancer. Front. Oncol. 2021, 10, 3465. [Google Scholar] [CrossRef]
- Chun, F.; Steuber, T.; Erbersdobler, A.; Currlin, E.; Walz, J.; Schlomm, T.; Haese, A.; Heinzer, H.; McCormack, M.; Huland, H.; et al. Development and Internal Validation of a Nomogram Predicting the Probability of Prostate Cancer Gleason Sum Upgrading Between Biopsy and Radical Prostatectomy Pathology. Eur. Urol. 2006, 49, 820–826. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gleason Grade Score | Gleason Group | Number |
|---|---|---|
| Gleason Grade Score ≤6 | Group 1 | 67 |
| Gleason Grade Score 3 + 4 = 7 | Group 2 | 54 |
| Gleason Grade Score 4 + 3 = 7 | Group 3 | 79 |
| and above |
| Covariate | Univariate Logistic Regression | Multivariable Logistic Regression | ||||||
|---|---|---|---|---|---|---|---|---|
| OR | 95%CI | p Value | OR | 95%CI | p Value | |||
| Lower | Upper | Lower | Upper | |||||
| PSAD | 6.889 | 0.500 | 94.847 | 0.149 | - | |||
| PI-RADS 3 | Ref | 0.356 | - | |||||
| PI-RADS 4 | 1.570 | 0.568 | 4.342 | 0.385 | ||||
| PI-RADS 5 | 2.296 | 0.718 | 7.342 | 0.161 | ||||
| Angular Second Moment T2WI | 1.529 | 0.219 | 10.678 | 0.668 | - | |||
| Contrast T2WI | 1.023 | 1.007 | 1.040 | 0.005 | 1.017 | 0.993 | 1.041 | 0.168 |
| Sum Square Variaqnce T2WI | 0.976 | 0.965 | 0.988 | <0.001 | 0.981 | 0.963 | 1.001 | 0.051 |
| Sum Variance T2WI | 0.905 | 0.877 | 0.933 | <0.001 | 0.909 | 0.873 | 0.948 | <0.001 |
| Sum Entropy T2WI | 1.923 | 1.417 | 2.609 | <0.001 | 2.022 | 1.220 | 3.350 | 0.006 |
| Difference Variance T2WI | 1.056 | 1.024 | 1.090 | 0.001 | 1.068 | 1.015 | 1.124 | 0.011 |
| Difference Entropy T2WI | 1.278 | 1.020 | 1.601 | 0.033 | 1.065 | 0.776 | 1.463 | 0.696 |
| Correlation ADC | 8.400 | 1.998 | 35.308 | 0.004 | 5.030 | 0.766 | 33.050 | 0.093 |
| Sum Square Variance ADC | 1.002 | 0.986 | 1.018 | 0.839 | - | |||
| Sum Entropy ADC | 1.504 | 1.095 | 2.066 | 0.012 | 1.103 | 0.702 | 1.732 | 0.672 |
| Entropy ADC | 2.667 | 1.691 | 4.208 | <0.001 | 1.835 | 1.017 | 3.312 | 0.044 |
| Difference Variance ADC | 1.072 | 1.033 | 1.113 | <0.001 | 1.105 | 1.042 | 1.172 | 0.001 |
| Actual Significant PCa | Actual Non Significant PCa | AUC | Standard Error | Difference AUC | Standard Error of Difference | z Value | p Value | |
|---|---|---|---|---|---|---|---|---|
| Radiomic Features | 72 | 128 | 0.901 | 0.021 | 0.350 | 0.048 | 7.274 | <0.001 |
| PIRADS | 67 | 123 | 0.551 | 0.044 | ||||
| Radiomic Features | 72 | 128 | 0.901 | 0.021 | 0.344 | 0.045 | 7.577 | <0.001 |
| PSAD | 67 | 123 | 0.557 | 0.045 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ogbonnaya, C.N.; Zhang, X.; Alsaedi, B.S.O.; Pratt, N.; Zhang, Y.; Johnston, L.; Nabi, G. Prediction of Clinically Significant Cancer Using Radiomics Features of Pre-Biopsy of Multiparametric MRI in Men Suspected of Prostate Cancer. Cancers 2021, 13, 6199. https://doi.org/10.3390/cancers13246199
Ogbonnaya CN, Zhang X, Alsaedi BSO, Pratt N, Zhang Y, Johnston L, Nabi G. Prediction of Clinically Significant Cancer Using Radiomics Features of Pre-Biopsy of Multiparametric MRI in Men Suspected of Prostate Cancer. Cancers. 2021; 13(24):6199. https://doi.org/10.3390/cancers13246199
Chicago/Turabian StyleOgbonnaya, Chidozie N., Xinyu Zhang, Basim S. O. Alsaedi, Norman Pratt, Yilong Zhang, Lisa Johnston, and Ghulam Nabi. 2021. "Prediction of Clinically Significant Cancer Using Radiomics Features of Pre-Biopsy of Multiparametric MRI in Men Suspected of Prostate Cancer" Cancers 13, no. 24: 6199. https://doi.org/10.3390/cancers13246199
APA StyleOgbonnaya, C. N., Zhang, X., Alsaedi, B. S. O., Pratt, N., Zhang, Y., Johnston, L., & Nabi, G. (2021). Prediction of Clinically Significant Cancer Using Radiomics Features of Pre-Biopsy of Multiparametric MRI in Men Suspected of Prostate Cancer. Cancers, 13(24), 6199. https://doi.org/10.3390/cancers13246199