
Probe-Based Confocal Laser Endomicroscopy versus White-Light Endoscopy with Narrow-Band Imaging for Predicting and Collecting Residual Cancer Tissue in Patients with Gastric Cancer Receiving Chemotherapy

 ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
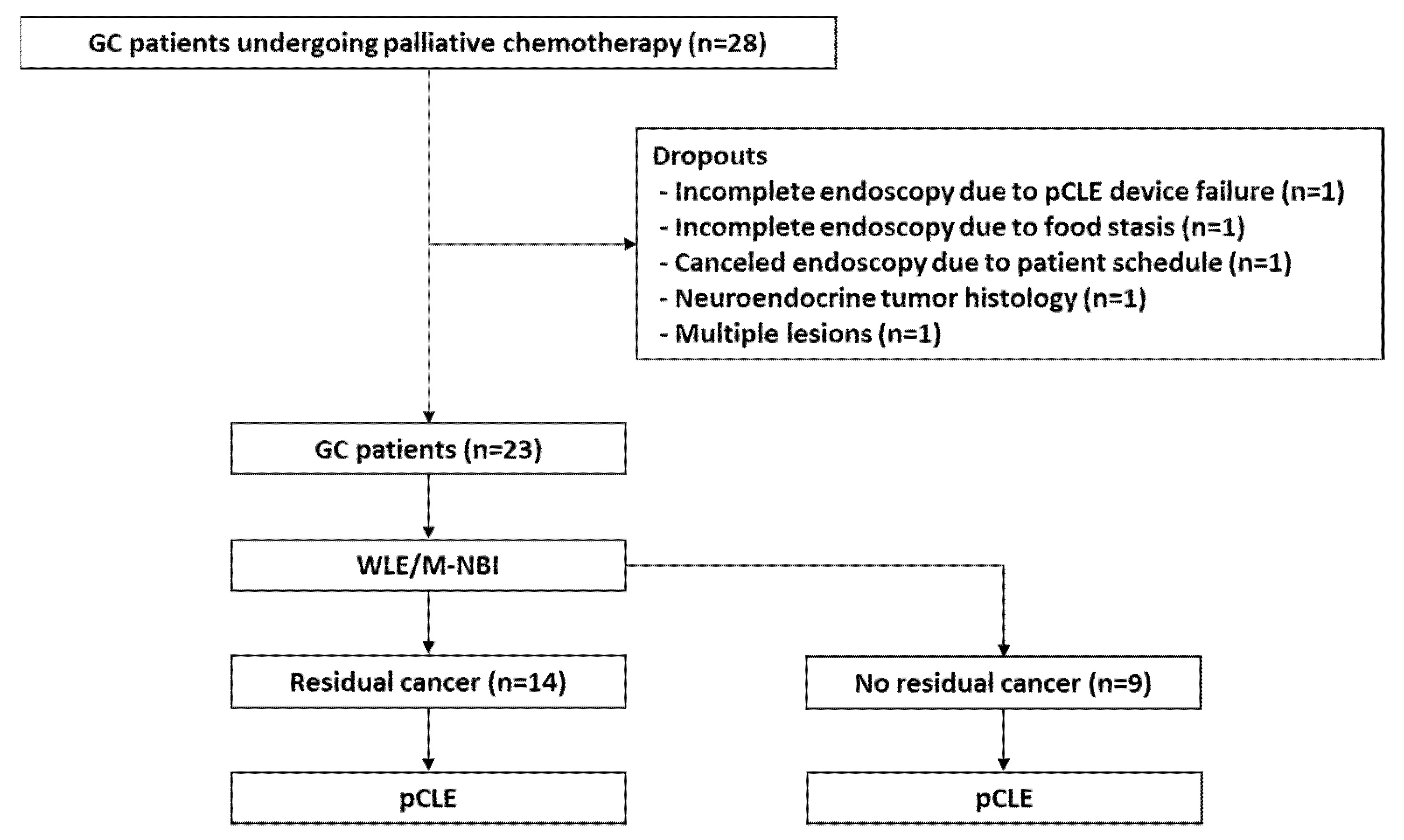
2.1. Patients
2.2. Study Protocol and Patient Grouping
2.3. Histopathological Assessment
2.4. Sample Size Calculation
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
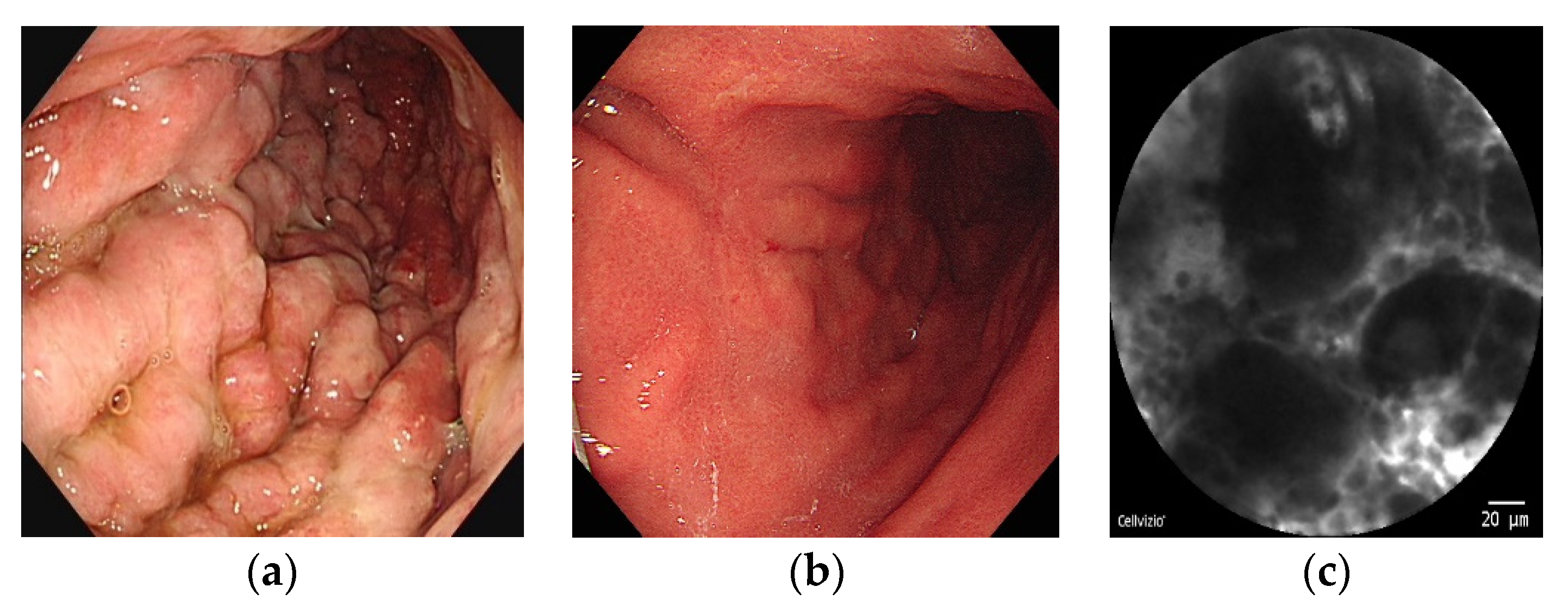
3.2. Accuracy of WLE/M-NBI versus pCLE
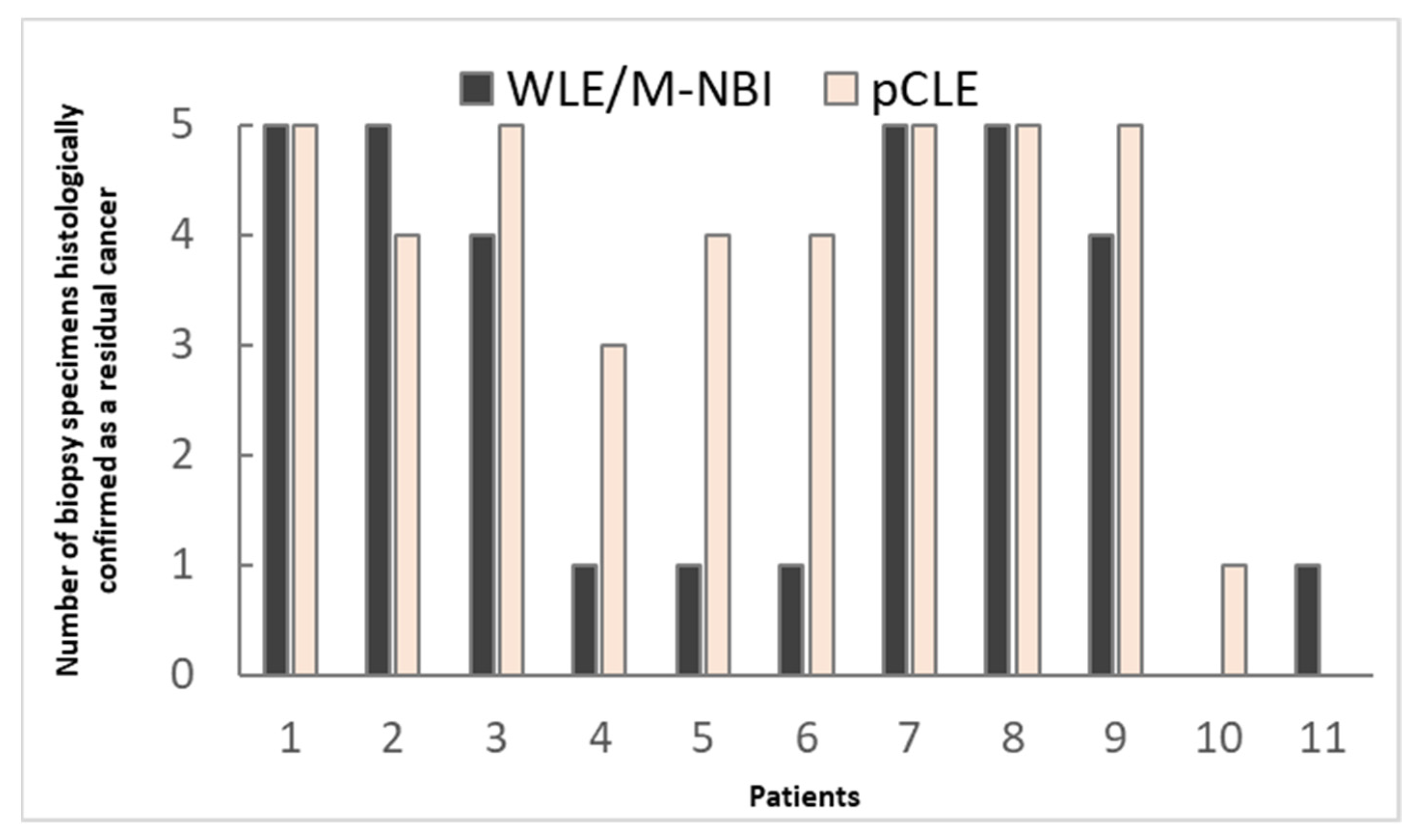
3.3. Comparison of WLE/M-NBI and pCLE by Number of Biopsy Specimens Histologically Confirmed as Containing GC
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Salati, M.; Orsi, G.; Smyth, E.; Beretta, G.; De Vita, F.; Di Bartolomeo, M.; Fanotto, V.; Lonardi, S.; Morano, F.; Pietrantonio, F. Gastric cancer: Translating novels concepts into clinical practice. Cancer Treat. Rev. 2019, 79, 101889. [Google Scholar] [CrossRef] [PubMed]
- Cristescu, R.; Lee, J.; Nebozhyn, M.; Kim, K.-M.; Ting, J.C.; Wong, S.S.; Liu, J.; Yue, Y.G.; Wang, J.; Yu, K.; et al. Molecular analysis of gastric cancer identifies subtypes associated with distinct clinical outcomes. Nat. Med. 2015, 21, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Spirina, L.V.; Avgustinovich, A.V.; Afanas’ev, S.G.; Cheremisina, O.V.; Volkov, M.Y.; Choynzonov, E.L.; Gorbunov, A.K.; Usynin, E.A. Molecular Mechanism of Resistance to Chemotherapy in Gastric Cancers, the Role of Autophagy. Curr. Drug Targets 2020, 21, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Park, C.H.; Kim, H.; Jo, J.H.; Hahn, K.Y.; Yoon, J.H.; Kim, S.Y.; Lee, Y.C.; Noh, S.H.; Chung, H.C.; Lee, S.K. Role of probe-based confocal laser endomicroscopy-targeted biopsy in the molecular and histopathological study of gastric cancer. J. Gastroenterol. Hepatol. 2019, 34, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Kato, M.; Kaise, M.; Yonezawa, J.; Toyoizumi, H.; Yoshimura, N.; Yoshida, Y.; Kawamura, M.; Tajiri, H. Magnifying endoscopy with narrow-band imaging achieves superior accuracy in the differential diagnosis of superficial gastric lesions identified with white-light endoscopy: A prospective study. Gastrointest. Endosc. 2010, 72, 523–529. [Google Scholar] [CrossRef]
- Buxbaum, J.L.; Hormozdi, D.; Dinis-Ribeiro, M.; Lane, C.; Dias-Silva, D.; Sahakian, A.; Jayaram, P.; Pimentel-Nunes, P.; Shue, D.; Pepper, M.; et al. Narrow-band imaging versus white light versus mapping biopsy for gastric intestinal metaplasia: A prospective blinded trial. Gastrointest. Endosc. 2017, 86, 857–865. [Google Scholar] [CrossRef] [PubMed]
- Jeon, S.R.; Cho, W.Y.; Jin, S.Y.; Cheon, Y.K.; Choi, S.R.; Cho, J.Y. Optical biopsies by confocal endomicroscopy prevent additive endoscopic biopsies before endoscopic submucosal dissection in gastric epithelial neoplasias: A prospective, comparative study. Gastrointest. Endosc. 2011, 74, 772–780. [Google Scholar] [CrossRef]
- Capuano, A.; Andreuzzi, E.; Pivetta, E.; Doliana, R.; Favero, A.; Canzonieri, V.; Maiero, S.; Fornasarig, M.; Magris, R.; Cannizzaro, R.; et al. The Probe Based Confocal Laser Endomicroscopy (pCLE) in Locally Advanced Gastric Cancer: A Powerful Technique for Real–Time Analysis of Vasculature. Front. Oncol. 2019, 9, 513. [Google Scholar] [CrossRef]
- Wallace, M.B.; Fockens, P. Probe-Based Confocal Laser Endomicroscopy. Gastroenterology 2009, 136, 1509–1513. [Google Scholar] [CrossRef]
- Shahid, M.W.; Buchner, A.M.; Heckman, M.G.; Krishna, M.; Raimondo, M.; Woodward, T.; Wallace, M.B. Diagnostic Accuracy of Probe-Based Confocal Laser Endomicroscopy and Narrow Band Imaging for Small Colorectal Polyps: A Feasibility Study. Off. J. Am. Coll. Gastroenterol. ACG 2012, 107, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Shah, T.; Lippman, R.; Kohli, D.; Mutha, P.; Solomon, S.; Zfass, A. Accuracy of probe-based confocal laser endomicroscopy (pCLE) compared to random biopsies during endoscopic surveillance of Barrett’s esophagus. Endosc. Int. Open 2018, 6, E414–E420. [Google Scholar] [CrossRef] [PubMed]
- De Palma, G.D. Confocal laser endomicroscopy in the “in vivo” histological diagnosis of the gastrointestinal tract. World J. Gastroenterol. 2009, 15, 5770–5775. [Google Scholar] [CrossRef]
- Zhang, Q.-W.; Zhou, Y.; Zhang, J.-J.; Li, H.-Y.; Song, J.-Y.; Ge, Z.-Z.; Li, X.-B. Role of targeted biopsy under magnifying endoscopy with narrow band imaging may be not necessary: A prospective diagnostic accuracy study. Eur. J. Gastroenterol. Hepatol. 2017, 29, 414–422. [Google Scholar] [CrossRef]
- Choi, Y.; Choi, H.S.; Jeon, W.K.; Kim, B.I.; Park, D.I.; Cho, Y.K.; Kim, H.J.; Park, J.H.; Sohn, C.I. Optimal number of endoscopic biopsies in diagnosis of advanced gastric and colorectal cancer. J. Korean Med. Sci. 2012, 27, 36–39. [Google Scholar] [CrossRef] [PubMed]
- Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2018 (5th edition). Gastric Cancer 2021, 24, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.K. Usefulness of Probe-Based Confocal Laser Endomicroscopy for Esophageal Squamous Cell Neoplasm. Clin. Endosc. 2019, 52, 91–92. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.K. Usefulness and Future Prospects of Confocal Laser Endomicroscopy for Gastric Premalignant and Malignant Lesions. Clin. Endosc. 2015, 48, 511–515. [Google Scholar] [CrossRef]
- Nagahama, T.; Yao, K.; Uedo, N.; Doyama, H.; Ueo, T.; Uchita, K.; Ishikawa, H.; Kanesaka, T.; Takeda, Y.; Wada, K.; et al. Delineation of the extent of early gastric cancer by magnifying narrow-band imaging and chromoendoscopy: A multicenter randomized controlled trial. Endoscopy 2018, 50, 566–576. [Google Scholar] [CrossRef]
- Sarkaria, I.S.; Rizk, N.P.; Bains, M.S.; Tang, L.H.; Ilson, D.H.; Minsky, B.I.; Rusch, V.W. Post-treatment endoscopic biopsy is a poor-predictor of pathologic response in patients undergoing chemoradiation therapy for esophageal cancer. Ann. Surg. 2009, 249, 764–767. [Google Scholar] [CrossRef]
- Kim, J.H.; Choi, E.K.; Kim, S.B.; Park, S.I.; Kim, D.K.; Song, H.Y.; Jung, H.Y.; Min, Y.I. Preoperative hyperfractionated radiotherapy with concurrent chemotherapy in resectable esophageal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2001, 50, 1–12. [Google Scholar] [CrossRef]
- Bates, B.A.; Detterbeck, F.C.; Bernard, S.A.; Qaqish, B.F.; Tepper, J.E. Concurrent radiation therapy and chemotherapy followed by esophagectomy for localized esophageal carcinoma. J. Clin. Oncol. 1996, 14, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Brown, W.A.; Thomas, J.; Gotley, D.; Burmeister, B.H.; Lim, K.H.; Martin, I.; Walpole, E.T.; Thomson, D.B.; Harvey, J.A.; Smithers, B.M. Use of oesophagogastroscopy to assess the response of oesophageal carcinoma to neoadjuvant therapy. Br. J. Surg. 2004, 91, 199–204. [Google Scholar] [CrossRef]
- Bok, G.H.; Jeon, S.R.; Cho, J.Y.; Cho, J.-H.; Lee, W.C.; Jin, S.Y.; Choi, I.H.; Kim, H.G.; Lee, T.H.; Park, E.J. The accuracy of probe-based confocal endomicroscopy versus conventional endoscopic biopsies for the diagnosis of superficial gastric neoplasia (with videos). Gastrointest. Endosc. 2013, 77, 899–908. [Google Scholar] [CrossRef] [PubMed]
- Zuo, X.L.; Li, Z.; Li, C.Q.; Zheng, Y.Y.; Xu, L.D.; Chen, J.; Lin, R.; Song, J.; Yu, C.H.; Yue, M.; et al. Probe-based endomicroscopy for in vivo detection of gastric intestinal metaplasia and neoplasia: A multicenter randomized controlled trial. Endoscopy 2017, 49, 1033–1042. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.P.; Yang, S.; Chen, W.H.; Hu, T.T.; Lin, J. The diagnostic value of confocal laser endomicroscopy for gastric cancer and precancerous lesions among Asian population: A system review and meta-analysis. Scand. J. Gastroenterol. 2017, 52, 382–388. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Age (years), mean ± SD | 57.2 ± 10.1 |
| Sex, n (%) | |
| Male | 15 (65.2) |
| Female | 8 (34.8) |
| Reason for endoscopic biopsy, n (%) | |
| Response evaluation during chemotherapy | 21 (91.3) |
| Registration for clinical study | 2 (8.7) |
| TNM stage, n (%) | |
| I | 0 (0) |
| II | 0 (0) |
| III | 0 (0) |
| IV | 23 (100) |
| Response after chemotherapy, n (%) | |
| Complete response | 0 (0) |
| Partial response | 4 (17.4) |
| Stable disease | 15 (65.2) |
| Progressive disease | 4 (17.4) |
| WLE/M-NBI | pCLE | |||
|---|---|---|---|---|
| % | 95% CI | % | 95% CI | |
| Sensitivity | 47 | 0.35–0.59 | 67 | 0.55–0.78 |
| Specificity | 100 | 0.92–1.0 | 100 | 0.92–1.0 |
| PPV | 100 | 0.89–1.0 | 100 | 0.92–1.0 |
| NPV | 55 | 0.43–0.66 | 66 | 0.54–0.77 |
| Accuracy | 68 | 80 | ||
| Predictive Ability of WLE/M-NBI | Predictive Ability of pCLE | |
|---|---|---|
| Same results | 16/17(94.1%) | 16/17 (94.1%) |
| Contradictory results | 2/6 (33.3%) | 4/6 (66.6%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.; Kim, H.; Jung, M.; Rha, S.Y.; Chung, H.C.; Lee, S.K. Probe-Based Confocal Laser Endomicroscopy versus White-Light Endoscopy with Narrow-Band Imaging for Predicting and Collecting Residual Cancer Tissue in Patients with Gastric Cancer Receiving Chemotherapy. Cancers 2022, 14, 4319. https://doi.org/10.3390/cancers14174319
Kim Y, Kim H, Jung M, Rha SY, Chung HC, Lee SK. Probe-Based Confocal Laser Endomicroscopy versus White-Light Endoscopy with Narrow-Band Imaging for Predicting and Collecting Residual Cancer Tissue in Patients with Gastric Cancer Receiving Chemotherapy. Cancers. 2022; 14(17):4319. https://doi.org/10.3390/cancers14174319
Chicago/Turabian StyleKim, Yuna, Hyunki Kim, Minkyu Jung, Sun Young Rha, Hyun Cheol Chung, and Sang Kil Lee. 2022. "Probe-Based Confocal Laser Endomicroscopy versus White-Light Endoscopy with Narrow-Band Imaging for Predicting and Collecting Residual Cancer Tissue in Patients with Gastric Cancer Receiving Chemotherapy" Cancers 14, no. 17: 4319. https://doi.org/10.3390/cancers14174319
APA StyleKim, Y., Kim, H., Jung, M., Rha, S. Y., Chung, H. C., & Lee, S. K. (2022). Probe-Based Confocal Laser Endomicroscopy versus White-Light Endoscopy with Narrow-Band Imaging for Predicting and Collecting Residual Cancer Tissue in Patients with Gastric Cancer Receiving Chemotherapy. Cancers, 14(17), 4319. https://doi.org/10.3390/cancers14174319