
Changes in the Epidemiology of Hepatocellular Carcinoma in Asia



Abstract
:Simple Summary
Abstract
1. Introduction
2. Viral Hepatitis-Related HCC
2.1. Hepatitis B Virus (HBV)
2.2. Hepatitis C Virus (HCV)
3. NAFLD and Obesity-Related HCC
4. Aflatoxin-Related HCC
5. Alcoholic Liver Disease
6. Estimated Trend of Liver Cancer in Asia
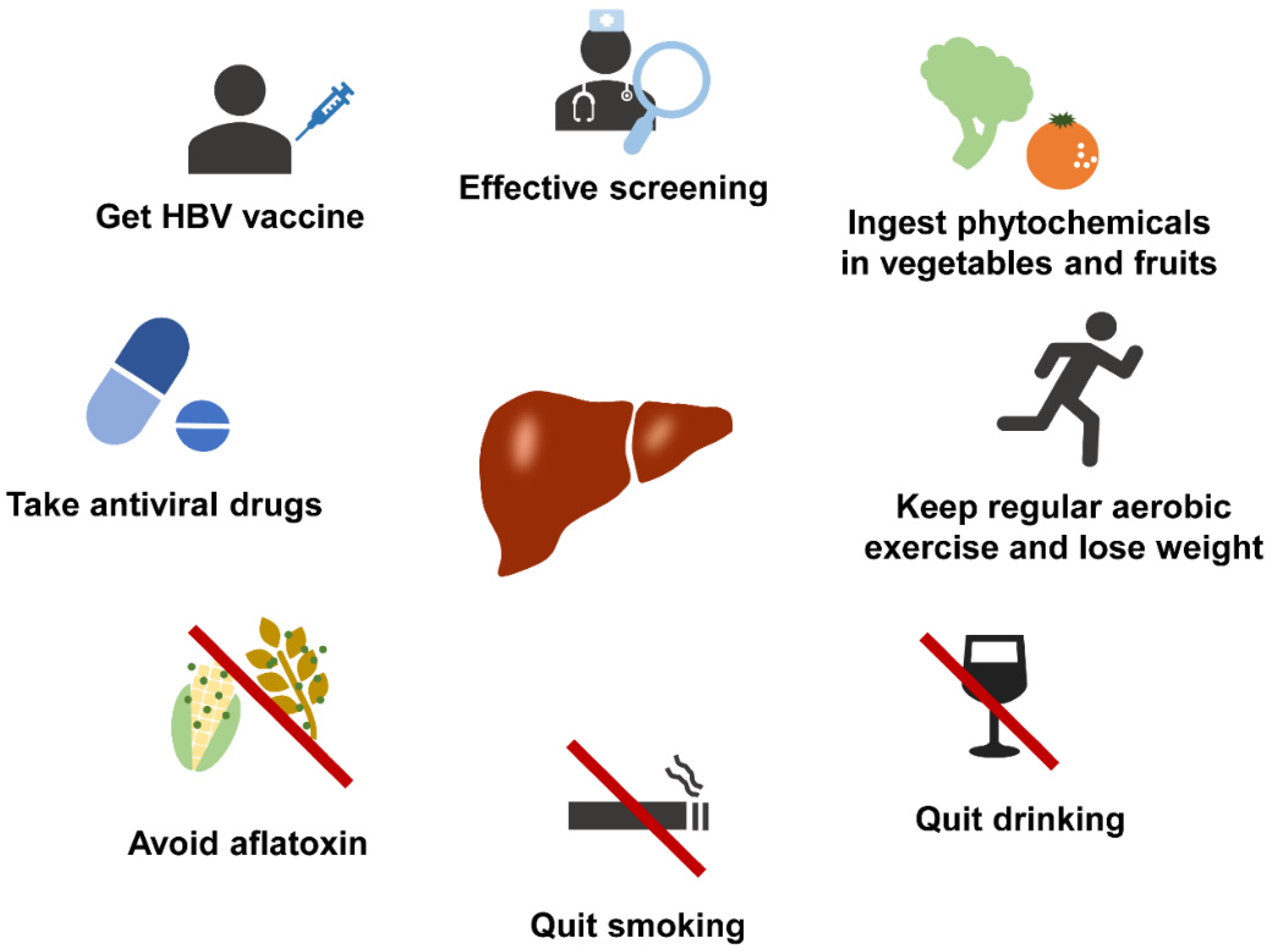
7. Prevention Methods of HCC in Asia
7.1. Prevention of Viral Hepatitis-Related HCC
7.2. Maintain a Healthy Lifestyle
7.3. Pharmacological Therapies
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| AAPC | average annual percent change |
| ASR | Age-Standardized Rate |
| CHB | chronic hepatitis B |
| DAA | direct-acting antiviral |
| HBV | hepatitis B virus |
| HCC | hepatocellular carcinoma |
| HCV | hepatitis C virus |
| IFN | interferon |
| NAFLD | non-alcoholic liver disease |
| NAs | nucleos(c)ide analogs |
References
- WHO. Data Visualization Tools for Exploring the Global Cancer Burden in 2020. 2020. Available online: https://gco.iarc.fr/today/ (accessed on 1 September 2022).
- Llovet, J.M.; Zucman-Rossi, J.; Pikarsky, E.; Sangro, B.; Schwartz, M.; Sherman, M.; Gores, G. Hepatocellular carcinoma. Nat. Rev. Dis. Primers 2016, 2, 16018. [Google Scholar] [CrossRef]
- Kulik, L.; El-Serag, H.B. Epidemiology and Management of Hepatocellular Carcinoma. Gastroenterology 2019, 156, 477–491.e1. [Google Scholar] [CrossRef]
- Petrick, J.L.; Florio, A.A.; Znaor, A.; Ruggieri, D.; Laversanne, M.; Alvarez, C.S.; Ferlay, J.; Valery, P.C.; Bray, F.; McGlynn, K.A. International trends in hepatocellular carcinoma incidence, 1978–2012. Int. J. Cancer 2020, 147, 317–330. [Google Scholar] [CrossRef]
- Zhang, C.H.; Cheng, Y.; Zhang, S.; Fan, J.; Gao, Q. Changing epidemiology of hepatocellular carcinoma in Asia. Liver Int. 2022, 42, 2029–2041. [Google Scholar] [CrossRef] [PubMed]
- Zucman-Rossi, J.; Villanueva, A.; Nault, J.C.; Llovet, J.M. Genetic Landscape and Biomarkers of Hepatocellular Carcinoma. Gastroenterology 2015, 149, 1226–1239.e1224. [Google Scholar] [CrossRef]
- Tang, A.; Hallouch, O.; Chernyak, V.; Kamaya, A.; Sirlin, C.B. Epidemiology of hepatocellular carcinoma: Target population for surveillance and diagnosis. Abdom. Radiol. 2018, 43, 13–25. [Google Scholar] [CrossRef]
- Liaw, Y.F. Antiviral therapy of chronic hepatitis B: Opportunities and challenges in Asia. J. Hepatol. 2009, 51, 403–410. [Google Scholar] [CrossRef]
- Global Burden of Disease Liver Cancer Collaboration; Akinyemiju, T.; Abera, S.; Ahmed, M.; Alam, N.; Alemayohu, M.A.; Allen, C.; Al-Raddadi, R.; Alvis-Guzman, N.; Amoako, Y.; et al. The Burden of Primary Liver Cancer and Underlying Etiologies from 1990 to 2015 at the Global, Regional, and National Level: Results from the Global Burden of Disease Study 2015. JAMA Oncol. 2017, 3, 1683–1691. [Google Scholar] [CrossRef]
- Chen, C.J.; Wang, L.Y.; Yu, M.W. Epidemiology of hepatitis B virus infection in the Asia-Pacific region. J. Gastroenterol. Hepatol. 2000, 15, E3–E6. [Google Scholar] [CrossRef] [PubMed]
- Bhaumik, P. Epidemiology of Viral Hepatitis and Liver Diseases in India. Euroasian J. Hepatogastroenterol. 2015, 5, 34–36. [Google Scholar] [CrossRef]
- Liang, X.; Bi, S.; Yang, W.; Wang, L.; Cui, G.; Cui, F.; Zhang, Y.; Liu, J.; Gong, X.; Chen, Y.; et al. Epidemiological serosurvey of hepatitis B in China--declining HBV prevalence due to hepatitis B vaccination. Vaccine 2009, 27, 6550–6557. [Google Scholar] [CrossRef]
- WHO. Global Health Estimates 2015: Deaths by Cause, Age, Sex, by Country and by Region, 2000–2015. 2016. Available online: https://www.who.int/healthinfo/global_burden_disease/estimates_regional_2000_2015/en/ (accessed on 10 June 2017).
- Ang, S.F.; Ng, E.S.; Li, H.; Ong, Y.H.; Choo, S.P.; Ngeow, J.; Toh, H.C.; Lim, K.H.; Yap, H.Y.; Tan, C.K.; et al. The Singapore Liver Cancer Recurrence (SLICER) Score for relapse prediction in patients with surgically resected hepatocellular carcinoma. PLoS ONE 2015, 10, e0118658. [Google Scholar] [CrossRef]
- Chiang, C.J.; Yang, Y.W.; You, S.L.; Lai, M.S.; Chen, C.J. Thirty-year outcomes of the national hepatitis B immunization program in Taiwan. JAMA 2013, 310, 974–976. [Google Scholar] [CrossRef]
- Chen, C.H.; Yang, P.M.; Huang, G.T.; Lee, H.S.; Sung, J.L.; Sheu, J.C. Estimation of seroprevalence of hepatitis B virus and hepatitis C virus in Taiwan from a large-scale survey of free hepatitis screening participants. J. Formos Med. Assoc. 2007, 106, 148–155. [Google Scholar] [CrossRef]
- Yuen, M.F.; Cheng, C.C.; Lauder, I.J.; Lam, S.K.; Ooi, C.G.; Lai, C.L. Early detection of hepatocellular carcinoma increases the chance of treatment: Hong Kong experience. Hepatology 2000, 31, 330–335. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.L.; Yuen, M.F. Prevention of hepatitis B virus-related hepatocellular carcinoma with antiviral therapy. Hepatology 2013, 57, 399–408. [Google Scholar] [CrossRef]
- Hosaka, T.; Suzuki, F.; Kobayashi, M.; Seko, Y.; Kawamura, Y.; Sezaki, H.; Akuta, N.; Suzuki, Y.; Saitoh, S.; Arase, Y.; et al. Long-term entecavir treatment reduces hepatocellular carcinoma incidence in patients with hepatitis B virus infection. Hepatology 2013, 58, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Wong, G.L.; Chan, H.L.; Mak, C.W.; Lee, S.K.; Ip, Z.M.; Lam, A.T.; Iu, H.W.; Leung, J.M.; Lai, J.W.; Lo, A.O.; et al. Entecavir treatment reduces hepatic events and deaths in chronic hepatitis B patients with liver cirrhosis. Hepatology 2013, 58, 1537–1547. [Google Scholar] [CrossRef]
- Wu, C.Y.; Lin, J.T.; Ho, H.J.; Su, C.W.; Lee, T.Y.; Wang, S.Y.; Wu, C.; Wu, J.C. Association of nucleos(t)ide analogue therapy with reduced risk of hepatocellular carcinoma in patients with chronic hepatitis B: A nationwide cohort study. Gastroenterology 2014, 147, 143–151.e5. [Google Scholar] [CrossRef]
- Gower, E.; Estes, C.; Blach, S.; Razavi-Shearer, K.; Razavi, H. Global epidemiology and genotype distribution of the hepatitis C virus infection. J. Hepatol. 2014, 61 (Suppl. 1), S45–S57. [Google Scholar] [CrossRef] [Green Version]
- Butt, A.S.; Abbas, Z.; Jafri, W. Hepatocellular carcinoma in pakistan: Where do we stand? Hepat. Mon. 2012, 12, e6023. [Google Scholar] [CrossRef]
- Ahmed, B.; Ali, T.; Qureshi, H.; Hamid, S. Population-attributable estimates for risk factors associated with hepatitis B and C: Policy implications for Pakistan and other South Asian countries. Hepatol. Int. 2013, 7, 500–507. [Google Scholar] [CrossRef]
- Bosan, A.; Qureshi, H.; Bile, K.M.; Ahmad, I.; Hafiz, R. A review of hepatitis viral infections in Pakistan. J. Pak. Med. Assoc. 2010, 60, 1045–1058. [Google Scholar]
- Okuda, K.; Ohtsuki, T.; Obata, H.; Tomimatsu, M.; Okazaki, N.; Hasegawa, H.; Nakajima, Y.; Ohnishi, K. Natural history of hepatocellular carcinoma and prognosis in relation to treatment. Study of 850 patients. Cancer 1985, 56, 918–928. [Google Scholar] [CrossRef]
- Kudo, M. Management of Hepatocellular Carcinoma in Japan as a World-Leading Model. Liver Cancer 2018, 7, 134–147. [Google Scholar] [CrossRef]
- Tanaka, H.; Imai, Y.; Hiramatsu, N.; Ito, Y.; Imanaka, K.; Oshita, M.; Hijioka, T.; Katayama, K.; Yabuuchi, I.; Yoshihara, H.; et al. Declining incidence of hepatocellular carcinoma in Osaka, Japan, from 1990 to 2003. Ann. Intern Med. 2008, 148, 820–826. [Google Scholar] [CrossRef]
- Umemura, T.; Ichijo, T.; Yoshizawa, K.; Tanaka, E.; Kiyosawa, K. Epidemiology of hepatocellular carcinoma in Japan. J. Gastroenterol. 2009, 44 (Suppl. 19), 102–107. [Google Scholar] [CrossRef]
- Yeole, B.B. Trends in cancer incidence in esophagus, stomach, colon, rectum and liver in males in India. Asian Pac. J. Cancer Prev. 2008, 9, 97–100. [Google Scholar]
- Kumar, M.; Kumar, R.; Hissar, S.S.; Saraswat, M.K.; Sharma, B.C.; Sakhuja, P.; Sarin, S.K. Risk factors analysis for hepatocellular carcinoma in patients with and without cirrhosis: A case-control study of 213 hepatocellular carcinoma patients from India. J. Gastroenterol. Hepatol. 2007, 22, 1104–1111. [Google Scholar] [CrossRef]
- Angulo, P. Nonalcoholic fatty liver disease. N. Engl. J. Med. 2002, 346, 1221–1231. [Google Scholar] [CrossRef]
- Wong, V.W.; Hui, A.Y.; Tsang, S.W.; Chan, J.L.; Wong, G.L.; Chan, A.W.; So, W.Y.; Cheng, A.Y.; Tong, P.C.; Chan, F.K.; et al. Prevalence of undiagnosed diabetes and postchallenge hyperglycaemia in Chinese patients with non-alcoholic fatty liver disease. Aliment. Pharmacol. Ther. 2006, 24, 1215–1222. [Google Scholar] [CrossRef]
- Ascha, M.S.; Hanouneh, I.A.; Lopez, R.; Tamimi, T.A.; Feldstein, A.F.; Zein, N.N. The incidence and risk factors of hepatocellular carcinoma in patients with nonalcoholic steatohepatitis. Hepatology 2010, 51, 1972–1978. [Google Scholar] [CrossRef]
- Fan, J.G. Epidemiology of alcoholic and nonalcoholic fatty liver disease in China. J. Gastroenterol. Hepatol. 2013, 28 (Suppl. 1), 11–17. [Google Scholar] [CrossRef] [PubMed]
- Estes, C.; Anstee, Q.M.; Arias-Loste, M.T.; Bantel, H.; Bellentani, S.; Caballeria, J.; Colombo, M.; Craxi, A.; Crespo, J.; Day, C.P.; et al. Modeling NAFLD disease burden in China, France, Germany, Italy, Japan, Spain, United Kingdom, and United States for the period 2016–2030. J. Hepatol. 2018, 69, 896–904. [Google Scholar] [CrossRef] [PubMed]
- Cho, E.J.; Kwack, M.S.; Jang, E.S.; You, S.J.; Lee, J.H.; Kim, Y.J.; Yoon, J.H.; Lee, H.S. Relative etiological role of prior hepatitis B virus infection and nonalcoholic fatty liver disease in the development of non-B non-C hepatocellular carcinoma in a hepatitis B-endemic area. Digestion 2011, 84 (Suppl. 1), 17–22. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.G.; Kim, S.U.; Wong, V.W. New trends on obesity and NAFLD in Asia. J. Hepatol. 2017, 67, 862–873. [Google Scholar] [CrossRef] [PubMed]
- Asia Pacific Cohort Studies Collaboration. The burden of overweight and obesity in the Asia-Pacific region. Obes. Rev. 2007, 8, 191–196. [Google Scholar] [CrossRef]
- Yu, M.W.; Shih, W.L.; Lin, C.L.; Liu, C.J.; Jian, J.W.; Tsai, K.S.; Chen, C.J. Body-mass index and progression of hepatitis B: A population-based cohort study in men. J. Clin. Oncol. 2008, 26, 5576–5582. [Google Scholar] [CrossRef]
- Chen, C.L.; Yang, H.I.; Yang, W.S.; Liu, C.J.; Chen, P.J.; You, S.L.; Wang, L.Y.; Sun, C.A.; Lu, S.N.; Chen, D.S.; et al. Metabolic factors and risk of hepatocellular carcinoma by chronic hepatitis B/C infection: A follow-up study in Taiwan. Gastroenterology 2008, 135, 111–121. [Google Scholar] [CrossRef]
- Huang, T.S.; Lin, C.L.; Lu, M.J.; Yeh, C.T.; Liang, K.H.; Sun, C.C.; Shyu, Y.C.; Chien, R.N. Diabetes, hepatocellular carcinoma, and mortality in hepatitis C-infected patients: A population-based cohort study. J. Gastroenterol. Hepatol. 2017, 32, 1355–1362. [Google Scholar] [CrossRef]
- Ramachandran, A.; Snehalatha, C. Rising burden of obesity in Asia. J. Obes. 2010, 2010, 868573. [Google Scholar] [CrossRef] [PubMed]
- Caldwell, S.H.; Crespo, D.M.; Kang, H.S.; Al-Osaimi, A.M. Obesity and hepatocellular carcinoma. Gastroenterology 2004, 127 (Suppl. 1), S97–S103. [Google Scholar] [CrossRef] [PubMed]
- Yoon, K.H.; Lee, J.H.; Kim, J.W.; Cho, J.H.; Choi, Y.H.; Ko, S.H.; Zimmet, P.; Son, H.Y. Epidemic obesity and type 2 diabetes in Asia. Lancet 2006, 368, 1681–1688. [Google Scholar] [CrossRef]
- Magnussen, A.; Parsi, M.A. Aflatoxins, hepatocellular carcinoma and public health. World J. Gastroenterol. 2013, 19, 1508–1512. [Google Scholar] [CrossRef]
- McGlynn, K.A.; Petrick, J.L.; London, W.T. Global epidemiology of hepatocellular carcinoma: An emphasis on demographic and regional variability. Clin. Liver Dis. 2015, 19, 223–238. [Google Scholar] [CrossRef]
- Sun, Z.; Chen, T.; Thorgeirsson, S.S.; Zhan, Q.; Chen, J.; Park, J.H.; Lu, P.; Hsia, C.C.; Wang, N.; Xu, L.; et al. Dramatic reduction of liver cancer incidence in young adults: 28 year follow-up of etiological interventions in an endemic area of China. Carcinogenesis 2013, 34, 1800–1805. [Google Scholar] [CrossRef]
- Chen, J.G.; Egner, P.A.; Ng, D.; Jacobson, L.P.; Munoz, A.; Zhu, Y.R.; Qian, G.S.; Wu, F.; Yuan, J.M.; Groopman, J.D.; et al. Reduced aflatoxin exposure presages decline in liver cancer mortality in an endemic region of China. Cancer Prev. Res. 2013, 6, 1038–1045. [Google Scholar] [CrossRef]
- Hassan, M.M.; Hwang, L.Y.; Hatten, C.J.; Swaim, M.; Li, D.; Abbruzzese, J.L.; Beasley, P.; Patt, Y.Z. Risk factors for hepatocellular carcinoma: Synergism of alcohol with viral hepatitis and diabetes mellitus. Hepatology 2002, 36, 1206–1213. [Google Scholar] [CrossRef]
- Setshedi, M.; Wands, J.R.; Monte, S.M. Acetaldehyde adducts in alcoholic liver disease. Oxid. Med. Cell Longev. 2010, 3, 178–185. [Google Scholar] [CrossRef]
- Poustchi, H.; Sepanlou, S.; Esmaili, S.; Mehrabi, N.; Ansarymoghadam, A. Hepatocellular carcinoma in the world and the middle East. Middle East J. Dig. Dis. 2010, 2, 31–41. [Google Scholar]
- Tateishi, R.; Uchino, K.; Fujiwara, N.; Takehara, T.; Okanoue, T.; Seike, M.; Yoshiji, H.; Yatsuhashi, H.; Shimizu, M.; Torimura, T.; et al. A nationwide survey on non-B, non-C hepatocellular carcinoma in Japan: 2011–2015 update. J. Gastroenterol. 2019, 54, 367–376. [Google Scholar] [CrossRef]
- Observation, G.H. Patterns of Drinking Score-By Country. 2014. Available online: http://apps.who.int/gho/data/node.main.A1048?lang=en?showonly=GISAH (accessed on 1 September 2022).
- Rehm, J.; Samokhvalov, A.V.; Shield, K.D. Global burden of alcoholic liver diseases. J. Hepatol. 2013, 59, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Rehm, J.; Rehn, N.; Room, R.; Monteiro, M.; Gmel, G.; Jernigan, D.; Frick, U. The global distribution of average volume of alcohol consumption and patterns of drinking. Eur. Addict. Res. 2003, 9, 147–156. [Google Scholar] [CrossRef] [Green Version]
- Obsearvatory, G.H. Estimate of 5-Year Change in Recorded Alcohol per Capita (15+ Years) Consumption, 2006–2010. 2014. Available online: http://www.who.int/gho/alcohol/consumption_levels/change_adult_percapita/en/ (accessed on 1 September 2022).
- Wong, M.C.S.; Huang, J.L.W.; George, J.; Huang, J.; Leung, C.; Eslam, M.; Chan, H.L.Y.; Ng, S.C. The changing epidemiology of liver diseases in the Asia-Pacific region. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 57–73. [Google Scholar] [CrossRef]
- Mak, L.Y.; Cruz-Ramon, V.; Chinchilla-Lopez, P.; Torres, H.A.; LoConte, N.K.; Rice, J.P.; Foxhall, L.E.; Sturgis, E.M.; Merrill, J.K.; Bailey, H.H.; et al. Global Epidemiology, Prevention, and Management of Hepatocellular Carcinoma. Am. Soc. Clin. Oncol. Educ. Book 2018, 38, 262–279. [Google Scholar] [CrossRef]
- WHO. Immunization, Vaccines and Biologicals: Hepatitis B. 2017. Available online: www.who.int/immunization/diseases/hepatitisB/en/ (accessed on 1 September 2022).
- Lee, C.; Gong, Y.; Brok, J.; Boxall, E.H.; Gluud, C. Effect of hepatitis B immunisation in newborn infants of mothers positive for hepatitis B surface antigen: Systematic review and meta-analysis. BMJ 2006, 332, 328–336. [Google Scholar] [CrossRef]
- Varbobitis, I.; Papatheodoridis, G.V. The assessment of hepatocellular carcinoma risk in patients with chronic hepatitis B under antiviral therapy. Clin. Mol. Hepatol. 2016, 22, 319–326. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Recommendations for prevention and control of hepatitis C virus (HCV) infection and HCV-related chronic disease. MMWR Recomm. Rep. 1998, 47, 1–39. [Google Scholar]
- AASLD-IDSA. When and in Whom to Initiate HCV Therapy. 2017. Available online: http://www.hcvguidelines.org/evaluate/when-whom (accessed on 1 September 2022).
- Esposito, K.; Chiodini, P.; Colao, A.; Lenzi, A.; Giugliano, D. Metabolic syndrome and risk of cancer: A systematic review and meta-analysis. Diabetes Care 2012, 35, 2402–2411. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef]
- Bruix, J.; Sherman, M.; American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma: An update. Hepatology 2011, 53, 1020–1022. [Google Scholar] [CrossRef]
- Degasperi, E.; Colombo, M. Distinctive features of hepatocellular carcinoma in non-alcoholic fatty liver disease. Lancet Gastroenterol. Hepatol. 2016, 1, 156–164. [Google Scholar] [CrossRef]
- Konyn, P.; Ahmed, A.; Kim, D. Current epidemiology in hepatocellular carcinoma. Expert Rev. Gastroenterol. Hepatol. 2021, 15, 1295–1307. [Google Scholar] [CrossRef]
- Piguet, A.C.; Saran, U.; Simillion, C.; Keller, I.; Terracciano, L.; Reeves, H.L.; Dufour, J.F. Regular exercise decreases liver tumors development in hepatocyte-specific PTEN-deficient mice independently of steatosis. J. Hepatol. 2015, 62, 1296–1303. [Google Scholar] [CrossRef] [Green Version]
- Baumeister, S.E.; Leitzmann, M.F.; Linseisen, J.; Schlesinger, S. Physical Activity and the Risk of Liver Cancer: A Systematic Review and Meta-Analysis of Prospective Studies and a Bias Analysis. J. Natl. Cancer Inst. 2019, 111, 1142–1151. [Google Scholar] [CrossRef]
- Zhang, W.; Xiang, Y.B.; Li, H.L.; Yang, G.; Cai, H.; Ji, B.T.; Gao, Y.T.; Zheng, W.; Shu, X.O. Vegetable-based dietary pattern and liver cancer risk: Results from the Shanghai women’s and men’s health studies. Cancer Sci. 2013, 104, 1353–1361. [Google Scholar] [CrossRef]
- Kurahashi, N.; Inoue, M.; Iwasaki, M.; Tanaka, Y.; Mizokami, M.; Tsugane, S.; Group, J.S. Vegetable, fruit and antioxidant nutrient consumption and subsequent risk of hepatocellular carcinoma: A prospective cohort study in Japan. Br. J. Cancer 2009, 100, 181–184. [Google Scholar] [CrossRef] [PubMed]
- Montella, M.; Crispo, A.; Giudice, A. HCC, diet and metabolic factors: Diet and HCC. Hepat. Mon. 2011, 11, 159–162. [Google Scholar]
- Turati, F.; Trichopoulos, D.; Polesel, J.; Bravi, F.; Rossi, M.; Talamini, R.; Franceschi, S.; Montella, M.; Trichopoulou, A.; La Vecchia, C.; et al. Mediterranean diet and hepatocellular carcinoma. J. Hepatol. 2014, 60, 606–611. [Google Scholar] [CrossRef]
- Yang, J.D.; Hainaut, P.; Gores, G.J.; Amadou, A.; Plymoth, A.; Roberts, L.R. A global view of hepatocellular carcinoma: Trends, risk, prevention and management. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 589–604. [Google Scholar] [CrossRef]
- Goh, G.B.; Chang, P.E.; Tan, C.K. Changing epidemiology of hepatocellular carcinoma in Asia. Best Pract. Res. Clin. Gastroenterol. 2015, 29, 919–928. [Google Scholar] [CrossRef] [PubMed]
- World Cancer Research Fund. Diet, Nutrition, Physical Activity and Liver Cancer. 2015. Available online: https://www.wcrf.org/wp-content/uploads/2021/02/liver-cancer-report.pdf (accessed on 1 September 2022).
- Jafri, W.; Kamran, M. Hepatocellular Carcinoma in Asia: A Challenging Situation. Euroasian J. Hepatogastroenterol. 2019, 9, 27–33. [Google Scholar] [CrossRef]
- Omata, M.; Cheng, A.L.; Kokudo, N.; Kudo, M.; Lee, J.M.; Jia, J.; Tateishi, R.; Han, K.H.; Chawla, Y.K.; Shiina, S.; et al. Asia-Pacific clinical practice guidelines on the management of hepatocellular carcinoma: A 2017 update. Hepatol. Int. 2017, 11, 317–370. [Google Scholar] [CrossRef]
- Wilhelm, S.M.; Dumas, J.; Adnane, L.; Lynch, M.; Carter, C.A.; Schutz, G.; Thierauch, K.H.; Zopf, D. Regorafenib (BAY 73-4506): A new oral multikinase inhibitor of angiogenic, stromal and oncogenic receptor tyrosine kinases with potent preclinical antitumor activity. Int. J. Cancer 2011, 129, 245–255. [Google Scholar] [CrossRef]
- Topalian, S.L.; Hodi, F.S.; Brahmer, J.R.; Gettinger, S.N.; Smith, D.C.; McDermott, D.F.; Powderly, J.D.; Carvajal, R.D.; Sosman, J.A.; Atkins, M.B.; et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N. Engl. J. Med. 2012, 366, 2443–2454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hodi, F.S.; O’Day, S.J.; McDermott, D.F.; Weber, R.W.; Sosman, J.A.; Haanen, J.B.; Gonzalez, R.; Robert, C.; Schadendorf, D.; Hassel, J.C.; et al. Improved survival with ipilimumab in patients with metastatic melanoma. N. Engl. J. Med. 2010, 363, 711–723. [Google Scholar] [CrossRef]
- Singal, A.G.; Lampertico, P.; Nahon, P. Epidemiology and surveillance for hepatocellular carcinoma: New trends. J. Hepatol. 2020, 72, 250–261. [Google Scholar] [CrossRef] [PubMed]
- Bosetti, C.; Turati, F.; La Vecchia, C. Hepatocellular carcinoma epidemiology. Best Pract. Res. Clin. Gastroenterol. 2014, 28, 753–770. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population | Annual Population | Number of New Cases | Change in Number of Cases | ||
|---|---|---|---|---|---|
| 2020 | 2040 | 2020 | 2040 | ||
| Afghanistan | 38,928,341 | 56,912,008 | 956 | 2024 | +111.7% |
| Armenia | 2,963,234 | 2,905,147 | 427 | 599 | +40.3% |
| Azerbaijan | 10,139,175 | 11,055,063 | 510 | 914 | +79.2% |
| Bahrain | 1,701,583 | 2,199,706 | 36 | 109 | +202.8% |
| Bangladesh | 164,689,383 | 188,416,728 | 3261 | 5928 | +81.8% |
| Bhutan | 771,612 | 885,158 | 34 | 61 | +79.4% |
| Brunei Darussalam | 437,483 | 488,817 | 43 | 108 | +151.2% |
| Cambodia | 16,718,971 | 20,526,539 | 3142 | 5999 | +90.9% |
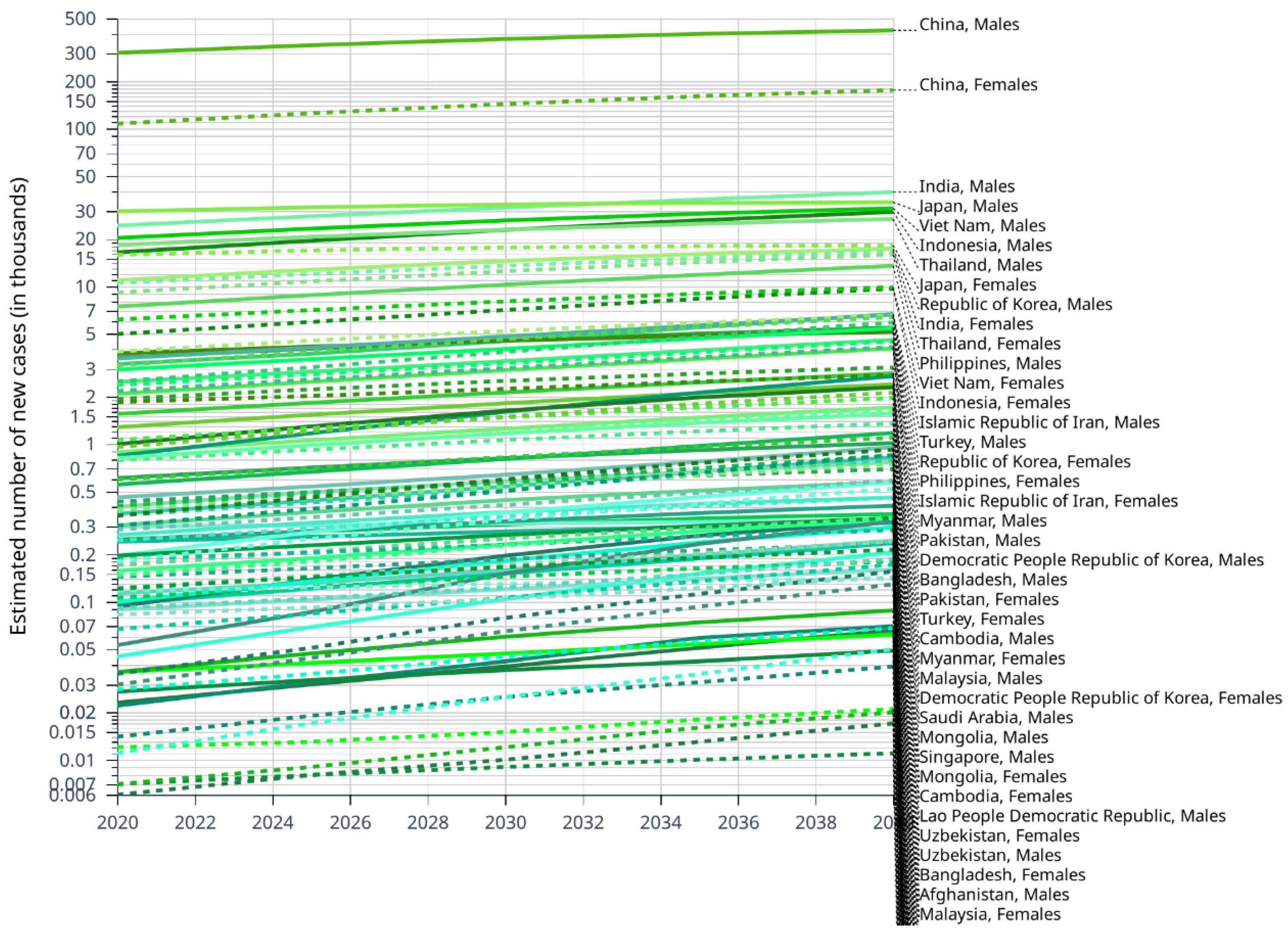
| China | 1,447,470,092 | 1,457,962,454 | 410,038 | 595,242 | +45.2% |
| Democratic People Republic of Korea | 25,778,815 | 26,858,031 | 5607 | 7882 | +40.6% |
| Georgia | 3,989,175 | 3,689,311 | 418 | 463 | +10.8% |
| India | 1,380,004,391 | 1,592,691,531 | 34,743 | 56,309 | +62.1% |
| Indonesia | 273,523,621 | 318,637,860 | 21,392 | 39,273 | +83.6% |
| Iraq | 40,222,503 | 60,583,717 | 713 | 1604 | +125.0% |
| Islamic Republic of Iran | 83,992,953 | 98,593,610 | 5701 | 12,581 | +120.7% |
| Israel | 8,655,541 | 11,332,909 | 388 | 640 | +64.9% |
| Japan | 126,476,458 | 113,356,481 | 45,663 | 52,218 | +14.4% |
| Jordan | 10,203,140 | 11,886,728 | 204 | 430 | +110.8% |
| Kazakhstan | 18,776,707 | 22,370,403 | 1039 | 1707 | +64.3% |
| Kuwait | 4,270,563 | 5,152,526 | 128 | 482 | +276.6% |
| Kyrgyzstan | 6,524,191 | 8,307,138 | 476 | 911 | +91.4% |
| Lao People Democratic Republic | 7,275,556 | 8,971,941 | 1272 | 2453 | +92.8% |
| Lebanon | 6,825,442 | 6,376,397 | 172 | 302 | +75.6% |
| Malaysia | 32,365,998 | 38,754,576 | 2149 | 3906 | +81.8% |
| Maldives | 540,542 | 556,282 | 29 | 83 | +186.2% |
| Mongolia | 3,278,292 | 4,089,199 | 2236 | 4506 | +101.5% |
| Myanmar | 54,409,794 | 61,201,610 | 5466 | 8529 | +56.0% |
| Nepal | 29,136,808 | 34,889,298 | 524 | 1007 | +92.2% |
| Oman | 5,106,622 | 64,37,413 | 128 | 364 | +184.4% |
| Pakistan | 220,892,331 | 302,129,186 | 5331 | 9901 | +85.7% |
| Palestine | 5,101,416 | 7,599,231 | 164 | 407 | +148.2% |
| Philippines | 109,581,085 | 135,618,864 | 10,594 | 19,882 | +87.7% |
| Qatar | 2,881,060 | 3,628,689 | 56 | 256 | +357.1% |
| Republic of Korea | 51,269,183 | 49,783,741 | 14,788 | 23,763 | +60.7% |
| Saudi Arabia | 34,813,867 | 42,473,029 | 1145 | 3542 | +209.3% |
| Singapore | 5,850,343 | 6,445,489 | 1347 | 3213 | +138.5% |
| Sri Lanka | 21,413,250 | 22,186,243 | 354 | 540 | +52.5% |
| Syrian Arab Republic | 17,500,657 | 30,153,278 | 376 | 1093 | +190.7% |
| Tajikistan | 9,537,642 | 13,845,878 | 304 | 676 | +122.4% |
| Thailand | 69,799,978 | 69,008,295 | 27,394 | 42,614 | +55.6% |
| Timor-Leste | 1,318,442 | 1,809,281 | 48 | 83 | +72.9% |
| Turkey | 84,339,067 | 94,131,585 | 5649 | 10,733 | +90.0% |
| Turkmenistan | 6,031,187 | 7,408,523 | 317 | 554 | +74.8% |
| United Arab Emirates | 9,890,400 | 10,648,314 | 83 | 452 | +444.6% |
| Uzbekistan | 33,469,199 | 40,608,381 | 1629 | 3223 | +97.9% |
| Viet Nam | 97,338,583 | 107,795,035 | 26,418 | 41,124 | +55.7% |
| Yemen | 29,825,968 | 42,670,023 | 745 | 1541 | +106.8% |
| Totals | 4,616,030,644 | 5,164,031,646 | 643,637 | 970,231 | +50.7% |
| Regions | Main Factor | Trends of HCC |
|---|---|---|
| Singapore | HBV | Male incidence decreased from 27.4 cases per 100,000 population in 1973–1977 to 17.2 cases in 2008–2012; Female incidence decreased from 6.9 cases per 100,000 population in 1973–1977 to 4.8. |
| Taiwan | HBV | The mortality rate decreased from 0·81 deaths per 100,000 to 0·05 per 100,000. |
| Hong Kong | HBV | The incidence has declined over the past 25 years. |
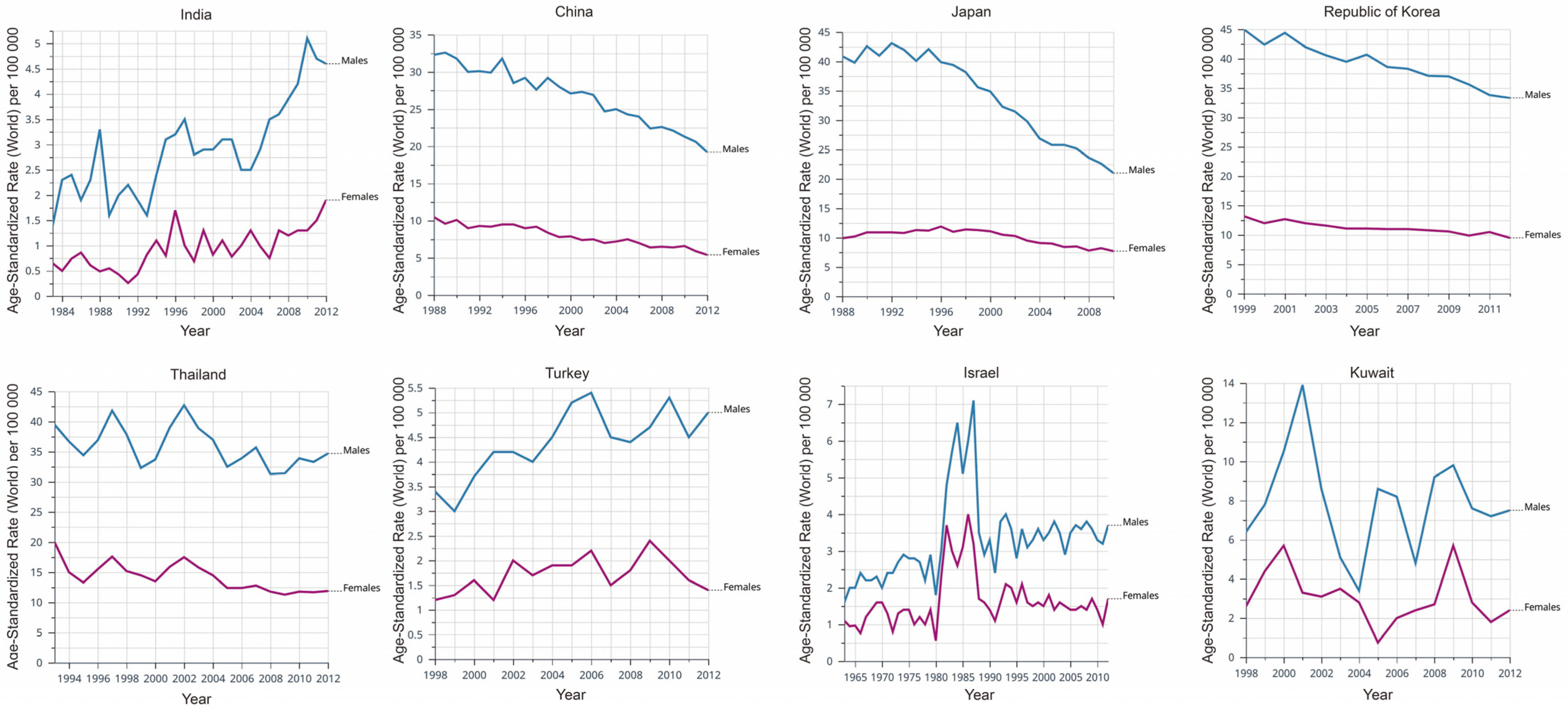
| Japan | HCV | The incidence and death have increased exponentially since 1970 and peaked in the early 2000s. After a plateau in 2002–2004, the number of deaths began to decline, reaching 28,889 in 2015. |
| India | HBV | The incidence has increased over the past two decades. |
| China | NAFLD | The incidence increased from 3.8% in 2001−2005 to 12.2% in 2006–2010. |
| Korea | NAFLD | The incidence increased from 3.8% in 2001−2005 to 12.2% in 2006–2010 |
| Philippines | Aflatoxin | The incidence of HCC was reduced. |
| Qidong | Aflatoxin | A significant decrease in the incidence of HCC in men (ASR = 89.9 from 1983 to 1987, ASR = 60.9 from 2008 to 2012, −32.3%) and a slight decrease in women (ASR = 24.5 from 1983 to 1987, ASR = 21.5 from 2008 to 2012, −12.2%) were observed. |
| Asia-Pacific region | Alcohol | The increase in alcohol intake across the Asia-Pacific region between 2006 and 2016 May have contributed to an increase in age-standardized liver cancer rates. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, Y.; Liu, L. Changes in the Epidemiology of Hepatocellular Carcinoma in Asia. Cancers 2022, 14, 4473. https://doi.org/10.3390/cancers14184473
Liu Y, Liu L. Changes in the Epidemiology of Hepatocellular Carcinoma in Asia. Cancers. 2022; 14(18):4473. https://doi.org/10.3390/cancers14184473
Chicago/Turabian StyleLiu, Yao, and Lianxin Liu. 2022. "Changes in the Epidemiology of Hepatocellular Carcinoma in Asia" Cancers 14, no. 18: 4473. https://doi.org/10.3390/cancers14184473
APA StyleLiu, Y., & Liu, L. (2022). Changes in the Epidemiology of Hepatocellular Carcinoma in Asia. Cancers, 14(18), 4473. https://doi.org/10.3390/cancers14184473