
Fourteen-Day Gemcitabine-Docetaxel Chemotherapy Is Effective and Safer Compared to 21-Day Regimen in Patients with Advanced Soft Tissue and Bone Sarcoma

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Data Collection
2.2. Gemcitabine, Docetaxel, and GCSF Administration
2.3. Assessment for Response, PFS, and OS
2.4. Next-Generation Sequencing (NGS) for Identifying Genomic Alterations
2.5. Statistical Analysis
3. Results
3.1. Demographics
3.2. Gemcitabine and Docetaxel Dosing
3.3. Lines of Therapy
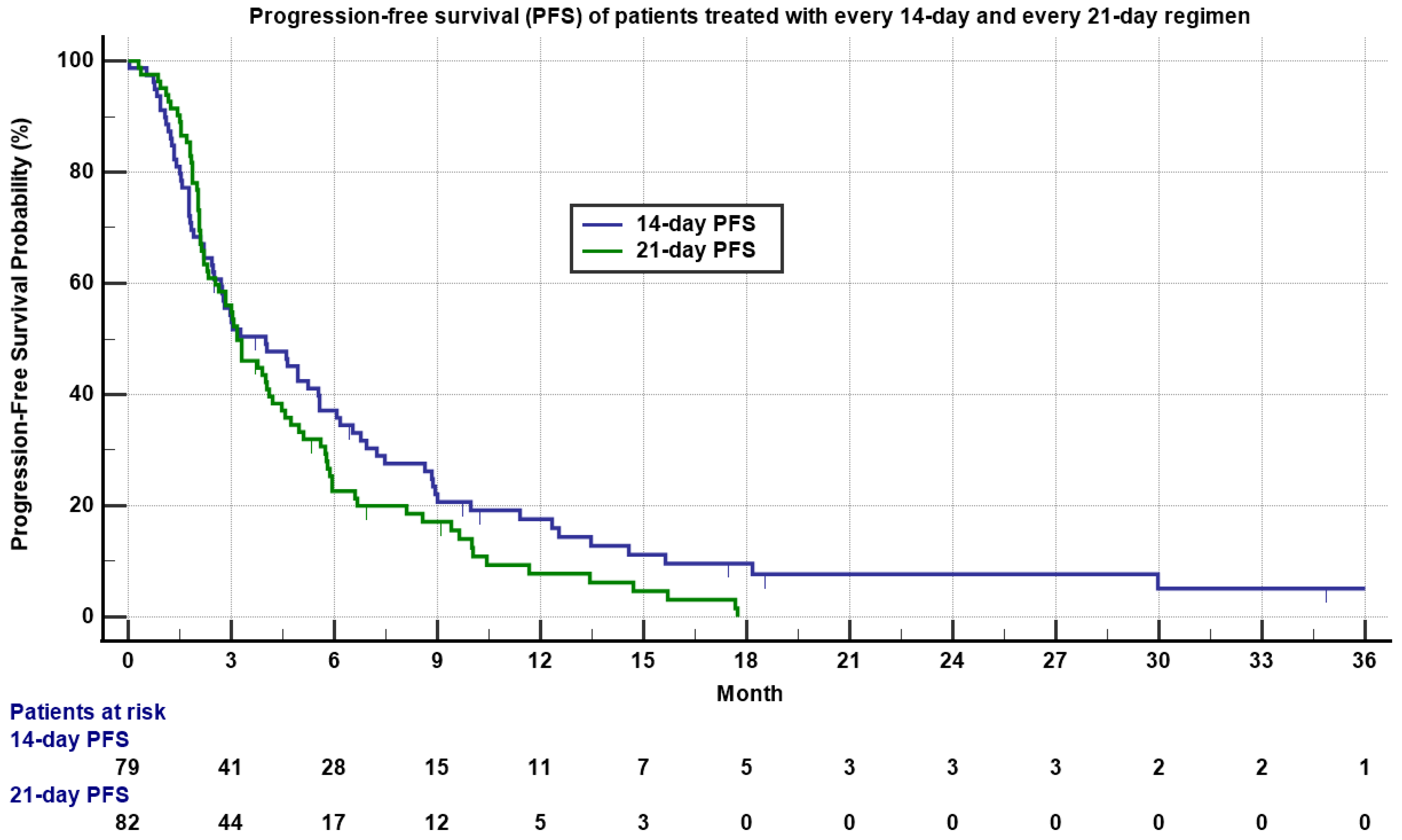
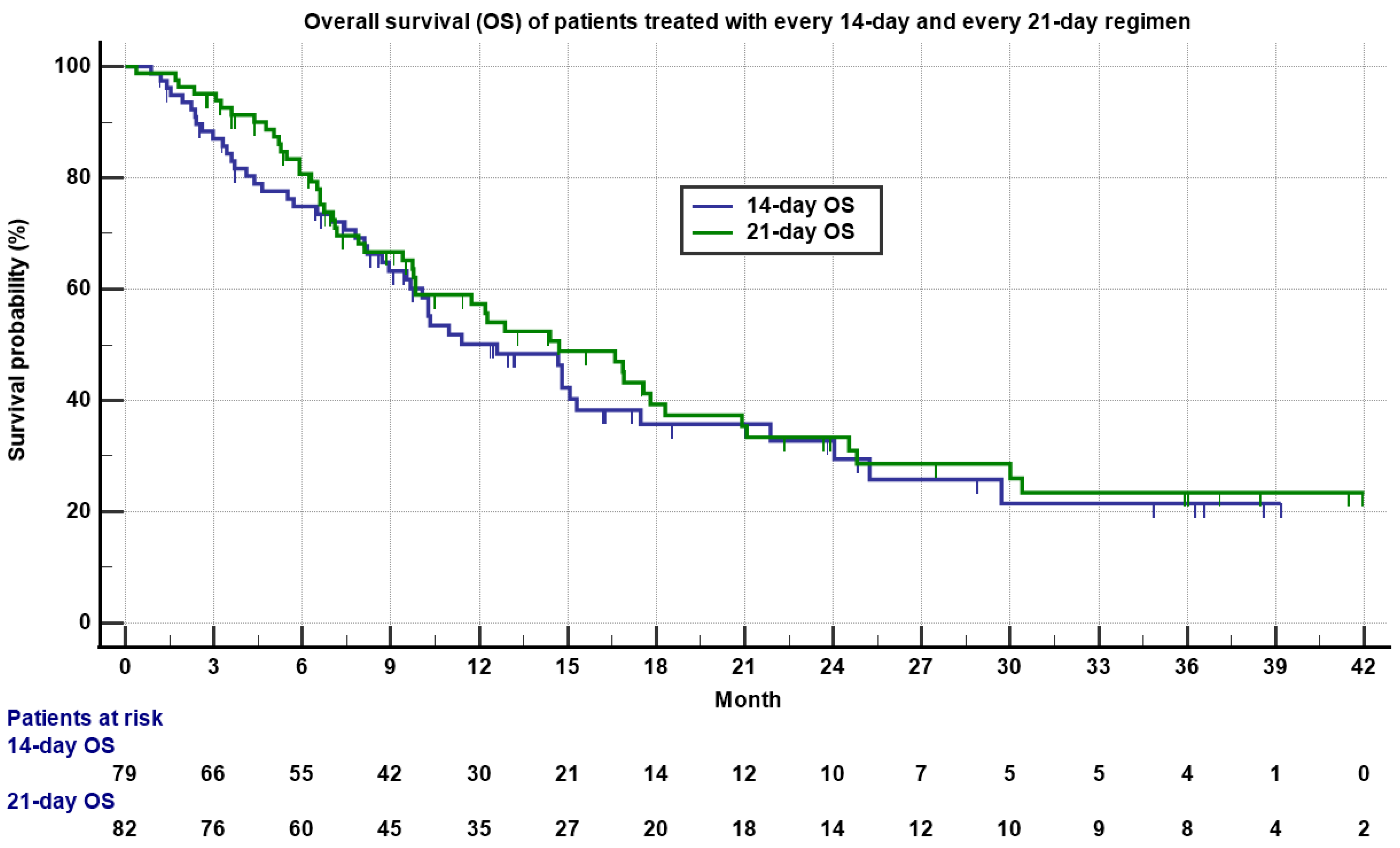
3.4. Response Rate, PFS and OS
3.5. Toxicity
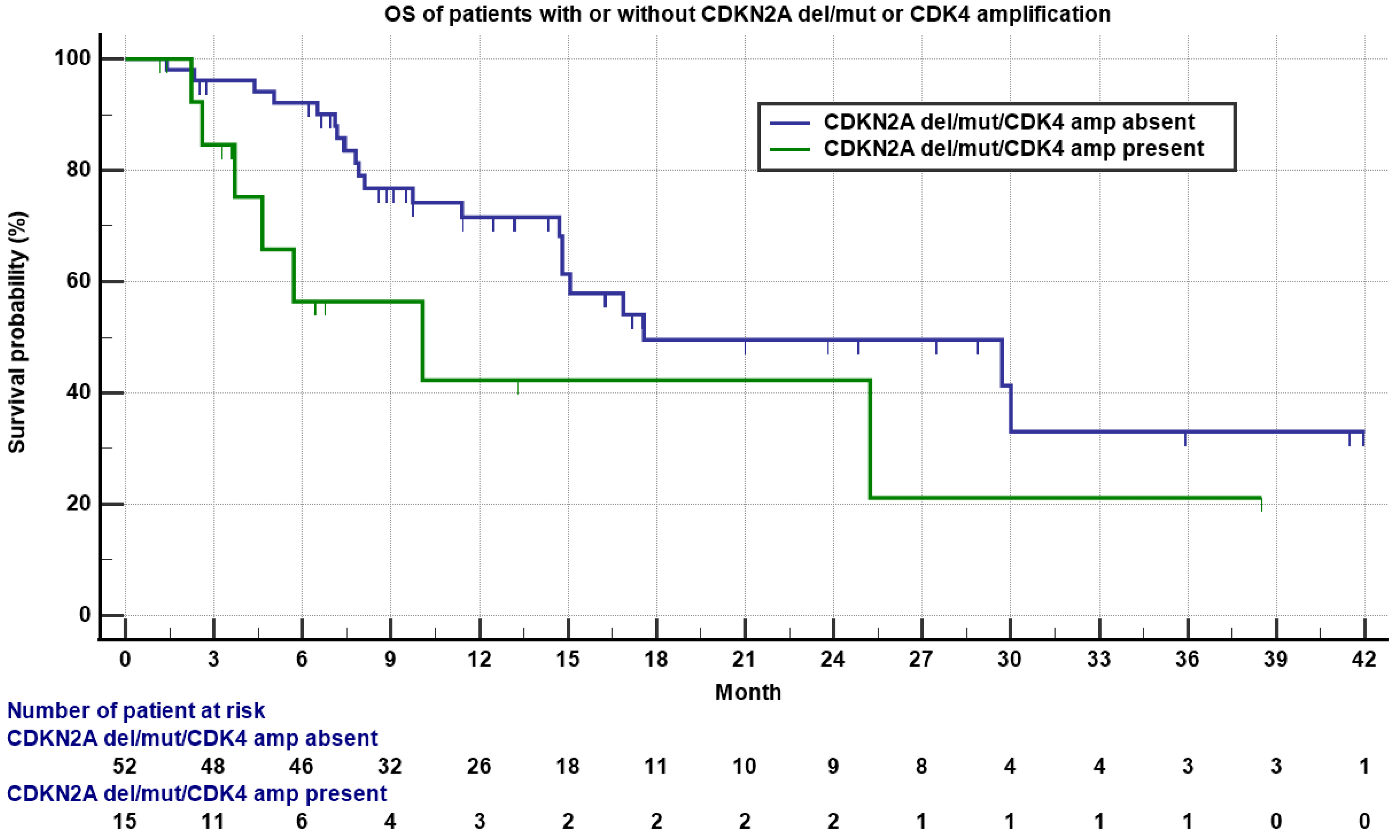
3.6. Association of Genomic Alterations with RR, PFS, and OS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Linch, M.; Miah, A.B.; Thway, K.; Judson, I.R.; Benson, C. Systemic treatment of soft-tissue sarcoma—Gold standard and novel therapies. Nat. Rev. Clin. Oncol. 2014, 11, 187–202. [Google Scholar] [CrossRef]
- Gamboa, A.C.; Gronchi, A.; Cardona, K. Soft-tissue sarcoma in adults: An update on the current state of histiotype-specific management in an era of personalized medicine. CA Cancer J. Clin. 2020, 70, 200–229. [Google Scholar] [CrossRef]
- Hensley, M.L.; Maki, R.; Venkatraman, E.; Geller, G.; Lovegren, M.; Aghajanian, C.; Sabbatini, P.; Tong, W.; Barakat, R.; Spriggs, D.R. Gemcitabine and Docetaxel in Patients with Unresectable Leiomyosarcoma: Results of a Phase II Trial. J. Clin. Oncol. 2002, 20, 2824–2831. [Google Scholar] [CrossRef] [PubMed]
- Hensley, M.L.; Blessing, J.A.; Mannel, R.; Rose, P.G. Fixed-dose rate gemcitabine plus docetaxel as first-line therapy for metastatic uterine leiomyosarcoma: A Gynecologic Oncology Group phase II trial. Gynecol. Oncol. 2008, 109, 329–334. [Google Scholar] [CrossRef]
- Hensley, M.L.; Blessing, J.A.; Mannel, R.; Rose, P.G. Fixed-dose rate gemcitabine plus docetaxel as second-line therapy for metastatic uterine leiomyosarcoma: A Gynecologic Oncology Group phase II trial. Gynecol. Oncol. 2008, 109, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Seddon, B.; Scurr, M.; Jones, R.L.; Wood, Z.; Propert-Lewis, C.; Fisher, C.; Flanagan, A.; Sunkersing, J.; A’Hern, R.; Whelan, J.; et al. A phase II trial to assess the activity of gemcitabine and docetaxel as first line chemotherapy treatment in patients with unresectable leiomyosarcoma. Clin. Sarcoma Res. 2015, 5, 1–7. [Google Scholar] [CrossRef]
- Bay, J.-O.; Ray-Coquard, I.; Fayette, J.; Leyvraz, S.; Cherix, S.; Piperno-Neumann, S.; Chevreau, C.; Isambert, N.; Brain, E.; Emile, G.; et al. Docetaxel and gemcitabine combination in 133 advanced soft-tissue sarcomas: A retrospective analysis. Int. J. Cancer 2006, 119, 706–711. [Google Scholar] [CrossRef] [PubMed]
- Maki, R.G.; Wathen, J.K.; Patel, S.R.; Priebat, D.A.; Okuno, S.H.; Samuels, B.; Fanucchi, M.; Harmon, D.C.; Schuetze, S.M.; Reinke, D.; et al. Randomized phase II study of gemcitabine and docetaxel compared with gemcitabine alone in patients with metastatic soft tissue sarcomas: Results of sarcoma alliance for research through collaboration study 002. J. Clin. Oncol. 2007, 25, 2755–2763. [Google Scholar] [CrossRef]
- Pautier, P.; Floquet, A.; Penel, N.; Piperno-Neumann, S.; Isambert, N.; Rey, A.; Bompas, E.; Cioffi, A.; Delcambre, C.; Cupissol, D.; et al. Randomized Multicenter and Stratified Phase II Study of Gemcitabine Alone Versus Gemcitabine and Docetaxel in Patients with Metastatic or Relapsed Leiomyosarcomas: A Fédération Nationale des Centres de Lutte Contre le Cancer (FNCLCC) French Sarcoma Group Study (TAXOGEM study). Oncologist 2012, 17, 1213–1220. [Google Scholar] [CrossRef]
- Dickson, M.A.; D’Adamo, D.R.; Keohan, M.L.; D’Angelo, S.P.; Carvajal, R.D.; Gounder, M.M.; Maki, R.G.; Qin, L.-X.; Lefkowitz, R.A.; McKennon, O.R.; et al. Phase II Trial of Gemcitabine and Docetaxel with Bevacizumab in Soft Tissue Sarcoma. Sarcoma 2015, 2015, 1–7. [Google Scholar] [CrossRef]
- Hensley, M.L.; Enserro, D.; Hatcher, H.; Ottevanger, P.B.; Krarup-Hansen, A.; Blay, J.-Y.; Fisher, C.; Moxley, K.M.; Lele, S.B.; Lea, J.S.; et al. Adjuvant Gemcitabine Plus Docetaxel Followed by Doxorubicin Versus Observation for High-Grade Uterine Leiomyosarcoma: A Phase III NRG Oncology/Gynecologic Oncology Group Study. J. Clin. Oncol. 2018, 36, 3324–3330. [Google Scholar] [CrossRef] [PubMed]
- Hensley, M.L.; Ishill, N.; Soslow, R.; Larkin, J.; Abu-Rustum, N.; Sabbatini, P.; Konner, J.; Tew, W.; Spriggs, D.; Aghajanian, C.A. Adjuvant gemcitabine plus docetaxel for completely resected stages I–IV high grade uterine leiomyosarcoma: Results of a prospective study. Gynecol. Oncol. 2009, 112, 563–567. [Google Scholar] [CrossRef] [PubMed]
- Seddon, B.; Strauss, S.J.; Whelan, J.; Leahy, M.; Woll, P.J.; Cowie, F.; Rothermundt, C.; Wood, Z.; Benson, C.; Ali, N.; et al. Gemcitabine and docetaxel versus doxorubicin as first-line treatment in previously untreated advanced unresectable or metastatic soft-tissue sarcomas (GeDDiS): A randomised controlled phase 3 trial. Lancet Oncol. 2017, 18, 1397–1410. [Google Scholar] [CrossRef]
- Verweij, J.; Lee, S.M.; Ruka, W.; Buesa, J.; Coleman, R.; Van Hoessel, R.; Seynaeve, C.; Di Paola, E.D.; Van Glabbeke, M.; Tonelli, D.; et al. Randomized Phase II Study of Docetaxel Versus Doxorubicin in First- and Second-Line Chemotherapy for Locally Advanced or Metastatic Soft Tissue Sarcomas in Adults: A Study of the European Organization for Research and Treatment of Cancer Soft Tissue and Bone Sarcoma Group. J. Clin. Oncol. 2000, 18, 2081–2086. [Google Scholar] [CrossRef] [PubMed]
- Nagano, T.; Yamada, Y.; Ikeda, T.; Kanki, H.; Kamo, T.; Nishigori, C. Docetaxel: A therapeutic option in the treatment of cutaneous angiosarcoma: Report of 9 patients. Cancer 2007, 110, 648–651. [Google Scholar] [CrossRef]
- Isogai, R.; Kawada, A.; Aragane, Y.; Tezuka, T. Successful treatment of pulmonary metastasis and local recurrence of angiosarcoma with docetaxel. J. Dermatol. 2004, 31, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Verschraegen, C.F.; Arias-Pulido, H.; Lee, S.-J.; Movva, S.; Cerilli, L.A.; Eberhardt, S.; Schmit, B.; Quinn, R.; Muller, C.Y.; Rabinowitz, I.; et al. Phase IB study of the combination of docetaxel, gemcitabine, and bevacizumab in patients with advanced or recurrent soft tissue sarcoma: The Axtell regimen. Ann. Oncol. 2012, 23, 785–790. [Google Scholar] [CrossRef]
- Hensley, M.L.; Miller, A.; O’Malley, D.M.; Mannel, R.S.; Behbakht, K.; Bakkum-Gamez, J.N.; Michael, H. Randomized Phase III Trial of Gemcitabine Plus Docetaxel Plus Bevacizumab or Placebo as First-Line Treatment for Metastatic Uterine Leiomyosarcoma: An NRG Oncology/Gynecologic Oncology Group Study. J. Clin. Oncol. 2015, 33, 1180–1185. [Google Scholar] [CrossRef]
- Bui, N.Q.; Przybyl, J.; Trabucco, S.E.; Frampton, G.; Hastie, T.; Van De Rijn, M.; Ganjoo, K.N. A clinico-genomic analysis of soft tissue sarcoma patients reveals CDKN2A deletion as a biomarker for poor prognosis. Clin. Sarcoma Res. 2019, 9, 1–11. [Google Scholar] [CrossRef]
- Wei, G.; Antonescu, C.R.; de Alava, E.; Leung, D.; Huvos, A.G.; Meyers, P.A.; Healey, J.H.; Ladanyi, M. Prognostic impact of INK4A deletion in Ewing sarcoma. Cancer 2000, 89, 793–799. [Google Scholar] [CrossRef]
- Lerman, D.M.; Monument, M.J.; McIlvaine, E.; McIlvaine, E.; Liu, X.Q.; Huang, D.; Monovich, L.; Beeler, N.; Gorlick, R.G.; Marina, N.M.; et al. Tumoral TP53 and/or CDKN2A alterations are not reliable prognostic biomarkers in patients with localized Ewing sarcoma: A report from the Children’s Oncology Group. Pediatr. Blood Cancer 2015, 62, 759–765. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Miller, T.I.; Zoumberos, N.A.; Johnson, B.; Rhodes, D.R.; Tomlins, S.A.; Chan, M.P.; Andea, A.A.; Lucas, D.R.; McHugh, J.B.; Smith, N.; et al. A genomic survey of sarcomas on sun-exposed skin reveals distinctive candidate drivers and potentially targetable mutations. Hum. Pathol. 2020, 102, 60–69. [Google Scholar] [CrossRef]
- Zhu, J.; Tucker, M.; Marin, D.; Gupta, R.T.; Healy, P.; Humeniuk, M.; Jarvis, C.; Zhang, T.; McNamara, M.; George, D.J.; et al. Clinical utility of FoundationOne tissue molecular profiling in men with metastatic prostate cancer. Urol. Oncol. Semin. Orig. Investig. 2019, 37, 813.e1–813.e9. [Google Scholar] [CrossRef]
- Dyson, N.J. RB1: A prototype tumor suppressor and an enigma. Genes Dev. 2016, 30, 1492–1502. [Google Scholar] [CrossRef] [PubMed]
- Foulkes, W.D.; Flanders, T.Y.; Pollock, P.M.; Hayward, N.K. The CDKN2A (p16) Gene and Human Cancer. Mol. Med. 1997, 3, 5–20. [Google Scholar] [CrossRef]
- Bargonetti, J.; Prives, C. Gain-of-function mutant p53: History and speculation. J. Mol. Cell Biol. 2019, 11, 605–609. [Google Scholar] [CrossRef] [PubMed]
- Jia, P.; Zhao, Z. Characterization of Tumor-Suppressor Gene Inactivation Events in 33 Cancer Types. Cell Rep. 2019, 26, 496–506.e3. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Sánchez-Tilló, E.; Lu, X.; Clem, B.; Telang, S.; Jenson, A.B.; Cuatrecasas, M.; Chesney, J.; Postigo, A.; Dean, D.C. Rb1 family mutation is sufficient for sarcoma initiation. Nat. Commun. 2013, 4, 2650. [Google Scholar] [CrossRef]
- Pereira, J.R.; Fein, L.; Del Giglio, A.; Blajman, C.R.; Richardet, E.; Schwartsmann, G.; Orlando, M.; Hall, B.J.; West, T.M.; Van Kooten, M. Gemcitabine administered as a short infusion versus a fixed dose rate in combination with cisplatin for the treatment of patients with advanced non-small cell lung cancer. Lung Cancer 2007, 58, 80–87. [Google Scholar] [CrossRef]
- Veltkamp, S.A.; Beijnen, J.H.; Schellens, J.H.M. Prolonged Versus Standard Gemcitabine Infusion: Translation of Molecular Pharmacology to New Treatment Strategy. Oncologist 2008, 13, 261–276. [Google Scholar] [CrossRef] [PubMed]
- Tempero, M.; Plunkett, W.; Van Haperen, V.R.; Hainsworth, J.; Hochster, H.; Lenzi, R.; Abbruzzese, J. Randomized Phase II Comparison of Dose-Intense Gemcitabine: Thirty-Minute Infusion and Fixed Dose Rate Infusion in Patients with Pancreatic Adenocarcinoma. J. Clin. Oncol. 2003, 21, 3402–3408. [Google Scholar] [CrossRef]
- Poplin, E.; Feng, Y.; Berlin, J.; Rothenberg, M.L.; Hochster, H.; Mitchell, E.; Alberts, S.; O’Dwyer, P.; Haller, D.; Catalano, P.; et al. Phase III, Randomized Study of Gemcitabine and Oxaliplatin Versus Gemcitabine (fixed-dose rate infusion) Compared with Gemcitabine (30-min infusion) in Patients with Pancreatic Carcinoma E6201: A Trial of the Eastern Cooperative Oncology Group. J. Clin. Oncol. 2009, 27, 3778–3785. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, E.S.; Nambiar, R.; Rosario, S.R.; Smiraglia, D.J.; Goodrich, D.W.; Witkiewicz, A.K. Pan-cancer molecular analysis of the RB tumor suppressor pathway. Commun. Biol. 2020, 3, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Babenko, O.V.; Zemliakova, V.V.; Saakian, S.V.; Brovkina, A.F.; Strel’Nikov, V.V.; Zaletaev, D.V.; Nemtsova, M.V. RB1 and CDKN2A functional defects resulting in retinoblastoma. Mol. Biol. 2002, 36, 777–783. [Google Scholar] [PubMed]
- Sherr, C.J. The INK4a/ARF network in tumour suppression. Nat. Rev. Mol. Cell Biol. 2001, 2, 731–737. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | 14-Day Regimen (N = 79) | 21-Day Regimen (N = 82) | p-Value | ||
|---|---|---|---|---|---|
| Age | 61 (25–81) | 60 (22–85) | 0.92 | ||
| Sex (Female) (%) | 49 (62) | 55 (67.1) | 0.50 | ||
| Median follow-up (month) | 9.3 (0.1–41) | 9.5 (1.5–46) | N/A | ||
| Ethnicity | White (%) | 40 (50.6) | 50 (61) | 0.69 | |
| Hispanic (%) | 14 (17.7) | 21 (25.6) | |||
| Asian (%) | 19 (24.1) | 7 (8.5) | |||
| Black (%) | 6 (7.6) | 4 (4.9) | |||
| Histology | LMS (%) | 39 (49) | 39 (47.5) | 0.78 | |
| Non-LMS (%) | 40 (51) | 43 (52.5) | |||
| Non-LMS subtypes | UPS (%) | 8 (10.1) | 10 (12.2) | 0.82 | |
| LPS (%) | 7 (8.9) | 10 (12.2) | |||
| Bone sarcoma (%) | 3 (3.4) | 4 (4.5) | |||
| Others (%) | 22 (27.8) | 19 (23.2) | |||
| RP sarcoma (%) | 11 (13.9) | 10 (12.2) | 0.75 | ||
| Median cycles of G-D chemotherapy administered | 5 (1–33) | 5 (1–18) | N/A | ||
| Line of chemotherapy administered | 1st (%) | 47 (59.5) | 52 (63.4) | 0.41 | |
| 2nd (%) | 27 (34.2) | 22 (26.8) | |||
| Later (%) | 5 (6.3) | 8 (9.8) | |||
| Physical Performance | ECOG 0 to 1 | 63 (79.7) | 64 (78.5) | 0.75 | |
| ECOG 2 to 4 | 16 (20.2) | 18 (21.5) | |||
| Gemcitabine | 1000 mg/m2 (%) | 63 (80) | N/A | ||
| 1250 mg/m2 (%) | 2 (2.5) | ||||
| 1500 mg/m2 (%) | 14 (17.5) | ||||
| Docetaxel | 50 mg/m2 (%) | 73 (92.5) | |||
| <50 mg/m2 (%) | 6 (7.5) | ||||
| Gemcitabine | 900 mg/m2 (%) | 75 (91.5) | N/A | ||
| 750 mg/m2 (%) | 1 (1.2) | ||||
| 675 mg/m2 (%) | 6 (7.3) | ||||
| Docetaxel | 60 mg/m2 (%) | 1 (1.2) | N/A | ||
| 75 mg/m2 (%) | 72 (87.8) | ||||
| 100 mg/m2 (%) | 9 (11.0) | ||||
| Filgrastim administered (%) | 77 (97.5) | 82 (100) | 0.15 | ||
| Prior chemotherapy if 2nd and later line | Doxorubicin-based (%) | 62 (78) | 72 (88) | 0.09 | |
| Others (%) | 17 (22) | 10 (12) | |||
| Genomic alterations (N = 67) | N = 36 | N = 31 | |||
| CDKN2A del/mut/CDK4 amp (%) | 11 (30.5) | 4 (12.9) | 0.08 | ||
| RB1 del/mut (%) | 10 (27.8) | 8 (25.8) | 0.85 | ||
| TP53 del/mut/MDM2 amp (%) | 18 (50) | 19 (61.3) | 0.36 | ||
| PFS, OS, and Toxicities | 14-Day Regimen (N = 79) | 21-Day Regimen (N = 82) | p-Value |
|---|---|---|---|
| RR | 22.8% | 15.8% | 0.26 |
| Median PFS (month) | 4.0 (0.03–36.5) | 3.2 (0.3–17.7) | 0.15 |
| Median OS (month) | 12.6 (0.9–39.2) | 14.7 (0.4–46.6) | 0.55 |
| Febrile neutropenia (%) | 1 (1.3) | 10 (12.2) | 0.006 |
| Intolerance (%) | 2 (2.5) | 12 (14.6) | 0.006 |
| Peripheral neuropathy (%) | 8 (10.1) | 10 (12.2) | 0.67 |
| Anemia (hemoglobin < 10/dL) | (%) 45 (57.5) | 56 (68.4) | 0.15 |
| Thrombocytopenia (<100.000/mm3) (%) | 7 (8.9) | 17 (20.5) | 0.03 |
| Diarrhea (%) | 5 (6.3) | 7 (8.5) | 0.74 |
| PFS and OS | 14-Day Regimen (Month) | 21-Day Regimen (Month) | p-Value |
|---|---|---|---|
| First-line Median PFS | 5.2 (2.7–7.7) | 3.2 (2.2–4.0) | 0.01 |
| First-line median OS | 25.2 (9.5–40.0) | 17.6 (7.1–20.9) | 0.57 |
| LMS median PFS | 4.9 (2.8–8.6) | 3.8 (2.1–4.6) | 0.01 |
| LMS median OS | 29.7 (14.8–29.7) | 16.7 (9.8–30.0) | 0.2 |
| N = 67 | RR | PFS (Month) | OS (Month) | |
|---|---|---|---|---|
| CDK4amp/ CDKN2A del/mut | Yes (N = 15) | 6.7% | 3.0 | 10.1 |
| No (N = 52) | 23.1% | 4.9 | 17.6 | |
| p-value | 0.16 | 0.37 | 0.06 | |
| RB1 del/mut | Yes (N = 18) | 33.3% | 6.2 | 17.6 |
| No (N = 49) | 14.3% | 3.2 | 16.9 | |
| p-value | 0.08 | 0.05 | 0.42 | |
| TP53 del/mut, MDM2 amp | Yes (N = 37) | 13.5% | 3.9 | 16.9 |
| No (N = 30) | 26.7% | 5.6 | 25.2 | |
| p-value | 0.18 | 0.57 | 0.65 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pan, M.; Trieu, M.K.; Sidhu, M.; Yu, J.; Seto, T.; Ganjoo, K. Fourteen-Day Gemcitabine-Docetaxel Chemotherapy Is Effective and Safer Compared to 21-Day Regimen in Patients with Advanced Soft Tissue and Bone Sarcoma. Cancers 2021, 13, 1983. https://doi.org/10.3390/cancers13081983
Pan M, Trieu MK, Sidhu M, Yu J, Seto T, Ganjoo K. Fourteen-Day Gemcitabine-Docetaxel Chemotherapy Is Effective and Safer Compared to 21-Day Regimen in Patients with Advanced Soft Tissue and Bone Sarcoma. Cancers. 2021; 13(8):1983. https://doi.org/10.3390/cancers13081983
Chicago/Turabian StylePan, Minggui, Maily K. Trieu, Manpreet Sidhu, Jeanette Yu, Tiffany Seto, and Kristen Ganjoo. 2021. "Fourteen-Day Gemcitabine-Docetaxel Chemotherapy Is Effective and Safer Compared to 21-Day Regimen in Patients with Advanced Soft Tissue and Bone Sarcoma" Cancers 13, no. 8: 1983. https://doi.org/10.3390/cancers13081983
APA StylePan, M., Trieu, M. K., Sidhu, M., Yu, J., Seto, T., & Ganjoo, K. (2021). Fourteen-Day Gemcitabine-Docetaxel Chemotherapy Is Effective and Safer Compared to 21-Day Regimen in Patients with Advanced Soft Tissue and Bone Sarcoma. Cancers, 13(8), 1983. https://doi.org/10.3390/cancers13081983