
Microsatellite Instability, Epstein–Barr Virus, and Programmed Cell Death Ligand 1 as Predictive Markers for Immunotherapy in Gastric Cancer

 , , , , , , ,
, , , , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Investigation of Potential Biomarkers for Immunotherapy
2.3. Clinical Response, Durations of Response, and Survival Analysis
2.4. Tumor Mutation Burden (TMB) and Tumor Infiltrating Lymphocytes (TILs) Analysis Using TCGA Database
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Overall Response Rates (ORRs) and Progression-Free Survival (PFS) in Patients with Different Biomarkers
3.3. ORRs and PFS in Different Cut-Off Levels of CPS (CPS ≥ 1, ≥ 5, and ≥ 10)
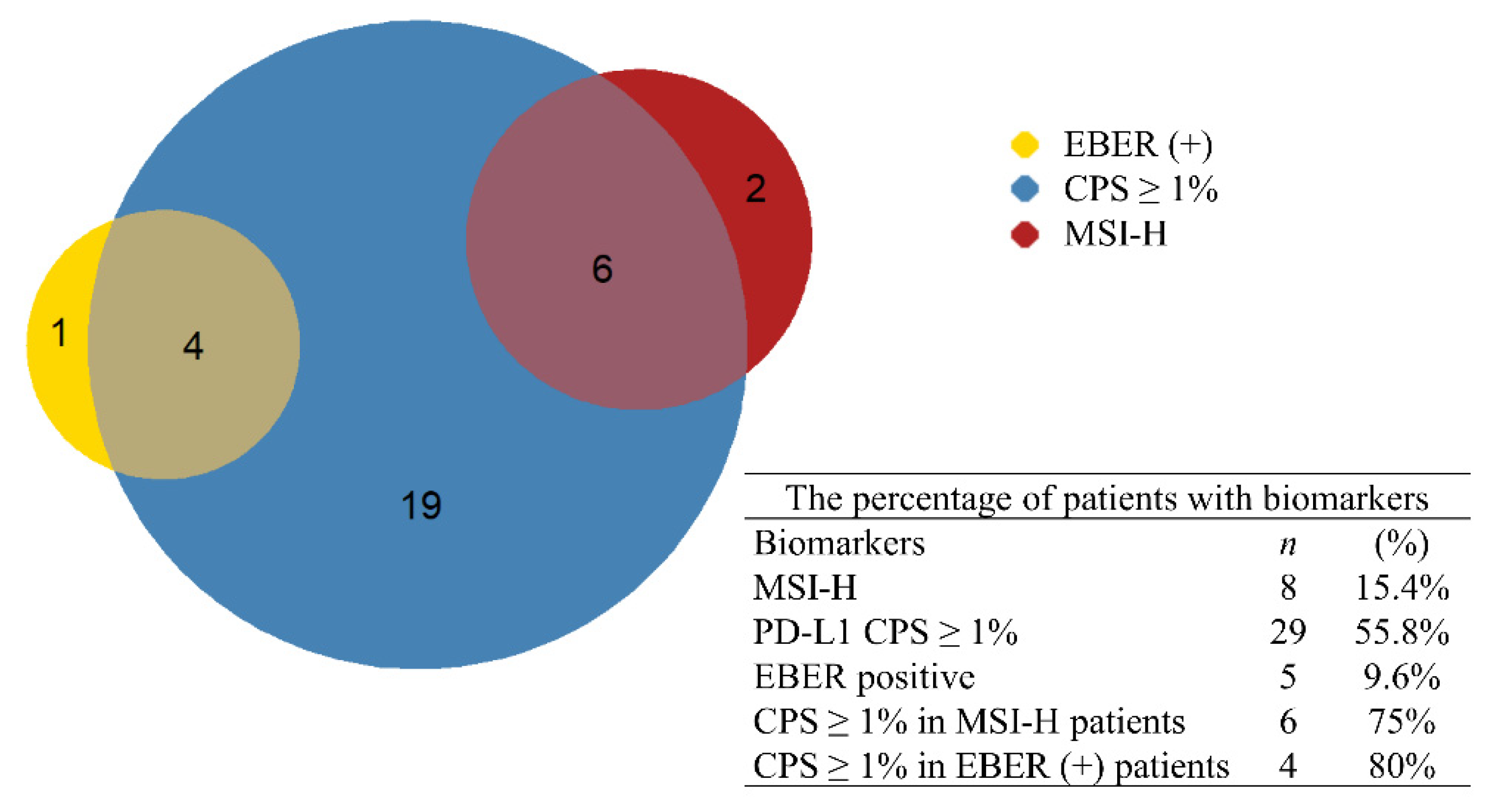
3.4. Combined Biomarkers: Incidence, ORR, and PFS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Bass, A.J.; Thorsson, V.; Shmulevich, I.; Reynolds, S.M.; Miller, M.; Bernard, B.; Hinoue, T.; Laird, P.W.; Curtis, C.; Shen, H.; et al. Comprehensive molecular characterization of gastric adenocarcinoma. Nature 2014, 513, 202–209. [Google Scholar] [CrossRef] [Green Version]
- Camargo, M.C.; Kim, W.H.; Chiaravalli, A.M.; Kim, K.M.; Corvalan, A.H.; Matsuo, K.; Yu, J.; Sung, J.J.; Herrera-Goepfert, R.; Meneses-Gonzalez, F.; et al. Improved survival of gastric cancer with tumour Epstein-Barr virus positivity: An international pooled analysis. Gut 2014, 63, 236–243. [Google Scholar] [CrossRef]
- Sun, K.; Jia, K.; Lv, H.; Wang, S.Q.; Wu, Y.; Lei, H.; Chen, X. EBV-Positive Gastric Cancer: Current Knowledge and Future Perspectives. Front. Oncol. 2020, 10, 583463. [Google Scholar] [CrossRef] [PubMed]
- Pietrantonio, F.; Randon, G.; Di Bartolomeo, M.; Luciani, A.; Chao, J.; Smyth, E.C.; Petrelli, F. Predictive role of microsatellite instability for PD-1 blockade in patients with advanced gastric cancer: A meta-analysis of randomized clinical trials. ESMO Open 2021, 6, 100036. [Google Scholar] [CrossRef] [PubMed]
- Puliga, E.; Corso, S.; Pietrantonio, F.; Giordano, S. Microsatellite instability in Gastric Cancer: Between lights and shadows. Cancer Treat. Rev. 2021, 95, 102175. [Google Scholar] [CrossRef]
- Fuchs, C.S.; Doi, T.; Jang, R.W.; Muro, K.; Satoh, T.; Machado, M.; Sun, W.; Jalal, S.I.; Shah, M.A.; Metges, J.P.; et al. Safety and Efficacy of Pembrolizumab Monotherapy in Patients with Previously Treated Advanced Gastric and Gastroesophageal Junction Cancer: Phase 2 Clinical KEYNOTE-059 Trial. JAMA Oncol. 2018, 4, e180013. [Google Scholar] [CrossRef]
- Shitara, K.; Van Cutsem, E.; Bang, Y.J.; Fuchs, C.; Wyrwicz, L.; Lee, K.W.; Kudaba, I.; Garrido, M.; Chung, H.C.; Lee, J.; et al. Efficacy and Safety of Pembrolizumab or Pembrolizumab Plus Chemotherapy vs Chemotherapy Alone for Patients with First-line, Advanced Gastric Cancer: The KEYNOTE-062 Phase 3 Randomized Clinical Trial. JAMA Oncol. 2020, 6, 1571–1580. [Google Scholar] [CrossRef] [PubMed]
- Hsu, J.L.; Glaser, S.L. Epstein-barr virus-associated malignancies: Epidemiologic patterns and etiologic implications. Crit. Rev. Oncol. Hematol. 2000, 34, 27–53. [Google Scholar] [CrossRef]
- Fang, W.L.; Chen, M.H.; Huang, K.H.; Lin, C.H.; Chao, Y.; Lo, S.S.; Li, A.F.; Wu, C.W.; Shyr, Y.M. The Clinicopathological Features and Genetic Alterations in Epstein-Barr Virus-Associated Gastric Cancer Patients after Curative Surgery. Cancers 2020, 12, 1517. [Google Scholar] [CrossRef] [PubMed]
- Murphy, G.; Pfeiffer, R.; Camargo, M.C.; Rabkin, C.S. Meta-analysis shows that prevalence of Epstein-Barr virus-positive gastric cancer differs based on sex and anatomic location. Gastroenterology 2009, 137, 824–833. [Google Scholar] [CrossRef] [Green Version]
- Shinozaki-Ushiku, A.; Kunita, A.; Fukayama, M. Update on Epstein-Barr virus and gastric cancer (review). Int. J. Oncol. 2015, 46, 1421–1434. [Google Scholar] [CrossRef] [Green Version]
- Xie, T.; Liu, Y.; Zhang, Z.; Zhang, X.; Gong, J.; Qi, C.; Li, J.; Shen, L.; Peng, Z. Positive Status of Epstein-Barr Virus as a Biomarker for Gastric Cancer Immunotherapy: A Prospective Observational Study. J. Immunother. 2020, 43, 139–144. [Google Scholar] [CrossRef]
- Polom, K.; Marano, L.; Marrelli, D.; De Luca, R.; Roviello, G.; Savelli, V.; Tan, P.; Roviello, F. Meta-analysis of microsatellite instability in relation to clinicopathological characteristics and overall survival in gastric cancer. J. Br. Surg. 2018, 105, 159–167. [Google Scholar] [CrossRef]
- Bolandi, N.; Derakhshani, A.; Hemmat, N.; Baghbanzadeh, A.; Asadzadeh, Z.; Nour, M.A.; Brunetti, O.; Bernardini, R.; Silvestris, N.; Baradaran, B. The Positive and Negative Immunoregulatory Role of B7 Family: Promising Novel Targets in Gastric Cancer Treatment. Int. J. Mol. Sci. 2021, 22, 10719. [Google Scholar] [CrossRef]
- Garon, E.B.; Rizvi, N.A.; Hui, R.; Leighl, N.; Balmanoukian, A.S.; Eder, J.P.; Patnaik, A.; Aggarwal, C.; Gubens, M.; Horn, L.; et al. Pembrolizumab for the Treatment of Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 372, 2018–2028. [Google Scholar] [CrossRef]
- Kulangara, K.; Zhang, N.; Corigliano, E.; Guerrero, L.; Waldroup, S.; Jaiswal, D.; Ms, M.J.; Shah, S.; Hanks, D.; Wang, J.; et al. Clinical Utility of the Combined Positive Score for Programmed Death Ligand-1 Expression and the Approval of Pembrolizumab for Treatment of Gastric Cancer. Arch. Pathol. Lab. Med. 2019, 143, 330–337. [Google Scholar] [CrossRef] [Green Version]
- Conroy, J.M.; Pabla, S.; Nesline, M.K.; Glenn, S.T.; Papanicolau-Sengos, A.; Burgher, B.; Andreas, J.; Giamo, V.; Wang, Y.; Lenzo, F.L.; et al. Next generation sequencing of PD-L1 for predicting response to immune checkpoint inhibitors. J. Immunother. Cancer 2019, 7, 18. [Google Scholar] [CrossRef] [Green Version]
- Becht, E.; Giraldo, N.A.; Lacroix, L.; Buttard, B.; Elarouci, N.; Petitprez, F.; Selves, J.; Laurent-Puig, P.; Sautes-Fridman, C.; Fridman, W.H.; et al. Estimating the population abundance of tissue-infiltrating immune and stromal cell populations using gene expression. Genome Biol. 2016, 17, 218. [Google Scholar] [CrossRef]
- Ellrott, K.; Bailey, M.H.; Saksena, G.; Covington, K.R.; Kandoth, C.; Stewart, C.; Hess, J.; Ma, S.; Chiotti, K.E.; McLellan, M.; et al. Scalable Open Science Approach for Mutation Calling of Tumor Exomes Using Multiple Genomic Pipelines. Cell Syst. 2018, 6, 271–281.e7. [Google Scholar] [CrossRef] [Green Version]
- Janjigian, Y.Y.; Shitara, K.; Moehler, M.; Garrido, M.; Salman, P.; Shen, L.; Wyrwicz, L.; Yamaguchi, K.; Skoczylas, T.; Bragagnoli, A.C.; et al. First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (CheckMate 649): A randomised, open-label, phase 3 trial. Lancet 2021, 398, 27–40. [Google Scholar] [CrossRef]
- Boku, N.; Ryu, M.H.; Kato, K.; Chung, H.C.; Minashi, K.; Lee, K.W.; Cho, H.; Kang, W.K.; Komatsu, Y.; Tsuda, M.; et al. Safety and efficacy of nivolumab in combination with S-1/capecitabine plus oxaliplatin in patients with previously untreated, unresectable, advanced, or recurrent gastric/gastroesophageal junction cancer: Interim results of a randomized, phase II trial (ATTRACTION-4). Ann. Oncol. 2019, 30, 250–258. [Google Scholar] [CrossRef] [Green Version]
- Kang, Y.K.; Boku, N.; Satoh, T.; Ryu, M.H.; Chao, Y.; Kato, K.; Chung, H.C.; Chen, J.S.; Muro, K.; Kang, W.K.; et al. Nivolumab in patients with advanced gastric or gastro-oesophageal junction cancer refractory to, or intolerant of, at least two previous chemotherapy regimens (ONO-4538-12, ATTRACTION-2): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 390, 2461–2471. [Google Scholar] [CrossRef]
- Zhao, P.; Li, L.; Jiang, X.; Li, Q. Mismatch repair deficiency/microsatellite instability-high as a predictor for anti-PD-1/PD-L1 immunotherapy efficacy. J. Hematol. Oncol. 2019, 12, 54. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, J.; Oliveira, A.; Malta, M.; Oliveira, C.; Silva, F.; Galaghar, A.; Afonso, L.P.; Neves, M.C.; Medeiros, R.; Pimentel-Nunes, P.; et al. Clinical and pathological characterization of Epstein-Barr virus-associated gastric carcinomas in Portugal. World J. Gastroenterol. 2017, 23, 7292–7302. [Google Scholar] [CrossRef] [PubMed]
- Saito, R.; Abe, H.; Kunita, A.; Yamashita, H.; Seto, Y.; Fukayama, M. Overexpression and gene amplification of PD-L1 in cancer cells and PD-L1+ immune cells in Epstein-Barr virus-associated gastric cancer: The prognostic implications. Mod. Pathol. 2017, 30, 427–439. [Google Scholar] [CrossRef] [PubMed]
- Bigras, G.; Mairs, S.; Swanson, P.E.; Morel, D.; Lai, R.; Izevbaye, I. Small Biopsies Misclassify up to 35% of PD-L1 Assessments in Advanced Lung Non-Small Cell Lung Carcinomas. Appl. Immunohistochem. Mol. Morphol. 2018, 26, 701–708. [Google Scholar] [CrossRef]
- Nogueira, C.; Mota, M.; Gradiz, R.; Cipriano, M.A.; Caramelo, F.; Cruz, H.; Alarcão, A.; e Sousa, F.C.; Oliveira, F.; Martinho, F.; et al. Prevalence and characteristics of Epstein-Barr virus-associated gastric carcinomas in Portugal. Infect. Agents Cancer 2017, 12, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakayama, A.; Abe, H.; Kunita, A.; Saito, R.; Kanda, T.; Yamashita, H.; Seto, Y.; Ishikawa, S.; Fukayama, M. Viral loads correlate with upregulation of PD-L1 and worse patient prognosis in Epstein-Barr Virus-associated gastric carcinoma. PLoS ONE 2019, 14, e0211358. [Google Scholar] [CrossRef]
- Koriyama, C.; Akiba, S.; Itoh, T.; Kijima, Y.; Sueyoshi, K.; Corvalan, A.; Herrera-Goepfer, R.; Eizuru, Y. Prognostic significance of Epstein-Barr virus involvement in gastric carcinoma in Japan. Int. J. Mol. Med. 2002, 10, 635–639. [Google Scholar]
- Lee, H.S.; Chang, M.S.; Yang, H.-K.; Lee, B.L.; Kim, W.H. Epstein-Barr Virus-Positive Gastric Carcinoma Has a Distinct Protein Expression Profile in Comparison with Epstein-Barr Virus-Negative Carcinoma. Clin. Cancer Res. 2004, 10, 1698–1705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cristescu, R.; Lee, J.; Nebozhyn, M.; Kim, K.-M.; Ting, J.C.; Wong, S.S.; Liu, J.; Yue, Y.G.; Wang, J.; Yu, K.; et al. Molecular analysis of gastric cancer identifies subtypes associated with distinct clinical outcomes. Nat. Med. 2015, 21, 449–456. [Google Scholar] [CrossRef]
- Cai, L.; Sun, Y.; Wang, K.; Guan, W.; Yue, J.; Li, J.; Wang, R.; Wang, L. The Better Survival of MSI Subtype Is Associated with the Oxidative Stress Related Pathways in Gastric Cancer. Front. Oncol. 2020, 10, 1269. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Patel, K.; Singhi, A.D.; Ren, B.; Zhu, B.; Shaikh, F.; Sun, W. Programmed Death-Ligand 1 Expression Is Common in Gastric Cancer Associated with Epstein-Barr Virus or Microsatellite Instability. Am. J. Surg. Pathol. 2016, 40, 1496–1506. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | n | Range/Percentage |
|---|---|---|
| Age (years) | 65.5 | 20–93 |
| Sex(male) | 23 | 44.2% |
| Staging IV | 39 | 75% |
| ECOG 0–1 | 48 | 92.3% |
| Normal liver function | 48 | 92.3% |
| Normal renal function | 48 | 92.3% |
| Biomarkers | ||
| MMR | 8 | 15.4% |
| EBER | 5 | 9.6% |
| PD-L1 | ||
| ≥1 | 29 | 55.8% |
| ≥5 | 9 | 17.3% |
| ≥10 | 6 | 11.5% |
| Lines of treatment | ||
| 1st | 10 | 19.2% |
| 2nd | 10 | 19.2% |
| 3rd or later | 32 | 61.5% |
| Immunotherapy | ||
| Nivolumab | 38 | 73.1% |
| Pembrolizumab | 12 | 23.1% |
| Atezolizumab | 2 | 3.8% |
| Treatment courses | 6 | 1–64 |
| Previous therapies | ||
| Previous surgery | ||
| Curative | 19 | 36.5% |
| Palliative | 12 | 23.1% |
| No surgery | 21 | 40.4% |
| RT at primary tumor | 12 | 23.1% |
| Cisplatin | 10 | 19.2% |
| Oxaliplatin | 32 | 61.5% |
| 5-FU | 22 | 42.3% |
| Taxanes | 27 | 51.9% |
| Response | All Negative | CPS1 | MSI-H | EBER |
|---|---|---|---|---|
| CR | 0 | 3 | 0 | 1 |
| PR | 3 | 10 | 6 | 2 |
| SD | 12 | 3 | 1 | 0 |
| PD | 5 | 13 | 1 | 2 |
| ORR | 15.0% | 44.8% | 75% | 60% |
| p | 0.035 | 0.005 | 0.07 |
| Response | All Negative | CPS ≥ 1 | CPS ≥ 5 | EBER ≥ 10 |
|---|---|---|---|---|
| CR | 0 | 3 | 3 | 3 |
| PR | 3 | 10 | 3 | 2 |
| SD | 12 | 3 | 1 | 0 |
| PD | 5 | 13 | 2 | 1 |
| ORR | 15.0% | 44.8% | 66.7% | 83.3% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, H.-Y.; Li, C.-P.; Huang, Y.-H.; Hsu, S.-J.; Wang, Y.-P.; Hsieh, Y.-C.; Fang, W.-L.; Huang, K.-H.; Li, A.F.-Y.; Lee, R.-C.; et al. Microsatellite Instability, Epstein–Barr Virus, and Programmed Cell Death Ligand 1 as Predictive Markers for Immunotherapy in Gastric Cancer. Cancers 2022, 14, 218. https://doi.org/10.3390/cancers14010218
Yu H-Y, Li C-P, Huang Y-H, Hsu S-J, Wang Y-P, Hsieh Y-C, Fang W-L, Huang K-H, Li AF-Y, Lee R-C, et al. Microsatellite Instability, Epstein–Barr Virus, and Programmed Cell Death Ligand 1 as Predictive Markers for Immunotherapy in Gastric Cancer. Cancers. 2022; 14(1):218. https://doi.org/10.3390/cancers14010218
Chicago/Turabian StyleYu, Hung-Yuan, Chung-Pin Li, Yi-Hsiang Huang, Shao-Jung Hsu, Yen-Po Wang, Yun-Cheng Hsieh, Wen-Liang Fang, Kuo-Hung Huang, Anna Fen-Yau Li, Rheun-Chuan Lee, and et al. 2022. "Microsatellite Instability, Epstein–Barr Virus, and Programmed Cell Death Ligand 1 as Predictive Markers for Immunotherapy in Gastric Cancer" Cancers 14, no. 1: 218. https://doi.org/10.3390/cancers14010218
APA StyleYu, H. -Y., Li, C. -P., Huang, Y. -H., Hsu, S. -J., Wang, Y. -P., Hsieh, Y. -C., Fang, W. -L., Huang, K. -H., Li, A. F. -Y., Lee, R. -C., Lee, K. -L., Wu, Y. -H., Lai, I. -C., Yang, W. -C., Hung, Y. -P., Wang, Y. -C., Chen, S. -H., Chen, M. -H., & Chao, Y. (2022). Microsatellite Instability, Epstein–Barr Virus, and Programmed Cell Death Ligand 1 as Predictive Markers for Immunotherapy in Gastric Cancer. Cancers, 14(1), 218. https://doi.org/10.3390/cancers14010218