Aromatase and CDK4/6 Inhibitor-Induced Musculoskeletal Symptoms: A Systematic Review

 , ,
, ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
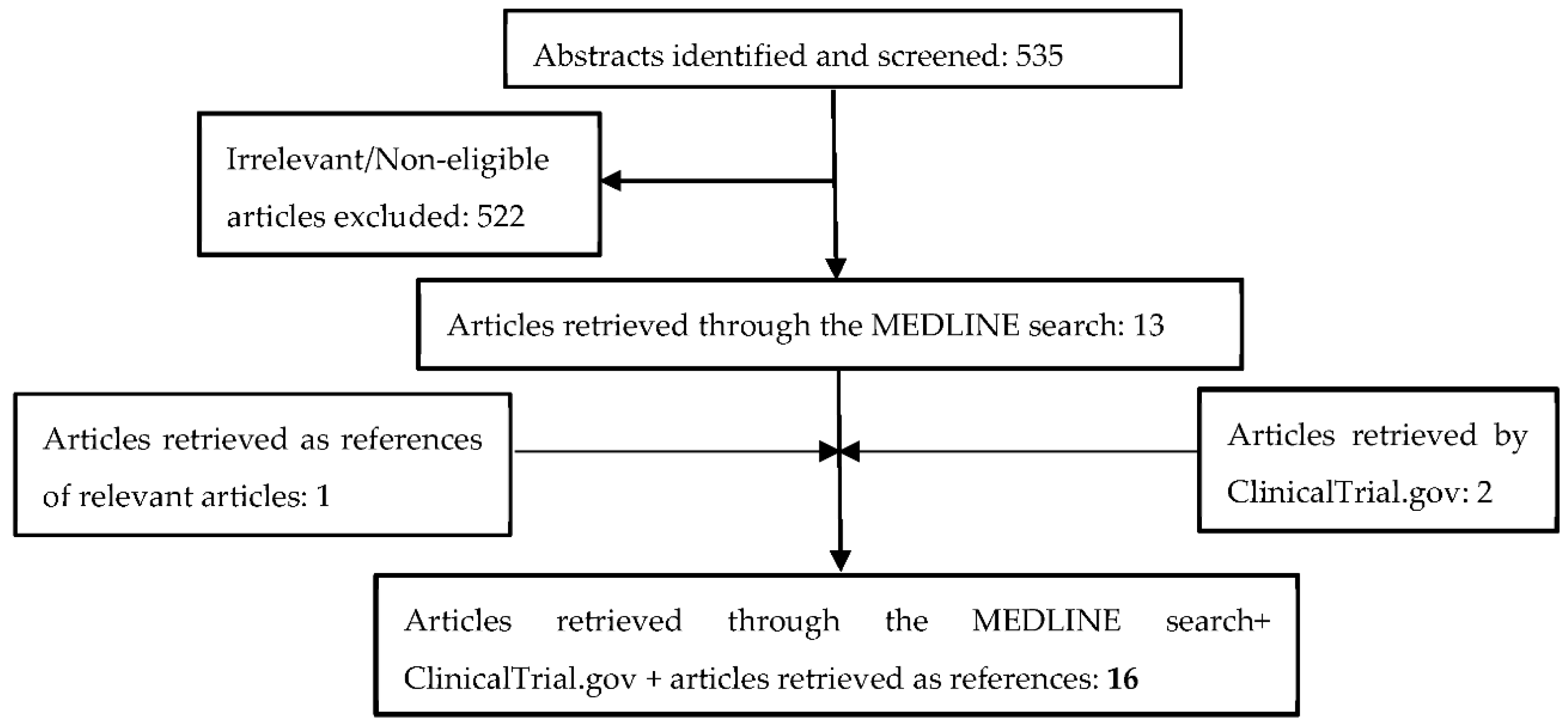
2.1. Search Strategy and Eligibility of Studies
2.2. Data Extraction
3. Results
3.1. Arthralgia
3.2. Myalgia
3.3. Bone Pain
3.4. Back Pain
3.5. Osteoporosis-Osteoporotic Fracture
4. Discussion
5. Conlusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- Howlader, N.; Altekruse, S.F.; Li, C.I.; Chen, V.W.; Clarke, C.A.; Ries, L.A.G.; Cronin, K.A. US incidence of breast cancer subtypes defined by joint hormone receptor and HER2 status. J. Natl. Cancer Inst. 2014, 106. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.H.F.; Giuliano, M.; Trivedi, M.V.; Schiff, R.; Kent Osborne, C. Metastasis dormancy in estrogen receptor-positive breast cancer. Clin. Cancer Res. 2013, 19, 6389–6397. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Huo, X.; Zhao, F.; Ren, D.; Ahmad, R.; Yuan, X.; Du, F.; Zhao, J. Association of Cyclin-Dependent Kinases 4 and 6 Inhibitors with Survival in Patients with Hormone Receptor–Positive Metastatic Breast Cancer. JAMA Netw. Open 2020, 3, e2020312. [Google Scholar] [CrossRef]
- Goss, P.E.; Ingle, J.N.; Pritchard, K.I.; Robert, N.J.; Muss, H.; Gralow, J.; Gelmon, K.; Whelan, T.; Strasser-Weippl, K.; Rubin, S.; et al. Extending Aromatase-Inhibitor Adjuvant Therapy to 10 Years. N. Engl. J. Med. 2016, 375, 209–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Regan, M.M.; Price, K.N.; Giobbie-Hurder, A.; Thürlimann, B.; Gelber, R.D. Interpreting breast international group (BIG) 1-98: A randomized, double-blind, phase III trial comparing letrozole and tamoxifen as adjuvant endocrine therapy for postmenopausal women with hormone receptor-positive, early breast cancer. Breast Cancer Res. 2011, 13, 209. [Google Scholar] [CrossRef] [PubMed]
- Coombes, R.; Kilburn, L.; Snowdon, C.; Paridaens, R.; Coleman, R.; Jones, S.; Jassem, J.; Van de Velde, C.; Delozier, T.; Alvarez, I.; et al. Survival and safety of exemestane versus tamoxifen after 2–3 years’ tamoxifen treatment (Intergroup Exemestane Study): A randomised controlled trial. Lancet 2007, 369, 559–570. [Google Scholar] [CrossRef]
- Jeselsohn, R.; Buchwalter, G.; De Angelis, C.; Brown, M.; Schiff, R. ESR1 mutations-a mechanism for acquired endocrine resistance in breast cancer. Nat. Rev. Clin. Oncol. 2015, 12, 573–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hortobagyi, G.N.; Stemmer, S.M.; Burris, H.A.; Yap, Y.S.; Sonke, G.S.; Paluch-Shimon, S.; Campone, M.; Petrakova, K.; Blackwell, K.L.; Winer, E.P.; et al. Updated results from MONALEESA-2, a phase III trial of first-line ribociclib plus letrozole versus placebo plus letrozole in hormone receptor-positive, HER2-negative advanced breast cancer. Ann. Oncol. 2018, 29, 1541–1547. [Google Scholar] [CrossRef] [PubMed]
- Finn, R.S.; Martin, M.; Rugo, H.S.; Jones, S.; Im, S.-A.; Gelmon, K.; Harbeck, N.; Lipatov, O.N.; Walshe, J.M.; Moulder, S.; et al. Palbociclib and Letrozole in Advanced Breast Cancer. N. Engl. J. Med. 2016, 375, 1925–1936. [Google Scholar] [CrossRef] [PubMed]
- Goetz, M.P.; Toi, M.; Campone, M.; Trédan, O.; Bourayou, N.; Sohn, J.; Park, I.H.; Paluch-Shimon, S.; Huober, J.; Chen, S.C.; et al. MONARCH 3: Abemaciclib as initial therapy for advanced breast cancer. J. Clin. Oncol. 2017, 35, 3638–3646. [Google Scholar] [CrossRef] [PubMed]
- Klein, M.E.; Kovatcheva, M.; Davis, L.E.; Tap, W.D.; Koff, A. CDK4/6 Inhibitors: The Mechanism of Action May Not Be as Simple as Once Thought. Cancer Cell 2018, 34, 9–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beckwée, D.; Leysen, L.; Meuwis, K.; Adriaenssens, N. Prevalence of aromatase inhibitor-induced arthralgia in breast cancer: A systematic review and meta-analysis. Support. Care Cancer 2017, 25, 1673–1686. [Google Scholar] [CrossRef] [PubMed]
- Henry, N.L.; Azzouz, F.; Desta, Z.; Li, L.; Nguyen, A.T.; Lemler, S.; Hayden, J.; Tarpinian, K.; Yakim, E.; Flockhart, D.A.; et al. Predictors of aromatase inhibitor discontinuation as a result of treatment-emergent symptoms in early-stage breast cancer. J. Clin. Oncol. 2012, 30, 936–942. [Google Scholar] [CrossRef] [Green Version]
- Hadji, P. Aromatase inhibitor-associated bone loss in breast cancer patients is distinct from postmenopausal osteoporosis. Crit. Rev. Oncol. Hematol. 2009, 69, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Henry, N.L.; Giles, J.T.; Ang, D.; Mohan, M.; Dadabhoy, D.; Robarge, J.; Hayden, J.; Lemler, S.; Shahverdi, K.; Powers, P.; et al. Prospective characterization of musculoskeletal symptoms in early stage breast cancer patients treated with aromatase inhibitors. Breast Cancer Res. Treat. 2008, 111, 365–372. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [Green Version]
- Buzdar, A.; Douma, J.; Davidson, N.; Elledge, R.; Morgan, M.; Smith, R.; Porter, L.; Nabholtz, J.; Xiang, X.; Brady, C. Phase III, multicenter, double-blind, randomized study of letrozole, an aromatase inhibitor, for advanced breast cancer versus megestrol acetate. J. Clin. Oncol. 2001, 19, 3357–3366. [Google Scholar] [CrossRef]
- Kaufmann, M.; Bajetta, E.; Dirix, L.Y.; Fein, L.E.; Jones, S.E.; Zilembo, N.; Dugardyn, J.L.; Nasurdi, C.; Mennel, R.G.; Cervek, J.; et al. Exemestane is superior to megestrol acetate after tamoxifen failure in postmenopausal women with advanced breast cancer: Results of a phase III randomized double-blind trial. J. Clin. Oncol. 2000, 18, 1399–1411. [Google Scholar] [CrossRef]
- Buzdar, A.; Jonat, W.; Howell, A.; Jones, S.E.; Blomqvist, C.; Vogel, C.L.; Eiermann, W.; Wolter, J.M.; Azab, M.; Webster, A.; et al. Anastrozole, a potent and selective aromatase inhibitor, versus megestrol acetate in postmenopausal women with advanced breast cancer: Results of overview analysis of two phase III trials. J. Clin. Oncol. 1996, 14, 2000–2011. [Google Scholar] [CrossRef] [PubMed]
- Dombernowsky, P.; Smith, I.; Falkson, G.; Leonard, R.; Panasci, L.; Bellmunt, J.; Bezwoda, W.; Gardin, G.; Gudgeon, A.; Morgan, M.; et al. Letrozole, a new oral aromatase inhibitor for advanced breast cancer: Double-blind randomized trial showing a dose effect and improved efficacy and tolerability compared with megestrol acetate. J. Clin. Oncol. 1998, 16, 453–461. [Google Scholar] [CrossRef] [PubMed]
- Jonat, W.; Howell, A.; Blomqvist, C.; Eiermann, W.; Winblad, G.; Tyrrell, C.; Mauriac, L.; Roche, H.; Lundgren, S.; Hellmund, R.; et al. A randomised trial comparing two doses of the new selective aromatase inhibitor anastrozole (Arimidex)* with megestrol acetate in postmenopausal patients with advanced breast cancer. Eur. J. Cancer 1996, 32, 404–412. [Google Scholar] [CrossRef]
- Freue, M.; Kjaer, M.; Boni, C.; Joliver, J.; Jänicke, F.; Willemse, H.B.; Coombes, R.C.; Van Belle, S.; Pérez-Carrión, R.; Zieschang, J.; et al. Open comparative trial of formestane versus megestrol acetate in postmenopausal patients with advanced breast cancer previously treated with tamoxifen. Breast 2000, 9, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Tripathy, D.; Im, S.A.; Colleoni, M.; Franke, F.; Bardia, A.; Harbeck, N.; Hurvitz, S.A.; Chow, L.; Sohn, J.; Lee, K.S.; et al. Ribociclib plus endocrine therapy for premenopausal women with hormone-receptor-positive, advanced breast cancer (MONALEESA-7): A randomised phase 3 trial. Lancet Oncol. 2018, 19, 904–915. [Google Scholar] [CrossRef]
- Study of Efficacy and Safety in Premenopausal Women with Hormone Receptor Positive, HER2-Negative Advanced Breast Cancer Full Text View ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT02278120?term=ribociclib&cond=Breast+Cancer&draw=6&rank=43 (accessed on 9 January 2021).
- Ellis, M.J.; Llombart-Cussac, A.; Feltl, D.; Dewar, J.A.; Jasiówka, M.; Hewson, N.; Rukazenkov, Y.; Robertson, J.F.R. Fulvestrant 500 mg versus anastrozole 1 mg for the first-line treatment of advanced breast cancer: Overall survival analysis from the phase II first study. J. Clin. Oncol. 2015, 33, 3781–3786. [Google Scholar] [CrossRef] [PubMed]
- Dickler, M.N.; Barry, W.T.; Cirrincione, C.T.; Ellis, M.J.; Moynahan, M.E.; Innocenti, F.; Hurria, A.; Rugo, H.S.; Lake, D.E.; Hahn, O.; et al. Phase III trial evaluating letrozole as first-line endocrine therapy with or without bevacizumab for the treatment of postmenopausal women with hormone receptor-positive advanced-stage breast cancer: CALGB 40503 (Alliance). J. Clin. Oncol. 2016, 34, 2602–2609. [Google Scholar] [CrossRef] [PubMed]
- Huober, J.; Fasching, P.A.; Barsoum, M.; Petruzelka, L.; Wallwiener, D.; Thomssen, C.; Reimer, T.; Paepke, S.; Azim, H.A.; Ragosch, V.; et al. Higher efficacy of letrozole in combination with trastuzumab compared to letrozole monotherapy as first-line treatment in patients with HER2-positive, hormone-receptor-positive metastatic breast cancer Results of the eLEcTRA trial. Breast 2012, 21, 27–33. [Google Scholar] [CrossRef]
- Wolff, A.C.; Lazar, A.A.; Bondarenko, I.; Garin, A.M.; Brincat, S.; Chow, L.; Sun, Y.; Neskovic-Konstantinovic, Z.; Guimaraes, R.C.; Fumoleau, P.; et al. Randomized phase III placebo-controlled trial of letrozole plus oral temsirolimus as first-line endocrine therapy in postmenopausal women with locally advanced or metastatic breast cancer. J. Clin. Oncol. 2013, 31, 196–202. [Google Scholar] [CrossRef] [Green Version]
- Pritchard, K.I.; Burris, H.A.; Ito, Y.; Rugo, H.S.; Dakhil, S.; Hortobagyi, G.N.; Campone, M.; Csöszi, T.; Baselga, J.; Puttawibul, P.; et al. Safety and efficacy of everolimus with exemestane vs. Exemestane alone in elderly patients with HER2-negative, hormone receptor-positive breast cancer in BOLERO-2. Clin. Breast Cancer 2013, 13, 421–432.e8. [Google Scholar] [CrossRef] [Green Version]
- Falandry, C.; Debled, M.; Bachelot, T.; Delozier, T.; Crétin, J.; Romestaing, P.; Mille, D.; You, B.; Mauriac, L.; Pujade-Lauraine, E.; et al. Celecoxib and exemestane versus placebo and exemestane in postmenopausal metastatic breast cancer patients: A double-blind phase III GINECO study. Breast Cancer Res. Treat. 2009, 116, 501–508. [Google Scholar] [CrossRef]
- Martín, M.; Loibl, S.; Von Minckwitz, G.; Morales, S.; Martinez, N.; Guerrero, A.; Anton, A.; Aktas, B.; Schoenegg, W.; Muñoz, M.; et al. Phase III trial evaluating the addition of bevacizumab to endocrine therapy as first-line treatment for advanced breast cancer:The Letrozole/Fulvestrant and Avastin (LEA) study. J. Clin. Oncol. 2015, 33, 1045–1052. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, B.; Mackey, J.R.; Clemens, M.R.; Bapsy, P.P.; Vaid, A.; Wardley, A.; Tjulandin, S.; Jahn, M.; Lehle, M.; Feyereislova, A.; et al. Trastuzumab plus anastrozole versus anastrozole alone for the treatment of postmenopausal women with human epidermal growth factor receptor 2-positive, hormone receptor-positive metastatic breast cancer: Results from the randomized phase III TAnDEM study. J. Clin. Oncol. 2009, 27, 5529–5537. [Google Scholar] [CrossRef] [PubMed]
- Van Poznak, C.; Hannon, R.A.; Mackey, J.R.; Campone, M.; Apffelstaedt, J.P.; Clack, G.; Barlow, D.; Makris, A.; Eastell, R. Prevention of aromatase inhibitor-induced bone loss using risedronate: The SABRE trial. J. Clin. Oncol. 2010, 28, 967–975. [Google Scholar] [CrossRef] [PubMed]
- Markopoulos, C.; Tzoracoleftherakis, E.; Polychronis, A.; Venizelos, B.; Dafni, U.; Xepapadakis, G.; Papadiamantis, J.; Zobolas, V.; Misitzis, J.; Kalogerakos, K.; et al. Management of anastrozole-induced bone loss in breast cancer patients with oral risedronate: Results from the ARBI prospective clinical trial. Breast Cancer Res. 2010, 12, R24. [Google Scholar] [CrossRef] [Green Version]
- Wagner-Johnston, N.D.; Sloan, J.A.; Liu, H.; Kearns, A.E.; Hines, S.L.; Puttabasavaiah, S.; Dakhil, S.R.; Lafky, J.M.; Perez, E.A.; Loprinzi, C.L. 5-year follow-up of a randomized controlled trial of immediate versus delayed zoledronic acid for the prevention of bone loss in postmenopausal women with breast cancer starting letrozole after tamoxifen: N03CC (Alliance) trial. Cancer 2015, 121, 2537–2543. [Google Scholar] [CrossRef] [Green Version]
- Gnant, M.; Pfeiler, G.; Dubsky, P.C.; Hubalek, M.; Greil, R.; Jakesz, R.; Wette, V.; Balic, M.; Haslbauer, F.; Melbinger, E.; et al. Adjuvant denosumab in breast cancer (ABCSG-18): A multicentre, randomised, double-blind, placebo-controlled trial. Lancet 2015, 386, 433–443. [Google Scholar] [CrossRef]
- Taylor-Stokes, G.; Mitra, D.; Waller, J.; Gibson, K.; Milligan, G.; Iyer, S. Treatment patterns and clinical outcomes among patients receiving palbociclib in combination with an aromatase inhibitor or fulvestrant for HR+/HER2-negative advanced/metastatic breast cancer in real-world settings in the US: Results from the IRIS study. Breast 2019, 43, 22–27. [Google Scholar] [CrossRef] [Green Version]
- Ibrance Real World Insights Full Text View ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT03159195?term=palbociclib+PD-0332991&cond=Breast+Cancer&draw=15&rank=133 (accessed on 9 January 2021).
- Waller, J.; Mitra, D.; Mycock, K.; Taylor-Stokes, G.; Milligan, G.; Zhan, L.; Iyer, S. Real-world treatment patterns and clinical outcomes in patients receiving palbociclib for hormone receptor–positive, human epidermal growth factor receptor 2–negative advanced or metastatic breast cancer in Argentina: The IRIS study. J. Glob. Oncol. 2019, 2019. [Google Scholar] [CrossRef]
- Robertson, J.F.R.; Bondarenko, I.M.; Trishkina, E.; Dvorkin, M.; Panasci, L.; Manikhas, A.; Shparyk, Y.; Cardona-Huerta, S.; Cheung, K.L.; Philco-Salas, M.J.; et al. Fulvestrant 500 mg versus anastrozole 1 mg for hormone receptor-positive advanced breast cancer (FALCON): An international, randomised, double-blind, phase 3 trial. Lancet 2016, 388, 2997–3005. [Google Scholar] [CrossRef]
- Noguchi, S.; Ellis, M.J.; Robertson, J.F.R.; Thirlwell, J.; Fazal, M.; Shao, Z. Progression-free survival results in postmenopausal Asian women: Subgroup analysis from a phase III randomized trial of fulvestrant 500 mg vs anastrozole 1 mg for hormone receptor-positive advanced breast cancer (FALCON). Breast Cancer 2018, 25, 356–364. [Google Scholar] [CrossRef]
- A Global Study to Compare the Effects of Fulvestrant and Arimidex in a Subset of Patients with Breast Cancer. Study Results ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/results/NCT01602380?term=aromatase+inhibitors+phase+3&cond=Breast+Cancer&draw=17 (accessed on 14 November 2020).
- Howell, A.; Pippen, J.; Elledge, R.M.; Mauriac, L.; Vergote, I.; Jones, S.E.; Come, S.E.; Osborne, C.K.; Robertson, J.F.R. Fulvestrant versus anastrozole for the treatment of advanced breast carcinoma: A prospectively planned combined survival analysis of two multicenter trials. Cancer 2005, 104, 236–239. [Google Scholar] [CrossRef] [PubMed]
- Martin, M.; Zielinski, C.; Ruiz-Borrego, M.; Carrasco, E.; Turner, N.; Ciruelos, E.M.; Muñoz, M.; Bermejo, B.; Margeli, M.; Anton, A.; et al. Palbociclib in combination with endocrine therapy versus capecitabine in hormonal receptor-positive, human epidermal growth factor 2-negative, aromatase inhibitor-resistant metastatic breast cancer: A phase III randomised controlled trial-PEARL. Ann. Oncol. 2020. [Google Scholar] [CrossRef]
- Johnston, S.R.D.; Kilburn, L.S.; Ellis, P.; Dodwell, D.; Cameron, D.; Hayward, L.; Im, Y.H.; Braybrooke, J.P.; Brunt, A.M.; Cheung, K.L.; et al. Fulvestrant plus anastrozole or placebo versus exemestane alone after progression on non-steroidal aromatase inhibitors in postmenopausal patients with hormone-receptor-positive locally advanced or metastatic breast cancer (SoFEA): A composite, multicentre, phase 3 randomised trial. Lancet Oncol. 2013, 14, 989–998. [Google Scholar] [CrossRef] [Green Version]
- Chia, S.; Gradishar, W.; Mauriac, L.; Bines, J.; Amant, F.; Federico, M.; Fein, L.; Romieu, G.; Buzdar, A.; Robertson, J.F.R.; et al. Double-blind, randomized placebo controlled trial of fulvestrant compared with exemestane after prior nonsteroidal aromatase inhibitor therapy in postmenopausal women with hormone receptor-positive, advanced breast cancer: Rsults from EFECT. J. Clin. Oncol. 2008, 26, 1664–1670. [Google Scholar] [CrossRef] [PubMed]
- Paridaens, R.J.; Dirix, L.Y.; Beex, L.V.; Nooij, M.; Cameron, D.A.; Cufer, T.; Piccart, M.J.; Bogaerts, J.; Therasse, P. Phase III study comparing exemestane with tamoxifen as first-line hormonal treatment of metastatic breast cancer in postmenopausal women: The European Organisation for Research and Treatment of Cancer Breast Cancer Cooperative Group. J. Clin. Oncol. 2008, 26, 4883–4890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, R.S.; Barlow, W.E.; Albain, K.S.; Vandenberg, T.A.; Dakhil, S.R.; Tirumali, N.R.; Lew, D.L.; Hayes, D.F.; Gralow, J.R.; Livingston, R.B.; et al. Combination Anastrozole and Fulvestrant in Metastatic Breast Cancer. N. Engl. J. Med. 2012, 367, 435–444. [Google Scholar] [CrossRef] [Green Version]
- Iwata, H.; Masuda, N.; Ohno, S.; Rai, Y.; Sato, Y.; Ohsumi, S.; Hashigaki, S.; Nishizawa, Y.; Hiraoka, M.; Morimoto, T.; et al. A randomized, double-blind, controlled study of exemestane versus anastrozole for the first-line treatment of postmenopausal Japanese women with hormone-receptor-positive advanced breast cancer. Breast Cancer Res. Treat. 2013, 139, 441–451. [Google Scholar] [CrossRef] [Green Version]
- Xu, B.; Jiang, Z.; Shao, Z.; Wang, J.; Feng, J.; Song, S.; Chen, Z.; Gu, K.; Yu, S.; Zhang, Y.; et al. Fulvestrant 250 mg versus anastrozole for Chinese patients with advanced breast cancer: Results of a multicentre, double-blind, randomised phase III trial. Cancer Chemother. Pharmacol. 2011, 67, 223–230. [Google Scholar] [CrossRef]
- Bergh, J.; Jönsson, P.E.; Lidbrink, E.K.; Trudeau, M.; Eiermann, W.; Brattström, D.; Lindemann, J.P.O.; Wiklund, F.; Henriksson, R. FACT: An open-label randomized phase III study of fulvestrant and anastrozole in combination compared with anastrozole alone as first-line therapy for patients with receptor-positive postmenopausal breast cancer. J. Clin. Oncol. 2012, 30, 1919–1925. [Google Scholar] [CrossRef]
- A Study of Abemaciclib (LY2835219) in Participants with Breast Cancer Study Results ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/results/NCT02763566?term=aromatase+inhibitors+phase+3&cond=Breast+Cancer&draw=8&rank=66 (accessed on 14 November 2020).
- Palbociclib Plus Letrozole For Postmenopausal Women with HR(+) HER2(-) Advanced Breast Cancer For Whom Letrozole is Deemed Appropriate Full Text View ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT02600923?term=NCT02600923&draw=2&rank=1 (accessed on 14 November 2020).
- Mehta, R.S.; Barlow, W.E.; Albain, K.S.; Vandenberg, T.A.; Dakhil, S.R.; Tirumali, N.R.; Lew, D.L.; Hayes, D.F.; Gralow, J.R.; Linden, H.M.; et al. Overall Survival with Fulvestrant plus Anastrozole in Metastatic Breast Cancer. N. Engl. J. Med. 2019, 380, 1226–1234. [Google Scholar] [CrossRef]
- Exemestane Compared with Tamoxifen in Treating Women with Locally Recurrent or Metastatic Breast Cancer Full Text View ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT00002777?term=aromatase+inhibitors+phase+3&cond=Breast+Cancer&draw=22 (accessed on 14 November 2020).
- Study of Efficacy and Safety of LEE011 in Postmenopausal Women with Advanced Breast Cancer.(MONALEESA-2) Full Text View ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT01958021?term=NCT01958021&draw=2&rank=1 (accessed on 12 November 2020).
- A Study of Palbociclib (PD-0332991) + Letrozole vs. Letrozole for 1st Line Treatment of Postmenopausal Women with ER+/HER2- Advanced Breast Cancer (PALOMA-2) Study Results ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/results/NCT01740427?term=NCT01740427&draw=2&rank=1 (accessed on 14 November 2020).
- A Study of Nonsteroidal Aromatase Inhibitors Plus Abemaciclib (LY2835219) in Postmenopausal Women with Breast Cancer Study Results ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/results/NCT02246621?term=NCT02246621&draw=2 (accessed on 14 November 2020).
- Anastrozole Monotherapy versus Maximal Oestrogen Blockade with Anastrozole and Fulvestrant Combination Therapy Study Results ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/results/NCT00256698?term=aromatase+inhibitors+phase+3&cond=Breast+Cancer&draw=19&rank=179&view=results (accessed on 14 November 2020).
- Aromasin vs. Arimidex Study as Initial Hormonal Therapy in Postmenopausal Women with Advanced/Recurrent Breast Cancer Study Results ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/results/NCT00143390?term=exemestane+phase+3&cond=Breast+Cancer&draw=6&rank=44 (accessed on 14 November 2020).
- S0226 Anastrozole with or without Fulvestrant as First-Line Therapy in Postmenopausal Women with Metastatic Breast Cancer Study Results ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/results/NCT00075764?term=aromatase+inhibitors+phase+3&cond=Breast+Cancer&draw=13&view=results (accessed on 14 November 2020).
- Faslodex Advanced Breast Cancer Local Chinese Study Full Text View ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT00327769?term=anastrozole+phase+3&cond=Breast+Cancer&draw=5&rank=39 (accessed on 14 November 2020).
- Phase III Palbociclib with Endocrine Therapy vs. Capecitabine in HR+/HER2–MBC with Resistance to Aromatase Inhibitors Full Text View ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/study/NCT02028507?term=palbociclib+PD-0332991&cond=Breast+Cancer&draw=10%5C (accessed on 9 January 2021).
- Zhang, Q.Y.; Sun, T.; Yin, Y.M.; Li, H.P.; Yan, M.; Tong, Z.S.; Oppermann, C.P.; Liu, Y.P.; Costa, R.; Li, M.; et al. MONARCH plus: Abemaciclib plus endocrine therapy in women with HR+/HER2– advanced breast cancer: The multinational randomized phase III study. Ther. Adv. Med. Oncol. 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Crew, K.D.; Greenlee, H.; Capodice, J.; Raptis, G.; Brafman, L.; Fuentes, D.; Sierra, A.; Hershman, D.L. Prevalence of joint symptoms in postmenopausal women taking aromatase inhibitors for early-stage breast cancer. J. Clin. Oncol. 2007, 25, 3877–3883. [Google Scholar] [CrossRef] [PubMed]
- Dongsheng, H.; Ling, B.; Jun, Z.; Yinghui, T.; Qingwei, Z.; Jing, C.; Xiaoyang, L. Incidence of menopausal symptoms in postmenopausal breast cancer patients treated with aromatase inhibitors. Oncotarget 2017, 8, 40558–40567. [Google Scholar] [CrossRef] [Green Version]
- Morales, L.; Pans, S.; Paridaens, R.; Westhovens, R.; Timmerman, D.; Verhaeghe, J.; Wildiers, H.; Leunen, K.; Amant, F.; Berteloot, P.; et al. Debilitating musculoskeletal pain and stiffness with letrozole and exemestane: Associated tenosynovial changes on magnetic resonance imaging. Breast Cancer Res. Treat. 2007, 104, 87–91. [Google Scholar] [CrossRef]
- Oesterreich, S.; Henry, N.L.; Kidwell, K.M.; Van Poznak, C.H.; Skaar, T.C.; Dantzer, J.; Li, L.; Hangartner, T.N.; Peacock, M.; Nguyen, A.T.; et al. Associations between genetic variants and the effect of letrozole and exemestane on bone mass and bone turnover. Breast Cancer Res. Treat. 2015, 154, 263–273. [Google Scholar] [CrossRef] [Green Version]
- Castel, L.D.; Hartmann, K.E.; Mayer, I.A.; Saville, B.R.; Alvarez, J.; Boomershine, C.S.; Abramson, V.G.; Chakravarthy, A.B.; Friedman, D.L.; Cella, D.F. Time course of arthralgia among women initiating aromatase inhibitor therapy and a postmenopausal comparison group in a prospective cohort. Cancer 2013, 119, 2375–2382. [Google Scholar] [CrossRef]
- Laroche, F.; Coste, J.; Medkour, T.; Cottu, P.H.; Pierga, J.Y.; Lotz, J.P.; Beerblock, K.; Tournigand, C.; Declèves, X.; De Cremoux, P.; et al. Classification of and risk factors for estrogen deprivation pain syndromes related to aromatase inhibitor treatments in women with breast cancer: A prospective multicenter cohort study. J. Pain 2014, 15, 293–303. [Google Scholar] [CrossRef]
- Henry, N.L.; Giles, J.T. Vered Stearns Aromatase inhibitor-associated musculoskeletal symptoms: Etiology and strategies for management. Breast Cancer 2008, 22, 12. [Google Scholar]
- Geisler, J.; Haynes, B.; Anker, G.; Dowsett, M.; Lønning, P.E. Influence of Letrozole and Anastrozole on Total Body Aromatization and Plasma Estrogen Levels in Postmenopausal Breast Cancer Patients Evaluated in a Randomized, Cross-Over Study. J. Clin. Oncol. 2002, 20, 751–757. [Google Scholar] [CrossRef]
- Ushiyama, T.; Ueyama, H.; Inoue, K.; Ohkubo, I.; Hukuda, S. Expression of genes for estrogen receptors α and β in human articular chondrocytes. Osteoarthr. Cartil. 1999, 7, 560–566. [Google Scholar] [CrossRef] [Green Version]
- Coleman, R.E.; Bolten, W.W.; Lansdown, M.; Dale, S.; Jackisch, C.; Merkel, D.; Maass, N.; Hadji, P. Aromatase inhibitor-induced arthralgia: Clinical experience and treatment recommendations. Cancer Treat. Rev. 2008, 34, 275–282. [Google Scholar] [CrossRef]
- Felson, D.T.; Cummings, S.R. Aromatase inhibitors and the syndrome of arthralgias with estrogen deprivation. Arthritis Rheum. 2005, 52, 2594–2598. [Google Scholar] [CrossRef]
- Nevitt, M.C.; Cummings, S.R.; Lane, N.E.; Hochberg, M.C.; Scott, J.C.; Pressman, A.R.; Genant, H.K.; Cauley, J.A. Association of estrogen replacement therapy with the risk of osteoarthritis of the hip in elderly white women. Arch. Intern. Med. 1996, 156, 2073–2080. [Google Scholar] [CrossRef]
- Spector, T.D.; Nandra, D.; Hart, D.J.; Doyle, D.V. Is hormone replacement therapy protective for hand and knee osteoarthritis in women?: The Chingford Study. Ann. Rheum. Dis. 1997, 56, 432–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jingxuan, W.; Qingyuan, Z.; Shi, J.; Meiyan, F.; Xinmei, K.; Shu, Z.; Shuling, L.; Wenhui, Z. Immoderate inhibition of estrogen by anastrozole enhances the severity of experimental polyarthritis. Exp. Gerontol. 2009, 44, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Zarkavelis, G.; Kollas, A.; Kampletsas, E.; Vasiliou, V.; Kaltsonoudis, E.; Drosos, A.; Khaled, H.; Pavlidis, N. Aromatase inhibitors induced autoimmune disorders in patients with breast cancer: A review. J. Adv. Res. 2016, 7, 719–726. [Google Scholar] [CrossRef] [Green Version]
- Morel, B.; Marotte, H.; Miossec, P. Will steroidal aromatase inhibitors induce rheumatoid arthritis? Ann. Rheum. Dis. 2007, 66, 557–558. [Google Scholar] [CrossRef] [Green Version]
- Laroche, M.; Seniow, M.; Roche, H.; Ruyssen-Witrand, A. Arthralgia associated with autoimmune abnormalities under aromatase inhibitor therapy: Outcome after cessation of treatment. J. Rheumatol. 2016, 43, 1945–1946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szekanecz, Z.; Gomez, I.; Soós, B.; Bodoki, L.; Szamosi, S.; András, C.; Juhász, B.; Váróczy, L.; Antal-Szalmás, P.; Szodoray, P.; et al. Eight pillars of oncorheumatology: Crossroads between malignancies and musculoskeletal diseases. Autoimmun. Rev. 2020, 19, 102658. [Google Scholar] [CrossRef] [PubMed]
- Carlsten, H. Immune responses and bone loss: The estrogen connection. Immunol. Rev. 2005, 208, 194–206. [Google Scholar] [CrossRef]
- Murphy, C.G.; Dickler, M.N. The Role of CDK4/6 Inhibition in Breast Cancer. Oncologist 2015, 20, 483–490. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Wang, L.; Wu, C.; Sun, S.; Pan, J.H. E2F2 directly regulates the STAT1 and PI3K/AKT/NF-κB pathways to exacerbate the inflammatory phenotype in rheumatoid arthritis synovial fibroblasts and mouse embryonic fibroblasts. Arthritis Res. Ther. 2018, 20, 225. [Google Scholar] [CrossRef] [Green Version]
- Zhang, R.; Wang, L.; Pan, J.H.; Han, J. A critical role of E2F transcription factor 2 in proinflammatory cytokines-dependent proliferation and invasiveness of fibroblast-like synoviocytes in rheumatoid Arthritis. Sci. Rep. 2018, 8. [Google Scholar] [CrossRef] [Green Version]
- Park, I.H.; Lee, Y.S.; Lee, K.S.; Kim, S.Y.; Hong, S.H.; Jeong, J.; Lee, H.; Ro, J.; Nam, B.H. Single nucleotide polymorphisms of CYP19A1 predict clinical outcomes and adverse events associated with letrozole in patients with metastatic breast cancer. Cancer Chemother. Pharmacol. 2011, 68, 1263–1271. [Google Scholar] [CrossRef]
- Fontein, D.B.Y.; Houtsma, D.; Nortier, J.W.R.; Baak-Pablo, R.F.; Kranenbarg, E.M.K.; Van Der Straaten, T.R.J.H.M.; Putter, H.; Seynaeve, C.; Gelderblom, H.; Van De Velde, C.J.H.; et al. Germline variants in the CYP19A1 gene are related to specific adverse events in aromatase inhibitor users: A substudy of Dutch patients in the TEAM trial. Breast Cancer Res. Treat. 2014, 144, 599–606. [Google Scholar] [CrossRef]
- Mao, J.J.; Su, H.I.; Feng, R.; Donelson, M.L.; Aplenc, R.; Rebbeck, T.R.; Stanczyk, F.; DeMichele, A. Association of functional polymorphisms in CYP19A1 with aromatase inhibitor associated arthralgia in breast cancer survivors. Breast Cancer Res. 2011, 13. [Google Scholar] [CrossRef] [Green Version]
- Napoli, N.; Rastelli, A.; Ma, C.; Yarramaneni, J.; Vattikutti, S.; Moskowitz, G.; Giri, T.; Mueller, C.; Kulkarny, V.; Qualls, C.; et al. Genetic polymorphism at Val80 (rs700518) of the CYP19A1 gene is associated with aromatase inhibitor associated bone loss in women with ER (+) breast cancer. Bone 2013, 55, 309–314. [Google Scholar] [CrossRef] [Green Version]
- Leyland-Jones, B.; Gray, K.P.; Abramovitz, M.; Bouzyk, M.; Young, B.; Long, B.; Kammler, R.; Dell’Orto, P.; Biasi, M.O.; Thürlimann, B.; et al. ESR1 and ESR2 polymorphisms in the BIG 1-98 trial comparing adjuvant letrozole versus tamoxifen or their sequence for early breast cancer. Breast Cancer Res. Treat. 2015, 154, 543–555. [Google Scholar] [CrossRef] [PubMed]
- Henry, N.L.; Skaar, T.C.; Dantzer, J.; Li, L.; Kidwell, K.; Gersch, C.; Nguyen, A.T.; Rae, J.M.; Desta, Z.; Oesterreich, S.; et al. Genetic associations with toxicity-related discontinuation of aromatase inhibitor therapy for breast cancer. Breast Cancer Res. Treat. 2013, 138, 807–816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Giralt, N.; Rodríguez-Sanz, M.; Prieto-Alhambra, D.; Servitja, S.; Torres-Del Pliego, E.; Balcells, S.; Albanell, J.; Grinberg, D.; Diez-Perez, A.; Tusquets, I.; et al. Genetic determinants of aromatase inhibitor-related arthralgia: The B-ABLE cohort study. Breast Cancer Res. Treat. 2013, 140, 385–395. [Google Scholar] [CrossRef]


{kind=link}
| Reference | Trial | Treatment Arms | Study Sample | Median Age | Median Follow-Up | PFS | OR | Bone Mets (%) | Arthralgia (%) | Myalgia (%) | Bone Pain (%) | Back Pain (%) | Osteoporosis (%) | Fracture (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Johnston et al. 2013 [46] | SOFEA (NCT00253422, NCT00944918) | fulvestrant plus anastrozole vs. fulvestrant plus placebo vs. exemestane | 723 (243/231/249) | 63.8/63.4/66 | 37.9 | 4.4 vs. 4.8 (H: 1.0) | 7% vs. 7% p = 0.88 | 15/16/13 | 40/43/47 | 4/2/2 | 9/6/7 | 7/10/7 | NR | NR |
| 4.8 vs. 3.4 (H: 0.95) | 7% vs. 4% p = 0. 27 | |||||||||||||
| Chia et al. 2007 [47] | EFECT (NCT00065325) | fulvestrant vs. exemestane | 693 (351/342) | 63/63 | 13 | 3.7/3.7 H: 0.93 | 7.4% vs. 6.7%; p = 0.73 | 67.2/66.4 | 3.7/5.6 | 4/4.1 | NR | NR | NR | NR |
| Robertson JFR et al. 2016 [41,43] | FALCON (NCT01602380) | fulvestrant vs. anastrozole | 462 (230/232) | 63.8/63.3 | 16.6 vs. 13.8; H: 0.797 | 46.1% vs. 44.9%; p = 0.729 | 10/10 (bone only) | 16.6/10.3 | 7/3.4 | NR | 9.2/6 | NR | NR | |
| Bergh J et al. 2012 [52,60] | FACT (NCT00256698) | fulvestrant plus anastrozole vs. anastrozole | 514 (258/256) | 65.2/63.4 | 8.9 | 10.8 vs. 10.2; H: 0.99 | 31.8 vs. 33.6; p = 0.76 | 63/71 (bone only) | 12.1/10.6 | NR | NR | 5/5.9 | NR | NR |
| Paridaens RJ et al. 200 [48,56] | EORTC (NCT00002777) | exemestane vs. tamoxifen | 371 (182/189) | 63/62 | 29 | 9.9 vs. 5.8; H: | 46% vs. 31%; p = 0.005 | 35.1/35.4 | 11.5/5.3 | NR | 32.9/34.9 | NR | NR | NR |
| Mehta RS et al. 2012 et 2019 [49,55,62] | SWOG TRIAL S0226 (NCT00075764) | anastrozole vs. anastrozole plus fulvestrant | 694 (345/349) | 65/65 | 84 | 13.5 vs. 15; H: 0.81 | Median OS: 49.8 vs. 42; H: 0.82 | 22/21.5 (bone only) | 45.1/44.5 | 23.7/22.9 | 27.8/32.7 | 40/38.2 | NR | 0.2/0.5 |
| Iwata et al. 2013 [50,61] | NCT00143390 | exemestane vs. anastrozole | 298 (149/149) | 63.4/64 | NR | 13.8 vs. 11.1; H: 1.007 | 43.9% vs. 39.1%; | 26.8/26.8 (bone only) | 18.7/21.4 | 2.6/5.3 | NR | 11.4/14.7 | NR | 0/0.6 |
| Xu B et al. 2011 [51,63] | NCT00327769 | fulvestrant vs. anastrozole | 234 (121/113) | 53.4/54.8 | 3.6 vs. 5.3; H: 1.31 | 10% vs. 14%; p = 0.343 | 4/1 | NR | NR | 1/6 | NR | NR | ||
| Howell A et al. 2005 [44] | Trial 0020 Trial 0021 | fulvestrant vs. anastrozole | 851 (428/423) | 63/63 | 27 | 5.5 vs. 4.1 (H, 0.95; p = 0.48) | 27.4 vs. 27.7; (H: 0.98; p = 0.809) | 19.9/19.6 (bone only) | 8.3/12.8 | NR | NR | NR | NR | NR |
| Reference | Trial | Treatment Arms | Study Sample | Median Age | Median Follow-Up | PFS | OR | Bone Mets Only | Arthralgia (%) | Myalgia (%) | Bone Pain (%) | Back Pain (%) | Osteoporosis (%) | Fracture (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Richard S. Finn et al. 2016 [10,58] | PALOMA-2 (NCT01740427) | palbociclib plus letrozole vs. letrozole plus placebo | 666 (444/222) | 62/61 | 23 | 24.8/14.5 (H: 0.58; p < 0.001) | 42.1/34.7 (p = 0.06) | 23.2/21.6 | 33.3/33.8 | 11.9/9 | 8.5/9 | 21.6/21.6 | NR | 0.45/0 |
| Martin et al. 2020 [45,64] | PEARL (NCT02028507) | Cohort 1: palbociclib plus exemestane vs. capecitabine Cohort 2: palbociclib plus fulvestrant vs. capecitabine | 296 (153/143) 305 (149/156) | 60/60 62/60 | 18.9 * 13.5 | 8 * vs. 10.6 (H: 1.11; p = 0.404) 7.5 vs. 10 (H: 1.13; p = 0.398) | NR | NR | NR | NR | NR | NR | NR | NR |
| G.N. Hortobagyi et al. 2016 [9,57] | MONALEESA-2 (NCT01958021) | ribociclib plus letrozole vs. placebo plus letrozole | 668 (334/334) | 62/63 | 26.4 | 25.3/16 (H: 0.568) | 42.5/28.7; H: 0.746 | 20.7/23.4 | 27.5/28.8 | 6.5/6.3 | 7.1/10.6 | 20.6/17.8 | NR | 0/0.3 |
| Tripathy et al. 2018 [24,25] | MONALEESA-7 (NCT02278120) | ribociclib plus tamoxifen/NSAI plus goserelin Vs placebo plus tamoxifen/NSAI plus goserelin | 672 (335/337) | 42.6/43.7 | 19.2 | 23.8 vs. 13 (H: 0·55, p < 0·0001) | NR | 24.2/23.1 | 29.85/27.3 | 10.1/11 | 8/9.5 | 18.5/19.6 | NR | 0.3/0.3 |
| Matthew P. Goetz, 2017 [11,59] | MONARCHE-3 (NCT02246621) | abemaciclib plus anastrozole or letrozole vs. placebo plus anastrozole or letrozole | 493 (328/165) | 63/63 | 26 | Not reached vs. 14.7; H: 0.54 | 48.2/34.5 | 21.3/23.6 | 12.8/16.7 | 8.5/5.5 | 7.9/7.45 | 12.2/14.9 | NR | NR |
| NCT02763566 [53,65] | MONARCHE PLUS | abemaciclib plus NSAI vs. placebo plus NSAI or abemaciclib plus fulvestrant vs. placebo plus fulvestrant | 463 (207/99/104/53) | 56/59/55/58 | 26 | Not reached vs. 14.7; H: 0.49 | 56/30 (p < 0.0001) | NR | 5.8/13.1 | 4.8/5 | 2.9/5 | 7.8/9 | NR | NR |
| 11.47 vs. 5.59; H: 0.37 | 38.5/7.5 (p < 0.0001) | 6.7/5.6 | 1.9/0 | 0.9/1.8 | 4.8/5.6 | |||||||||
| NCT02600923 [54] | palbociclib plus letrozole | 131 | NR | NR | NR | NR | NR | 20 | 6.1 | NR | 17.6 | NR | NR |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andrikopoulou, A.; Fiste, O.; Liontos, M.; Dimopoulos, M.-A.; Zagouri, F. Aromatase and CDK4/6 Inhibitor-Induced Musculoskeletal Symptoms: A Systematic Review. Cancers 2021, 13, 465. https://doi.org/10.3390/cancers13030465
Andrikopoulou A, Fiste O, Liontos M, Dimopoulos M-A, Zagouri F. Aromatase and CDK4/6 Inhibitor-Induced Musculoskeletal Symptoms: A Systematic Review. Cancers. 2021; 13(3):465. https://doi.org/10.3390/cancers13030465
Chicago/Turabian StyleAndrikopoulou, Angeliki, Oraianthi Fiste, Michalis Liontos, Meletios-Athanasios Dimopoulos, and Flora Zagouri. 2021. "Aromatase and CDK4/6 Inhibitor-Induced Musculoskeletal Symptoms: A Systematic Review" Cancers 13, no. 3: 465. https://doi.org/10.3390/cancers13030465
APA StyleAndrikopoulou, A., Fiste, O., Liontos, M., Dimopoulos, M. -A., & Zagouri, F. (2021). Aromatase and CDK4/6 Inhibitor-Induced Musculoskeletal Symptoms: A Systematic Review. Cancers, 13(3), 465. https://doi.org/10.3390/cancers13030465