


Impact of Preoperative Chemotherapy Features on Patient Outcomes after Hepatectomy for Initially Unresectable Colorectal Cancer Liver Metastases: A LiverMetSurvey Analysis

 , ,
, ,  , ,
, ,  , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
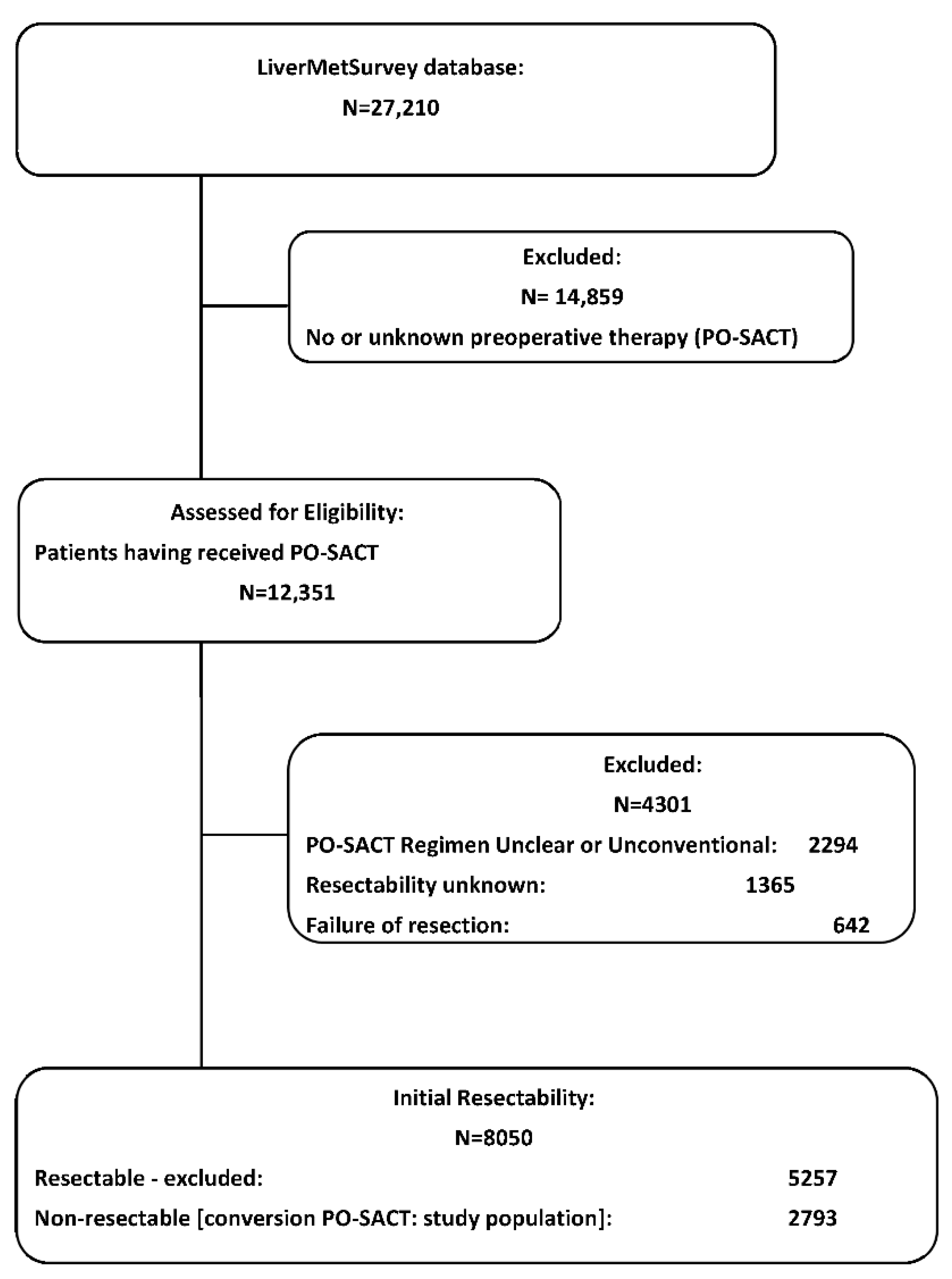
2.1. LiverMetSurvey and Patient Selection
2.2. Preoperative Management and Hepatic Resection
2.3. Postoperative Chemotherapy
2.4. Follow-Up
2.5. Statistical Analyses
3. Results
3.1. Study Population
3.2. Preoperative Chemotherapy Features and Outcomes
3.3. Surgical Complications
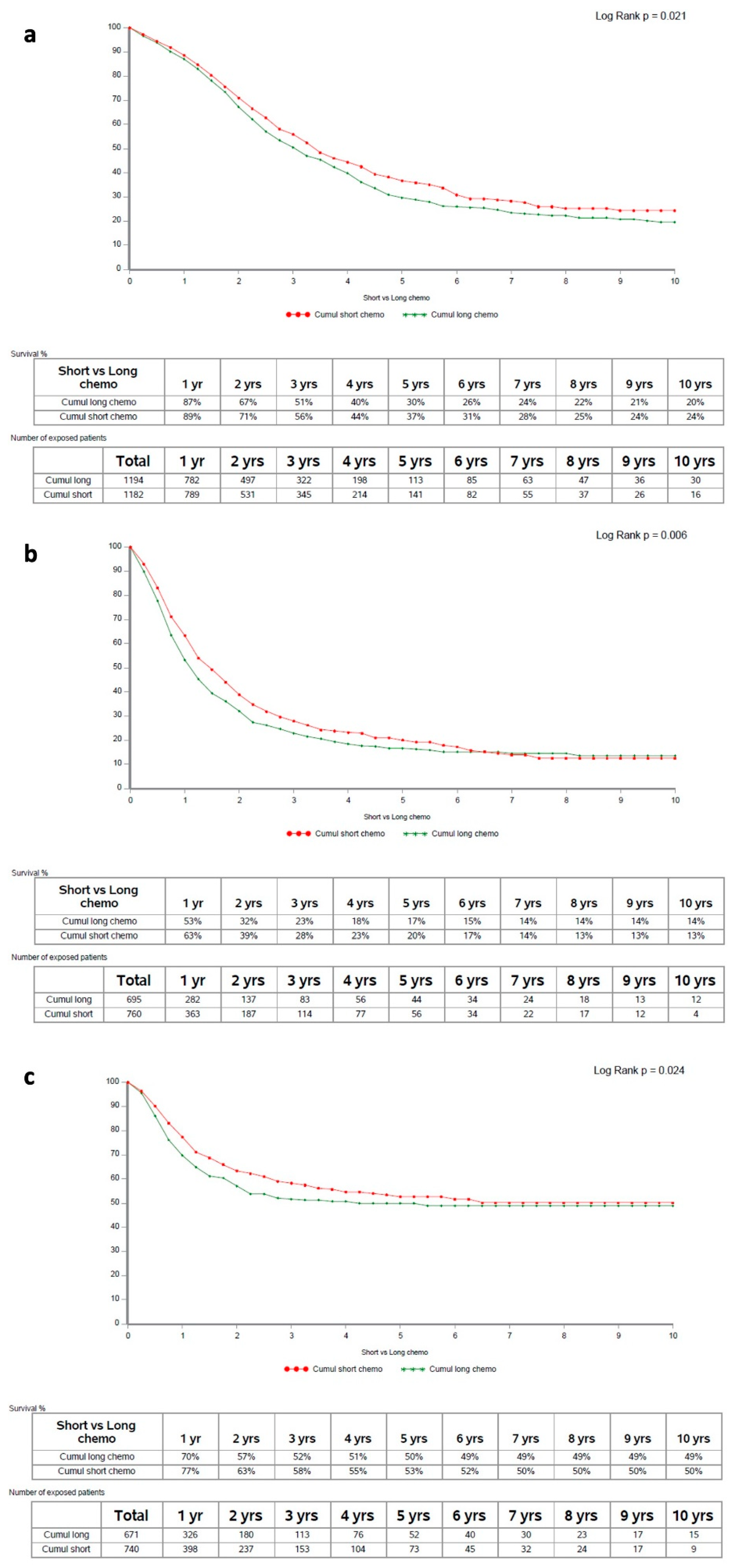
3.4. Pre-Operative Systemic Anticancer Therapy Duration
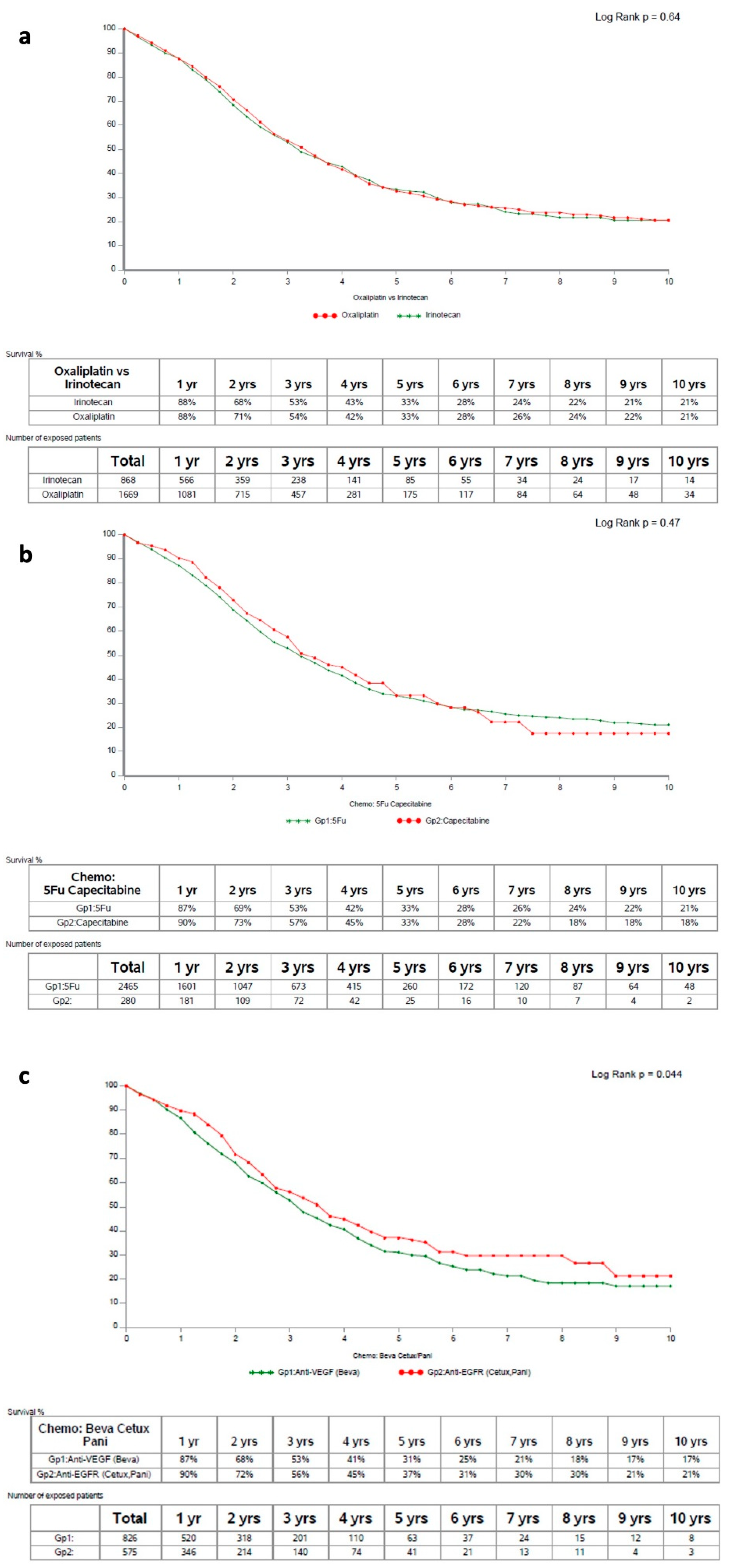
3.5. Pre-Operative Systemic Anticancer Therapy Modalities
3.6. Multivariable Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Prior Presentation
Abbreviations
| 5-FU: | 5-fluorouracil |
| CEA: | carcinoembryonic antigen |
| CLM: | colorectal liver metastases |
| CONSORT: | consolidated standards of reporting trials |
| CR: | complete response |
| DFS: | disease-free survival |
| EGFR: | epithelial growth factor receptor |
| HR: | hazard ratio |
| HS-RFS: | hepatic-specific relapse-free survival |
| IQR: | interquartile range |
| IV: | intravenous |
| mAb: | monoclonal antibody |
| N: | number |
| NA: | not available |
| NC/SD: | no change/stable disease |
| NE: | not evaluable |
| OS: | overall survival |
| PD: | progression of disease |
| PO: | per os |
| PO-SACT: | pre-operative systemic anticancer therapy |
| PR: | partial response |
| RAS: | rat sarcoma virus |
| SD: | standard deviation |
| UK: | unknown |
| VEGF: | vascular endothelial growth factor |
| Y: | yes |
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Vera, R.; González-Flores, E.; Rubio, C.; Urbano, J.; Camps, M.V.; Ciampi-Dopazo, J.J.; Rincón, J.O.; Macías, V.M.; Braco, M.A.G.; Suarez-Artacho, G. Multidisciplinary management of liver metastases in patients with colorectal cancer: A consensus of SEOM, AEC, SEOR, SERVEI, and SEMNIM. Clin. Transl. Oncol. 2020, 22, 647–662. [Google Scholar] [CrossRef] [PubMed]
- Poston, G.J.; Figueras, J.; Giuliante, F.; Nuzzo, G.; Sobrero, A.F.; Gigot, J.-F.; Nordlinger, B.; Adam, R.; Gruenberger, T.; Choti, M.A.; et al. Urgent need for a new staging system in advanced colorectal cancer. J. Clin. Oncol. 2008, 26, 4828–4833. [Google Scholar] [CrossRef] [PubMed]
- Bolhuis, K.; Kos, M.; van Oijen, M.G.H.; Swijnenburg, R.J.; Punt, C.J.A. Conversion strategies with chemotherapy plus targeted agents for colorectal cancer liver-only metastases: A systematic review. Eur. J. Cancer 2020, 141, 225–238. [Google Scholar] [CrossRef] [PubMed]
- Nordlinger, B.; Van Cutsem, E.; Rougier, P.; Köhne, C.-H.; Ychou, M.; Sobrero, A.; Adam, R.; Arvidsson, D.; Carrato, A.; Georgoulias, V.; et al. Does chemotherapy prior to liver resection increase the potential for cure in patients with metastatic colorectal cancer? A report from the European Colorectal Metastases Treatment Group. Eur. J. Cancer 2007, 43, 2037–2045. [Google Scholar] [CrossRef]
- Dekker, E.; Tanis, P.J.; Vleugels, J.L.A.; Kasi, P.M.; Wallace, M.B. Colorectal cancer. Lancet 2019, 394, 1467–1480. [Google Scholar] [CrossRef]
- Adam, R.; de Gramont, A.; Figueras, J.; Kokudo, N.; Kunstlinger, F.; Loyer, E.; Poston, G.; Rougier, P.; Rubbia-Brandt, L.; Sobrero, A.; et al. Managing synchronous liver metastases from colorectal cancer: A multidisciplinary international consensus. Cancer Treat. Rev. 2015, 41, 729–741. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Cervantes, A.; Nordlinger, B.; Arnold, D.; Group, E.G.W. Metastatic colorectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2014, 25 (Suppl. S3), iii1–iii9. [Google Scholar] [CrossRef]
- Adam, R.; Kitano, Y. Multidisciplinary approach of liver metastases from colorectal cancer. Ann. Gastroenterol. Surg. 2019, 3, 50–56. [Google Scholar] [CrossRef]
- Imai, K.; Adam, R.; Baba, H. How to increase the resectability of initially unresectable colorectal liver metastases: A surgical perspective. Ann. Gastroenterol. Surg. 2019, 3, 476–486. [Google Scholar] [CrossRef] [Green Version]
- Van Cutsem, E.; Cervantes, A.; Adam, R.; Sobrero, A.; van Krieken, J.H.; Aderka, D.; Aguilar, E.A.; Bardelli, A.; Benson, A.; Bodoky, G.; et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann. Oncol. 2016, 27, 1386–1422. [Google Scholar] [CrossRef] [PubMed]
- Kawaguchi, Y.; Vauthey, J.N. The Landmark Series: Randomized Control Trials Examining Perioperative Chemotherapy and Postoperative Adjuvant Chemotherapy for Resectable Colorectal Liver Metastasis. Ann. Surg. Oncol. 2020, 27, 4263–4270. [Google Scholar] [CrossRef] [PubMed]
- Poston, G.; Adam, R.; Xu, J.; Byrne, B.; Esser, R.; Malik, H.; Wasan, H. The role of cetuximab in converting initially unresectable colorectal cancer liver metastases for resection. Eur. J. Surg. Oncol. 2017, 43, 2001–2011. [Google Scholar] [CrossRef]
- Bridgewater, J.A.; Pugh, S.A.; Maishman, T.; Eminton, Z.; Mellor, J.; Whitehead, A.; Stanton, L.; Radford, M.; Corkhill, A.; Griffiths, G.O.; et al. Systemic chemotherapy with or without cetuximab in patients with resectable colorectal liver metastasis (New EPOC): Long-term results of a multicentre, randomised, controlled, phase 3 trial. Lancet Oncol. 2020, 21, 398–411. [Google Scholar] [CrossRef]
- Kumar, A.; Guss, Z.D.; Courtney, P.T.; Nalawade, V.; Sheridan, P.; Sarkar, R.R.; Banegas, M.P.; Rose, B.S.; Xu, R.; Murphy, J.D. Evaluation of the Use of Cancer Registry Data for Comparative Effectiveness Research. JAMA Netw. Open 2020, 3, e2011985. [Google Scholar] [CrossRef] [PubMed]
- Adam, R.; Yi, B.; Innominato, P.F.; Barroso, E.; Laurent, C.; Giuliante, F.; Capussotti, L.; Lapointe, R.; Regimbeau, J.-M.; Lopez-Ben, S.; et al. Resection of colorectal liver metastases after second-line chemotherapy: Is it worthwhile? A LiverMetSurvey analysis of 6415 patients. Eur. J. Cancer 2017, 78, 7–15. [Google Scholar] [CrossRef]
- Bonney, G.K.; Coldham, C.; Adam, R.; Kaiser, G.; Barroso, E.; Capussotti, L.; Laurent, C.; Verhoef, C.; Nuzzo, G.; Elias, D.; et al. Role of neoadjuvant chemotherapy in resectable synchronous colorectal liver metastasis; An international multi-center data analysis using LiverMetSurvey. J. Surg. Oncol. 2015, 111, 716–724. [Google Scholar] [CrossRef]
- Therasse, P.; Arbuck, S.G.; Eisenhauer, E.A.; Wanders, J.; Kaplan, R.S.; Rubinstein, L.; Verweij, J.; Van Glabbeke, M.; Van Oosterom, A.T.; Christian, M.C.; et al. New guidelines to evaluate the response to treatment in solid tumors. J. Natl. Cancer Inst. 2000, 92, 205–216. [Google Scholar] [CrossRef]
- Garden, O.J.; Rees, M.; Poston, G.J.; Mirza, D.; Saunders, M.; Ledermann, J.; Primrose, J.N.; Parks, R.W. Guidelines for resection of colorectal cancer liver metastases. Gut 2006, 55 (Suppl. S3), iii1–iii8. [Google Scholar] [CrossRef]
- Adam, R.; De Gramont, A.; Figueras, J.; Guthrie, A.; Kokudo, N.; Kunstlinger, F.; Loyer, E.; Poston, G.; Rougier, P.; Rubbia-Brandt, L.; et al. The oncosurgery approach to managing liver metastases from colorectal cancer: A multidisciplinary international consensus. Oncologist 2012, 17, 1225–1239. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, D.; Allum, W.H.; Stenning, S.P.; Thompson, J.N.; Van de Velde, C.J.; Nicolson, M.; Scarffe, J.H.; Lofts, F.J.; Falk, S.J.; Iveson, T.J.; et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N. Engl. J. Med. 2006, 355, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Al-Batran, S.-E.; Homann, N.; Pauligk, C.; Goetze, T.O.; Meiler, J.; Kasper, S.; Kopp, H.-G.; Mayer, F.; Haag, G.M.; Luley, K.; et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): A randomised, phase 2/3 trial. Lancet 2019, 393, 1948–1957. [Google Scholar] [PubMed]
- Nordlinger, B.; Sorbye, H.; Glimelius, B.; Poston, G.J.; Schlag, P.M.; Rougier, P.; Bechstein, W.O.; Primrose, J.N.; Walpole, E.T.; Finch-Jones, M.; et al. Perioperative FOLFOX4 chemotherapy and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC 40983): Long-term results of a randomised, controlled, phase 3 trial. Lancet Oncol. 2013, 14, 1208–1215. [Google Scholar] [CrossRef]
- Chionh, F.; Lau, D.; Yeung, Y.; Price, T.; Tebbutt, N. Oral versus intravenous fluoropyrimidines for colorectal cancer. Cochrane Database Syst. Rev. 2017, 7, CD008398. [Google Scholar] [CrossRef]
- Poston, G.J. The use of irinotecan and oxaliplatin in the treatment of advanced colorectal cancer. Eur. J. Surg. Oncol. 2005, 31, 325–330. [Google Scholar] [CrossRef]
- Innominato, P.F.; Karaboué, A.; Focan, C.; Chollet, P.; Giacchetti, S.; Bouchahda, M.; Ulusakarya, A.; Torsello, A.; Adam, R.; Lévi, F.A.; et al. Efficacy and safety of chronomodulated irinotecan, oxaliplatin, 5-fluorouracil and leucovorin combination as first- or second-line treatment against metastatic colorectal cancer: Results from the International EORTC 05011 Trial. Int. J. Cancer 2020, 148, 2512–2521. [Google Scholar] [CrossRef]
- Tappenden, P.; Jones, R.; Paisley, S.; Carroll, C. Systematic review and economic evaluation of bevacizumab and cetuximab for the treatment of metastatic colorectal cancer. Health Technol. Assess. 2007, 11, 1–128. [Google Scholar] [CrossRef] [PubMed]
- Melstrom, L.G.; Warner, S.G.; Wong, P.; Sun, V.; Raoof, M.; Singh, G.; Chavin, K.D.; Fong, Y.; Adam, R.; Hugh, T.J. Management of disappearing colorectal liver metastases: An international survey. HPB 2020, 23, 506–511. [Google Scholar] [CrossRef]
- Ulusakarya, A.; Innominato, P.F.; Bouchahda, M.; Levi, F.A.; Adam, R. Hepatic metastases resection after cetuximab: Are we missing something? Lancet Oncol. 2020, 21, e228. [Google Scholar] [CrossRef]
- Duwe, G.; Knitter, S.; Pesthy, S.; Beierle, A.; Bahra, M.; Schmelzle, M.; Schmuck, R.; Lohneis, P.; Raschzok, N.; Öllinger, R.; et al. Hepatotoxicity following systemic therapy for colorectal liver metastases and the impact of chemotherapy-associated liver injury on outcomes after curative liver resection. Eur. J. Surg. Oncol. 2017, 43, 1668–1681. [Google Scholar] [CrossRef]
- Choti, M.A. Chemotherapy-associated hepatotoxicity: Do we need to be concerned? Ann. Surg. Oncol. 2009, 16, 2391–2394. [Google Scholar] [CrossRef] [PubMed]
- Booth, C.M.; Nanji, S.; Wei, X.; Mackillop, W.J. Management and Outcome of Colorectal Cancer Liver Metastases in Elderly Patients: A Population-Based Study. JAMA Oncol. 2015, 1, 1111–1119. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Deng, Y. Capecitabine versus Continuous Infusion Fluorouracil for the Treatment of Advanced or Metastatic Colorectal Cancer: A Meta-analysis. Curr. Treat. Options Oncol. 2018, 19, 77. [Google Scholar] [CrossRef]
- Petrelli, F.; Cabiddu, M.; Barni, S. 5-Fluorouracil or capecitabine in the treatment of advanced colorectal cancer: A pooled-analysis of randomized trials. Med. Oncol. 2012, 29, 1020–1029. [Google Scholar] [CrossRef] [PubMed]
- Grothey, A.; Sobrero, A.F.; Shields, A.F.; Yoshino, T.; Paul, J.; Taieb, J.; Souglakos, J.; Shi, Q.; Kerr, R.; Labianca, R.; et al. Duration of Adjuvant Chemotherapy for Stage III Colon Cancer. N. Engl. J. Med. 2018, 378, 1177–1188. [Google Scholar] [CrossRef] [PubMed]
- Tournigand, C.; André, T.; Achille, E.; Lledo, G.; Flesh, M.; Mery-Mignard, D.; Quinaux, E.; Couteau, C.; Buyse, M.; Ganem, G.; et al. FOLFIRI followed by FOLFOX6 or the reverse sequence in advanced colorectal cancer: A randomized GERCOR study. J. Clin. Oncol. 2004, 22, 229–237. [Google Scholar] [CrossRef]
- Grothey, A.; Sargent, D.; Goldberg, R.M.; Schmoll, H.J. Survival of patients with advanced colorectal cancer improves with the availability of fluorouracil-leucovorin, irinotecan, and oxaliplatin in the course of treatment. J. Clin. Oncol. 2004, 22, 1209–1214. [Google Scholar] [CrossRef]
- Allegra, C.J.; Rumble, R.B.; Hamilton, S.R.; Mangu, P.B.; Roach, N.; Hantel, A.; Schilsky, R.L. Extended RAS Gene Mutation Testing in Metastatic Colorectal Carcinoma to Predict Response to Anti-Epidermal Growth Factor Receptor Monoclonal Antibody Therapy: American Society of Clinical Oncology Provisional Clinical Opinion Update 2015. J. Clin. Oncol. 2016, 34, 179–185. [Google Scholar] [CrossRef]
- Kafatos, G.; Niepel, D.; Lowe, K.; Jenkins-Anderson, S.; Westhead, H.; Garawin, T.; Traugottová, Z.; Bilalis, A.; Molnar, E.; Timar, J.; et al. RAS mutation prevalence among patients with metastatic colorectal cancer: A meta-analysis of real-world data. Biomark. Med. 2017, 11, 751–760. [Google Scholar] [CrossRef]
- Brudvik, K.W.; Kopetz, S.E.; Li, L.; Conrad, C.; Aloia, T.A.; Vauthey, J. Meta-analysis of KRAS mutations and survival after resection of colorectal liver metastases. Br. J. Surg. 2015, 102, 1175–1183. [Google Scholar] [CrossRef] [Green Version]
- Phipps, A.I.; Buchanan, D.D.; Makar, K.W.; Win, A.K.; Baron, J.A.; Lindor, N.M.; Potter, J.D.; Newcomb, P.A. KRAS-mutation status in relation to colorectal cancer survival: The joint impact of correlated tumour markers. Br. J. Cancer 2013, 108, 1757–1764. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Liang, M.; Liang, X.; Yang, L.; Su, M.; Lai, K.P. Chemotherapeutic Effectiveness of Combining Cetuximab for Metastatic Colorectal Cancer Treatment: A System Review and Meta-Analysis. Front. Oncol. 2020, 10, 868. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, E.M.; Abouelkhair, K.M. Clinical outcome of panitumumab for metastatic colorectal cancer with wild-type KRAS status: A meta-analysis of randomized clinical trials. Med. Oncol. 2011, 28 (Suppl. S1), S310–S317. [Google Scholar] [CrossRef] [PubMed]
- Serrano, P.E.; Carter, D.N.; Li, C.; Valencia, M.; Ruo, L.; Parpia, S.; Simunovic, M.; Levine, O. Adjuvant Chemotherapy with or without Biologics Including Antiangiogenics and Monoclonal Antibodies Targeting EGFR and EpCAM in Colorectal Cancer: A Systematic Review and Meta-analysis. J. Surg. Res. 2019, 239, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Khattak, M.A.; Martin, H.; Davidson, A.; Phillips, M. Role of first-line anti-epidermal growth factor receptor therapy compared with anti-vascular endothelial growth factor therapy in advanced colorectal cancer: A meta-analysis of randomized clinical trials. Clin. Colorectal Cancer 2015, 14, 81–90. [Google Scholar] [CrossRef]
- Tomasello, G.; Petrelli, F.; Ghidini, M.; Russo, A.; Passalacqua, R.; Barni, S. FOLFOXIRI Plus Bevacizumab as Conversion Therapy for Patients with Initially Unresectable Metastatic Colorectal Cancer: A Systematic Review and Pooled Analysis. JAMA Oncol. 2017, 3, e170278. [Google Scholar] [CrossRef]
- Lévi, F.A.; Boige, V.; Hebbar, M.; Smith, D.; Lepère, C.; Focan, C.; Karaboué, A.; Guimbaud, R.; Carvalho, C.; Tumolo, S.; et al. Conversion to resection of liver metastases from colorectal cancer with hepatic artery infusion of combined chemotherapy and systemic cetuximab in multicenter trial OPTILIV. Ann. Oncol. 2016, 27, 267–274. [Google Scholar] [CrossRef]
- Adam, R.; Aloia, T.; Lévi, F.; Wicherts, D.A.; de Haas, R.J.; Paule, B.; Bralet, M.-P.; Bouchahda, M.; Machover, D.; Ducreux, M.; et al. Hepatic resection after rescue cetuximab treatment for colorectal liver metastases previously refractory to conventional systemic therapy. J. Clin. Oncol. 2007, 25, 4593–4602. [Google Scholar] [CrossRef]
- Folprecht, G.; Grothey, A.; Alberts, S.; Raab, H.R.; Kohne, C.H. Neoadjuvant treatment of unresectable colorectal liver metastases: Correlation between tumour response and resection rates. Ann. Oncol. 2005, 16, 1311–1319. [Google Scholar] [CrossRef]
- Smolenschi, C.; Perret, A.; Dall’Armellina, F.; Boige, V.; Malka, D.; Hollebecque, A.; Ducreux, M. An appraisal of emerging second line therapies for metastatic colorectal cancer. Expert Rev. Gastroenterol. Hepatol. 2020, 1840975, 165–179. [Google Scholar] [CrossRef]
- Galvano, A.; Incorvaia, L.; Badalamenti, G.; Rizzo, S.; Guarini, A.; Cusenza, S.; Castellana, L.; Barraco, N.; Calò, V.; Cutaia, S.; et al. How to Deal with Second Line Dilemma in Metastatic Colorectal Cancer? A Systematic Review and Meta-Analysis. Cancers 2019, 11, 1189. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, S.; Chun, Y.S.; Kopetz, S.E.; Vauthey, J.N. Biomarkers in colorectal liver metastases. Br. J. Surg. 2018, 105, 618–627. [Google Scholar] [CrossRef] [PubMed]
- Guinney, J.; Dienstmann, R.; Wang, X.; De Reyniès, A.; Schlicker, A.; Soneson, C.; Marisa, L.; Roepman, P.; Nyamundanda, G.; Angelino, P.; et al. The consensus molecular subtypes of colorectal cancer. Nat. Med. 2015, 21, 1350–1356. [Google Scholar] [CrossRef] [PubMed]
- Testa, U.; Castelli, G.; Pelosi, E. Genetic Alterations of Metastatic Colorectal Cancer. Biomedicines 2020, 8, 414. [Google Scholar] [CrossRef] [PubMed]
- Malka, D.; Lièvre, A.; André, T.; Taïeb, J.; Ducreux, M.; Bibeau, F. Immune scores in colorectal cancer: Where are we? Eur. J. Cancer 2020, 140, 105–118. [Google Scholar] [CrossRef]
- Yu, X.; Zhu, L.; Liu, J.; Xie, M.; Chen, J.; Li, J. Emerging Role of Immunotherapy for Colorectal Cancer with Liver Metastasis. Onco Targets Ther. 2020, 13, 11645–11658. [Google Scholar] [CrossRef]
- Bilchik, A.J.; Poston, G.; Adam, R.; Choti, M.A. Prognostic variables for resection of colorectal cancer hepatic metastases: An evolving paradigm. J. Clin. Oncol. 2008, 26, 5320–5321. [Google Scholar] [CrossRef]
- Rehman, A.H.; Jones, R.P.; Poston, G. Prognostic and predictive markers in liver limited stage IV colorectal cancer. Eur. J. Surg. Oncol. 2019, 45, 2251–2256. [Google Scholar] [CrossRef]
- Gomez, D.; Cameron, I.C. Prognostic scores for colorectal liver metastasis: Clinically important or an academic exercise? HPB 2010, 12, 227–238. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | (N = 2793) |
|---|---|
| Age [median; IQR] Mean ± SD | [61.3; 14.8] 60.6 ± 12.3 |
| Gender [M/F]; N (%) | 1712 (61.4)/1076 (38.6) |
| Primary Tumor Location [Left-sided/Right-sided/multiple] | 2131 (77.6)/549 (20.0)/65 (2.4) |
| Adjuvant chemotherapy [Y] | 738 (28.5) |
| Neoadjuvant radiotherapy [Y] | 270 (10.4) |
| Synchronous Liver Metastases [Y] | 2168 (78.0) |
| Number of liver metastases [1/>3/>7] | 440 (18.4)/1341 (56.2)/611 (25.6) |
| The largest size (mm) of liver metastases (mean ± SD) | 48.7 ± 42.4 |
| At least one lesion ≥50 mm [Y] | 929 (40.1) |
| Bilobar involvement [Y] | 1984 (71.9) |
| Concomitant extrahepatic disease [Y] | 305 (12.9) |
| Type of Resection [non anatomical/staged/combined techniques/portal occlusion] | 1826 (67.5)/614 (22.4)/1259 (46.1)/734 (27.1) |
| Major hepatectomy [Y] | 1910 (70.3) |
| Only 1 hepatectomy/patient [Y] | 2073 (74.2) |
| Microscopically complete resection [Y] | 1622 (70.7) |
| Complete pathological response [Y] | 244 (10.2) |
| Length (days) of post-op hospital stay (mean/SD) | 13.0/10.4 |
| Postoperative complications [Y] | 891 (34.6) |
| Abnormal non-tumoral liver [Y] | 1379 (59.9) |
| 1-month mortality [Y] | 38 (1.5) |
| PO-SACT Feature | N (%) |
| Regimen drugs [Y] | |
| 5-FluoroUracil | 2465 (88.3) |
| Capecitabine | 280 (10.0) |
| Oxaliplatin | 1669 (59.8) |
| Irinotecan | 868 (31.1) |
| Anti-EGFR mAb | 575 (20.6) |
| Anti-VEGF mAb | 826 (29.6) |
| Triplet combination | 208 (7.4) |
| Doublet | 2537 (90.8) |
| Line of treatment | |
| 1 | 2333 (83.5) |
| 2 | 333 (11.9) |
| 3+ | 127 (4.5) |
| Cumulative # of cycles | |
| (mean/SD) | 7.5/4.0 |
| Median | 8.0 |
| IQR | [6; 12] |
| 1–6 | 1046 (37.5) |
| 7–12 | 1003 (35.9) |
| 13+ | 369 (13.2) |
| UK | 375 (13.4) |
| Objective response to PO-SACT | |
| CR | 70 (2.5) |
| PR | 2103 (75.2) |
| NC/SD | 359 (12.9) |
| PD | 109 (3.9) |
| NA or NE | 152 (5.4) |
| Received postoperative chemotherapy [Y] | |
| 1341 (48.0) |
| Parameter | Value | Univariate p | Multivariable p | Multivariable HR | HR 95% Confidence Limits |
|---|---|---|---|---|---|
| Liver curative surgery | No | <0.0001 | <0.0001 | 1.77 | 1.43; 2.17 |
| Concomitant extrahepatic disease | Yes | 0.003 | 0.0442 | 1.27 | 1.01; 1.61 |
| Isolated liver metastasis | No | <0.0001 | 0.0022 | 1.44 | 1.14; 1.82 |
| Nodal involvement of primary | Yes | <0.0001 | 0.0051 | 1.28 | 1.08; 1.53 |
| First-line PO-SACT | No | 0.0008 | 0.0003 | 1.50 | 1.21; 1.87 |
| Use of anti-EGFR mAb | No | 0.081 | 0.0491 | 1.24 | 1.00; 1.55 |
| PO-SACT duration | Long | 0.001 | 0.0460 | 1.18 | 1.00; 1.39 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Innominato, P.F.; Cailliez, V.; Allard, M.-A.; Lopez-Ben, S.; Ferrero, A.; Marques, H.; Hubert, C.; Giuliante, F.; Pereira, F.; Cugat, E.; et al. Impact of Preoperative Chemotherapy Features on Patient Outcomes after Hepatectomy for Initially Unresectable Colorectal Cancer Liver Metastases: A LiverMetSurvey Analysis. Cancers 2022, 14, 4340. https://doi.org/10.3390/cancers14174340
Innominato PF, Cailliez V, Allard M-A, Lopez-Ben S, Ferrero A, Marques H, Hubert C, Giuliante F, Pereira F, Cugat E, et al. Impact of Preoperative Chemotherapy Features on Patient Outcomes after Hepatectomy for Initially Unresectable Colorectal Cancer Liver Metastases: A LiverMetSurvey Analysis. Cancers. 2022; 14(17):4340. https://doi.org/10.3390/cancers14174340
Chicago/Turabian StyleInnominato, Pasquale F., Valérie Cailliez, Marc-Antoine Allard, Santiago Lopez-Ben, Alessandro Ferrero, Hugo Marques, Catherine Hubert, Felice Giuliante, Fernando Pereira, Esteban Cugat, and et al. 2022. "Impact of Preoperative Chemotherapy Features on Patient Outcomes after Hepatectomy for Initially Unresectable Colorectal Cancer Liver Metastases: A LiverMetSurvey Analysis" Cancers 14, no. 17: 4340. https://doi.org/10.3390/cancers14174340
APA StyleInnominato, P. F., Cailliez, V., Allard, M. -A., Lopez-Ben, S., Ferrero, A., Marques, H., Hubert, C., Giuliante, F., Pereira, F., Cugat, E., Mirza, D. F., Costa-Maia, J., Serrablo, A., Lapointe, R., Dopazo, C., Tralhao, J., Kaiser, G., Chen, J. -S., Garcia-Borobia, F., ... Adam, R. (2022). Impact of Preoperative Chemotherapy Features on Patient Outcomes after Hepatectomy for Initially Unresectable Colorectal Cancer Liver Metastases: A LiverMetSurvey Analysis. Cancers, 14(17), 4340. https://doi.org/10.3390/cancers14174340