
Age-Related Biology of Early-Stage Operable Breast Cancer and Its Impact on Clinical Outcome


 , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
- 1.
- Explore the natural progression, if any, of the change in the biological characteristics according to age as a whole. Given that the ER positive and ER negative phenotypes show completely distinct clinical behaviours, their biological characteristics were also compared and assessed according to age.
- 2.
- Compare clinical outcomes of the patients in different age groups, if significant changes in their biological characteristics were found.
- 3.
- Compare the treatment patterns, if significant differences in clinical outcome were found.
2. Results
2.1. Biological Features
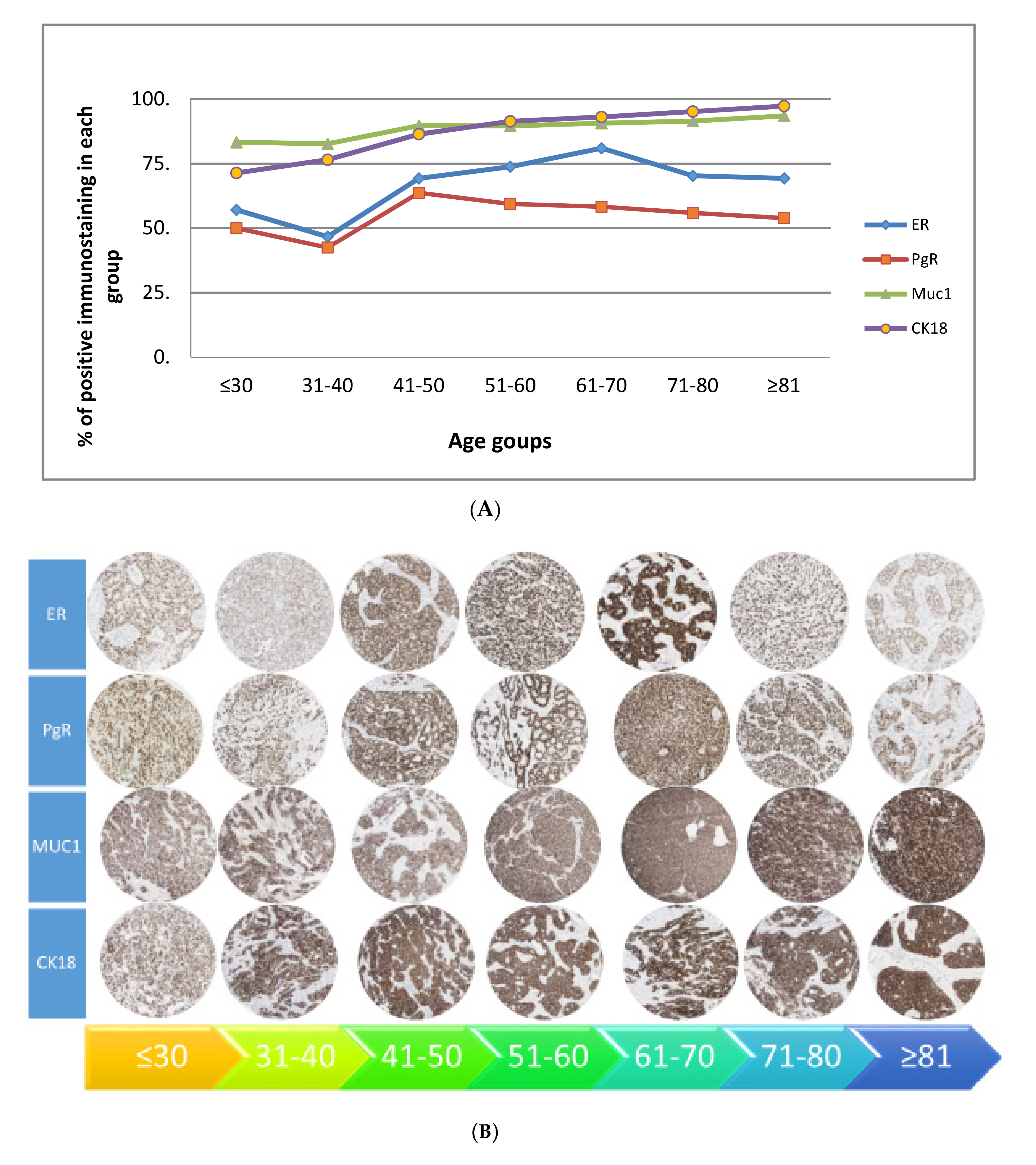
2.1.1. Overall Pattern of Biomarkers
- 4.
- A gradual rise starting at 40 years—ER, PgR, MUC1 and CK18.
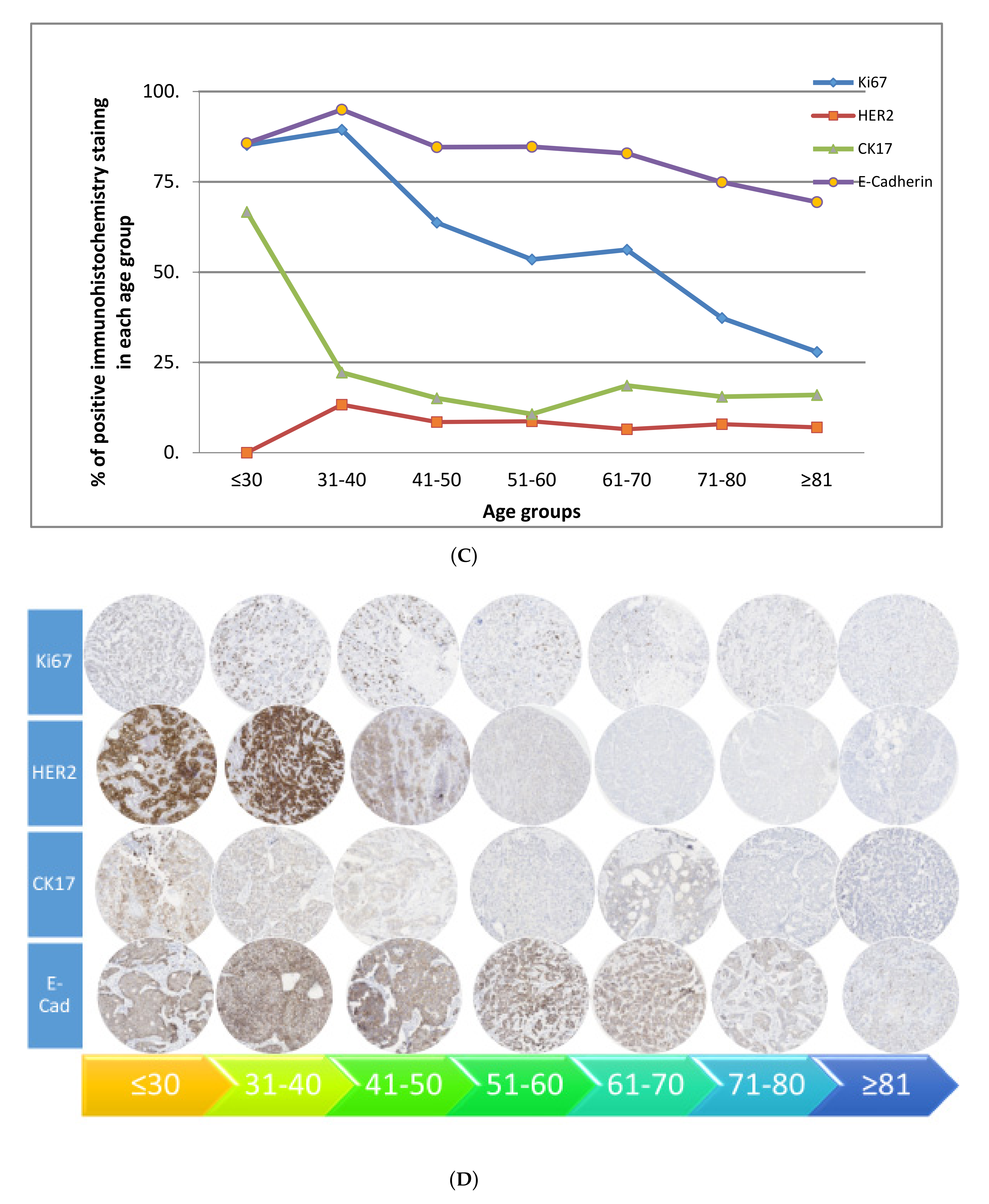
- 5.
- A gradual decline starting at 40 years—Ki67, HER2, CK17 and E-cadherin.
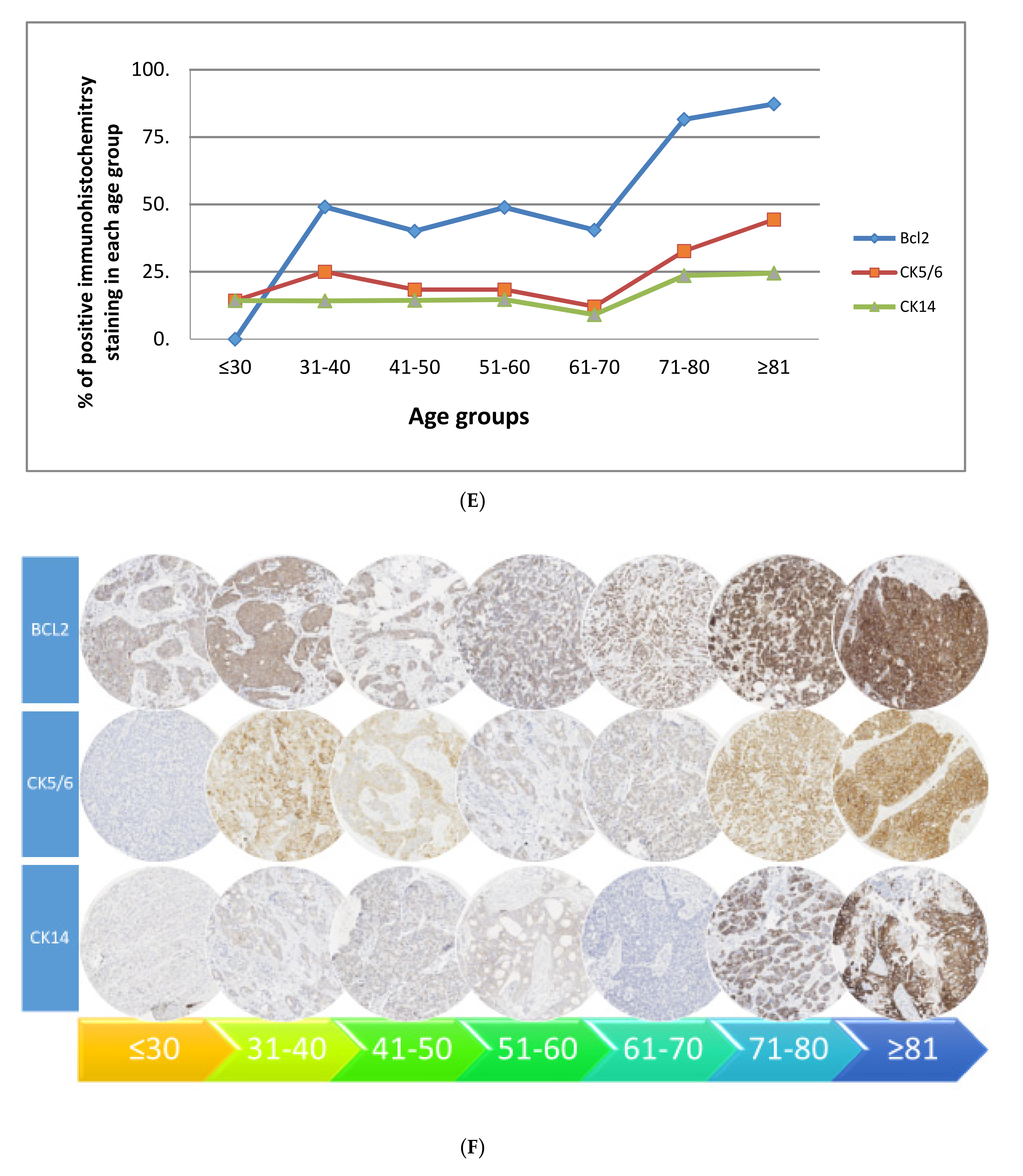
- 6.
- A rise at 70 years—bcl2, CK5/6 and CK14.
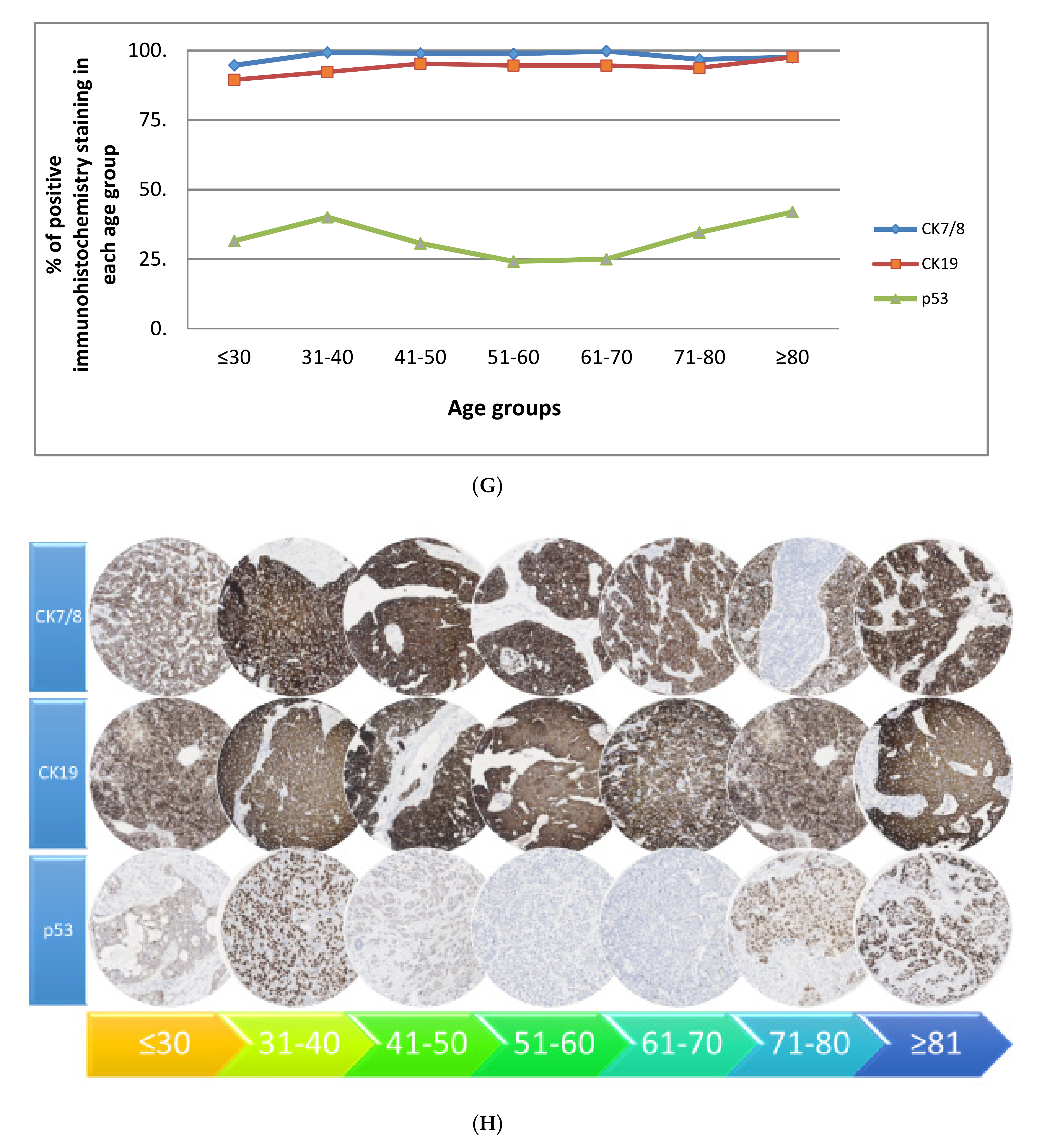
- 7.
- Two peaks—CK7/8, CK19 and p53 (i.e., peak at 40 years then decline, rising again at 70 years).
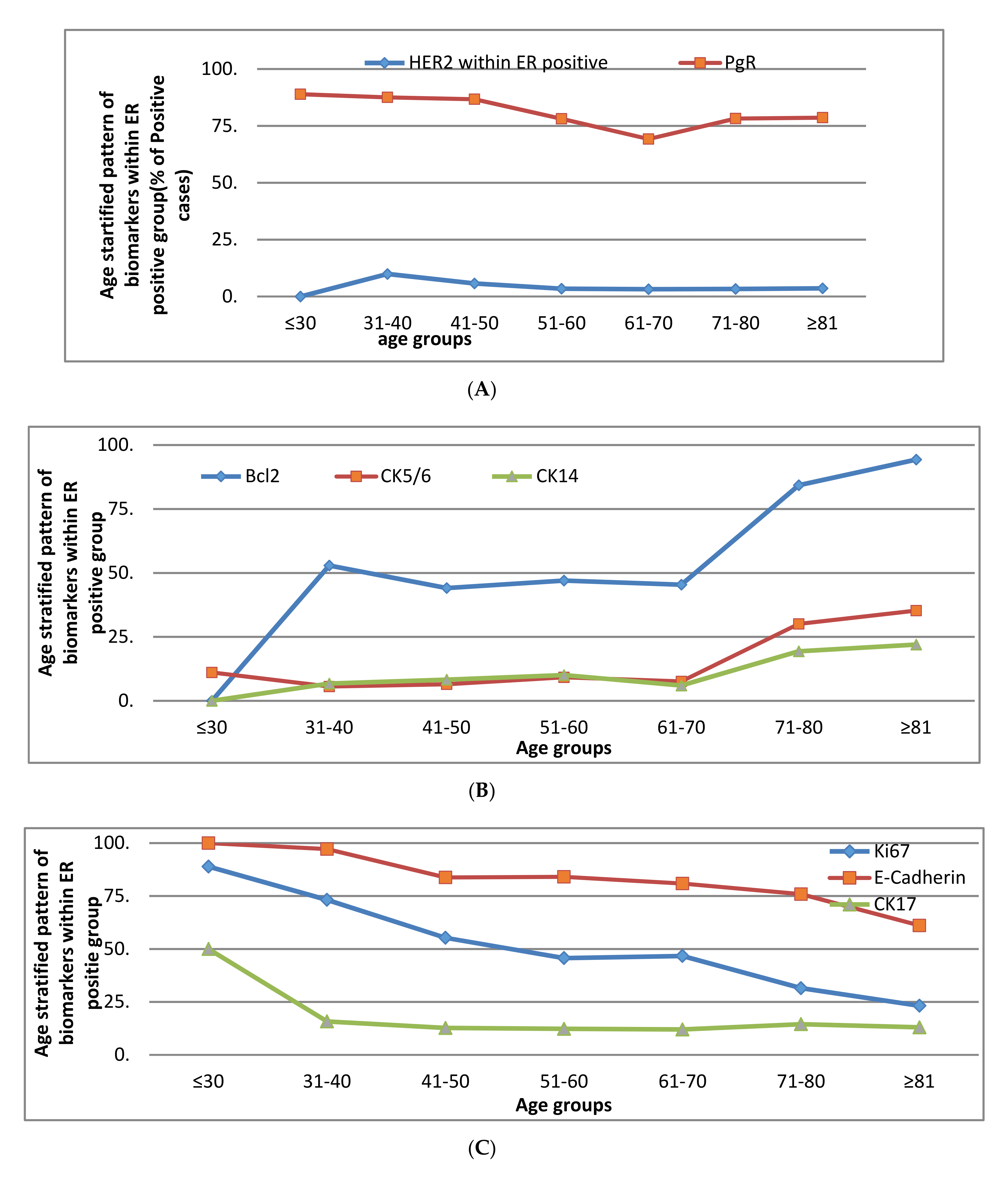
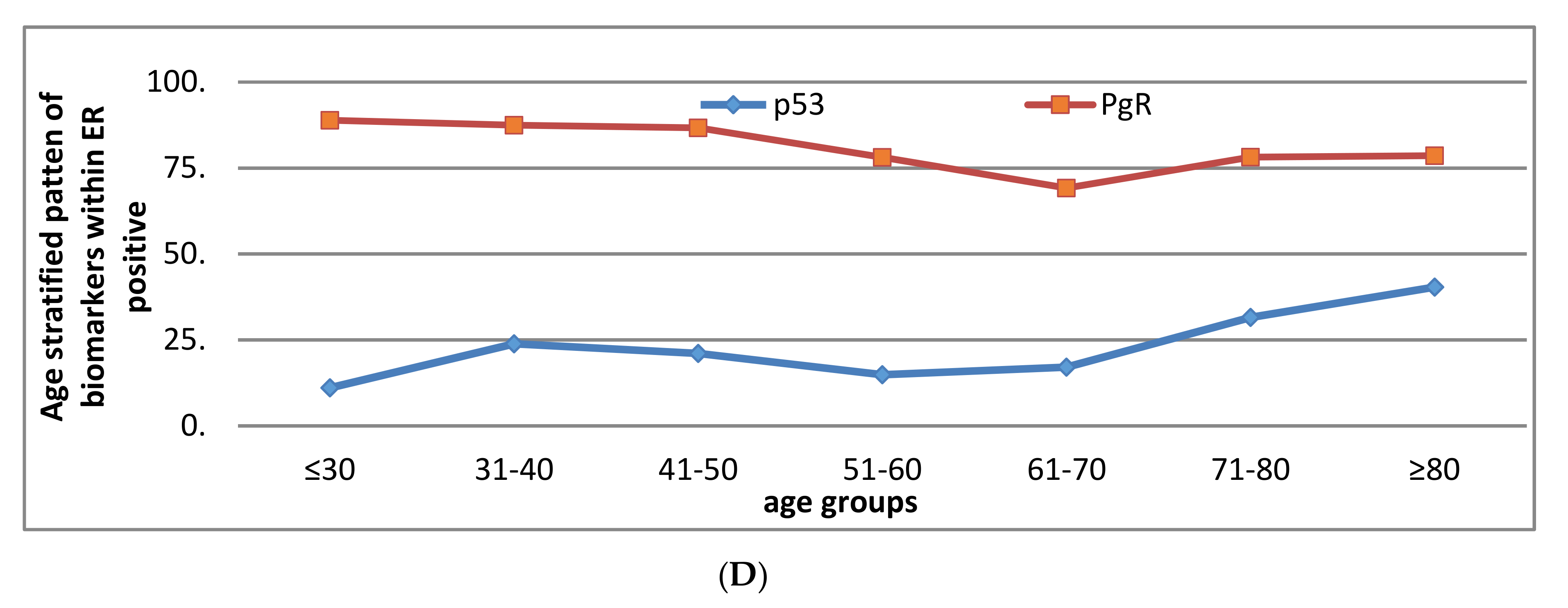
2.1.2. Pattern of Biomarkers According to ER Status
ER Positive Group
- a.
- A rise at 40 years—HER2
- b.
- A rise at 70 years—bcl2, CK5/6, CK14
- c.
- Decline with advancing age—Ki67, E-cadherin
- d.
- Two peaks—p53 and PgR (at 40 and 70 years)
- e.
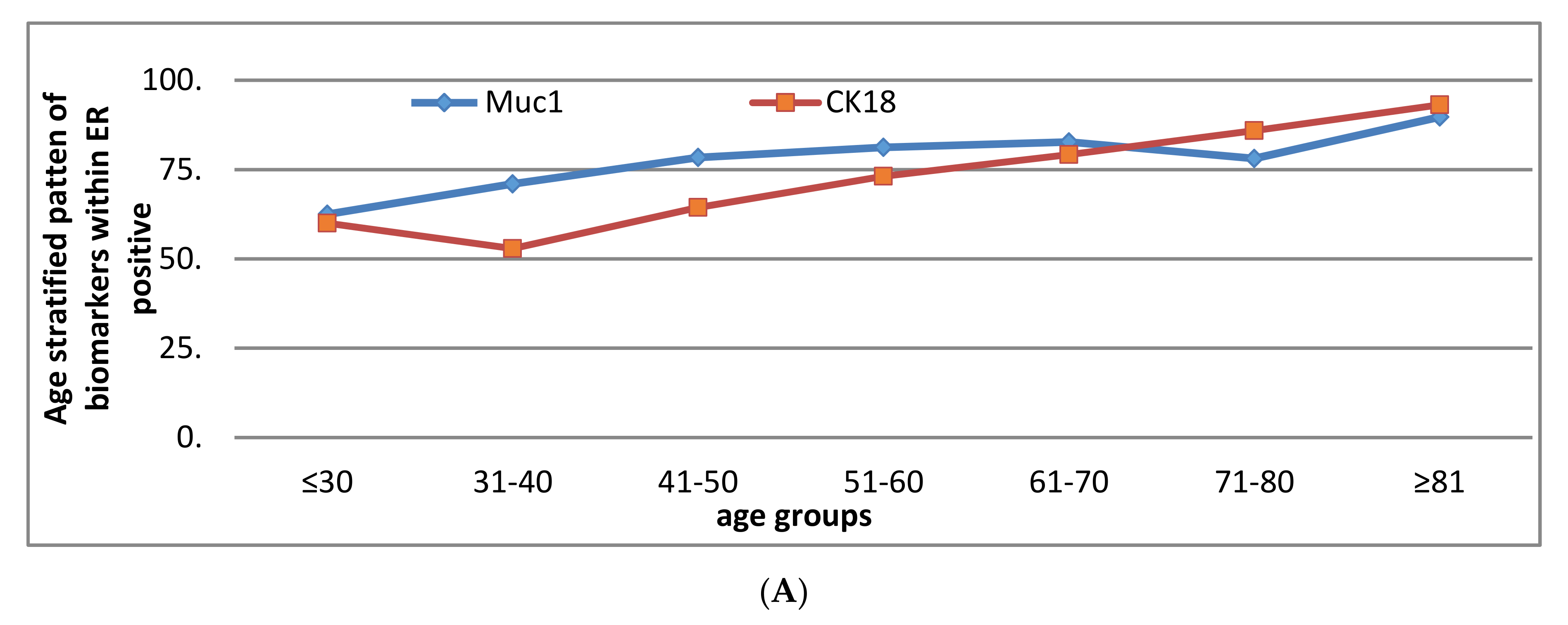
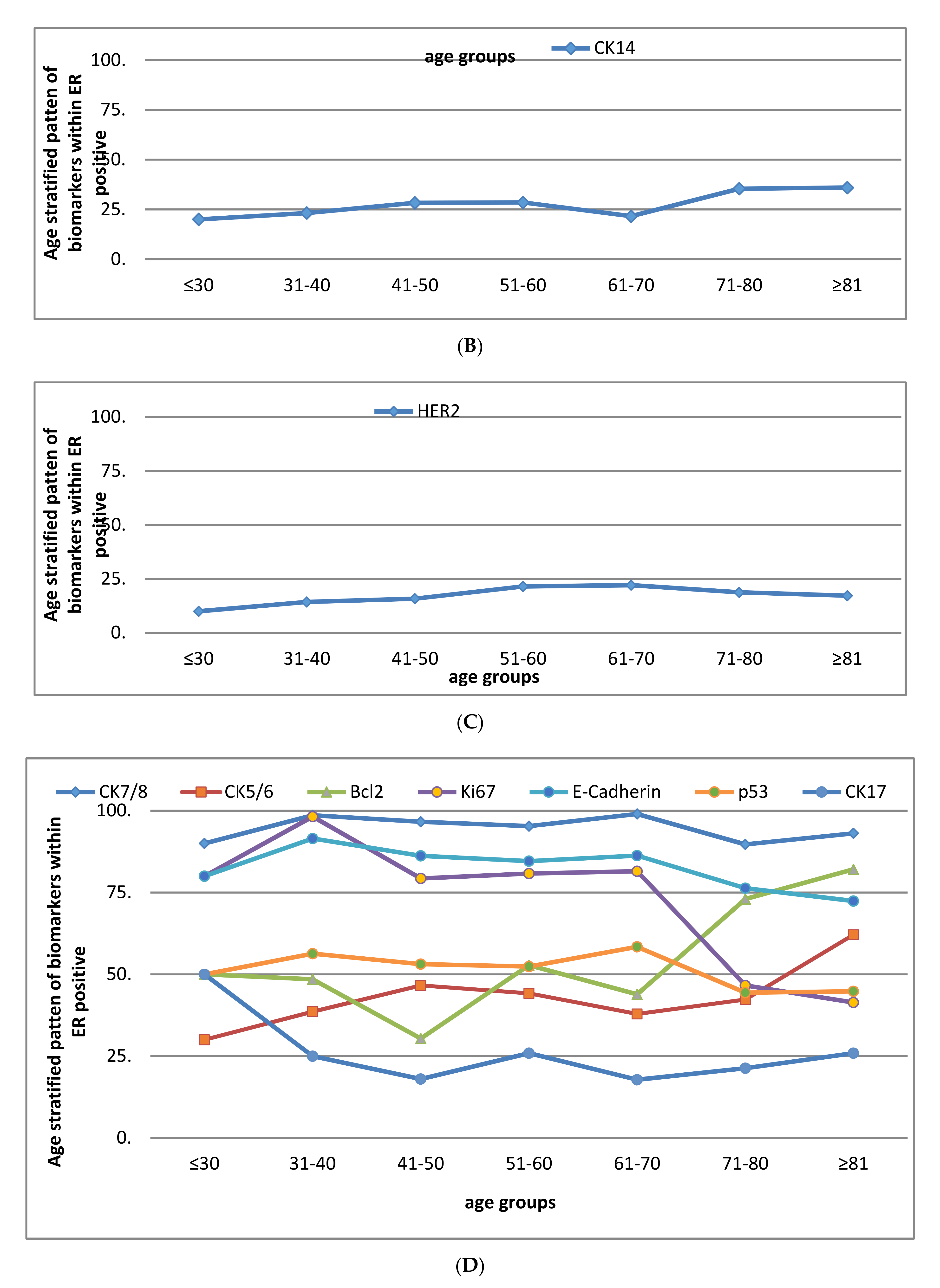
- ER negative group
- a.
- A rise at 40 years—MUC1 and CK18
- b.
- A rise at 70 years—CK14
- c.
- Rise at 30 years then decline at 70 years—HER2
- d.
- Two peaks—Bcl2, CK5/6, Ki67, CK7/8, E-cadherin, p53 and CK17 (at 40 and 70 years).
2.2. Clinical Outcome
Breast Cancer Specific and Metastasis Free Survival Rates
2.3. Treatment Pattern
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Tumour Analysis
4.3. Clinical Outcome
4.4. Statistical analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2016. CA A Cancer J. Clin. 2016, 66, 7–30. [Google Scholar] [CrossRef] [Green Version]
- Diab, S.G.; Elledge, R.M.; Clark, G.M. Tumor Characteristics and Clinical Outcome of Elderly Women with Breast Cancer. J. Natl. Cancer Inst. 2000, 92, 550–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durbecq, V.; Ameye, L.; Veys, I.; Paesmans, M.; Desmedt, C.; Sirtaine, N.; Sotiriou, C.; Bernard-Marty, C.; Nogaret, J.; Piccart, M.; et al. A significant proportion of elderly patients develop hormone-dependant “luminal-B” tumours associated with aggressive characteristics. Crit. Rev. Oncol. 2008, 67, 80–92. [Google Scholar] [CrossRef]
- Li, C.I.; Uribe, D.J.; Daling, J.R. Daling, Clinical characreristics of different histologic types of breast cancer. Br. J. Cancer 2005, 93, 1046–1052. [Google Scholar] [CrossRef] [PubMed]
- Pappo, I.; Karni, T.; Sandbank, J.; Dinur, I.; Sella, A.; Stahl-Kent, V.; Wasserman, I.; Halevy, A. Breast cancer in the elderly: Histological, hormonal and surgical characteristics. Breast 2007, 16, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Fisher, C.J.; Egan, M.K.; Smith, P.; Wicks, K.; Millis, R.R.; Fentiman, I.S. Histopathology of breast cancer in relation to age. Br. J. Cancer 1997, 75, 593–596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Syed, B.M.; Green, A.R.; Paish, E.C.; Soria, D.; Garibaldi, J.M.; Morgan, L.M.; Morgan, D.A.L.; Ellis, I.O.; Cheung, K.L. Biology of primary breast cancer in older women treated by surgery: With correlation with long-term clinical outcome and comparison with their younger counterparts. Br. J. Cancer 2013, 108, 1042–1051. [Google Scholar] [CrossRef] [Green Version]
- Syed, B.M.; Green, A.R.; Morgan, D.; Ellis, I.O.; Cheung, K.-L. Differing pattern of biological characteristics of early operable primary breast cancer according to age. J. Clin. Oncol. 2016, 34, e23272. [Google Scholar] [CrossRef]
- Daidone, M.G.; Coradini, D.; Martelli, G.; Veneroni, S. Primary breast cancer in elderly women: Biological profile and relation with clinical outcome. Crit. Rev. Oncol. 2003, 45, 313–325. [Google Scholar] [CrossRef]
- Eppenberger-Castori, S.; Moore, D.H.; Thor, A.D.; Edgerton, S.M.; Kueng, W.; Eppenberger, U.; Benz, C.C. Age-associated biomarker profiles of human breast cancer. Int. J. Biochem. Cell Biol. 2002, 34, 1318–1330. [Google Scholar] [CrossRef]
- Abd El-Rehim, D.M.; Ball, G.; Pinder, S.E.; Rakha, E.; Paish, C.; Robertson, J.F.; Ellis, I.O. High-throughput protein expression analysis using tissue microarray technology of a large well-characterised series identifies biologically distinct classes of breast cancer confirming recent cDNA expression analyses. Int. J. Cancer 2005, 116, 340–350. [Google Scholar] [CrossRef]
- Van Der Vegt, B.; De Roos MA, J.; Peterse, J.L.; Patriarca, C.; Hilkens, J.; De Bock, G.H.; Wesseling, J. The expression pattern of MUC1 (EMA) is related to tumour characteristics and clinical outcome of invasive ductal breast carcinoma. Histopathology 2007, 51, 322–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.M.; Hwang, T.Y.; Kang, S.H.; Lee, S.J.; Bae, Y.K. Prognostic Significance of Basal Markers in Triple-negative Breast Cancers. J. Breast Cancer 2009, 12, 4–13. [Google Scholar] [CrossRef] [Green Version]
- Cheung, K.; Wong, A.; Parker, H.; Li, V.; Winterbottom, L.; Morgan, D.; Ellis, I. Pathological features of primary breast cancer in the elderly based on needle core biopsies—A large series from a single centre. Crit. Rev. Oncol. 2008, 67, 263–267. [Google Scholar] [CrossRef] [PubMed]
- Gee, J.M.; Robertson, J.F.; Ellis, I.O.; Willsher, P.; McClelland, R.A.; Hoyle, H.B.; Kyme, S.R.; Finlay, P.; Blamey, R.W.; Robert, I. Nicholson Immunohistochemical localisation of Bcl-2 protein in human breast cancer and its relationship to a series of prognostic markers and response to endocrine therapy. Int. J. Cancer 1994, 59, 619–628. [Google Scholar] [CrossRef] [PubMed]
- Antoniou, A.; Pharoah, P.D.; Narod, S.; Risch, H.A.; Eyfjord, J.E.; Hopper, J.L.; Easton, D.F. Average risks of breast and ovarian cancer associated with BRCA1 or BRCA2 mutations detected in case series unselected for family histor: A combined analysis of 22 studies. Am. J. Hum. Genetics 2003, 72, 1117–1130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Syed, B.M.; Johnston, S.J.; Wong, D.W.M.; Green, A.R.; Winterbottom, L.; Kennedy, H.; Simpson, N.; Morgan, D.A.L.; Ellis, I.O.; Cheung, K.L. Long-term (37 years) clinical outcome of older women with early operable primary breast cancer managed in a dedicated clinic. Ann. Oncol. 2011, 23, 1465–1471. [Google Scholar] [CrossRef]
- Rakha, E.A.; Elsheikh, S.E.; Aleskandarany, M.A.; Habashi, H.O.; Green, A.R.; Powe, D.G.; El-Sayed, M.E.; Benhasouna, A.; Brunet, J.-S.; Akslen, L.A.; et al. Triple-Negative Breast Cancer: Distinguishing between Basal and Nonbasal Subtypes. Clin. Cancer Res. 2009, 15, 2302–2310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rao, V.S.; Garimella, V.; Hwang, M.; Drew, P.J. Management of early breast cancer in the elderly. Int. J. Cancer 2007, 120, 1155–1160. [Google Scholar] [CrossRef]
- Howell, A.; Barnes, D.M.; Harland, R.N.; Redford, J.; Bramwell, V.H.; Wilkinson, M.J.; Swindell, R.; Crowther, D.; Sellwood, R.A. Steroid-hormone receptors and survival after first relapse in breast cancer. Lancet 1984, 1, 588–591. [Google Scholar] [CrossRef]
- Tan, D.S.P.; Marchió, C.; Jones, R.L.; Savage, K.; Smith, I.E.; Dowsett, M.; Reis-Filho, J.S. Triple negative breast cancer: Molecular profiling and prognostic impact in adjuvant anthracycline-treated patients. Breast Cancer Res. Treat. 2007, 111, 27–44. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Biomarker (n) | ≤30 n (%) | 31–40 n (%) | 41–50 n (%) | 51–60 n (%) | 61–70 n (%) | 71–80 n (%) | ≥81 n (%) | p-Value |
|---|---|---|---|---|---|---|---|---|
| Lymph node stage | ||||||||
| 1 | 7(50) | 62 (50.8) | 281 (62.0) | 378 (64.1) | 395 (68.6) | 192 (57.1) | 38 (57.6) | 0.01 |
| 2 | 4 (28.6) | 44 (36.1) | 133 (29.4) | 168 (28.5) | 133 (23.1) | 106 (31.5) | 21 (31.8) | |
| 3 | 3 (21.4) | 16 (13.1) | 39 (8.6) | 44 (7.5) | 48 (8.3) | 38 (11.3) | 7 (10.6) | |
| Histological Grade | ||||||||
| 1 | 0 | 5 (4.1) | 83 (18.3) | 131 (22.2) | 110 (19.0) | 51 (12.1) | 13 (12.9) | <0.001 |
| 2 | 2 (14.3) | 25 (20.5) | 140 (30.9) | 200 (34.0) | 209 (36.1) | 166 (39.2) | 46 (45.5) | |
| 3 | 12 (85.7) | 92 (75.4) | 230 (50.8) | 258 (43.8) | 260 (44.9) | 206 (48.7) | 42 (41.6) | |
| Pathological size | ||||||||
| 0.1–3.0 cm | 9 (64.3) | 100 (82.0) | 402 (88.9) | 533 (90.5) | 537 (92.7) | 377 (80.2) | 87 (77.0) | <0.001 |
| 3.1–5.0 cm | 3 (21.4) | 16 (13.1) | 41 (9.1) | 45 (7.6) | 40 (6.9) | 84 (17.9) | 19 (16.8) | |
| >5.0 cm | 2 (14.3) | 6 (4.9) | 9 (2.0) | 11 (1.9) | 2 (0.3) | 9 (1.9) | 7 (6.2) | |
| ER positive (n = 2333) | 8 (57.1) | 57 (46.7) | 314 (69.3) | 436 (73.8) | 470 (81.0) | 322 (70.3) | 79 (69.3) | <0.001 |
| PgR (n = 2278) | 7 (50.0) | 51 (42.5) | 281 (63.7) | 339 (59.4) | 327 (58.3) | 255 (55.9) | 62 (53.9) | 0.003 |
| HER2 (n = 2297) | 0 | 16 (13.3) | 37 (8.5) | 50 (8.7) | 37 (6.5) | 37 (7.9) | 8 (7.0) | 0.232 |
| Ki67 (n = 2020) | 12 (85.7) | 84 (89.4) | 239 (63.7) | 255 (53.5) | 251 (56.2) | 183 (37.3) | 34 (27.9) | <0.001 |
| P53 (n = 2267) | 3 (21.4) | 53 (44.2) | 133 (30.2) | 152 (26.6) | 127 (22.6) | 156 (34.8) | 43 (39.1) | <0.001 |
| Bcl2 (n = 1221) | 0 | 28 (49.1) | 73 (40.1) | 110 (48.9) | 90 (40.5) | 345 (81.6) | 96 (87.3) | <0.001 |
| Muc1 (n = 1962) | 10 (83.3) | 86 (82.7) | 330 (89.7) | 413 (89.6) | 419 (90.7) | 409 (91.5) | 101 (93.5) | 0.133 |
| BRCA1 (n = 1979) | 11 (84.6) | 83 (80.6) | 313 (82.8) | 393 (83.4) | 403 (86.1) | 152 (34.5) | 36 (34.3) | <0.001 |
| CK5/6 (n = 2274) | 2 (14.3) | 30 (25.0) | 82 (18.4) | 105 (18.4) | 69 (12.1) | 146 (32.7) | 48 (44.4) | <0.001 |
| CK7/8 (n = 2296) | 13 (92.6) | 119 (99.2) | 441 (98.9) | 573 (99.0) | 571 (99.7) | 440 (97.1) | 108 (97.3) | 0.006 |
| CK14 (n = 2193) | 2 (14.3) | 17 (14.2) | 64 (14.4) | 84 (14.7) | 51 (9.1) | 91 (23.6) | 25 (24.5) | <0.001 |
| CK17 (n = 1160) | 2 (66.7) | 8 (22.2) | 24 (15.1) | 32 (10.7) | 80 (18.6) | 17 (15.5) | 186 (16.0) | 0.035 |
| CK18 (n = 2176) | 10 (71.4) | 91 (76.5) | 361 (86.4) | 490 (91.4) | 501 (93.1) | 417 (95.2) | 110 (97.3) | <0.001 |
| CK19 (n = 2292) | 12 (85.7) | 111 (92.5) | 425 (95.3) | 547 (94.3) | 538 (94.6) | 424 (94.0) | 109 (97.3) | 0.481 |
| E-Cadherin (n = 2289) | 12 (85.7) | 115 (95.0) | 374 (84.6) | 488 (84.7) | 469 (82.9) | 344 (74.9) | 77 (69.4) | <0.001 |
| Outcome Measure | ≤40 Years | 41–70 Years | ≥70 years | p-Value |
|---|---|---|---|---|
| 5-year Metastases free survival (%) | ||||
| ER positive | 68 | 85 | 87 | 0.003 |
| ER negative | 68 | 70 | 71 | 0.81 |
| 5-year Breast cancer specific survival (%) | ||||
| ER positive | 85 | 89 | 94 | 0.03 |
| ER negative | 70 | 73 | 75 | 0.88 |
| Surgery Only | Surgery Followed by Chemotherapy + /− Radiotherapy | Surgery Followed by Endocrine Therapy + /− Radiotherapy | Surgery Followed by Radiotherapy | |
|---|---|---|---|---|
| ER negative age groups n (%) | ||||
| ≤40 | 5 (6.7) | 61 (81.3) | 0 | 9 (12.0) |
| 41–70 | 59 (16.3) | 124 (34.3) | 108 (29.8) | 71 (19.6) |
| >70 | 122 (72.2) | 0 | 18 (10.7) | 29 (17.2) |
| ER positive age groups n (%) | ||||
| ≤40 | 14 (1) | 29 (36.7) | 17 (21.5) | 19 (24.1) |
| 41–70 | 326 (28.5) | 94 (8.2) | 463 (40.5) | 260 (22.7) |
| >70 | 116 (29.1) | 2 (0.5) | 257 (64.4) | 24 (6.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Syed, B.M.; Green, A.R.; Rakha, E.A.; Morgan, D.A.L.; Ellis, I.O.; Cheung, K.-L. Age-Related Biology of Early-Stage Operable Breast Cancer and Its Impact on Clinical Outcome. Cancers 2021, 13, 1417. https://doi.org/10.3390/cancers13061417
Syed BM, Green AR, Rakha EA, Morgan DAL, Ellis IO, Cheung K-L. Age-Related Biology of Early-Stage Operable Breast Cancer and Its Impact on Clinical Outcome. Cancers. 2021; 13(6):1417. https://doi.org/10.3390/cancers13061417
Chicago/Turabian StyleSyed, Binafsha M., Andrew R. Green, Emad A. Rakha, David A.L. Morgan, Ian O. Ellis, and Kwok-Leung Cheung. 2021. "Age-Related Biology of Early-Stage Operable Breast Cancer and Its Impact on Clinical Outcome" Cancers 13, no. 6: 1417. https://doi.org/10.3390/cancers13061417
APA StyleSyed, B. M., Green, A. R., Rakha, E. A., Morgan, D. A. L., Ellis, I. O., & Cheung, K. -L. (2021). Age-Related Biology of Early-Stage Operable Breast Cancer and Its Impact on Clinical Outcome. Cancers, 13(6), 1417. https://doi.org/10.3390/cancers13061417