
Retinoblastoma Survival Following Primary Enucleation by AJCC Staging


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection and Ethics
2.2. Eligibility
2.3. Treatment
2.4. Statistical Analysis
3. Results
3.1. Clinical Characteristics and Treatments
3.2. Survival
3.3. Analysis of Patients Who Died
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kivelä, T. The epidemiological challenge of the most frequent eye cancer: Retinoblastoma, an issue of birth and death. Br. J. Ophthalmol. 2009, 93, 1129–1131. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Feng, Z.; Gallie, B. Natural History of Untreated Retinoblastoma. Cancers 2021, 13, 3646. [Google Scholar] [CrossRef] [PubMed]
- Abramson, D.H. Retinoblastoma in the 20th Century: Past Success and Future Challenges the Weisenfeld Lecture. Investig. Opthalmol. Vis. Sci. 2005, 46, 2684–2691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, H.S.L.; DeBoer, G.; Thiessen, J.J.; Budning, A.; Kingston, J.E.; O’Brien, J.M.; Koren, G.; Giesbrecht, E.; Haddad, G.; Verjee, Z.; et al. Combining cyclosporin with chemotherapy con-trols intraocular retinoblastoma without requiring radiation. Clin. Cancer Res. 1996, 2, 1499–1508. [Google Scholar] [PubMed]
- Murphree, A.L.; Villablanca, J.G.; Deegan, W.F.; Sato, J.K.; Malogolowkin, M.; Fisher, A.; Parker, R.; Reed, E.; Gomer, C.J. Chemotherapy Plus Local Treatment in the Management of Intraocular Retinoblastoma. Arch. Ophthalmol. 1996, 114, 1348–1356. [Google Scholar] [CrossRef] [PubMed]
- Kingston, J.E.; Hungerford, J.L.; Madreperla, S.A.; Plowman, P.N. Results of combined chemotherapy and radiotherapy for advanced intraocular retinoblastoma. Arch. Ophthalmol. 1996, 114, 1339–1343. [Google Scholar] [CrossRef] [PubMed]
- Gallie, B.L.; Budning, A.; DeBoer, G.; Thiessen, J.J.; Koren, G.; Verjee, Z.; Ling, V.; Chan, H.S.L. Chemotherapy with Focal Therapy Can Cure Intraocular Retinoblastoma Without Radiotherapy. Arch. Ophthalmol. 1996, 114, 1321–1328. [Google Scholar] [CrossRef] [PubMed]
- Francis, J.H.; Levin, A.M.; Zabor, E.C.; Gobin, Y.P.; Abramson, D.H. Ten-year experience with ophthalmic artery chemosurgery: Ocular and recurrence-free survival. PLoS ONE 2018, 13, e0197081. [Google Scholar] [CrossRef]
- Munier, F.L.; Mosimann, P.; Puccinelli, F.; Gaillard, M.C.; Stathopoulos, C.; Houghton, S.; Bergin, C.; Beck-Popovic, M. First-line intra-arterial versus intra-venous chemotherapy in unilateral sporadic group D retinoblastoma: Evidence of better visual outcomes, ocular survival and shorter time to success with intra-arterial delivery from retrospective review of 20 years of treatment. Br. J. Ophthalmol. 2016, 101, 1086–1093. [Google Scholar] [PubMed]
- Munier, F.L.; Soliman, S.; Moulin, A.P.; Gaillard, M.C.; Balmer, A.; Beck-Popovic, M. Profiling safety of intravitreal injections for reti-noblastoma using an anti-reflux procedure and sterilisation of the needle track. Br. J. Ophthalmol. 2012, 96, 1084–1087. [Google Scholar] [CrossRef]
- Berry, J.L.; Shah, S.; Bechtold, M.; Zolfaghari, E.; Jubran, R.; Kim, J.W. Long-term outcomes of Group D retinoblastoma eyes during the intravitreal melphalan era. Pediatr. Blood Cancer 2017, 64, e26696. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Li, Q.; Wu, S.; Jin, L.; Ma, X.; Jin, M.; Wang, Y.; Gallie, B. Pars Plana Vitrectomy and Endoresection of Refractory Intraocular Retinoblastoma. Ophthalmology 2018, 125, 320–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Global Retinoblastoma Study Group. Global Retinoblastoma Presentation and Analysis by National Income Level. JAMA Oncol. 2020, 6, 685–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chantada, G.L.; Qaddoumi, I.; Canturk, S.; Khetan, V.; Ma, Z.; Kimani, K.; Yeniad, B.; Sultan, I.; Sitorus, R.S.; Tacyildiz, N.; et al. Strategies to manage retinoblastoma in developing countries. Pediatr. Blood Cancer 2010, 56, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Feng, Z.X.; Wei, M.; Liu, G.; Solarte, C.E.; Li, B.; Wang, Y.; Zhang, C.; Gallie, B.L. Impact of Systemic Chemotherapy and Delayed Enucleation on Survival of Children with Advanced Intraocular Retinoblastoma. Ophthalmol. Retin. 2020, 4, 630–639. [Google Scholar] [CrossRef]
- Luna-Fineman, S.; Chantada, G.; Alejos, A.; Amador, G.; Barnoya, M.; Castellanos, M.E.; Fu, L.; Fuentes-Alabi, S.; Girón, V.; Goenz, M.A.; et al. Delayed Enucleation with Neoadjuvant Chemotherapy in Advanced Intraocular Unilateral Retinoblastoma: AHOPCA II, a Prospective, Multi-Institutional Protocol in Central America. J. Clin. Oncol. 2019, 37, 2875–2882. [Google Scholar] [CrossRef]
- Murphree, A.L. Intraocular Retinoblastoma: The Case for a New Group Classification. Ophthalmol. Clin. N. Am. 2005, 18, 41–53. [Google Scholar] [CrossRef]
- Shields, C.L.; Mashayekhi, A.; Au, A.K.; Czyz, C.; Leahey, A.; Meadows, A.T.; Shields, J.A. The International Classification of Retinoblastoma Predicts Chemoreduction Success. Ophthalmology 2006, 113, 2276–2280. [Google Scholar] [CrossRef]
- Children’s Oncology Group. Just Diagnosed. 2011. Available online: https://www.childrensoncologygroup.org/index.php/newlydiagnosedwithretinoblastoma (accessed on 21 July 2021).
- Scelfo, C.; Francis, J.H.; Khetan, V.; Jenkins, T.; Marr, B.; Abramson, D.H.; Shields, C.L.; Pe’Er, J.; Munier, F.; Berry, J.; et al. An international survey of classification and treatment choices for group D retinoblastoma. Int. J. Ophthalmol. 2017, 10, 961–967. [Google Scholar] [CrossRef]
- Finger, P.T. The 7th edition AJCC staging system for eye cancer: An international language for ophthalmic oncology. Arch. Pathol. Lab. Med. 2009, 133, 1197–1198. [Google Scholar] [CrossRef] [PubMed]
- Mallipatna, A.; Gallie, B.L.; Chévez-Barrios, P.; Lumbroso-Le Rouic, L.; Chantada, G.L.; Doz, F.; Brisse, H.J.; Munier, F.L.; Albert, D.M.; Català -Mora, J.; et al. Retinoblastoma. In AJCC Cancer Staging Manual, 8th ed.; Amin, M.B., Edge, S.B., Greene, F.L., Eds.; Springer: New York, NY, USA, 2017; pp. 819–831. [Google Scholar]
- Tomar, A.S.; Finger, P.T.; Gallie, B.; Mallipatna, A.; Kivela, T.T.; Zhang, C.; Zhao, J.; Wilson, M.W.; Brenna, R.C.; Burges, M.; et al. A Multicenter, International Collaborative Study for AJCC-Staging of Retinoblastoma: Treatment Success and Globe Salvage. Ophthalmology 2020, 127, 1733–1746. [Google Scholar] [CrossRef]
- Zhao, J.; Dimaras, H.; Massey, C.; Xu, X.; Huang, D.; Li, B.; Chan, H.S.L.; Gallie, B.L. Pre-enucleation chemotherapy for eyes severely affected by reti-noblastoma masks risk of tumor extension and increases death from metastasis. J. Clin. Oncol. 2011, 29, 845–851. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.E.; Francis, J.H.; Dunkel, I.J.; Shields, C.L.; Yu, M.D.; Berry, J.L.; Kogachi, K.; Skalet, A.H.; Miller, A.K.; Santapuram, P.R.; et al. Metastases and death rates after primary enucleation of unilateral retinoblastoma in the USA 2007–2017. Br. J. Ophthalmol. 2018, 103, 1272–1277. [Google Scholar] [CrossRef] [PubMed]
- Yannuzzi, N.A.; Francis, J.H.; Marr, B.P.; Belinsky, I.; Dunkel, I.J.; Gobin, Y.P.; Abramson, D.H. Enucleation vs Ophthalmic Artery Chemosurgery for Advanced Intraocular Retinoblastoma: A Retrospective Analysis. JAMA Ophthalmol. 2015, 133, 1062–1066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, R.D.; Gupta, S.K.; Aggarwal, H.; Kumar, P. A palliative approach for rehabilitation of a pediatric patient with retinoblastoma. Indian J. Palliat. Care 2013, 19, 67–70. [Google Scholar] [CrossRef] [PubMed]
- Tomar, A.S.; Finger, P.T.; Gallie, B.; Kivela, T.T.; Mallipatna, A.; Zhang, C.; Zhao, J.; Wilson, M.W.; Brenna, R.C.; Burges, M.; et al. Global Retinoblastoma Treatment Outcomes: Association with National Income Level. Ophthalmology 2021, 128, 740–753. [Google Scholar] [CrossRef] [PubMed]
- Sreelakshmi, K.V.; Chandra, A.; Krishnakumar, S.; Natarajan, V.; Khetan, V. Anterior Chamber Invasion in Retinoblastoma: Not an Indication for Adjuvant Chemotherapy. Investig. Opthalmol. Vis. Sci. 2017, 58, 4654. [Google Scholar] [CrossRef] [Green Version]
- Bosaleh, A.; Sampor, C.; Solernou, V.; Fandiño, A.; Domínguez, J.; De Davila, M.T.G.; Chantada, G.L. Outcome of Children with Retinoblastoma and Isolated Choroidal Invasion. Arch. Ophthalmol. 2012, 130, 724–729. [Google Scholar] [CrossRef] [Green Version]
- Hiasat, J.G.; Saleh, A.; Al-Hussaini, M.; Alnawaiseh, I.; Mehyar, M.; Qandeel, M.; Mohammad, M.; Deebajah, R.; Sultan, I.; Jaradat, I.; et al. The predictive value of magnetic resonance imaging of retinoblastoma for the likelihood of high-risk pathologic features. Eur. J. Ophthalmol. 2018, 29, 262–268. [Google Scholar] [CrossRef]
- Kletke, S.N.; Feng, Z.X.; Hazrati, L.N.; Gallie, B.L.; Soliman, S.E. Clinical Predictors at Diagnosis of Low-Risk Histopathology in Uni-lateral Advanced Retinoblastoma. Ophthalmology 2019, 126, 1306–1314. [Google Scholar] [CrossRef]
- Kaliki, S.; Srinivasan, V.; Gupta, A.; Mishra, D.K.; Naik, M.N. Clinical Features Predictive of High-Risk Retinoblastoma in 403 Asian Indian Patients: A Case-Control Study. Ophthalmology 2015, 122, 1165–1172. [Google Scholar] [CrossRef] [PubMed]
- Chévez-Barrios, P.; Eagle, R.C., Jr.; Krailo, M.; Piao, J.; Albert, D.M.; Gao, Y.; Vemuganti, G.; Ali, M.J.; Khetan, V.; Honavar, S.G.; et al. Study of Unilateral Retinoblastoma with and without Histopathologic High-Risk Features and the Role of Adjuvant Chemotherapy: A Children’s Oncology Group Study. J. Clin. Oncol. 2019, 37, 2883–2891. [Google Scholar] [CrossRef]
- Atchaneeyasakul, L.-O.; Wongsiwaroj, C.; Uiprasertkul, M.; Sanpakit, K.; Thephamongkhol, K.; Trinavarat, A. Prognostic factors and treatment outcomes of retinoblastoma in pediatric patients: A single-institution study. Jpn. J. Ophthalmol. 2009, 53, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Shields, C.L.; De Potter, P.; Himelstein, B.P.; Shields, J.A.; Meadows, A.T.; Maris, J.M. Chemoreduction in the Initial Management of Intraocular Retinoblastoma. Arch. Ophthalmol. 1996, 114, 1330–1338. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total Patients n = 700 | Death n = 31 | |
|---|---|---|---|
| Sex | Male | 404 (58%) | 19 (61%) |
| Female | 296 (42%) | 12 (39%) | |
| Age of diagnosis (months) | Median | 24 | 29 |
| Range | 1–212 | 4–63 | |
| Laterality | Right | 357 (51%) | 17 (55%) |
| Left | 342 (49%) | 14 (45%) | |
| Clinical Staging AJCC 8th edition | |||
| cT2b | Vitreous and/or subretinal seeding | 228 (32%) | 2 (6%) |
| cT3a | Phthisis or pre-phthisis bulbi | 3 (0.4%) | 0 (0%) |
| cT3b | Tumor invasion of choroid, pars plana, ciliary body, lens, zonules, iris, or anterior chamber | 150 (22%) | 2 (6%) |
| cT3c | Raised intraocular pressure with neovascularization and/or buphthalmos | 159 (23%) | 21 (68%) |
| cT3d | Hyphema and/or massive vitreous hemorrhage | 104 (15%) | 3 (10%) |
| cT3e | Aseptic orbital cellulitis | 2 (0.3%) | 1 (3%) |
| Unknown | 54 (8%) | 2 (6%) | |
| Pathological Staging AJCC 8th edition | |||
| pT1 | Intraocular tumor(s) without any local invasion, focal choroidal invasion, or pre- or intralaminar involvement of the optic nerve head | 383 (55%) | 3 (10%) |
| pT2a | Concomitant focal choroidal invasion and pre- or intralaminar involvement of the optic nerve head | 31 (5%) | 0 (0%) |
| pT2b | Tumor invasion of stroma of iris and/or trabecular meshwork and/or Schlemm’s canal | 22 (3%) | 1 (3%) |
| pT3a | Massive choroidal invasion (>3 mm in largest diameter, or multiple foci of focal choroidal involvement totaling >3 mm, or any full-thickness choroidal involvement) | 16 (2%) | 0 (0%) |
| pT3b | Retrolaminar invasion of the optic nerve head, not involving the transected end of the optic nerve | 143 (20%) | 10 (32%) |
| pT3c/d | Any partial-thickness involvement of inner two thirds sclera; full-thickness invasion into outer third of sclera and/or invasion into or around emissary channels | 13 (2%) | 1 (3%) |
| pT4 | Evidence of extraocular tumor: tumor at transected end of optic nerve, tumor in meningeal spaces around optic nerve, full- thickness invasion of sclera with invasion of episclera, adjacent adipose tissue, extraocular muscle, bone, conjunctiva, or eyelids | 22 (3%) | 13 (42%) |
| Unknown | 70 (10%) | 3 (10%) | |
| Classification | Variable | 5-Year Kaplan–Meier DSS Estimate (95% CI), % | ||
|---|---|---|---|---|
| IIRC Classification (n = 646) | Group D (n = 228) | 99.1 (97.9–100) | ||
| Group E (n = 418) | 93.7 (91.3–96.1) | |||
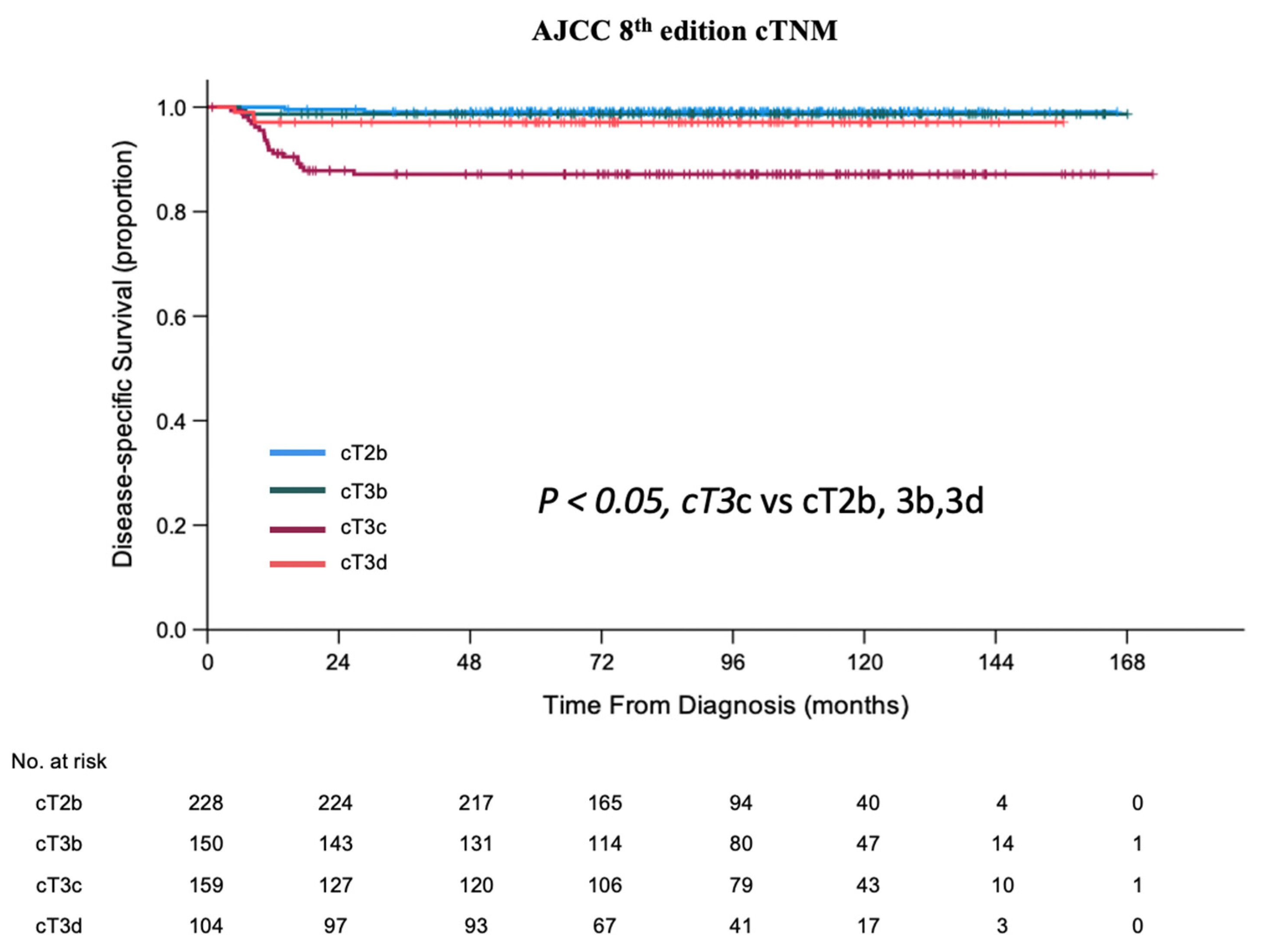
| AJCC cTNM (n = 641) | cT2b (n = 228) | 99.1 (97.9–100) | ||
| cT3b (n = 150) | 98.7 (96.8–100) | |||
| cT3c (n = 159) | 87.1 (81.8–92.7) | |||
| cT3d (n = 104) | 97.2 (93.8–100) | |||
| Pairwise Comparison p-value for AJCC | cT2b | cT3b | cT3c | |
| cT2b | ||||
| cT3b | 0.663 | |||
| cT3c | <0.001 | <0.001 | ||
| cT3d | 0.158 | 0.384 | 0.007 | |
| Overall Wilcoxon Log-Rank p < 0.001 | ||||
| Classification | Variable | 5-Year Kaplan–Meier DSS Estimate % (95% CI) | |||||
|---|---|---|---|---|---|---|---|
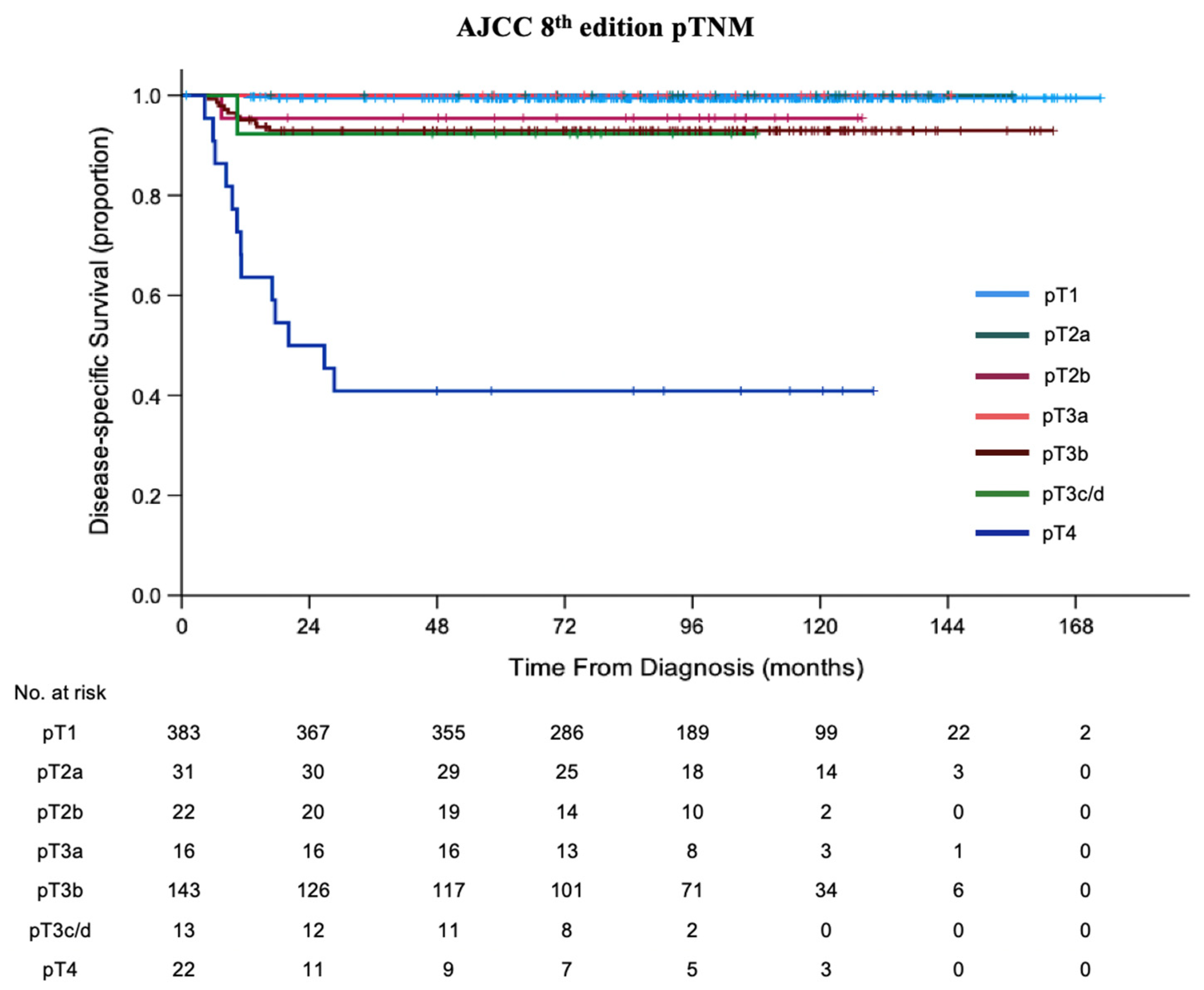
| AJCC 8th edition pTNM | pT1 (n = 383) | 99.5 (98.7–100) | |||||
| pT2a (n = 31) | 100 | ||||||
| pT2b (n = 22) | 95.5 (86.6–100) | ||||||
| pT3a (n = 16) | 100 | ||||||
| pT3b (n = 143) | 93.0 (88.7–97.3) | ||||||
| pT3c/d (n = 13) | 92.3 (77.5–100) | ||||||
| pT4 (n = 22) | 40.9 (20.0–61.9) | ||||||
| Pairwise Comparison p-value | pT1 | pT2a | pT2b | pT3a | pT3b | pT3c/d | |
| pT1 | |||||||
| pT2a | 0.685 | ||||||
| pT2b | 0.031 | 0.235 | |||||
| pT3a | 0.771 | - | 0.394 | ||||
| pT3b | <0.001 | 0.133 | 0.177 | 0.281 | |||
| pT3c/d | 0.003 | 0.123 | 0.719 | 0.267 | 0.935 | ||
| pT4 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | 0.005 | |
| Overall Wilcoxon Log-Rank p < 0.001 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, J.; Feng, Z.; Leung, G.; Gallie, B.L. Retinoblastoma Survival Following Primary Enucleation by AJCC Staging. Cancers 2021, 13, 6240. https://doi.org/10.3390/cancers13246240
Zhao J, Feng Z, Leung G, Gallie BL. Retinoblastoma Survival Following Primary Enucleation by AJCC Staging. Cancers. 2021; 13(24):6240. https://doi.org/10.3390/cancers13246240
Chicago/Turabian StyleZhao, Junyang, Zhaoxun Feng, Gareth Leung, and Brenda L. Gallie. 2021. "Retinoblastoma Survival Following Primary Enucleation by AJCC Staging" Cancers 13, no. 24: 6240. https://doi.org/10.3390/cancers13246240
APA StyleZhao, J., Feng, Z., Leung, G., & Gallie, B. L. (2021). Retinoblastoma Survival Following Primary Enucleation by AJCC Staging. Cancers, 13(24), 6240. https://doi.org/10.3390/cancers13246240