
Interstitial Photodynamic Therapy Using 5-ALA for Malignant Glioma Recurrences
 , , , , , , , ,
, , , , , , , , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patient Selection
2.2. Magnetic Resonance Imaging Protocol
2.3. Neuropathological Analysis
2.4. Interstitial PDT Protocol
2.5. Spectral Online Monitoring Analysis
2.6. Perioperative Management and Risk Assessment of iPDT
2.7. Treatment after iPDT and Follow-Up Evaluation
2.8. Statistical Evaluation
3. Results
3.1. Patient Characteristics
3.2. Interstitial PDT Treatment
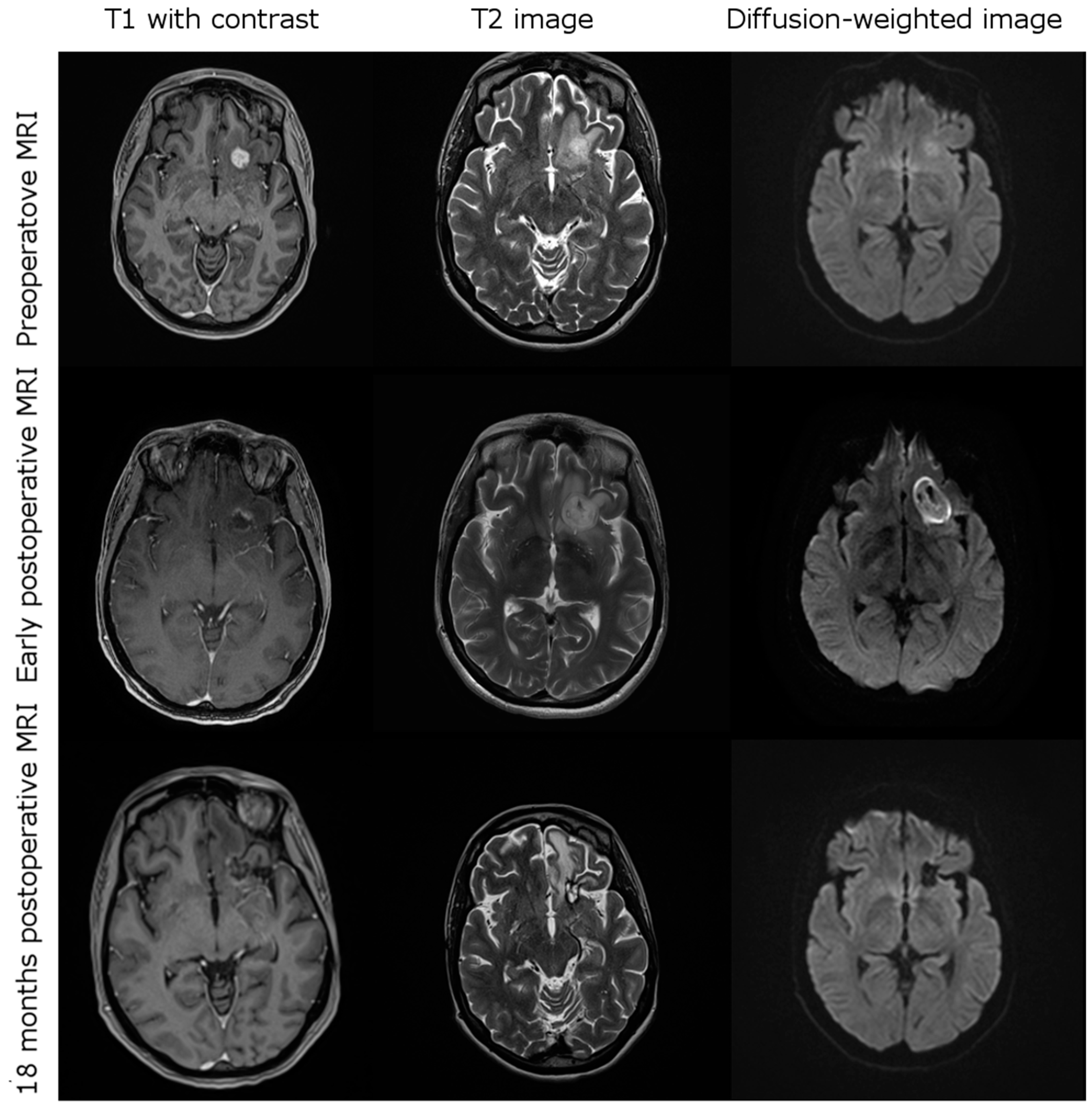
3.3. Imging after iPDT
3.4. Complications after iPDT
3.5. Treatment after iPDT
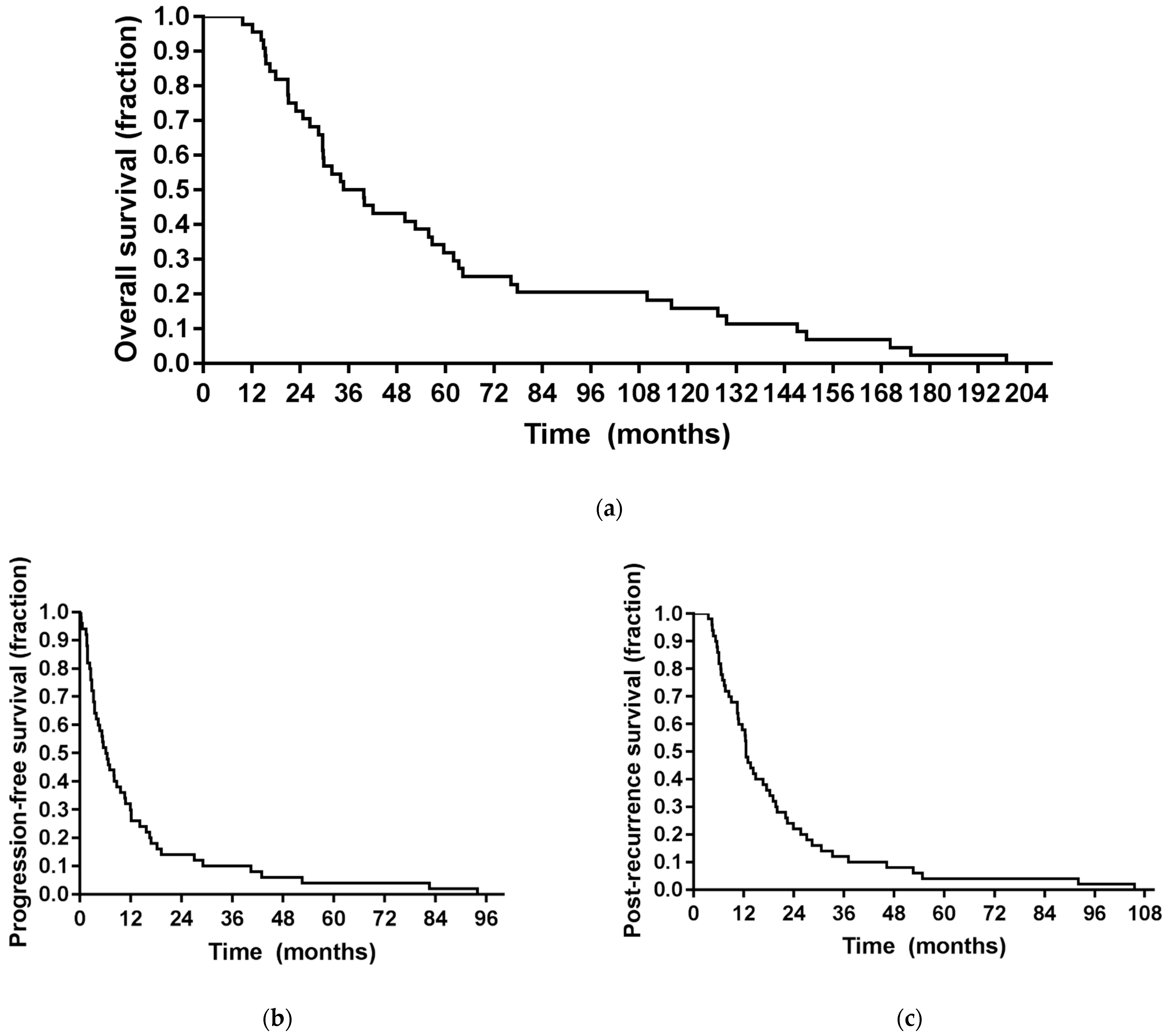
3.6. Outcome
3.7. Prognostic Factors
3.8. Intraoperative Spectral Online Monitoring
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stupp, R.; Taillibert, S.; Kanner, A.A.; Kesari, S.; Steinberg, D.M.; Toms, S.A.; Taylor, L.P.; Lieberman, F.; Silvani, A.; Fink, K.L.; et al. Maintenance Therapy with Tumor-Treating Fields Plus Temozolomide vs Temozolomide Alone for Glioblastoma: A Randomized Clinical Trial. JAMA 2015, 314, 2535–2543. [Google Scholar] [CrossRef]
- Stupp, R.; Taillibert, S.; Kanner, A.; Read, W.; Steinberg, D.M.; Lhermitte, B.; Toms, S.; Idbaih, A.; Ahluwalia, M.S.; Fink, K.; et al. Effect of Tumor-Treating Fields Plus Maintenance Temozolomide vs Maintenance Temozolomide Alone on Survival in Patients with Glioblastoma: A Randomized Clinical Trial. JAMA 2017, 318, 2306–2316. [Google Scholar] [CrossRef] [Green Version]
- Nam, J.Y.; Groot, J.F.D. Treatment of Glioblastoma. J. Oncol. Pract. 2017, 13, 629–638. [Google Scholar] [CrossRef] [PubMed]
- Brada, M.; Hoang-Xuan, K.; Rampling, R.; Dietrich, P.Y.; Dirix, L.Y.; Macdonald, D.; Heimans, J.J.; Zonnenberg, B.A.; Bravo-Marques, J.M.; Henriksson, R.; et al. Multicenter phase II trial of temozolomide in patients with glioblastoma multiforme at first relapse. Ann. Oncol. 2001, 12, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, G.; De Salvo, G.L.; Brandes, A.A.; Eoli, M.; Rudà, R.; Faedi, M.; Lolli, I.; Pace, A.; Daniele, B.; Pasqualetti, F.; et al. Regorafenib compared with lomustine in patients with relapsed glioblastoma (REGOMA): A multicentre, open-label, randomised, controlled, phase 2 trial. Lancet Oncol. 2019, 20, 110–119. [Google Scholar] [CrossRef]
- Stupp, R.; Wong, E.T.; Kanner, A.A.; Steinberg, D.; Engelhard, H.; Heidecke, V.; Kirson, E.D.; Taillibert, S.; Liebermann, F.; Dbaly, V.; et al. NovoTTF-100A versus physician’s choice chemotherapy in recurrent glioblastoma: A randomised phase III trial of a novel treatment modality. Eur. J. Cancer (Oxf. Engl. 1990) 2012, 48, 2192–2202. [Google Scholar] [CrossRef] [Green Version]
- Weller, M.; Le Rhun, E. How did lomustine become standard of care in recurrent glioblastoma? Cancer Treat. Rev. 2020, 87, 102029. [Google Scholar] [CrossRef]
- Desjardins, A.; Gromeier, M.; Herndon, J.E., 2nd; Beaubier, N.; Bolognesi, D.P.; Friedman, A.H.; Friedman, H.S.; McSherry, F.; Muscat, A.M.; Nair, S.; et al. Recurrent Glioblastoma Treated with Recombinant Poliovirus. N. Engl. J. Med. 2018, 379, 150–161. [Google Scholar] [CrossRef] [PubMed]
- Puduvalli, V.K.; Wu, J.; Yuan, Y.; Armstrong, T.S.; Vera, E.; Wu, J.; Xu, J.; Giglio, P.; Colman, H.; Walbert, T.; et al. A Bayesian Adaptive Randomized Phase II Multicenter Trial of Bevacizumab with or without Vorinostat in Adults with Recurrent Glioblastoma. Neuro-Oncology 2020, 1505–1515. [Google Scholar] [CrossRef] [PubMed]
- Suchorska, B.; Weller, M.; Tabatabai, G.; Senft, C.; Hau, P.; Sabel, M.C.; Herrlinger, U.; Ketter, R.; Schlegel, U.; Marosi, C.; et al. Complete resection of contrast-enhancing tumor volume is associated with improved survival in recurrent glioblastoma-results from the DIRECTOR trial. Neuro-Oncology 2016, 18, 549–556. [Google Scholar] [CrossRef]
- Chiocca, E.A.; Yu, J.S.; Lukas, R.V.; Solomon, I.H.; Ligon, K.L.; Nakashima, H.; Triggs, D.A.; Reardon, D.A.; Wen, P.; Stopa, B.M.; et al. Regulatable interleukin-12 gene therapy in patients with recurrent high-grade glioma: Results of a phase 1 trial. Sci. Transl. Med. 2019, 11. [Google Scholar] [CrossRef]
- Cloughesy, T.F.; Petrecca, K.; Walbert, T.; Butowski, N.; Salacz, M.; Perry, J.; Damek, D.; Bota, D.; Bettegowda, C.; Zhu, J.J.; et al. Effect of Vocimagene Amiretrorepvec in Combination With Flucytosine vs Standard of Care on Survival Following Tumor Resection in Patients With Recurrent High-Grade Glioma: A Randomized Clinical Trial. JAMA Oncol. 2020, 6, 1939–1946. [Google Scholar] [CrossRef] [PubMed]
- Stummer, W.; Reulen, H.J.; Meinel, T.; Pichlmeier, U.; Schumacher, W.; Tonn, J.C.; Rohde, V.; Oppel, F.; Turowski, B.; Woiciechowsky, C.; et al. Extent of resection and survival in glioblastoma multiforme: Identification of and adjustment for bias. Neurosurgery 2008, 62, 564–576. [Google Scholar] [CrossRef] [PubMed]
- Lu, V.M.; Jue, T.R.; McDonald, K.L.; Rovin, R.A. The Survival Effect of Repeat Surgery at Glioblastoma Recurrence and its Trend: A Systematic Review and Meta-Analysis. World Neurosurg. 2018, 115, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Wann, A.; Tully, P.A.; Barnes, E.H.; Lwin, Z.; Jeffree, R.; Drummond, K.J.; Gan, H.; Khasraw, M. Outcomes after second surgery for recurrent glioblastoma: A retrospective case-control study. J. Neuro-Oncol. 2018, 137, 409–415. [Google Scholar] [CrossRef]
- Wick, W.; Gorlia, T.; Bendszus, M.; Taphoorn, M.; Sahm, F.; Harting, I.; Brandes, A.A.; Taal, W.; Domont, J.; Idbaih, A.; et al. Lomustine and Bevacizumab in Progressive Glioblastoma. N. Engl. J. Med. 2017, 377, 1954–1963. [Google Scholar] [CrossRef]
- Seystahl, K.; Wick, W.; Weller, M. Therapeutic options in recurrent glioblastoma—An update. Crit. Rev. Oncol./Hematol. 2016, 99, 389–408. [Google Scholar] [CrossRef]
- Rosenthal, M.A.; Gruber, M.L.; Glass, J.; Nirenberg, A.; Finlay, J.; Hochster, H.; Muggia, F.M. Phase II Study of Combination Taxol and Estramustine Phosphate in the Treatment of Recurrent Glioblastoma Multiforme. J. Neuro-Oncol. 2000, 47, 59–63. [Google Scholar] [CrossRef]
- Oudard, S.; Carpentier, A.; Banu, E.; Fauchon, F.; Celerier, D.; Poupon, M.F.; Dutrillaux, B.; Andrieu, J.M.; Delattre, J.Y. Phase II study of lonidamine and diazepam in the treatment of recurrent glioblastoma multiforme. J. Neuro-Oncol. 2003, 63, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Puduvalli, V.K.; Yung, W.K.; Hess, K.R.; Kuhn, J.G.; Groves, M.D.; Levin, V.A.; Zwiebel, J.; Chang, S.M.; Cloughesy, T.F.; Junck, L.; et al. Phase II study of fenretinide (NSC 374551) in adults with recurrent malignant gliomas: A North American Brain Tumor Consortium study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2004, 22, 4282–4289. [Google Scholar] [CrossRef]
- Robe, P.A.; Martin, D.H.; Nguyen-Khac, M.T.; Artesi, M.; Deprez, M.; Albert, A.; Vanbelle, S.; Califice, S.; Bredel, M.; Bours, V. Early termination of ISRCTN45828668, a phase 1/2 prospective, randomized study of sulfasalazine for the treatment of progressing malignant gliomas in adults. BMC Cancer 2009, 9, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rich, J.N.; Reardon, D.A.; Peery, T.; Dowell, J.M.; Quinn, J.A.; Penne, K.L.; Wikstrand, C.J.; Van Duyn, L.B.; Dancey, J.E.; McLendon, R.E.; et al. Phase II trial of gefitinib in recurrent glioblastoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2004, 22, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Sathornsumetee, S.; Desjardins, A.; Vredenburgh, J.J.; McLendon, R.E.; Marcello, J.; Herndon, J.E.; Mathe, A.; Hamilton, M.; Rich, J.N.; Norfleet, J.A.; et al. Phase II trial of bevacizumab and erlotinib in patients with recurrent malignant glioma. Neuro-Oncology 2010, 12, 1300–1310. [Google Scholar] [CrossRef] [Green Version]
- Wick, W.; Puduvalli, V.K.; Chamberlain, M.C.; van den Bent, M.J.; Carpentier, A.F.; Cher, L.M.; Mason, W.; Weller, M.; Hong, S.; Musib, L.; et al. Phase III study of enzastaurin compared with lomustine in the treatment of recurrent intracranial glioblastoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 1168–1174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filley, A.C.; Henriquez, M.; Dey, M. Recurrent glioma clinical trial, CheckMate-143: The game is not over yet. Oncotarget 2017, 8, 91779–91794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, M.; Xia, Y.; Bettegowda, C.; Weller, M. Current state of immunotherapy for glioblastoma. Nat. Rev. Clin. Oncol. 2018, 15, 422–442. [Google Scholar] [CrossRef]
- Stupp, R.; Brada, M.; van den Bent, M.J.; Tonn, J.-C.; Pentheroudakis, G. High-grade glioma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up†. Ann. Oncol. 2014, 25, iii93–iii101. [Google Scholar] [CrossRef]
- Beck, T.J.; Kreth, F.W.; Beyer, W.; Mehrkens, J.H.; Obermeier, A.; Stepp, H.; Stummer, W.; Baumgartner, R. Interstitial photodynamic therapy of nonresectable malignant glioma recurrences using 5-aminolevulinic acid induced protoporphyrin IX. Lasers Surg. Med. 2007, 39, 386–393. [Google Scholar] [CrossRef]
- Stummer, W.; Pichlmeier, U.; Meinel, T.; Wiestler, O.D.; Zanella, F.; Reulen, H.J. Fluorescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma: A randomised controlled multicentre phase III trial. Lancet. Oncol. 2006, 7, 392–401. [Google Scholar] [CrossRef]
- Schucht, P.; Beck, J.; Abu-Isa, J.; Andereggen, L.; Murek, M.; Seidel, K.; Stieglitz, L.; Raabe, A. Gross total resection rates in contemporary glioblastoma surgery: Results of an institutional protocol combining 5-aminolevulinic acid intraoperative fluorescence imaging and brain mapping. Neurosurgery 2012, 71, 927–935. [Google Scholar] [CrossRef] [Green Version]
- Stylli, S.S.; Kaye, A.H.; MacGregor, L.; Howes, M.; Rajendra, P. Photodynamic therapy of high grade glioma-long term survival. J. Clin. Neurosci. Off. J. Neurosurg. Soc. Australas. 2005, 12, 389–398. [Google Scholar] [CrossRef]
- Dupont, C.; Vermandel, M.; Leroy, H.-A.; Quidet, M.; Lecomte, F.; Delhem, N.; Mordon, S.; Reyns, N. INtraoperative photoDYnamic Therapy for GliOblastomas (INDYGO): Study protocol for a phase I clinical trial. Neurosurgery 2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johansson, A.; Faber, F.; Kniebühler, G.; Stepp, H.; Sroka, R.; Egensperger, R.; Beyer, W.; Kreth, F.-W. Protoporphyrin IX Fluorescence and Photobleaching During Interstitial Photodynamic Therapy of Malignant Gliomas for Early Treatment Prognosis. Lasers Surg. Med. 2013, 45, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Stummer, W.; Beck, T.; Beyer, W.; Mehrkens, J.H.; Obermeier, A.; Etminan, N.; Stepp, H.; Tonn, J.C.; Baumgartner, R.; Herms, J.; et al. Long-sustaining response in a patient with non-resectable, distant recurrence of glioblastoma multiforme treated by interstitial photodynamic therapy using 5-ALA: Case report. J. Neuro-Oncol. 2008, 87, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, D.R.; Cascino, T.L.; Schold, S.C., Jr.; Cairncross, J.G. Response criteria for phase II studies of supratentorial malignant glioma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1990, 8, 1277–1280. [Google Scholar] [CrossRef] [PubMed]
- Wen, P.Y.; Macdonald, D.R.; Reardon, D.A.; Cloughesy, T.F.; Sorensen, A.G.; Galanis, E.; Degroot, J.; Wick, W.; Gilbert, M.R.; Lassman, A.B.; et al. Updated response assessment criteria for high-grade gliomas: Response assessment in neuro-oncology working group. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 1963–1972. [Google Scholar] [CrossRef]
- Eigenbrod, S.; Trabold, R.; Brucker, D.; Eros, C.; Egensperger, R.; La Fougere, C.; Gobel, W.; Ruhm, A.; Kretzschmar, H.A.; Tonn, J.C.; et al. Molecular stereotactic biopsy technique improves diagnostic accuracy and enables personalized treatment strategies in glioma patients. Acta Neurochir. 2014, 156, 1427–1440. [Google Scholar] [CrossRef]
- Louis, D.N.; Ohgaki, H.; Wiestler, O.D.; Cavenee, W.K.; Burger, P.C.; Jouvet, A.; Scheithauer, B.W.; Kleihues, P. The 2007 WHO Classification of Tumours of the Central Nervous System. Acta Neuropathol. 2007, 114, 97–109. [Google Scholar] [CrossRef] [Green Version]
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [Green Version]
- Rühm, A.; Stepp, H.; Beyer, W.; Hennig, G.; Pongratz, T.; Sroka, R.; Schnell, O.; Tonn, J.-C.; Kreth, F.-W. 5-ALA based photodynamic management of glioblastoma. In Proceedings of the SPIE, San Francisco, CA, USA, 24 March 2014. [Google Scholar]
- National Institutes of Health Common Terminology Criteria for Adverse Events (CTCAE); National Cancer Institute: Bethesda, MD, USA, 2017.
- Rachinger, W.; Goetz, C.; Popperl, G.; Gildehaus, F.J.; Kreth, F.W.; Holtmannspotter, M.; Herms, J.; Koch, W.; Tatsch, K.; Tonn, J.C. Positron emission tomography with O-(2-[18F]fluoroethyl)-l-tyrosine versus magnetic resonance imaging in the diagnosis of recurrent gliomas. Neurosurgery 2005, 57, 505–511. [Google Scholar] [CrossRef]
- Mehrkens, J.H.; Popperl, G.; Rachinger, W.; Herms, J.; Seelos, K.; Tatsch, K.; Tonn, J.C.; Kreth, F.W. The positive predictive value of O-(2-[18F]fluoroethyl)-L-tyrosine (FET) PET in the diagnosis of a glioma recurrence after multimodal treatment. J. Neuro-Oncol. 2008, 88, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Shafirstein, G.; Bellnier, D.; Oakley, E.; Hamilton, S.; Potasek, M.; Beeson, K.; Parilov, E. Interstitial Photodynamic Therapy-A Focused Review. Cancers 2017, 9, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collaud, S.; Juzeniene, A.; Moan, J.; Lange, N. On the selectivity of 5-aminolevulinic acid-induced protoporphyrin IX formation. Curr. Med. Chem. Anti-Cancer Agents 2004, 4, 301–316. [Google Scholar] [CrossRef]
- Agostinis, P.; Berg, K.; Cengel, K.A.; Foster, T.H.; Girotti, A.W.; Gollnick, S.O.; Hahn, S.M.; Hamblin, M.R.; Juzeniene, A.; Kessel, D.; et al. Photodynamic therapy of cancer: An update. CA A Cancer J. Clin. 2011, 61, 250–281. [Google Scholar] [CrossRef]
- Stepp, H.; Stummer, W. 5-ALA in the management of malignant glioma. Lasers Surg. Med. 2018, 50, 399–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beltrán Hernández, I.; Yu, Y.; Ossendorp, F.; Korbelik, M.; Oliveira, S. Preclinical and Clinical Evidence of Immune Responses Triggered in Oncologic Photodynamic Therapy: Clinical Recommendations. J. Clin. Med. 2020, 9, 333. [Google Scholar] [CrossRef] [Green Version]
- Kammerer, R.; Buchner, A.; Palluch, P.; Pongratz, T.; Oboukhovskij, K.; Beyer, W.; Johansson, A.; Stepp, H.; Baumgartner, R.; Zimmermann, W. Induction of immune mediators in glioma and prostate cancer cells by non-lethal photodynamic therapy. PLoS ONE 2011, 6, e21834. [Google Scholar] [CrossRef] [PubMed]
- Castano, A.P.; Mroz, P.; Hamblin, M.R. Photodynamic therapy and anti-tumour immunity. Nat. Rev. Cancer 2006, 6, 535–545. [Google Scholar] [CrossRef] [Green Version]
- Heckl, C.; Aumiller, M.; Rühm, A.; Sroka, R.; Stepp, H. Fluorescence and Treatment Light Monitoring for Interstitial Photodynamic Therapy. Photochem. Photobiol. 2020, 96, 388–396. [Google Scholar] [CrossRef] [Green Version]
- Stummer, W.; Tonn, J.C.; Mehdorn, H.M.; Nestler, U.; Franz, K.; Goetz, C.; Bink, A.; Pichlmeier, U. Counterbalancing risks and gains from extended resections in malignant glioma surgery: A supplemental analysis from the randomized 5-aminolevulinic acid glioma resection study. Clinical article. J. Neurosurg. 2011, 114, 613–623. [Google Scholar] [CrossRef]
- Magill, S.T.; Han, S.J.; Li, J.; Berger, M.S. Resection of primary motor cortex tumors: Feasibility and surgical outcomes. J. Neurosurg. 2018, 129, 961–972. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.M.; Parney, I.F.; McDermott, M.; Barker, F.G., 2nd; Schmidt, M.H.; Huang, W.; Laws, E.R., Jr.; Lillehei, K.O.; Bernstein, M.; Brem, H.; et al. Perioperative complications and neurological outcomes of first and second craniotomies among patients enrolled in the Glioma Outcome Project. J. Neurosurg. 2003, 98, 1175–1181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoover, J.M.; Nwojo, M.; Puffer, R.; Mandrekar, J.; Meyer, F.B.; Parney, I.F. Surgical outcomes in recurrent glioma: Clinical article. J. Neurosurg. 2013, 118, 1224–1231. [Google Scholar] [CrossRef]
- Flieger, M.; Ganswindt, U.; Schwarz, S.B.; Kreth, F.W.; Tonn, J.C.; la Fougere, C.; Ertl, L.; Linn, J.; Herrlinger, U.; Belka, C.; et al. Re-irradiation and bevacizumab in recurrent high-grade glioma: An effective treatment option. J. Neuro-Oncol. 2014, 117, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Ahn, S.S.; Chang, J.H.; Suh, C.O. Hypofractionated Re-irradiation after Maximal Surgical Resection for Recurrent Glioblastoma: Therapeutic Adequacy and Its Prognosticators of Survival. Yonsei Med. J. 2018, 59, 194–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weller, M.; Tabatabai, G.; Kästner, B.; Felsberg, J.; Steinbach, J.P.; Wick, A.; Schnell, O.; Hau, P.; Herrlinger, U.; Sabel, M.C.; et al. MGMT Promoter Methylation Is a Strong Prognostic Biomarker for Benefit from Dose-Intensified Temozolomide Rechallenge in Progressive Glioblastoma: The DIRECTOR Trial. Clin. Cancer Res. An Off. J. Am. Assoc. Cancer Res. 2015, 21, 2057–2064. [Google Scholar] [CrossRef] [Green Version]
- Wick, W.; Meisner, C.; Hentschel, B.; Platten, M.; Schilling, A.; Wiestler, B.; Sabel, M.C.; Koeppen, S.; Ketter, R.; Weiler, M.; et al. Prognostic or predictive value of MGMT promoter methylation in gliomas depends on IDH1 mutation. Neurology 2013, 81, 1515–1522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, F.; Cheng, Y.; Lu, J.; Hu, R.; Wan, Q.; Feng, H. Photodynamic therapy boosts anti-glioma immunity in mice: A dependence on the activities of T cells and complement C3. J. Cell. Biochem. 2011, 112, 3035–3043. [Google Scholar] [CrossRef]
- Hübner, M.; Strauss, G.; Effinger, D.; Pohla, H.; Kreth, F.-W.; Kreth, S. IMPS-15PDT-TREATED GBM CELLS INCREASE EFFECTOR FUNCTIONS OF HUMAN CD8+ T-CELLS. Neuro-Oncology 2015, 17, v116. [Google Scholar] [CrossRef] [Green Version]
- Etminan, N.; Peters, C.; Lakbir, D.; Bünemann, E.; Börger, V.; Sabel, M.C.; Hänggi, D.; Steiger, H.J.; Stummer, W.; Sorg, R.V. Heat-shock protein 70-dependent dendritic cell activation by 5-aminolevulinic acid-mediated photodynamic treatment of human glioblastoma spheroids in vitro. Br. J. Cancer 2011, 105, 961–969. [Google Scholar] [CrossRef]
- Cramer, G.M.; Moon, E.K.; Cengel, K.A.; Busch, T.M. Photodynamic Therapy and Immune Checkpoint Blockade(†). Photochem. Photobiol. 2020, 96, 954–961. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics at iPDT | All Patients (N = 44) |
|---|---|
| Age (years) | |
| Median | 49.4 |
| Range | 33.4–87.0 |
| Gender, n (%) | |
| Male | 27 (61.4) |
| Female | 17 (38.6) |
| KPS, n (%) | |
| 100 | 3 (6.8) |
| 90 | 29 (65.9) |
| 80 | 9 (20.5) |
| 70 | 3 (6.8) |
| Symptoms, n (%) | |
| Seizures | 27 (61.4) |
| Aphasia without paresis | 12 (27.3) |
| Paresis without aphasia | 4 (9.1) |
| Aphasia and paresis | 1 (2.3) 1 |
| Side, n (%) | |
| Right | 20 (45.5) |
| Left | 24 (54.5) |
| Localization, n (%) | |
| Deep-seated involvement | 31 (70.5) |
| Eloquent lobar localization | 17 (38.6) |
| Stage of disease, n (%) | |
| First tumor recurrence | 26 (59.1) |
| Second tumor recurrence | 9 (20.5) |
| Third tumor recurrence | 6 (13.6) |
| Later stages | 3 (6.8) |
| WHO grade, n (%) | |
| IV | 37 (84.1) |
| III | 7 (15.9) |
| WHO grade at initial diagnosis, n (%) | |
| IV | 30 (68.2) |
| III | 8 (18.2) |
| II | 6 (13.6) |
| MGMT promoter methylation status, n (%) | |
| Methylated | 30 (68.2) |
| Unmethylated | 14 (31.8) |
| IDH mutation, n (%) | |
| Wildtype | 29 (65.9) |
| Mutated | 9 (20.5) |
| Unknown (no material left) | 6 (13.6) |
| 1 p/19 q codeletion, n (%) | |
| 1 p/19 q codeletion | 1 (2.3) |
| No 1 p/19 q codeletion | 20 (45.5) |
| Not tested | 23 (52.3) |
| Treatment Algorithms | All Patients (N = 44) |
|---|---|
| Treatment before iPDT, n (%) | |
| Tumor resection | 36 (81.9) |
| Irradiation | 43 (97.7) |
| Chemotherapy | 39 (88.6) |
| Interstitial PDT characteristics | |
| Target volume (cm3) | |
| Median | 3.34 |
| Range | 0.50–22.8 |
| Number of cylindrical diffusing fibers (range) | 4 (3–8) |
| Applied light power per diffuser length (mW/cm) | |
| Median | 200 |
| Range | 82–210 |
| Treatment dose (J) | |
| Median | 8883 |
| Range | 5760–17,388 |
| Treatment time (minutes) | |
| Median | 60 (N = 29) |
| Range | 60–167 |
| Salvage treatment with iPDT, n (%) | |
| Chemotherapy | 20 (45,4) |
| Radiotherapy | 7 (15.9) |
| Radiochemotherapy | 4 (9.1) |
| Treatment after iPDT failure, n (%) | |
| Any chemotherapy | 31 (70.5) |
| Any (re-)radiotherapy | 20 (45.5) |
| Any tumor resection/debulking | 4 (9.1) |
| Complications after iPDT | All Patients (N = 44) |
|---|---|
| Postoperative CTCAE grade, N (%) | |
| 0 | 26 (59.1) |
| 1 | 4 (9.1) |
| 2 | 10 (22.7) |
| 3 | 3 (6.8) |
| 4 | 1 (2.3) |
| 5 | 0 (0.0) |
| CTCAE grade at six weeks, N (%) | |
| 0 | 32 (72.7) |
| 1 | 9 (20.5) |
| 2 | 2 (4.5) |
| 3 | 1 (2.3) |
| 4 | 0 (0.0) |
| 5 | 0 (0.0) |
| Type of complications, N (%) | |
| Aphasia | 7 (15.9) |
| Paresis | 6 (13.6) |
| Paresis and aphasia | 4 (9.1) |
| Hyp-/dysaesthesia only | 1 (2.3) |
| None | 26 (59.1) |
| Characteristic | HR | Univariate 95% CI | p-Value | HR | Multivariate 95% CI | p-Value |
|---|---|---|---|---|---|---|
| Post-recurrence survival (after iPDT) | ||||||
| Age at iPDT | 1.006 | 0.981–1.033 | 0.635 | 1.023 | 0.968–1.080 | 0.424 |
| KPS at iPDT | 0.936 | 0.886–0.989 | 0.019 | 1.961 | 0.755–5.092 | 0.167 |
| MGMT methylation | 0.751 | 0.392–1.438 | 0.388 | 1.000 | 0.339–2.946 | 1.000 |
| IDH mutation | 0.878 | 0.405–1.904 | 0.742 | 1.018 | 0.326–3.178 | 0.976 |
| Target volume | 1.019 | 0.956–1.086 | 0.557 | 1.017 | 0.943–1.096 | 0.666 |
| Time to iPDT | 1.003 | 0.996–1.010 | 0.392 | 1.003 | 0.992–1.015 | 0.553 |
| Further chemotherapy | 0.811 | 0.421–1.561 | 0.530 | 1.030 | 0.443–2.392 | 0.946 |
| Further radiotherapy | 0.999 | 0.540–1.849 | 0.999 | 1.005 | 0.317–3.189 | 0.994 |
| Further surgery | 0.782 | 0.276–2.212 | 0.643 | 1.303 | 0.258–6.568 | 0.748 |
| Spectral Data (N = 18) | Median TTF (CI) (Months) | p-Value | Median PRS (CI) (Months) | p-Value |
|---|---|---|---|---|
| Transmission < 75% | 9.63 (.978; 18.28) | 12.97 (12.03; 13.92) | ||
| Transmission > 75% | 15.73 (4.71; 24.96)) | 0.196 | 19.70 (4.32; 35.08) | 0.130 |
| Fluorescence < 75% | 9.63 (4.20; 15.06) | 16.57 (7.83; 25.31) | ||
| Fluorescence > 75% | 12.13 (3.84; 20.42) | 0.427 | 17.47 (4.20; 30.74) | 0.326 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lietke, S.; Schmutzer, M.; Schwartz, C.; Weller, J.; Siller, S.; Aumiller, M.; Heckl, C.; Forbrig, R.; Niyazi, M.; Egensperger, R.; et al. Interstitial Photodynamic Therapy Using 5-ALA for Malignant Glioma Recurrences. Cancers 2021, 13, 1767. https://doi.org/10.3390/cancers13081767
Lietke S, Schmutzer M, Schwartz C, Weller J, Siller S, Aumiller M, Heckl C, Forbrig R, Niyazi M, Egensperger R, et al. Interstitial Photodynamic Therapy Using 5-ALA for Malignant Glioma Recurrences. Cancers. 2021; 13(8):1767. https://doi.org/10.3390/cancers13081767
Chicago/Turabian StyleLietke, Stefanie, Michael Schmutzer, Christoph Schwartz, Jonathan Weller, Sebastian Siller, Maximilian Aumiller, Christian Heckl, Robert Forbrig, Maximilian Niyazi, Rupert Egensperger, and et al. 2021. "Interstitial Photodynamic Therapy Using 5-ALA for Malignant Glioma Recurrences" Cancers 13, no. 8: 1767. https://doi.org/10.3390/cancers13081767
APA StyleLietke, S., Schmutzer, M., Schwartz, C., Weller, J., Siller, S., Aumiller, M., Heckl, C., Forbrig, R., Niyazi, M., Egensperger, R., Stepp, H., Sroka, R., Tonn, J. -C., Rühm, A., & Thon, N. (2021). Interstitial Photodynamic Therapy Using 5-ALA for Malignant Glioma Recurrences. Cancers, 13(8), 1767. https://doi.org/10.3390/cancers13081767