
The Impact of Resampling and Denoising Deep Learning Algorithms on Radiomics in Brain Metastases MRI

 , , ,
, , ,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Magnetic Resonance Imaging (MRI) Acquisition
2.3. Dataset, Resampling and Denoisning DL Models
- MSE: Mean Squared Error
- MGE: Mean Gradient Error
- MS_SSIM: Multi-Scale SSIM corresponding to multiple SSIM image evaluations at different image scales [22].
- N: Number of batch over which SSIM has been averaged
- and : Mean of patches PY and , respectively
- and : Deviation of patches PY and , respectively
- and : Constants
2.4. Image Processing, Radiomics Extraction and Analysis
2.5. Statistical Analysis
3. Results
3.1. Resampling DL Model
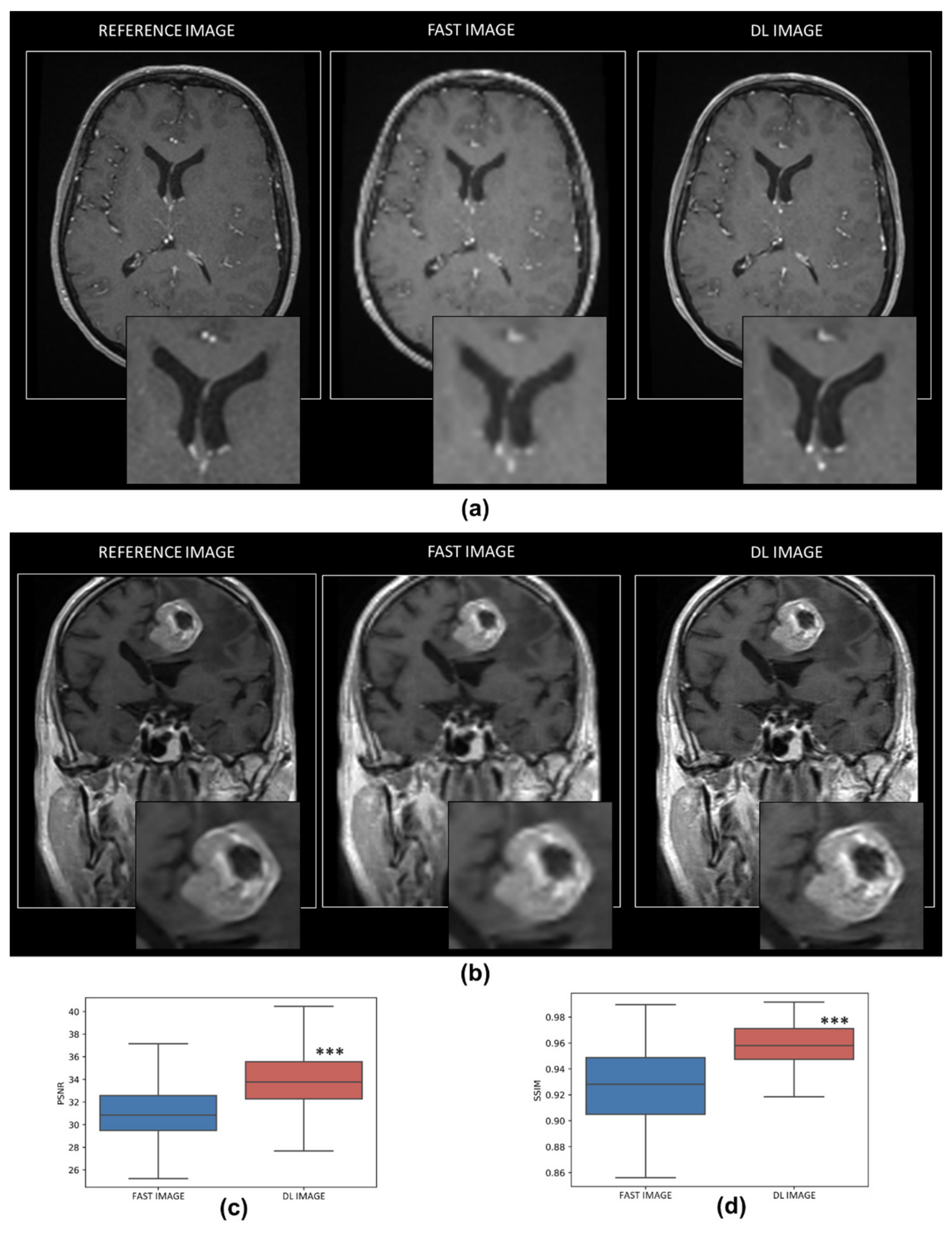
3.1.1. Quality of the Resampling DL Model
3.1.2. Impact of Resampling DL Model on Radiomics Features
3.2. Denoising DL Model
3.2.1. Quality of the Denoising DL Model
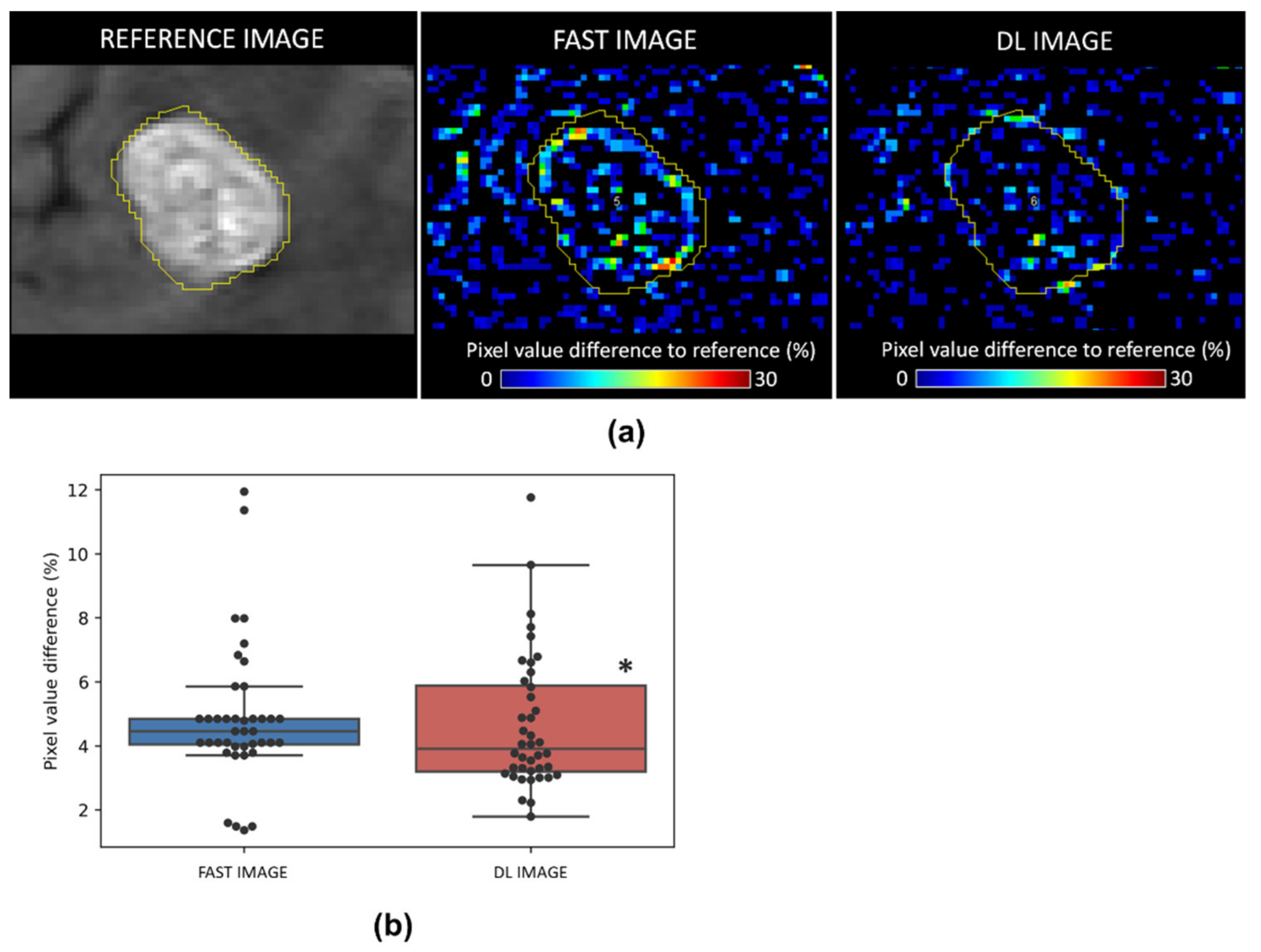
3.2.2. Impact of Denoising DL Model on Radiomics Features
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- OECD Statistiques. Available online: https://stats.oecd.org (accessed on 21 December 2021).
- Graciet, A.; Detournay, B.; Courouve, L. Les Insuffisances En Matière D’équipements D’imagerie Médicale En France; Banque de Données en Santé Publique: Bourg-la-Reine, France, 2018; Volume 33. [Google Scholar]
- McGibney, G.; Smith, M.R.; Nichols, S.T.; Crawley, A. Quantitative Evaluation of Several Partial Fourier Reconstruction Algorithms Used in MRI. Magn. Reson. Med. 1993, 30, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Pruessmann, K.P.; Weiger, M.; Scheidegger, M.B.; Boesiger, P. SENSE: Sensitivity Encoding for Fast MRI. Magn. Reson. Med. 1999, 42, 952–962. [Google Scholar] [CrossRef]
- Jaspan, O.N.; Fleysher, R.; Lipton, M.L. Compressed Sensing MRI: A Review of the Clinical Literature. Br. J. Radiol. 2015, 88, 20150487. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Preininger, A. AI in Health: State of the Art, Challenges, and Future Directions. Yearb. Med. Inf. 2019, 28, 16–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahuja, A.S. The Impact of Artificial Intelligence in Medicine on the Future Role of the Physician. PeerJ 2019, 2019, e7702. [Google Scholar] [CrossRef]
- Knoll, F.; Zbontar, J.; Sriram, A.; Muckley, M.J.; Bruno, M.; Defazio, A.; Parente, M.; Geras, K.J.; Katsnelson, J.; Chandarana, H.; et al. FastMRI: A Publicly Available Raw k-Space and DICOM Dataset of Knee Images for Accelerated MR Image Reconstruction Using Machine Learning. Radiol. Artif. Intell. 2020, 2, e190007. [Google Scholar] [CrossRef] [PubMed]
- Reina, G.A.; Stassen, M.; Pezzotti, N. White Paper Philips Healthcare Uses the Intel® Distribution of OpenVINOTM Toolkit and the Intel® DevCloud for the Edge to Accelerate Compressed Sensing Image Reconstruction Algorithms for MRI Authors. Available online: https://www.intel.com/content/dam/www/public/us/en/documents/white-papers/philips-healthcare-mri-white-paper.pdf (accessed on 21 December 2021).
- Behl, N. Deep Resolve—Mobilizing the Power of Networks. Available online: https://cdn0.scrvt.com/39b415fb07de4d9656c7b516d8e2d907/cc86f5120c06595c/d13b5f98477c/siemens-healthineers_MR_Deep_Resolve_Whitepaper.pdf (accessed on 21 December 2021).
- Zaharchuk, X.G.; Gong, X.E.; Wintermark, X.M.; Rubin, X.D.; Langlotz, X.C.P. Deep Learning in Neuroradiology. Am. J. Neuroradiol. 2018, 39, 1776–1784. [Google Scholar] [CrossRef] [Green Version]
- Shi, W.; Caballero, J.; Huszar, F.; Totz, J.; Aitken, A.P.; Bishop, R.; Rueckert, D.; Wang, Z. Real-Time Single Image and Video Super-Resolution Using an Efficient Sub-Pixel Convolutional Neural Network. IEEE Comput. Soc. Conf. Comput. Vis. Pattern Recognit. 2016, 12, 1874–1883. [Google Scholar] [CrossRef] [Green Version]
- Lu, Z.; Chen, Y. Single Image Super Resolution Based on a Modified U-Net with Mixed Gradient Loss. arXiv 2019, arXiv:1911.09428. [Google Scholar] [CrossRef]
- Lambin, P.; Rios-Velazquez, E.; Leijenaar, R.; Carvalho, S.; Van Stiphout, R.G.P.M.; Granton, P.; Zegers, C.M.L.; Gillies, R.; Boellard, R.; Dekker, A.; et al. Radiomics: Extracting More Information from Medical Images Using Advanced Feature Analysis. Eur. J. Cancer 2012, 48, 441–446. [Google Scholar] [CrossRef] [Green Version]
- Aerts, H.J.W.L.; Velazquez, E.R.; Leijenaar, R.T.H.; Parmar, C.; Grossmann, P.; Cavalho, S.; Bussink, J.; Monshouwer, R.; Haibe-Kains, B.; Rietveld, D.; et al. Decoding Tumour Phenotype by Noninvasive Imaging Using a Quantitative Radiomics Approach. Nat. Commun. 2014, 5. [Google Scholar] [CrossRef] [PubMed]
- Lohmann, P.; Kocher, M.; Ruge, M.I.; Visser-Vandewalle, V.; Shah, N.J.; Fink, G.R.; Langen, K.J.; Galldiks, N. PET/MRI Radiomics in Patients with Brain Metastases. Front. Neurol. 2020, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hatt, M.; Cheze Le Rest, C.; Antonorsi, N.; Tixier, F.; Tankyevych, O.; Jaouen, V.; Lucia, F.; Bourbonne, V.; Schick, U.; Badic, B.; et al. Radiomics in PET/CT: Current Status and Future AI-Based Evolutions. Semin. Nucl. Med. 2021, 51, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Edelstein, W.A.; Glover, G.H.; Hardy, C.J.; Redington, R.W. The Intrinsic Signal-to-noise Ratio in NMR Imaging. Magn. Reson. Med. 1986, 3, 604–618. [Google Scholar] [CrossRef] [PubMed]
- Macovski, A. Noise in MRI. Magn. Reson. Med. 1996, 36, 494–497. [Google Scholar] [CrossRef]
- Chollet, F. Keras 2015. Available online: https://github.com/fchollet/keras (accessed on 21 December 2021).
- Weng, W.; Zhu, X. U-Net: Convolutional Networks for Biomedical Image Segmentation. IEEE Access 2021, 9, 16591–16603. [Google Scholar] [CrossRef]
- Wang, Z.; Simoncelli, E.P.; Bovik, A.C. Multiscale Structural Similarity for Image Quality Assessment. In Proceedings of the Thrity-Seventh Asilomar Conference on Signals, Systems & Computers, Pacific Grove, CA, USA, 9–12 November 2003; IEEE: New York, NY, USA, 2003; Volume 2, pp. 1398–1402. [Google Scholar]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an Image Computing Platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [Green Version]
- Schneider, C.A.; Rasband, W.S.; Eliceiri, K.W. NIH Image to ImageJ: 25 Years of Image Analysis. Nat. Methods 2012, 9, 671–675. [Google Scholar] [CrossRef] [PubMed]
- Egger, J.; Kapur, T.; Fedorov, A.; Pieper, S.; Miller, J.V.; Veeraraghavan, H.; Freisleben, B.; Golby, A.J.; Nimsky, C.; Kikinis, R. GBM Volumetry Using the 3D Slicer Medical Image Computing Platform. Sci. Rep. 2013, 3, 1364. [Google Scholar] [CrossRef]
- Van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin, J.C.; Pieper, S.; Aerts, H.J.W.L. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaudet, C.; Weyts, K.; Lechervy, A.; Batalla, A.; Bardet, S.; Corroyer-Dulmont, A. The Impact of Artificial Intelligence CNN Based Denoising on FDG PET Radiomics. Front. Oncol. 2021, 11, 3136. [Google Scholar] [CrossRef] [PubMed]
- Zwanenburg, A.; Vallières, M.; Abdalah, M.A.; Aerts, H.J.W.L.; Andrearczyk, V.; Apte, A.; Ashrafinia, S.; Bakas, S.; Beukinga, R.J.; Boellaard, R.; et al. The Image Biomarker Standardization Initiative: Standardized Quantitative Radiomics for High-Throughput Image-Based Phenotyping. Radiology 2020, 295, 328–338. [Google Scholar] [CrossRef] [Green Version]
- Liao, C.-Y.; Lee, C.-C.; Yang, H.-C.; Chen, C.-J.; Chung, W.-Y.; Wu, H.-M.; Guo, W.; Liu, R.; Lu, C. Enhancement of Radiosurgical Treatment Outcome Prediction Using MRI Radiomics in Patients with Non-Small Cell Lung Cancer Brain Metastases. Cancers 2021, 13, 4030. [Google Scholar] [CrossRef] [PubMed]
- Su, C.Q.; Chen, X.T.; Duan, S.F.; Zhang, J.X.; You, Y.P.; Lu, S.S.; Hong, X.N. A Radiomics-Based Model to Differentiate Glioblastoma from Solitary Brain Metastases. Clin. Radiol. 2021, 76, 629.e11–629.e18. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.I.-K. A Concordance Correlation Coefficient to Evaluate Reproducibility. Biometrics 1989, 45, 255–268. [Google Scholar] [CrossRef] [PubMed]
- Peerlings, J.; Woodruff, H.C.; Winfield, J.M.; Ibrahim, A.; Van Beers, B.E.; Heerschap, A.; Jackson, A.; Wildberger, J.E.; Mottaghy, F.M.; DeSouza, N.M.; et al. Stability of Radiomics Features in Apparent Diffusion Coefficient Maps from a Multi-Centre Test-Retest Trial. Sci. Rep. 2019, 9, 4800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anaconda Software Distribution. (2020). Anaconda Documentation. Anaconda Inc. Available online: https://docs.anaconda.com (accessed on 21 December 2021).
- Keys, R. Cubic Convolution Interpolation for Digital Image Processing. IEEE Trans. Acoust. 1981, 29, 1153–1160. [Google Scholar] [CrossRef] [Green Version]
- Makinen, Y.; Azzari, L.; Foi, A. Collaborative Filtering of Correlated Noise: Exact Transform-Domain Variance for Improved Shrinkage and Patch Matching. IEEE Trans. Image Process. 2020, 29, 8339–8354. [Google Scholar] [CrossRef]
- Kim, J.; Lee, J.K.; Lee, K.M. Accurate Image Super-Resolution Using Very Deep Convolutional Networks. IEEE Comput. Soc. Conf. Comput. Vis. Pattern Recognit. 2016, 2016, 1646–1654. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Li, K.; Li, K.; Wang, L.; Zhong, B.; Fu, Y. Image Super-Resolution Using Very Deep Residual Channel Attention Networks. Lect. Notes Comput. Sci. 2018, 11211, 294–310. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J.P.; Luck, M.; Honari, S. Distribution Matching Losses Can Hallucinate Features in Medical Image Translation. Lect. Notes Comput. Sci. 2018, 11070, 529–536. [Google Scholar] [CrossRef] [Green Version]
- Ulyanov, D.; Vedaldi, A.; Lempitsky, V. Deep Image Prior. Int. J. Comput. Vis. 2020, 128, 1867–1888. [Google Scholar] [CrossRef]
- Zhang, K.; Zuo, W.; Chen, Y.; Meng, D.; Zhang, L. Beyond a Gaussian Denoiser: Residual Learning of Deep CNN for Image Denoising. IEEE Trans. Image Process. 2017, 26, 3142–3155. [Google Scholar] [CrossRef] [Green Version]
- Imai, K.; Miyata, T. Gated Texture CNN for Efficient and Configurable Image Denoising. Lect. Notes Comput. Sci. 2020, 12537, 665–681. [Google Scholar] [CrossRef]
- Gondara, L. Medical Image Denoising Using Convolutional Denoising Autoencoders. In Proceedings of the 2016 IEEE 16th International Conference on Data Mining Workshops (ICDMW), Barcelona, Spain, 12–15 December 2016; pp. 241–246. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; Chae, Y.; Stenger, B.; Datta, A. Residual Dense Network for Image Super Resolution. Int. Conf. Image Process. 2018, 71–75. [Google Scholar] [CrossRef]
- Zhao, H.; Gallo, O.; Frosio, I.; Kautz, J. Loss Functions for Image Restoration with Neural Networks. IEEE Trans. Comput. Imaging 2017, 3, 47–57. [Google Scholar] [CrossRef]
- Johnson, J.; Alahi, A.; Fei-Fei, L. Perceptual Losses for Real-Time Style Transfer and Super-Resolution. Lect. Notes Comput. Sci. 2016, 9906, 694–711. [Google Scholar] [CrossRef] [Green Version]
- Tamada, D.; Kromrey, M.L.; Ichikawa, S.; Onishi, H.; Motosugi, U. Motion Artifact Reduction Using a Convolutional Neural Network for Dynamic Contrast Enhanced Mr Imaging of the Liver. Magn. Reson. Med. Sci. 2020, 19, 64–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leijenaar, R.T.H.; Carvalho, S.; Velazquez, E.R.; Van Elmpt, W.J.C.; Parmar, C.; Hoekstra, O.S.; Hoekstra, C.J.; Boellaard, R.; Dekker, A.L.A.J.; Gillies, R.J.; et al. Stability of FDG-PET Radiomics Features: An Integrated Analysis of Test-Retest and Inter-Observer Variability. Acta Oncol. 2013, 52, 1391–1397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larue, R.T.H.M.; Van De Voorde, L.; van Timmeren, J.E.; Leijenaar, R.T.H.; Berbée, M.; Sosef, M.N.; Schreurs, W.M.J.; van Elmpt, W.; Lambin, P. 4DCT Imaging to Assess Radiomics Feature Stability: An Investigation for Thoracic Cancers. Radiother. Oncol. 2017, 125, 147–153. [Google Scholar] [CrossRef] [Green Version]
- Van Timmeren, J.E.; Leijenaar, R.T.H.; van Elmpt, W.; Wang, J.; Zhang, Z.; Dekker, A.; Lambin, P. Test-Retest Data for Radiomics Feature Stability Analysis: Generalizable or Study-Specific? Tomography 2016, 2, 361–365. [Google Scholar] [CrossRef]
- Gao, R.; Grauman, K. On-Demand Learning for Deep Image Restoration. IEEE Int. Conf. Comput. Vis. 2017, 2017, 1095–1104. [Google Scholar] [CrossRef] [Green Version]
- Yi, X.; Pei, Q.; Zhang, Y.; Zhu, H.; Wang, Z.; Chen, C.; Li, Q.; Long, X.; Tan, F.; Zhou, Z.; et al. MRI-Based Radiomics Predicts Tumor Response to Neoadjuvant Chemoradiotherapy in Locally Advanced Rectal Cancer. Front. Oncol. 2019, 9, 552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaalep, A.; Burggraaff, C.N.; Pieplenbosch, S.; Verwer, E.E.; Sera, T.; Zijlstra, J.; Hoekstra, O.S.; Oprea-Lager, D.E.; Boellaard, R. Quantitative Implications of the Updated EARL 2019 PET-CT Performance Standards. EJNMMI Phys. 2019, 6, 28. [Google Scholar] [CrossRef] [PubMed]
- Aide, N.; Lasnon, C.; Veit-Haibach, P.; Sera, T.; Sattler, B.; Boellaard, R. EANM/EARL Harmonization Strategies in PET Quantification: From Daily Practice to Multicentre Oncological Studies. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 17–31. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Included Patients (N) | 85 | Number |
|---|---|---|
| Sex | 58 | Female % |
| Age (Y) | 66.48 ± 10.31 | Mean ± SD |
| (46–88) | [range] | |
| Origin of BM | Number (%) | |
| Lung | 42 (48%) | |
| Breast | 28 (32%) | |
| Kidney | 6 (6.9%) | |
| Digestive System | 3 (3.4%) | |
| Melanoma | 3 (3.4%) | |
| Gynecologic | 2 (2.3%) | |
| Classes | Features | Signicantly Different | Classes | Features | Signicantly Different |
|---|---|---|---|---|---|
| Intensity | Min | NS p = 0.73 | Gray Level Dependence Matrix | gldm_DependenceEntropy | *** |
| gldm_DependenceNonUniformity | * | ||||
| gldm_DependenceNonUniformityNormalized | ** | ||||
| Max | NS p = 0.47 | gldm_DependenceVariance | * | ||
| Peak | NS p = 0.27 | gldm_GrayLevelNonUniformity | NS p = 0.56 | ||
| Mean | NS p = 0.07 | gldm_GrayLevelVariance | NS p = 0.69 | ||
| Median | NS p = 0.06 | gldm_HighGrayLevelEmphasis | NS p = 0.10 | ||
| Skewness | * | gldm_LargeDependenceEmphasis | ** | ||
| Kurtosis | NS p = 0.36 | gldm_LargeDependenceHighGrayLevelEmphasis | ** | ||
| CV(%) | * | gldm_LargeDependenceLowGrayLevelEmphasis | NS p = 0.81 | ||
| MaxOnMeanRing | NS p = 0.08 | gldm_LowGrayLevelEmphasis | NS p = 0.59 | ||
| firstorder_10Percentile | NS p = 0.14 | gldm_SmallDependenceEmphasis | ** | ||
| firstorder_90Percentile | ** | gldm_SmallDependenceHighGrayLevelEmphasis | NS p = 1.00 | ||
| firstorder_Energy | NS p = 0.16 | gldm_SmallDependenceLowGrayLevelEmphasis | NS p = 0.55 | ||
| firstorder_Entropy | NS p = 0.97 | Gray Level Run Length Matrix | glrlm_GrayLevelNonUniformity | NS p = 0.87 | |
| firstorder_InterquartileRange | NS p = 0.10 | glrlm_GrayLevelNonUniformityNormalized | NS p = 0.83 | ||
| firstorder_Kurtosis | NS p = 0.36 | glrlm_GrayLevelVariance | NS p = 0.71 | ||
| firstorder_Maximum | NS p = 0.47 | glrlm_HighGrayLevelRunEmphasis | NS p = 0.10 | ||
| firstorder_MeanAbsoluteDeviation | NS p = 0.13 | glrlm_LongRunEmphasis | ** | ||
| firstorder_Mean | NS p = 0.07 | glrlm_LongRunHighGrayLevelEmphasis | * | ||
| firstorder_Median | NS p = 0.10 | glrlm_LongRunLowGrayLevelEmphasis | NS p = 0.64 | ||
| firstorder_Minimum | NS p = 0.73 | glrlm_LowGrayLevelRunEmphasis | NS p = 0.61 | ||
| firstorder_Range | NS p = 0.46 | glrlm_RunEntropy | NS p = 0.52 | ||
| firstorder_RobustMeanAbsoluteDeviation | NS p = 0.20 | glrlm_RunLengthNonUniformity | * | ||
| firstorder_RootMeanSquared | NS p = 0.05 | glrlm_RunLengthNonUniformityNormalized | ** | ||
| firstorder_Skewness | * | glrlm_RunPercentage | ** | ||
| firstorder_TotalEnergy | NS p = 0.15 | glrlm_RunVariance | ** | ||
| firstorder_Uniformity | NS p = 0.89 | glrlm_ShortRunEmphasis | ** | ||
| firstorder_Variance | NS p = 0.11 | glrlm_ShortRunHighGrayLevelEmphasis | NS p = 0.11 | ||
| Gray Level Co-occurrence Matrix | glcm_Autocorrelation | * | glrlm_ShortRunLowGrayLevelEmphasis | NS p = 0.63 | |
| glcm_ClusterProminence | NS p = 0.81 | Gray Level Size Zone Matrix | glszm_GrayLevelNonUniformity | ** | |
| glcm_ClusterShade | NS p = 0.81 | glszm_GrayLevelNonUniformityNormalized | ** | ||
| glcm_ClusterTendency | NS p = 0.86 | glszm_GrayLevelVariance | NS p = 0.90 | ||
| glcm_Contrast | ** | glszm_HighGrayLevelZoneEmphasis | NS p = 0.88 | ||
| glcm_Correlation | *** | glszm_LargeAreaEmphasis | NS p = 0.16 | ||
| glcm_DifferenceAverage | ** | glszm_LargeAreaHighGrayLevelEmphasis | NS p = 0.07 | ||
| glcm_DifferenceEntropy | *** | glszm_LargeAreaLowGrayLevelEmphasis | NS p = 0.10 | ||
| glcm_DifferenceVariance | ** | glszm_LowGrayLevelZoneEmphasis | NS p = 0.28 | ||
| glcm_Id | *** | glszm_SizeZoneNonUniformity | NS p = 0.82 | ||
| glcm_Idm | *** | glszm_SizeZoneNonUniformityNormalized | NS p = 0.05 | ||
| glcm_Idmn | *** | glszm_SmallAreaEmphasis | ** | ||
| glcm_Idn | *** | glszm_SmallAreaHighGrayLevelEmphasis | NS p = 0.58 | ||
| glcm_Imc1 | NS p = 0.11 | glszm_SmallAreaLowGrayLevelEmphasis | NS p = 0.35 | ||
| glcm_Imc2 | * | glszm_ZoneEntropy | ** | ||
| glcm_InverseVariance | *** | glszm_ZonePercentage | ** | ||
| glcm_JointAverage | * | glszm_ZoneVariance | NS p = 0.09 | ||
| glcm_JointEnergy | * | Neighbouring Gray Tone Difference Matrix | ngtdm_Busyness | *** | |
| glcm_JointEntropy | * | ngtdm_Coarseness | *** | ||
| glcm_MCC | *** | ngtdm_Complexity | * | ||
| glcm_MaximumProbability | * | ngtdm_Contrast | ** | ||
| glcm_SumAverage | * | ngtdm_Strength | * | ||
| glcm_SumEntropy | NS p = 0.85 | IQ wavelets | IQwavelet_global | *** | |
| glcm_SumSquares | NS p = 0.33 | IQwavelet_local | *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moummad, I.; Jaudet, C.; Lechervy, A.; Valable, S.; Raboutet, C.; Soilihi, Z.; Thariat, J.; Falzone, N.; Lacroix, J.; Batalla, A.; et al. The Impact of Resampling and Denoising Deep Learning Algorithms on Radiomics in Brain Metastases MRI. Cancers 2022, 14, 36. https://doi.org/10.3390/cancers14010036
Moummad I, Jaudet C, Lechervy A, Valable S, Raboutet C, Soilihi Z, Thariat J, Falzone N, Lacroix J, Batalla A, et al. The Impact of Resampling and Denoising Deep Learning Algorithms on Radiomics in Brain Metastases MRI. Cancers. 2022; 14(1):36. https://doi.org/10.3390/cancers14010036
Chicago/Turabian StyleMoummad, Ilyass, Cyril Jaudet, Alexis Lechervy, Samuel Valable, Charlotte Raboutet, Zamila Soilihi, Juliette Thariat, Nadia Falzone, Joëlle Lacroix, Alain Batalla, and et al. 2022. "The Impact of Resampling and Denoising Deep Learning Algorithms on Radiomics in Brain Metastases MRI" Cancers 14, no. 1: 36. https://doi.org/10.3390/cancers14010036
APA StyleMoummad, I., Jaudet, C., Lechervy, A., Valable, S., Raboutet, C., Soilihi, Z., Thariat, J., Falzone, N., Lacroix, J., Batalla, A., & Corroyer-Dulmont, A. (2022). The Impact of Resampling and Denoising Deep Learning Algorithms on Radiomics in Brain Metastases MRI. Cancers, 14(1), 36. https://doi.org/10.3390/cancers14010036