
Clinical Application of Pectoralis Nerve Block II for Flap Dissection-Related Pain Control after Robot-Assisted Transaxillary Thyroidectomy: A Preliminary Retrospective Cohort Study

 , , , , , , and
, , , , , , and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Considerations
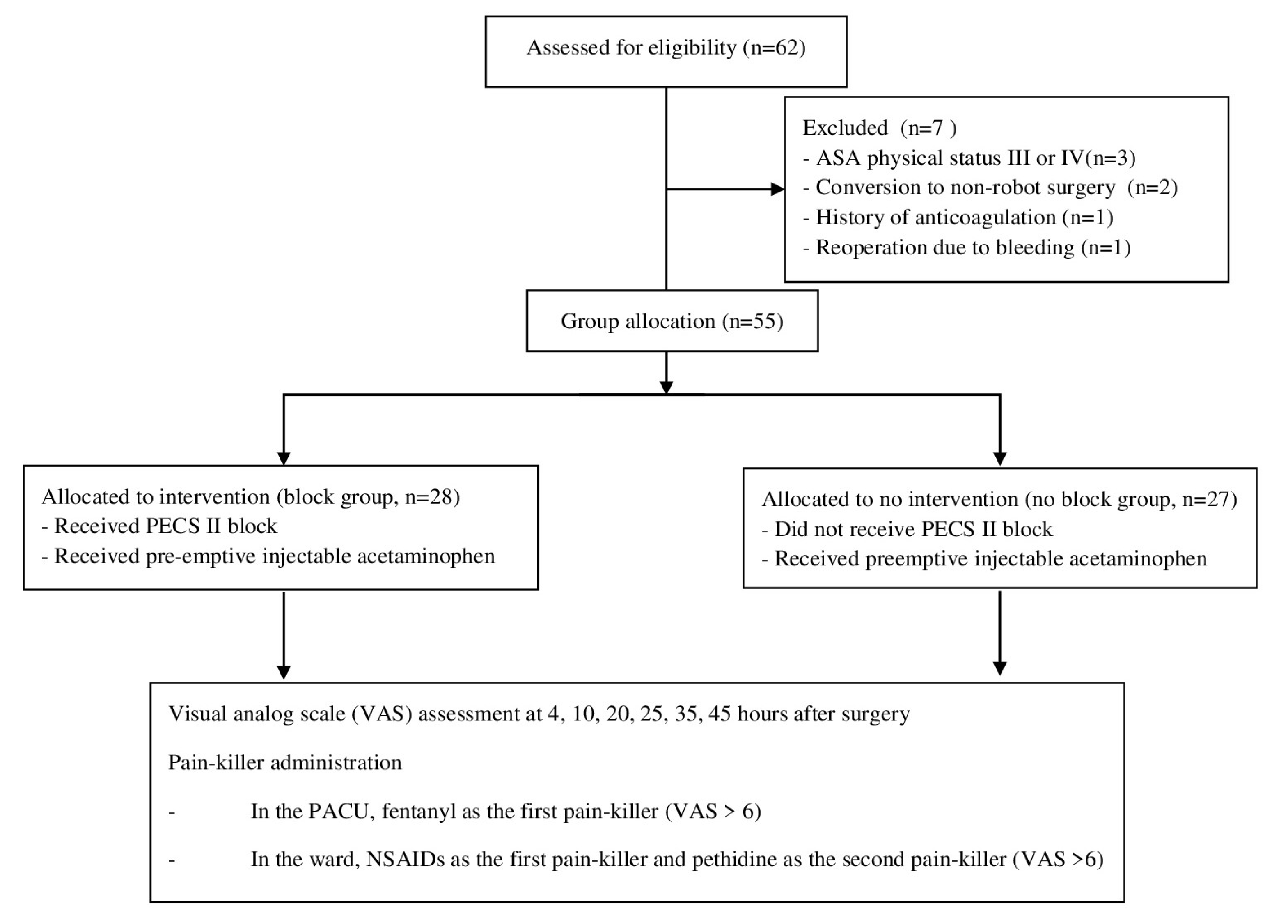
2.2. Study Population
2.3. RATT Proccedure
2.4. General Anesthesia
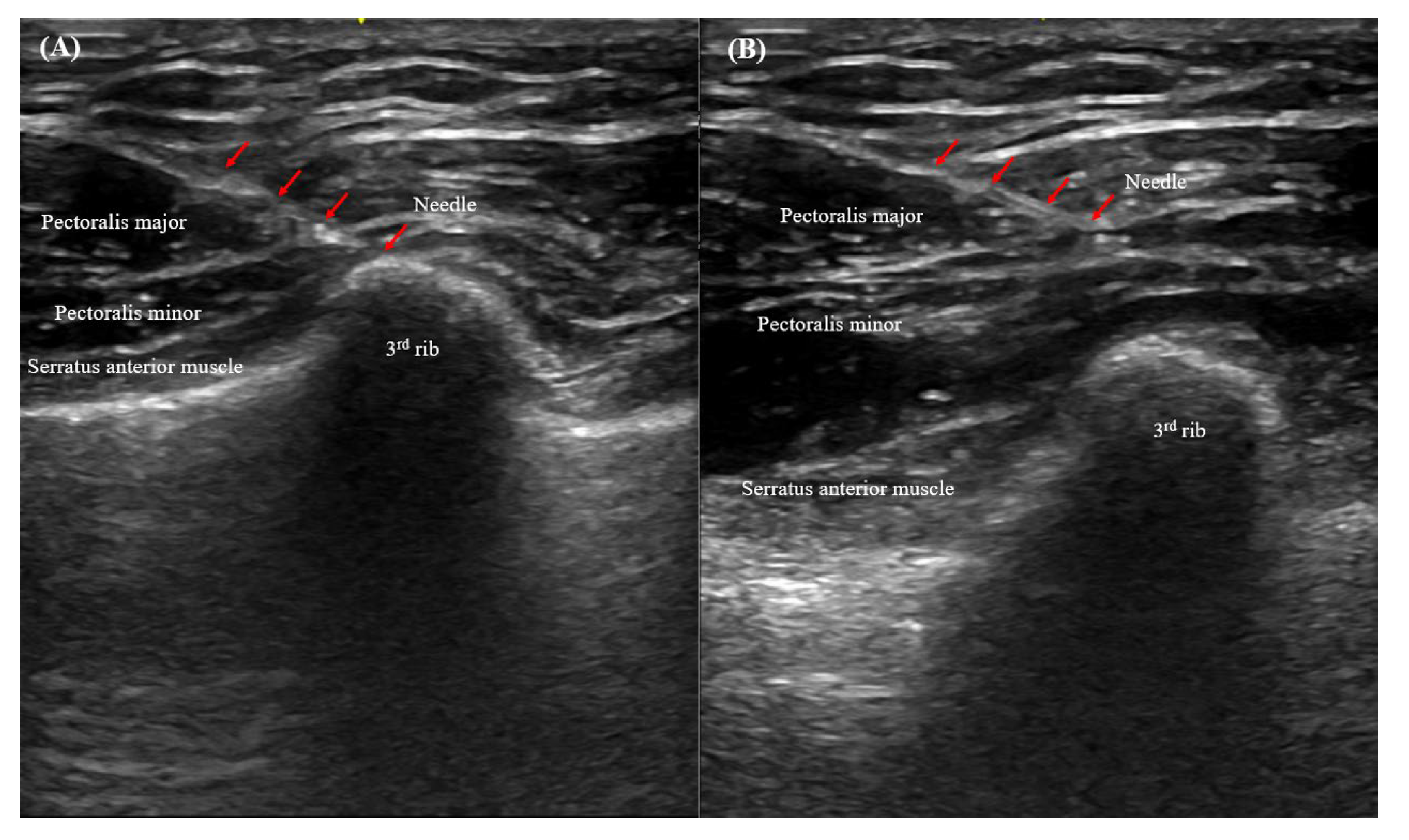
2.5. Ultrasonography-Guided PECS II
2.6. Pain Outcomes
2.7. Clinical Variables
2.8. Statistical Analysis
3. Results
3.1. Baseline Clinicopathological Characteristics
3.2. Postoperative Pain in the Block and No-Block Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lin, P.; Liang, F.; Cai, Q.; Han, P.; Chen, R.; Xiao, Z.; Wang, J.; Huang, X. Comparative study of gasless endoscopic selective lateral neck dissection via the anterior chest approach versus conventional open surgery for papillary thyroid carcinoma. Surg. Endosc. 2021, 35, 693–701. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, Y.; Takami, H.; Sasaki, Y.; Takayama, J.; Niimi, M.; Kan, S. Clinical benefits in endoscopic thyroidectomy by the axillary approach. J. Am. Coll. Surg. 2003, 196, 189–195. [Google Scholar] [CrossRef]
- Ikeda, Y.; Takami, H.; Sasaki, Y.; Takayama, J.; Niimi, M.; Kan, S. Comparative study of thyroidectomies. Endoscopic surgery versus conventional open surgery. Surg. Endosc. 2002, 16, 1741–1745. [Google Scholar] [CrossRef] [PubMed]
- Miyano, G.; Lobe, T.E.; Wright, S.K. Bilateral transaxillary endoscopic total thyroidectomy. J. Pediatric Surg. 2008, 43, 299–303. [Google Scholar] [CrossRef]
- Duncan, T.D.; Rashid, Q.; Speights, F.; Ejeh, I. Endoscopic transaxillary approach to the thyroid gland: Our early experience. Surg. Endosc. 2007, 21, 2166–2171. [Google Scholar] [CrossRef]
- Kim, K.; Kang, S.W.; Kim, J.K.; Lee, C.R.; Lee, J.; Jeong, J.J.; Nam, K.H.; Chung, W.Y. Robotic Transaxillary Hemithyroidectomy Using the da Vinci SP Robotic System: Initial Experience With 10 Consecutive Cases. Surg. Innov. 2020, 27, 256–264. [Google Scholar] [CrossRef]
- Warfield, D.J., Jr.; Barre, S.; Adhikary, S.D. Current understanding of the fascial plane blocks for analgesia of the chest wall: Techniques and indications update for 2020. Curr. Opin. Anaesthesiol. 2020, 33, 692–697. [Google Scholar] [CrossRef]
- Meißner, M.; Austenfeld, E.; Kranke, P.; Zahn, P.K.; Pogatzki-Zahn, E.M.; Meyer-Frießem, C.H.; Weibel, S.; Schnabel, A. Pectoral nerve blocks for breast surgery: A meta-analysis. Eur. J. Anaesthesiol. 2021, 38, 383–393. [Google Scholar] [CrossRef]
- Mancel, L.; Van Loon, K.; Lopez, A.M. Role of regional anesthesia in Enhanced Recovery After Surgery (ERAS) protocols. Curr. Opin. Anaesthesiol. 2021, 34, 616–625. [Google Scholar] [CrossRef]
- Marciniak, D.; Kelava, M.; Hargrave, J. Fascial plane blocks in thoracic surgery: A new era or plain painful? Curr. Opin. Anaesthesiol. 2020, 33, 1–9. [Google Scholar] [CrossRef]
- Hussain, N.; Brull, R.; McCartney, C.J.L.; Wong, P.; Kumar, N.; Essandoh, M.; Sawyer, T.; Sullivan, T.; Abdallah, F.W. Pectoralis-II Myofascial Block and Analgesia in Breast Cancer Surgery: A Systematic Review and Meta-analysis. Anesthesiology 2019, 131, 630–648. [Google Scholar] [CrossRef] [PubMed]
- Blanco, R.; Fajardo, M.; Parras Maldonado, T. Ultrasound description of Pecs II (modified Pecs I): A novel approach to breast surgery. Rev. Esp. Anestesiol. Reanim. 2012, 59, 470–475. [Google Scholar] [CrossRef]
- Martsiniv, V.V.; Loskutov, O.A.; Strokan, A.M.; Bondar, M.V. Efficacy of pectoral nerve block type II versus thoracic paravertebral block for analgesia in breast cancer surgery. Wiad. Lek. 2020, 73, 1470–1475. [Google Scholar] [CrossRef] [PubMed]
- Moon, E.J.; Kim, S.B.; Chung, J.Y.; Song, J.Y.; Yi, J.W. Pectoral nerve block (Pecs block) with sedation for breast conserving surgery without general anesthesia. Ann. Surg. Treat. Res. 2017, 93, 166–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helander, E.M.; Webb, M.P.; Kendrick, J.; Montet, T.; Kaye, A.J.; Cornett, E.M.; Kaye, A.D. PECS, serratus plane, erector spinae, and paravertebral blocks: A comprehensive review. Best practice & research. Clin. Anaesthesiol. 2019, 33, 573–581. [Google Scholar] [CrossRef]
- Lee, S.; Ryu, H.R.; Park, J.H.; Kim, K.H.; Kang, S.W.; Jeong, J.J.; Nam, K.H.; Chung, W.Y.; Park, C.S. Excellence in robotic thyroid surgery: A comparative study of robot-assisted versus conventional endoscopic thyroidectomy in papillary thyroid microcarcinoma patients. Ann. Surg. 2011, 253, 1060–1066. [Google Scholar] [CrossRef]
- Kim, H.Y.; Chai, Y.J.; Dionigi, G.; Anuwong, A.; Richmon, J.D. Transoral robotic thyroidectomy: Lessons learned from an initial consecutive series of 24 patients. Surg. Endosc. 2018, 32, 688–694. [Google Scholar] [CrossRef]
- Singer, M.C.; Terris, D.J. Robotic facelift thyroidectomy. Otolaryngol. Clin. North Am. 2014, 47, 425–431. [Google Scholar] [CrossRef]
- Lee, K.E.; Rao, J.; Youn, Y.K. Endoscopic thyroidectomy with the da Vinci robot system using the bilateral axillary breast approach (BABA) technique: Our initial experience. Surg. Laparosc. Endosc. Percutaneous Technol. 2009, 19, e71–e75. [Google Scholar] [CrossRef]
- Kim, M.J.; Nam, K.H.; Lee, S.G.; Choi, J.B.; Kim, T.H.; Lee, C.R.; Lee, J.; Kang, S.W.; Jeong, J.J.; Chung, W.Y. Yonsei Experience of 5000 Gasless Transaxillary Robotic Thyroidectomies. World J. Surg. 2018, 42, 393–401. [Google Scholar] [CrossRef]
- Hong, J.Y.; Kim, W.O.; Chung, W.Y.; Yun, J.S.; Kil, H.K. Paracetamol reduces postoperative pain and rescue analgesic demand after robot-assisted endoscopic thyroidectomy by the transaxillary approach. World J. Surg. 2010, 34, 521–526. [Google Scholar] [CrossRef] [PubMed]
- Grundmann, U.; Wörnle, C.; Biedler, A.; Kreuer, S.; Wrobel, M.; Wilhelm, W. The efficacy of the non-opioid analgesics parecoxib, paracetamol and metamizol for postoperative pain relief after lumbar microdiscectomy. Anesth. Analg. 2006, 103, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Hein, A.; Jakobsson, J.; Ryberg, G. Paracetamol 1 g given rectally at the end of minor gynaecological surgery is not efficacious in reducing postoperative pain. Acta Anaesthesiol. Scand. 1999, 43, 248–251. [Google Scholar] [CrossRef] [PubMed]
- Shim, J.W.; Ko, J.; Bae, J.H.; Park, J.; Lee, H.M.; Kim, Y.S.; Moon, Y.E.; Hong, S.H.; Chae, M.S. Pre-emptive multimodal analgesic bundle with transversus abdominis plane block enhances early recovery after laparoscopic cholecystectomy. Asian J. Surg. 2022, 45, 250–256. [Google Scholar] [CrossRef]
- Shim, J.W.; Jung, S.; Moon, H.W.; Lee, J.Y.; Park, J.; Lee, H.M.; Kim, Y.S.; Hong, S.H.; Chae, M.S. Rectus sheath block for acute pain management after robot-assisted laparoscopic prostatectomy. Asian J. Surg. 2021. [Google Scholar] [CrossRef]
- Lin, C.; Darling, C.; Tsui, B.C.H. Practical Regional Anesthesia Guide for Elderly Patients. Drugs Aging 2019, 36, 213–234. [Google Scholar] [CrossRef]
- Kelava, M.; Alfirevic, A.; Bustamante, S.; Hargrave, J.; Marciniak, D. Regional Anesthesia in Cardiac Surgery: An Overview of Fascial Plane Chest Wall Blocks. Anesth. Analg. 2020, 131, 127–135. [Google Scholar] [CrossRef]
- Jack, J.M.; McLellan, E.; Versyck, B.; Englesakis, M.F.; Chin, K.J. The role of serratus anterior plane and pectoral nerves blocks in cardiac surgery, thoracic surgery and trauma: A qualitative systematic review. Anaesthesia 2020, 75, 1372–1385. [Google Scholar] [CrossRef]
- Macfarlane, A.J.R.; Gitman, M.; Bornstein, K.J.; El-Boghdadly, K.; Weinberg, G. Updates in our understanding of local anaesthetic systemic toxicity: A narrative review. Anaesthesia 2021, 76, 27–39. [Google Scholar] [CrossRef]
- Vanderpump, M.P. The epidemiology of thyroid disease. Br. Med. Bull. 2011, 99, 39–51. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total 55 Patients | |
|---|---|
| Age (years) | 41.5 ± 12.4 (range, 18–69) |
| Gender | |
| Male | 3 (5.5%) |
| Female | 52 (95.5%) |
| Extent of operation | |
| Lobectomy | 48 (87.3%) |
| Total thyroidectomy | 7 (12.7%) |
| Pathology | |
| PTC | 45 (81.8%) |
| HCC | 1 (1.8%) |
| NIFTP | 3 (5.5%) |
| Follicular adenoma | 4 (7.3%) |
| Graves’ disease | 1 (1.8%) |
| Parathyroid adenoma | 1 (1.8%) |
| Tumor size (cm) | 1.1 ± 1.0 (range, 0.3–5.3) |
| Multifocality | 19/49 (38.8%) |
| ETE | |
| No | 19/49 (38.8%) |
| Minimal | 30/49 (61.2%) |
| Thyroiditis | 25 (45.5%) |
| Harvested LNs | 6.2 ± 3.5 |
| Positive LNs | 1.0 ± 1.6 |
| T stage | |
| T1/T2/T3a | 44 (95.7%)/1 (2.2%)/1 (2.2%) |
| N stage | |
| N0/N1a | 28 (60.9%)/18 (39.1%) |
| TNM stage | |
| Stage I/II | 44 (95.7%)/2 (4.3%) |
| Block (n = 28) | No Block (n = 27) | p-Value | |
|---|---|---|---|
| Age (years) | 43.8 ± 11.7 (range, 24–64) | 39.0 ± 12.8 (range, 18–69) | 0.157 |
| Female | 28 (100%) | 24 (88.9%) | 0.111 |
| Extent of operation | 0.206 | ||
| Lobectomy | 26 (92.9%) | 22 (81.5%) | |
| Total thyroidectomy | 2 (7.1%) | 22 (18.5%) | |
| Pathology | 0.648 | ||
| PTC | 23 (82.1%) | 22 (81.5%) | |
| HCC | 0 | 1 (3.7%) | |
| NIFTP | 2 (7.1%) | 1 (3.7%) | |
| Follicular adenoma | 2 (7.1%) | 2 (7.4%) | |
| Graves’ disease | 1 (3.6%) | 0 | |
| Parathyroid adenoma | 0 | 1 (3.7%) | |
| Tumor size (cm) | 0.9 ± 0.6 | 1.3 ± 1.2 | 0.160 |
| Multiplicity | 11/25 (44.0%) | 8/24 (33.3%) | 0.444 |
| Minimal ETE | 16/25 (64.0%) | 14/24 (58.3%) | 0.684 |
| Thyroiditis | 14 (50.0%) | 11 (40.7%) | 0.491 |
| Harvested LNs | 6.4 ± 3.1 | 5.9 ± 4.0 | 0.651 |
| Positive LNs | 1.0 ± 1.8 | 1.0 ± 1.6 | 1.000 |
| T stage | 0.352 | ||
| T1 | 23 (100%) | 21 (91.3%) | |
| T2 | 0 | 1 (3.7%) | |
| T3a | 0 | 1 (3.7%) | |
| N stage | 0.546 | ||
| N0 | 15 (65.2%) | 13 (56.5%) | |
| N1a | 8 (34.80%) | 10 (43.5%) | |
| TNM stage | 1.000 | ||
| Stage I | 22 (95.7%) | 22 (95.7%) | |
| Stage II | 1 (4.3%) | 1 (4.3%) |
| Block (n = 28) | No Block (n = 27) | p-Value | |
|---|---|---|---|
| VAS + 4 h | 4.2 ± 2.0 | 4.4 ± 2.1 | 0.628 |
| VAS + 10 h | 3.3 ± 1.7 †† | 4.3 ± 1.5 | 0.017 |
| VAS + 20 h | 3.4 ± 1.2 | 4.1 ± 1.4 | 0.053 |
| VAS + 25 h | 2.6 ± 1.3 †† | 3.5 ± 1.7 †† | 0.034 |
| VAS + 35 h | 2.4 ± 1.4 ††† | 2.7 ± 1.2 ††† | 0.350 |
| VAS + 45 h | 2.2 ± 1.5 †† | 2.5 ± 1.0 ††† | 0.511 |
| No. of painkiller used | |||
| In the PACU | 0.7 ± 0.6 | 1.7 ± 0.5 | <0.001 |
| In the ward | 1.0 ± 0.9 | 1.6 ± 1.6 | 0.062 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chae, M.S.; Park, Y.; Shim, J.-W.; Hong, S.H.; Park, J.; Kang, I.K.; Bae, J.S.; Kim, J.S.; Kim, K. Clinical Application of Pectoralis Nerve Block II for Flap Dissection-Related Pain Control after Robot-Assisted Transaxillary Thyroidectomy: A Preliminary Retrospective Cohort Study. Cancers 2022, 14, 4097. https://doi.org/10.3390/cancers14174097
Chae MS, Park Y, Shim J-W, Hong SH, Park J, Kang IK, Bae JS, Kim JS, Kim K. Clinical Application of Pectoralis Nerve Block II for Flap Dissection-Related Pain Control after Robot-Assisted Transaxillary Thyroidectomy: A Preliminary Retrospective Cohort Study. Cancers. 2022; 14(17):4097. https://doi.org/10.3390/cancers14174097
Chicago/Turabian StyleChae, Min Suk, Youngkyung Park, Jung-Woo Shim, Sang Hyun Hong, Joonseon Park, Il Ku Kang, Ja Seong Bae, Jeong Soo Kim, and Kwangsoon Kim. 2022. "Clinical Application of Pectoralis Nerve Block II for Flap Dissection-Related Pain Control after Robot-Assisted Transaxillary Thyroidectomy: A Preliminary Retrospective Cohort Study" Cancers 14, no. 17: 4097. https://doi.org/10.3390/cancers14174097
APA StyleChae, M. S., Park, Y., Shim, J. -W., Hong, S. H., Park, J., Kang, I. K., Bae, J. S., Kim, J. S., & Kim, K. (2022). Clinical Application of Pectoralis Nerve Block II for Flap Dissection-Related Pain Control after Robot-Assisted Transaxillary Thyroidectomy: A Preliminary Retrospective Cohort Study. Cancers, 14(17), 4097. https://doi.org/10.3390/cancers14174097