
Meta-Analysis of Repeat Hepatectomy versus Radiofrequency Ablation for Recurrence of Hepatocellular Carcinoma

 ,
,  ,
,  ,
,  and
and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
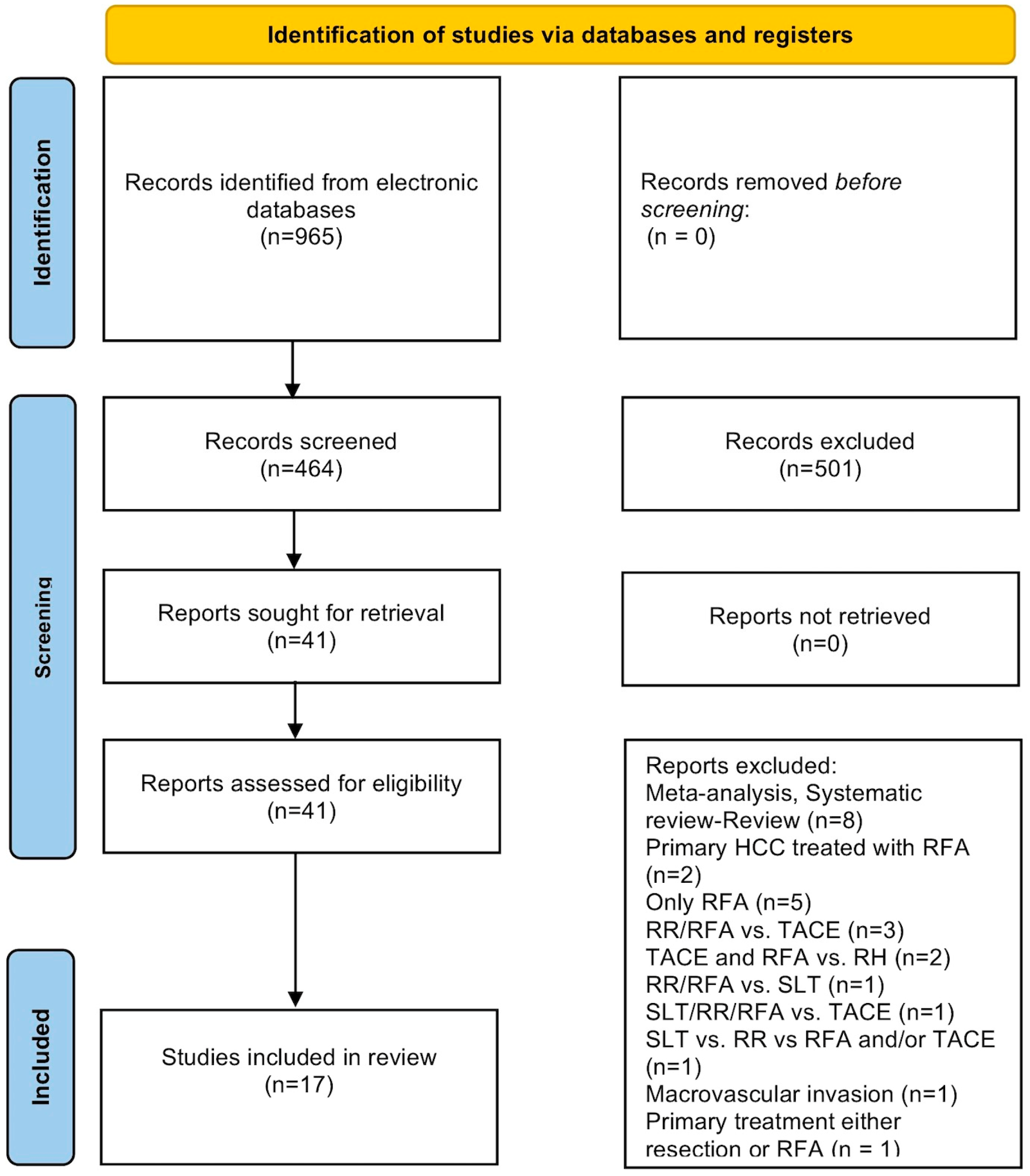
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Outcomes of Interest
2.4. Risk of Bias Assessment
2.5. Statistical Analysis
3. Results
3.1. Critical Appraisal and Risk of Bias Assessment
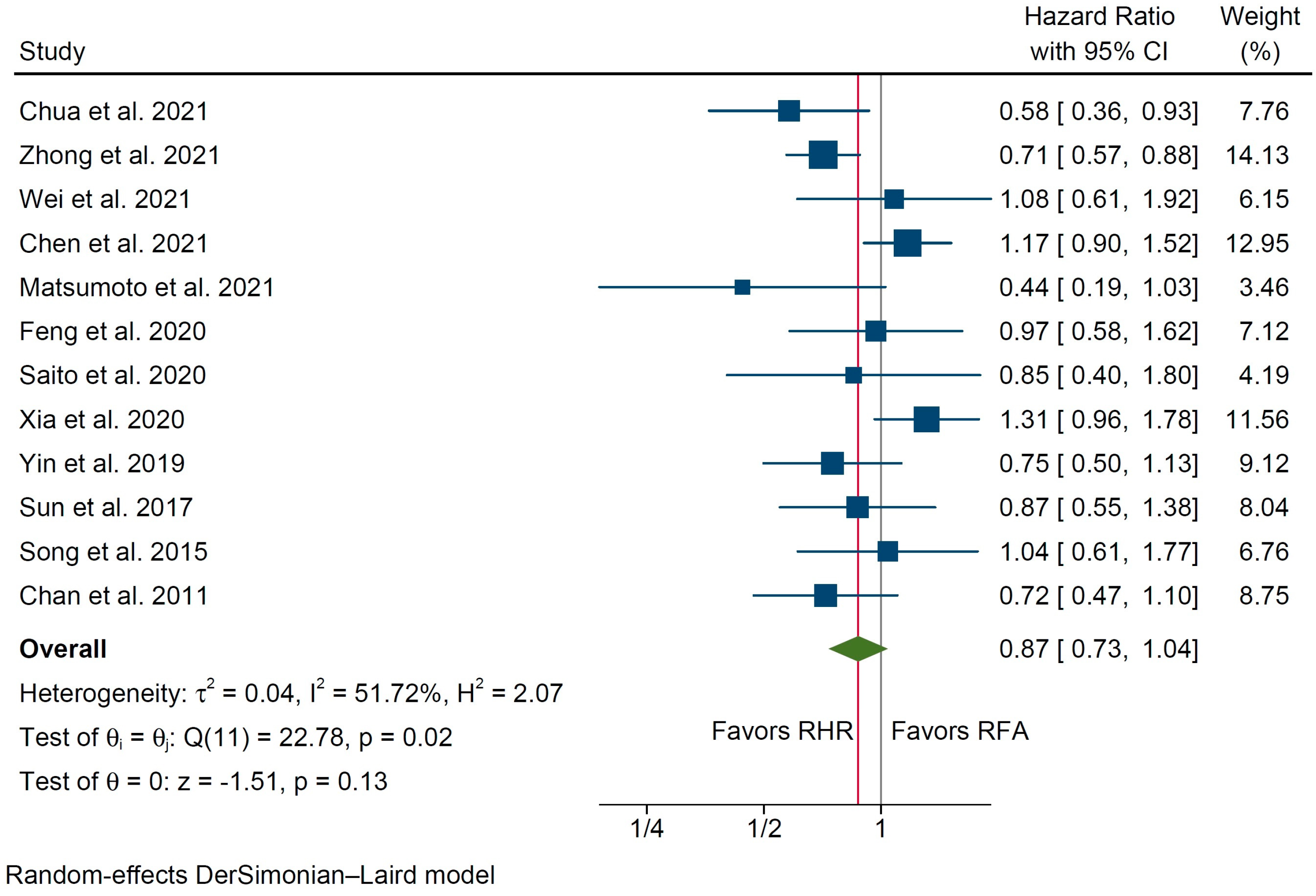
3.2. Primary Outcomes
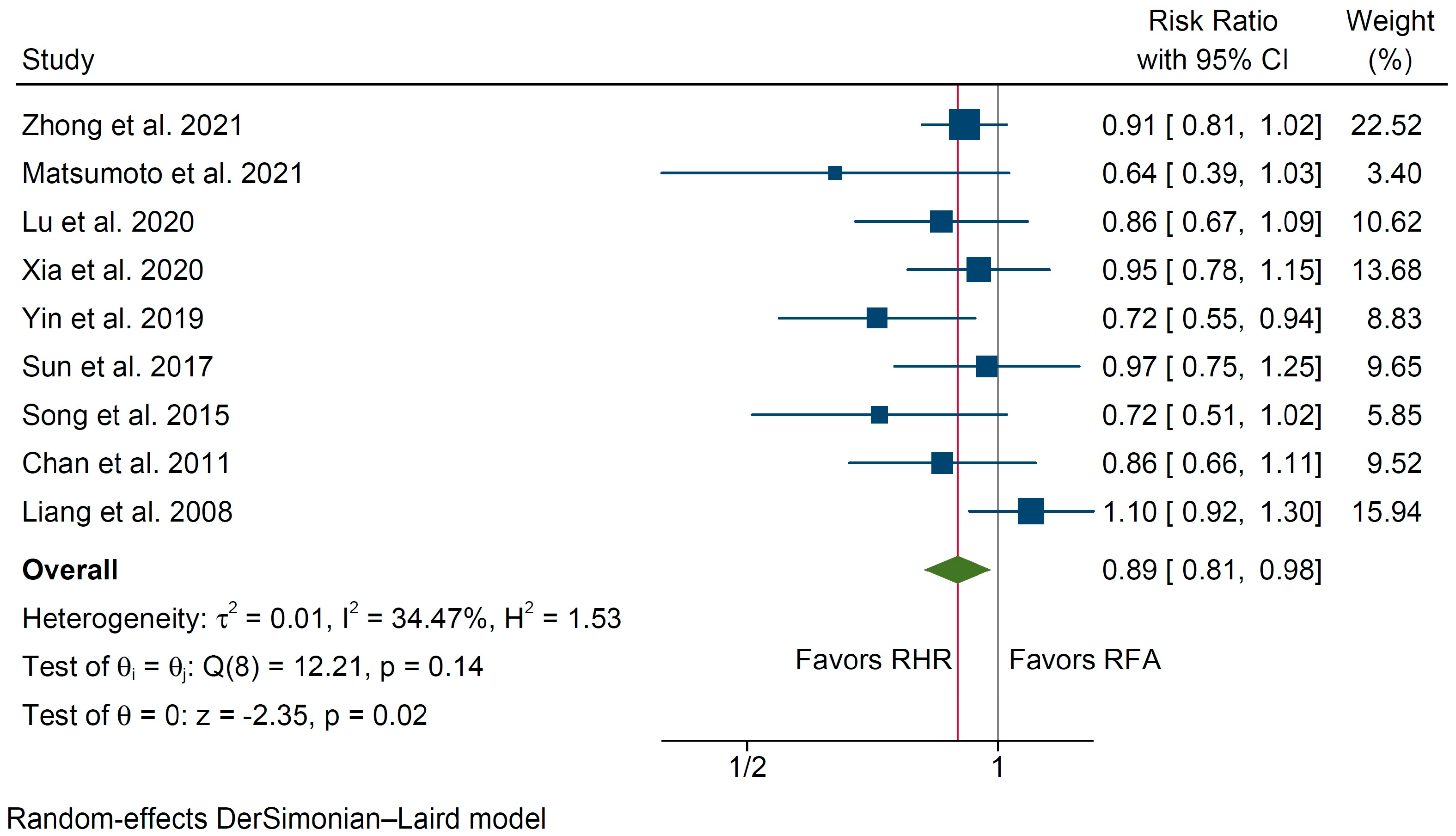
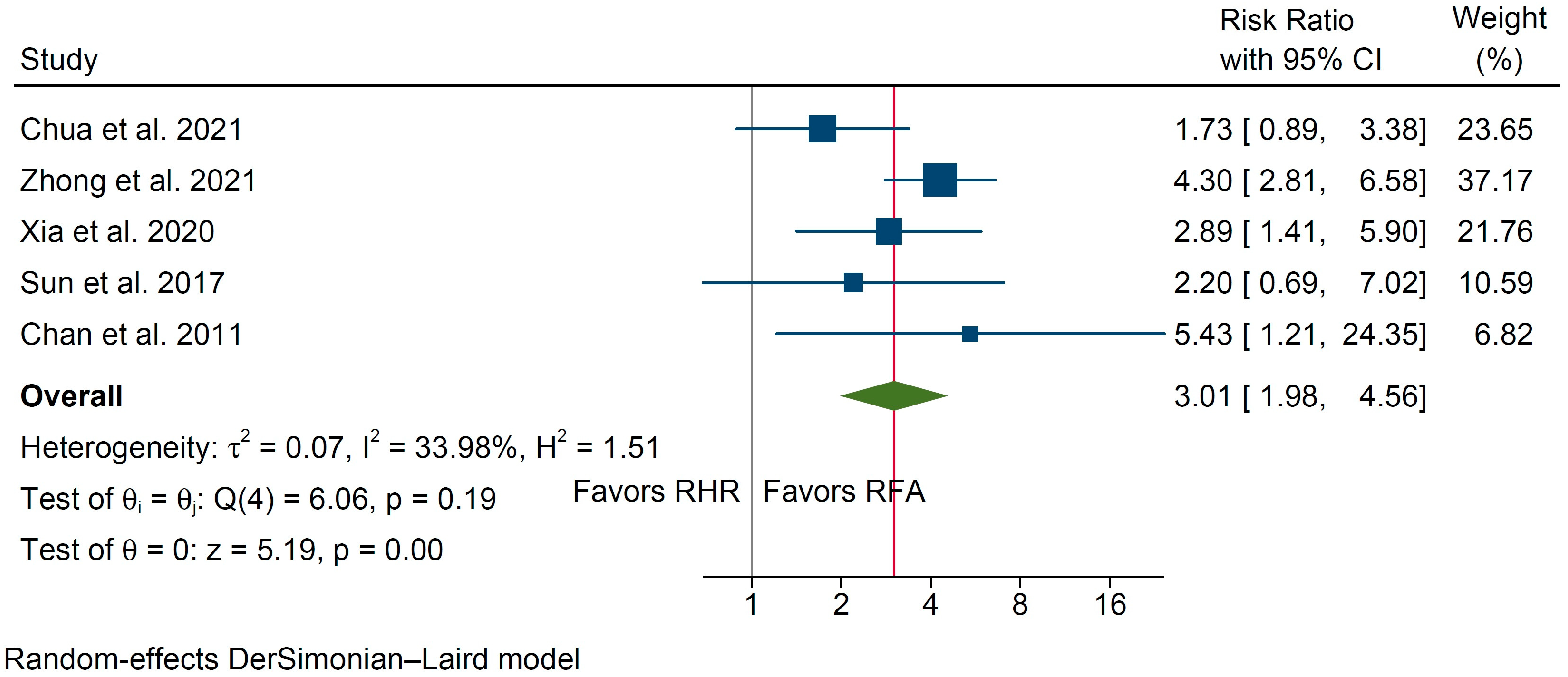
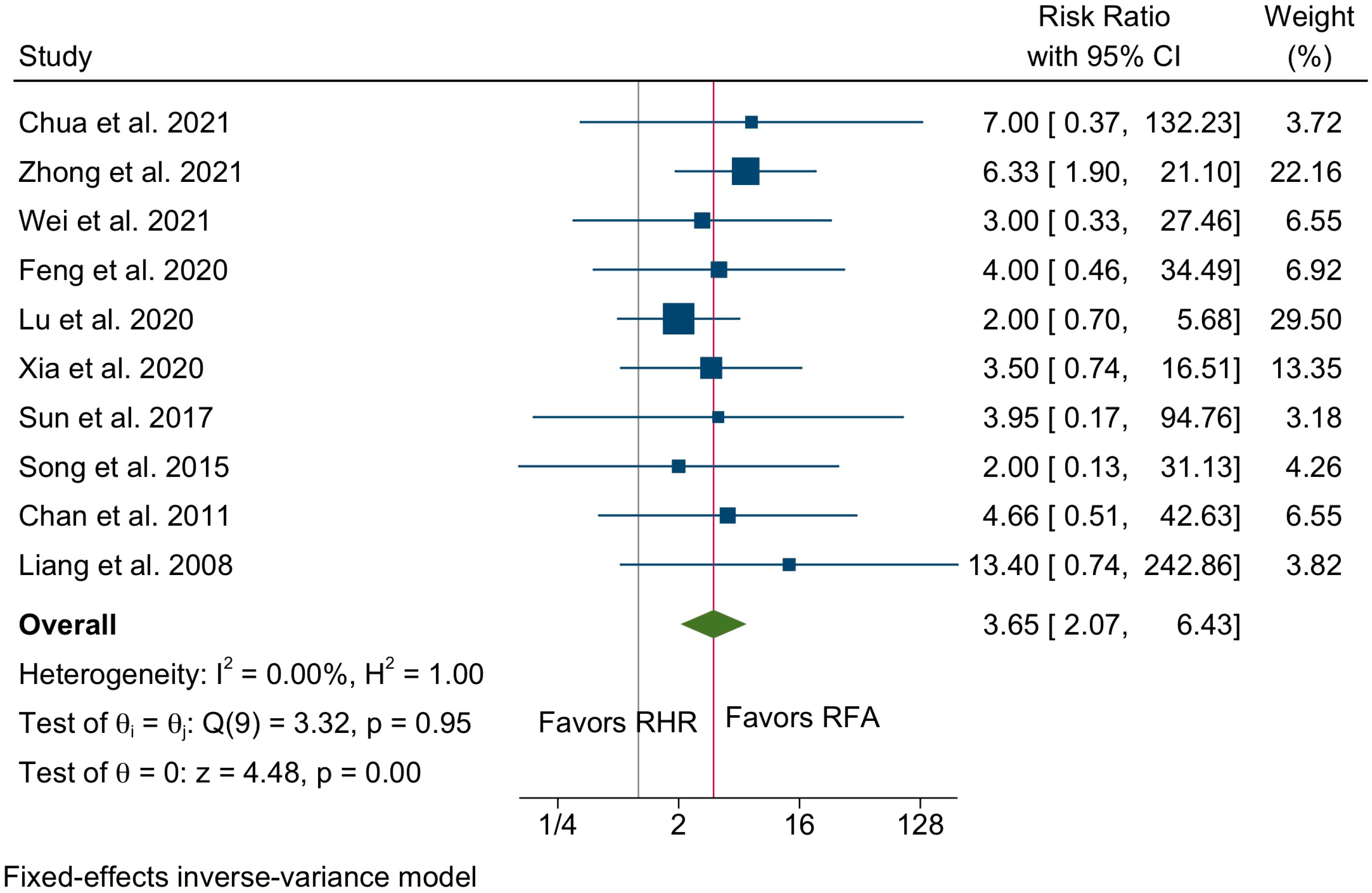
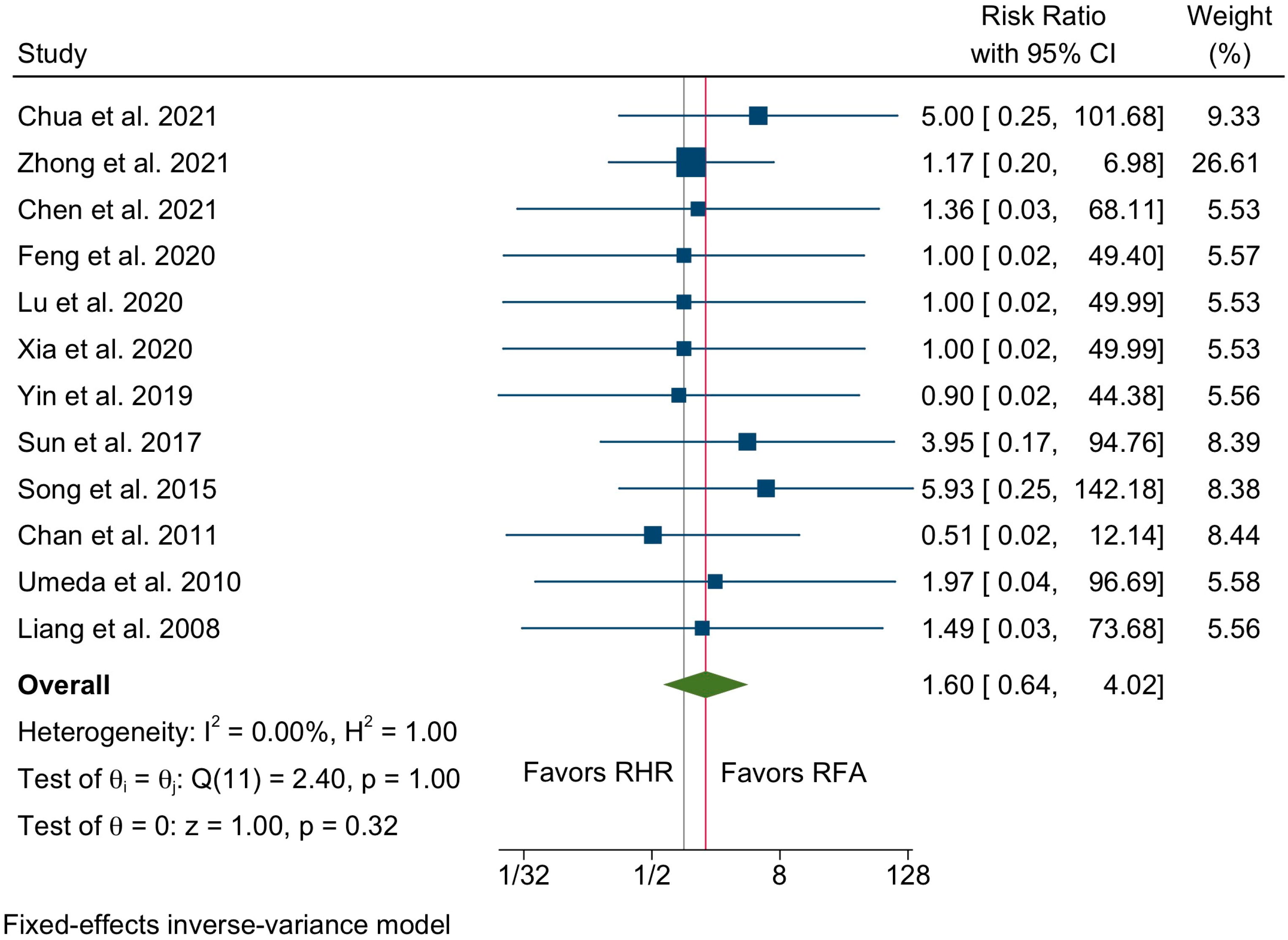
3.3. Secondary Outcomes
3.4. Subgroup Analysis
3.5. Level of Evidence
3.6. Publication Bias Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Machairas, N.; Tsilimigras, D.I.; Pawlik, T.M. Current Landscape of Immune Checkpoint Inhibitor Therapy for Hepatocellular Carcinoma. Cancers 2022, 14, 2018. [Google Scholar] [CrossRef] [PubMed]
- Villanueva, A. Hepatocellular Carcinoma. N. Engl. J. Med. 2019, 380, 1450–1462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ganne-Carrie, N.; Nahon, P. Hepatocellular carcinoma in the setting of alcohol-related liver disease. J. Hepatol. 2019, 70, 284–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Younossi, Z.M.; Henry, L. Epidemiology of non-alcoholic fatty liver disease and hepatocellular carcinoma. JHEP Rep. 2021, 3, 100305. [Google Scholar] [CrossRef]
- Forner, A.; Reig, M.; Bruix, J. Hepatocellular carcinoma. Lancet 2018, 391, 1301–1314. [Google Scholar] [CrossRef]
- Kotsifa, E.; Vergadis, C.; Vailas, M.; Machairas, N.; Kykalos, S.; Damaskos, C.; Garmpis, N.; Lianos, G.D.; Schizas, D. Transarterial Chemoembolization for Hepatocellular Carcinoma: Why, when, how? J. Pers. Med. 2022, 12, 436. [Google Scholar] [CrossRef]
- Machairas, N.; Tsilimigras, D.I.; Pawlik, T.M. State-of-the-art surgery for hepatocellular carcinoma. Langenbecks Arch. Surg. 2021, 406, 2151–2162. [Google Scholar] [CrossRef]
- Tsilimigras, D.I.; Bagante, F.; Moris, D.; Merath, K.; Paredes, A.Z.; Sahara, K.; Ratti, F.; Marques, H.P.; Soubrane, O.; Lam, V.; et al. Defining the chance of cure after resection for hepatocellular carcinoma within and beyond the Barcelona Clinic Liver Cancer guidelines: A multi-institutional analysis of 1010 patients. Surgery 2019, 166, 967–974. [Google Scholar] [CrossRef]
- Tsilimigras, D.I.; Bagante, F.; Sahara, K.; Moris, D.; Hyer, J.M.; Wu, L.; Ratti, F.; Marques, H.P.; Soubrane, O.; Paredes, A.Z.; et al. Prognosis After Resection of Barcelona Clinic Liver Cancer (BCLC) Stage 0, A, and B Hepatocellular Carcinoma: A Comprehensive Assessment of the Current BCLC Classification. Ann. Surg. Oncol. 2019, 26, 3693–3700. [Google Scholar] [CrossRef]
- Sotiropoulos, G.C.; Malago, M.; Machairas, N.; Fouzas, I.; Paul, A. AGMA Score: A Novel Prognostic Score for Patients Undergoing Liver Transplant for Hepatocellular Carcinoma. Transpl. Proc. 2019, 51, 1923–1925. [Google Scholar] [CrossRef] [PubMed]
- Sotiropoulos, G.C.; Spartalis, E.; Machairas, N.; Paul, A.; Malago, M.; Neuhauser, M. Liver transplantation for hepatocellular carcinoma with live donors or extended criteria donors: A propensity score-matched comparison. Ann. Gastroenterol. 2018, 31, 722–727. [Google Scholar] [CrossRef] [PubMed]
- Sotiropoulos, G.C.; Prodromidou, A.; Machairas, N. Meta-analysis of laparoscopic vs. open liver resection for hepatocellular carcinoma: The European experience. J. BUON 2017, 22, 1160–1171. [Google Scholar] [PubMed]
- European Association for the Study of the Liver. Electronic address eee, European Association for the Study of the L. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [Green Version]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef] [Green Version]
- Kostakis, I.D.; Machairas, N.; Prodromidou, A.; Stamopoulos, P.; Garoufalia, Z.; Fouzas, I.; Sotiropoulos, G.C. Comparison Between Salvage Liver Transplantation and Repeat Liver Resection for Recurrent Hepatocellular Carcinoma: A Systematic Review and Meta-analysis. Transpl. Proc. 2019, 51, 433–436. [Google Scholar] [CrossRef]
- Machairas, N.; Papaconstantinou, D.; Stamopoulos, P.; Prodromidou, A.; Garoufalia, Z.; Spartalis, E.; Kostakis, I.D.; Sotiropoulos, G.C. The Emerging Role of Laparoscopic Liver Resection in the Treatment of Recurrent Hepatocellular Carcinoma: A Systematic Review. Anticancer Res. 2018, 38, 3181–3186. [Google Scholar]
- Minagawa, M.; Makuuchi, M.; Takayama, T.; Kokudo, N. Selection criteria for repeat hepatectomy in patients with recurrent hepatocellular carcinoma. Ann. Surg. 2003, 238, 703–710. [Google Scholar] [CrossRef]
- Lau, W.Y.; Lai, E.C. The current role of radiofrequency ablation in the management of hepatocellular carcinoma: A systematic review. Ann. Surg. 2009, 249, 20–25. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann. Intern Med. 2009, 151, W65–W94. [Google Scholar] [CrossRef] [Green Version]
- Guyot, P.; Ades, A.E.; Ouwens, M.J.; Welton, N.J. Enhanced secondary analysis of survival data: Reconstructing the data from published Kaplan-Meier survival curves. BMC Med. Res. Methodol. 2012, 12, 9. [Google Scholar] [CrossRef]
- Chua, D.W.; Koh, Y.X.; Syn, N.L.; Chuan, T.Y.; Yao, T.J.; Lee, S.Y.; Goh, B.K.P.; Cheow, P.C.; Chung, A.Y.; Chan, C.Y. Repeat hepatectomy versus radiofrequency ablation in management of recurrent hepatocellular carcinoma: An average treatment effect analysis. Ann. Surg. Oncol. 2021, 28, 7731–7740. [Google Scholar] [CrossRef] [PubMed]
- Zhong, J.H.; Xing, B.C.; Zhang, W.G.; Chan, A.W.; Chong, C.C.N.; Serenari, M.; Peng, N.; Huang, T.; Lu, S.D.; Liang, Z.Y.; et al. Repeat hepatic resection versus radiofrequency ablation for recurrent hepatocellular carcinoma: Retrospective multicentre study. Br. J. Surg. 2021, 109, 71–78. [Google Scholar] [CrossRef]
- Wei, F.; Huang, Q.; Zhou, Y.; Luo, L.; Zeng, Y. Radiofrequency ablation versus repeat hepatectomy in the treatment of recurrent hepatocellular carcinoma in subcapsular location: A retrospective cohort study. World J. Surg. Oncol. 2021, 19, 175. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.Y.; Guo, Z.X.; Lu, L.H.; Mei, J.; Lin, W.P.; Li, S.H.; Wei, W.; Guo, R.P. The predictive value of vessels encapsulating tumor clusters in treatment optimization for recurrent early-stage hepatocellular carcinoma. Cancer Med. 2021, 10, 5466–5474. [Google Scholar] [CrossRef]
- Matsumoto, M.; Yanaga, K.; Shiba, H.; Wakiyama, S.; Sakamoto, T.; Futagawa, Y.; Gocho, T.; Ishida, Y.; Ikegami, T. Treatment of intrahepatic recurrence after hepatectomy for hepatocellular carcinoma. Ann. Gastroenterol. Surg. 2021, 5, 538–552. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Wu, H.; Huang, D.Q.; Xu, C.; Zheng, H.; Maeda, M.; Zhao, X.; Wang, L.; Xiao, F.; Lv, H.; et al. Radiofrequency ablation versus repeat resection for recurrent hepatocellular carcinoma (≤5 cm) after initial curative resection. Eur. Radiol. 2020, 30, 6357–6368. [Google Scholar] [CrossRef] [PubMed]
- Saito, R.; Amemiya, H.; Hosomura, N.; Kawaida, H.; Maruyama, S.; Shimizu, H.; Furuya, S.; Akaike, H.; Kawaguchi, Y.; Sudo, M.; et al. Prognostic Significance of Treatment Strategies for the Recurrent Hepatocellular Carcinomas After Radical Resection. Vivo 2020, 34, 1265–1270. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.H.; Mei, J.; Kan, A.; Ling, Y.H.; Li, S.H.; Wei, W.; Chen, M.S.; Zhang, Y.F.; Guo, R.P. Treatment optimization for recurrent hepatocellular carcinoma: Repeat hepatic resection versus radiofrequency ablation. Cancer Med. 2020, 9, 2997–3005. [Google Scholar] [CrossRef]
- Xia, Y.; Li, J.; Liu, G.; Wang, K.; Qian, G.; Lu, Z.; Yang, T.; Yan, Z.; Lei, Z.; Si, A.; et al. Long-term Effects of Repeat Hepatectomy vs. Percutaneous Radiofrequency Ablation Among Patients with Recurrent Hepatocellular Carcinoma: A Randomized Clinical Trial. JAMA Oncol. 2020, 6, 255–263. [Google Scholar] [CrossRef]
- Yin, X.; Hua, T.; Liang, C.; Chen, Z. Efficacy of re-resection versus radiofrequency ablation for recurrent Barcelona Clinic Liver Cancer stage 0/A hepatocellular carcinoma (HCC) after resection for primary HCC. Transl. Cancer Res. 2019, 8, 1035–1045. [Google Scholar] [CrossRef]
- Sun, W.C.; Chen, I.S.; Liang, H.L.; Tsai, C.C.; Chen, Y.C.; Wang, B.W.; Lin, H.S.; Chan, H.H.; Hsu, P.I.; Tsai, W.L.; et al. Comparison of repeated surgical resection and radiofrequency ablation for small recurrent hepatocellular carcinoma after primary resection. Oncotarget 2017, 8, 104571–104581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, K.; Liu, G.; Li, J.; Yan, Z.; Xia, Y.; Wan, X.; Ji, Y.; Lau, W.Y.; Wu, M.; Shen, F. Early intrahepatic recurrence of hepatocellular carcinoma after hepatectomy treated with re-hepatectomy, ablation or chemoembolization: A prospective cohort study. Eur. J. Surg. Oncol. 2015, 41, 236–242. [Google Scholar] [CrossRef]
- Song, K.D.; Lim, H.K.; Rhim, H.; Lee, M.W.; Kim, Y.S.; Lee, W.J.; Paik, Y.H.; Gwak, G.Y.; Kim, J.M.; Kwon, C.H.; et al. Repeated Hepatic Resection versus Radiofrequency Ablation for Recurrent Hepatocellular Carcinoma after Hepatic Resection: A Propensity Score Matching Study. Radiology 2015, 275, 599–608. [Google Scholar] [CrossRef]
- Ho, C.M.; Lee, P.H.; Shau, W.Y.; Ho, M.C.; Wu, Y.M.; Hu, R.H. Survival in patients with recurrent hepatocellular carcinoma after primary hepatectomy: Comparative effectiveness of treatment modalities. Surgery 2012, 151, 700–709. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.C.; Poon, R.T.; Cheung, T.T.; Chok, K.S.; Chan, S.C.; Fan, S.T.; Lo, C.M. Survival analysis of re-resection versus radiofrequency ablation for intrahepatic recurrence after hepatectomy for hepatocellular carcinoma. World J. Surg. 2012, 36, 151–156. [Google Scholar] [CrossRef] [Green Version]
- Umeda, Y.; Matsuda, H.; Sadamori, H.; Matsukawa, H.; Yagi, T.; Fujiwara, T. A prognostic model and treatment strategy for intrahepatic recurrence of hepatocellular carcinoma after curative resection. World J. Surg. 2011, 35, 170–177. [Google Scholar] [CrossRef]
- Liang, H.H.; Chen, M.S.; Peng, Z.W.; Zhang, Y.J.; Zhang, Y.Q.; Li, J.Q.; Lau, W.Y. Percutaneous radiofrequency ablation versus repeat hepatectomy for recurrent hepatocellular carcinoma: A retrospective study. Ann. Surg. Oncol. 2008, 15, 3484–3493. [Google Scholar] [CrossRef]
- Xu, X.F.; Xing, H.; Han, J.; Li, Z.L.; Lau, W.Y.; Zhou, Y.H.; Gu, W.M.; Wang, H.; Chen, T.H.; Zeng, Y.Y.; et al. Risk Factors, Patterns, and Outcomes of Late Recurrence After Liver Resection for Hepatocellular Carcinoma: A Multicenter Study from China. JAMA Surg. 2019, 154, 209–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imamura, H.; Matsuyama, Y.; Tanaka, E.; Ohkubo, T.; Hasegawa, K.; Miyagawa, S.; Sugawara, Y.; Minagawa, M.; Takayama, T.; Kawasaki, S.; et al. Risk factors contributing to early and late phase intrahepatic recurrence of hepatocellular carcinoma after hepatectomy. J. Hepatol. 2003, 38, 200–207. [Google Scholar] [CrossRef]
- Zheng, J.; Chou, J.F.; Gonen, M.; Vachharajani, N.; Chapman, W.C.; Majella Doyle, M.B.; Turcotte, S.; Vandenbroucke-Menu, F.; Lapointe, R.; Buettner, S.; et al. Prediction of Hepatocellular Carcinoma Recurrence Beyond Milan Criteria After Resection: Validation of a Clinical Risk Score in an International Cohort. Ann. Surg. 2017, 266, 693–701. [Google Scholar] [CrossRef] [PubMed]
- Machairas, N.; Tsilimigras, D.I.; Moris, D. CD24 as a Novel Predictive Biomarker in Patients with Hepatocellular Carcinoma: Friend or Foe? J. Investig. Surg. 2020, 33, 542–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsiao, C.Y.; Hu, R.H.; Ho, C.M.; Wu, Y.M.; Lee, P.H.; Ho, M.C. Surgical resection versus radiofrequency ablation for Barcelona Clinic Liver Cancer very early stage hepatocellular carcinoma: Long-term results of a single-center study. Am. J. Surg. 2020, 220, 958–964. [Google Scholar] [CrossRef]
- Chen, J.; Peng, K.; Hu, D.; Shen, J.; Zhou, Z.; Xu, L.; Chen, J.; Pan, Y.; Wang, J.; Zhang, Y.; et al. Tumor Location Influences Oncologic Outcomes of Hepatocellular Carcinoma Patients Undergoing Radiofrequency Ablation. Cancers 2018, 10, 378. [Google Scholar] [CrossRef] [Green Version]
- Cai, H.; Kong, W.; Zhou, T.; Qiu, Y. Radiofrequency ablation versus reresection in treating recurrent hepatocellular carcinoma: A meta-analysis. Medicine 2014, 93, e122. [Google Scholar] [CrossRef] [PubMed]
- Gavriilidis, P.; Askari, A.; Azoulay, D. Survival following redo hepatectomy vs. radiofrequency ablation for recurrent hepatocellular carcinoma: A systematic review and meta-analysis. HPB 2017, 19, 3–9. [Google Scholar] [CrossRef] [Green Version]
- Eisele, R.M.; Chopra, S.S.; Lock, J.F.; Glanemann, M. Treatment of recurrent hepatocellular carcinoma confined to the liver with repeated resection and radiofrequency ablation: A single center experience. Technol. Health Care 2013, 21, 9–18. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author; Year | Country | Type of Study | n Patients | Age | Sex (F) (%) |
|---|---|---|---|---|---|
| Chua; 2021 [22] | Singapore | Retrospective, PSM | 52 vs. 52 | 63.5 (56.5–71.0) * vs. 62.5 (56.5–66) * | 45 (92.6) vs. 46 (88.5) |
| Zhong; 2021 [23] | China | Retrospective, PSM | 227 vs. 227 | N/a | 33 (14.6) vs. 36 (15.9) |
| Wei; 2021 [24] | China | Retrospective, PSM | 35 vs. 35 | N/a | 4 (11.4) vs. 4 (11.4) |
| Chen; 2021 [25] | China | Retrospective | 138 vs. 138 | 50.7 ± 10.5 vs. 49.2 ± 10.9 | 13 (9.4) vs. 16 (8.5) |
| Matsumoto; 2021 [26] | Japan | Retrospective | 23 vs. 11 | 66 (55–84) * vs. 67 (42–79) | 3 (13.1) vs. 0 (0) |
| Feng; 2020 [27] | Multicenter | Retrospective, PSM | 48 vs. 48 | 56.6 ± 9.2 vs. 58.2 ± 7.5 | 7 (4.6) vs. 6 (2.5) |
| Saito; 2020 [28] | Japan | Retrospective | 17 vs. 26 | N/a | N/a |
| Lu; 2020 [29] | China | Retrospective, PSM | 120 vs. 120 | 50.9 ± 11.6 vs. 50.3 ± 10.3 | 16 (3.4) vs. 12 (10) |
| Xia; 2020 [30] | China | RCT | 120 vs. 120 | 50 (24–58) * vs. 52 (25–59) * | 13 (10.9) vs. 11 (9.2) |
| Yin; 2019 [31] | China | Retrospective | 57 vs. 51 | 57 ± 12 vs. 60.26 ± 9.5 | 16 (28.1) vs. 20 (39.2) |
| Sun; 2017 [32] | Taiwan | Retrospective | 43 vs. 57 | 60 (35–76) * vs. 63 (27–81) * | 9 (21) vs. 19 (33.4) |
| Wang; 2015 [33] | China | Prospective | 128 vs. 162 | 50.2 ± 10.1 vs. 51 ± 10.1 | 15 (11.8) vs. 14 (8.7) |
| Song; 2015 [34] | Korea | Retrospective, PSM | 39 vs. 78 | 52.5 ± 9.8 vs. 53.6 ± 10.9 | 8 (20.5) vs. 20 (25.7) |
| Ho; 2012 [35] | Taiwan | Retrospective | 54 vs. 50 | 56.3 ± 12.3 vs. 61 ± 11.1 | 14 (25.9) vs. 11 (22) |
| Chan; 2011 [36] | China | Prospective | 29 vs. 45 | 52 (38–79) * vs. 59 (36–80) * | N/a |
| Umeda; 2010 [37] | Japan | Retrospective | 29 vs. 58 | 64.8 ± 0.79 | N/a |
| Liang; 2008 [38] | China | Retrospective | 44 vs. 66 | 48.8 ± 12.0 vs. 54.6 ± 10.8 | 5 (11.4) vs. 12 (18.2) |
| Author; Year | CTP A/B | Single Nodule | Tumor Size (cm) | AFP (ng/mL) | HBV Infection | Vascular Involvement |
|---|---|---|---|---|---|---|
| RHR vs. RFA, n (%) | ||||||
| Chua; 2021 [22] | 45 (90)/7(10) vs. 49 (96)/2 (4) | 38 (74.5) vs. 43 (82.7) | 3.0 (2.0–4.5) vs. 2.9 (2.0–4.0) * | 12 (5–42) vs. 14(4–75) * | 31 (63.3%) vs. 41 (80.4%) | 5 (9.6%) vs. 9 (18%) |
| Zhong; 2021 [23] | 222 (97.8)/5 (2.2) vs. 224 (98.7)/3 (1.3) | 171 (75.3) vs. 172 (75.7) | ≥3 cm; 99 (43.6) vs. 92(40.5) <3 cm; 128 (56.4) vs. 135 (59.5) | ≥200; 45 (19.8) vs. 46 (20.2) <200; 182 (80.2) vs. 181 (79.7) | 193 (85) vs. 192 (84.5) | N/a |
| Wei; 2021 [24] | 35 (100)/0 vs. 35 (100)/0 | 24(68.6%) vs. 30(85.7%) | ≥3 cm; 3 (8.6) vs. 2 (5.7) <3 cm; 32 (91.4) vs. 3 (94.3) | ≥200; 12 (34.3) vs. 7 (2) <200; 23 (65.7) vs. 28 (80) | N/a | N/a |
| Chen; 2021 [25] | N/a | 119 (86.2) vs. 148 (78.7) | 2.4 ± 0.5 vs. 2.2 ± 0.4 | >20; 91 (65.9) vs. 127 (67.5) ≤20; 47 (34.1) vs. 61(32.5) | 117 (84.7) vs. 145 (77.1) | 32 (23.2) vs. 59 (31.4) |
| Matsumoto; 2021 [26] | 22 (95.6)/1 (4.4) vs. 9 (81.8)/2 (18.2) | 19 vs. 8 | 3.2 (0.9–10.5) vs. 2 (1.5–9.6) | N/a | 7 (30.4) vs. 2 (18.1) | N/a |
| Feng; 2020 [27] | 45 (93.8)/3 (6.2) vs. 41 (85.4)/7 (4.6) | 37 (77) vs. 34 (70.8) | 2.5 (2–3) vs. 2.5 (2–3.3) * | 13.1 (2.8–133.1) vs. 6.1 (2.4–182.1) * | 48 (100) vs. 48 (100) | N/a |
| Saito; 2020 [28] | N/a | N/a | N/a | N/a | N/a | N/a |
| Lu; 2020 [29] | 120 (100)/0 vs. 120 (100)/0 | 106 (88.3) vs. 106 (88.3) | 2.2 ± 1 vs. 2.4 ± 1.1 | >20; 50 (41.6) vs. 45 (37.5) ≤20; 70 (58.4) vs. 75 (62.5) | 108 (90) vs. 112 (93.3) | N/a |
| Xia; 2020 [30] | 120 (100)/0 vs. 120 (100)/0 | 99 (82.5) vs. 93 (77.5) | 4 (1–5) vs. 4 (1.1–11.2) * | >200; 70 (58.3) vs. 73 (60.8) ≤200; 50 (41.7) vs. 47 (39.2) | 98 (81.6) vs. 91 (75.8) | 38 (31.6) vs. 35 (29.1) |
| Yin; 2019 [31] | 55 (96.5)/2 (3.5) vs. 46 (90.1)/5 (9.9) | 52 (91.2) vs. 48 (94.1) | 3.2 ± 2.5 vs. 2.6 ± 0.9 | 167.9 ± 357.2 vs. 266.3 ± 420.2 | 53 (92.9) vs. 48 (94.1) | N/a |
| Sun; 2017 [32] | 35 (97.2)/1 (2.8) vs. 50 (100)/0 | N/a | 3.9 (1.0–16.0) vs. 3.9 (1.3–15.0) * | 602 (1–11681) vs. 1090 (3–29141) | 21 (48.8) vs. 32 (56.1) | 8 (18.6) vs. 7 (12.3) |
| Wang; 2015 [33] | N/a | 89 (69.5) vs. 107 (66) | 2.4 ± 0.9 vs. 2.3 ± 0.7 | >20; 56 (43.7) vs. 77 (47.5) ≤20; 72 (56.3) vs. 85 (52.5) | 119 (92.9) vs. 142 (87.6) | 23 (17.9) vs. 0 |
| Song; 2015 [34] | 39 (100)/0 vs. 78 (100)/0 | 32 (82) vs. 65 (83.3) | >2 cm; 17 (43.6) vs. 31 (39.7) ≤2 cm; 22 (56.4) vs. 57 (60.3) | >200; 6 (15.4) vs. 9 (11.5) ≤200; 33 (84.6) vs. 69 (88.5) | 36 (92.3) vs. 70 (89.7) | 15 (38.5) vs. 27 (34.6) |
| Ho; 2012 [35] | 51 (94.4)/2 (3.7) vs. 50 (100)/0 | N/a | 2.9 ± 1.8 vs. 2.3 ± 1.9 | >400; 10 (18.5) vs. 7 (14) | 39 (72.2) vs. 27 (54) | 4 (7) vs. 0 |
| Chan; 2011 [36] | 29 (100)/0 vs. 40 (88.8)/5 (11.2) | N/a | 3.5 (1.0–14.5) vs. 5.5 (1.5–22.0) * | 64 (2–167,138) vs. 90 (1–197,122) * | 26 (89.6) vs. 40 (88.8) | N/a |
| Umeda; 2010 [37] | 28 (96.5)/1 (3.5) vs. 54 (93.1)/4 (6.9) | 18 (62) vs. 34 (58.6) | 4.3 ± 0.55 vs. 3.2 ± 0.39 | ≥100; 7 (34.2) vs. 9 (15.5) <100; 22 (75.8) vs. 49 (84.5) | 8 (27.5) vs. 11 (18.9) | 9 (31) vs. 18 (31) |
| Liang; 2008 [38] | 44 (100)/0 vs. 64 (96.9)/2 (3.1) | 34 (77.2) vs. 48 (72.7) | ≤3 cm; 26 vs. 44 >3 cm; 18 vs. 22 | ≤400; 30 (59) vs. 52 (78.8) >400; 14 (41) vs. 14 (21.2) | 41 (93.2) vs. 60 (90.9) | N/a |
| Author; Year | 3-Year OS | 5-Year OS | 3-Year DFS | 5-Year DFS | Second Recurrence | Morbidity | CD ≥ III Morbidity | Mortality |
|---|---|---|---|---|---|---|---|---|
| RHR vs. RFA, n (%) | ||||||||
| Chua; 2021 [22] | 72.5% vs. 62.6% | 71.3% vs. 65.7% | N/a | 63.2% vs. 78.9% | N/a | 18 (34.6) vs. 10 (20) | 3 (6) vs. 0 | 2 (3.8) vs. 0 |
| Zhong; 2021 [23] | 67.4% vs. 71.3% | 56.4% vs. 53.1% | 37.5% vs. 28.1% | 25.5% vs. 16% | 155 (68.2) vs. 170 (74.8) | 66 (21.5) vs. 27 (5) | 19 (6.2) vs. 3 (0.5) | 2 (0.6) vs. 3 (0.5) |
| Wei; 2021 [24] | 59% vs. 71.4% | N/a | 32.3% vs. 34% | N/a | N/a | N/a | 3 (8.6) vs. 1 (2.9) | N/a |
| Chen; 2021 [25] | N/a | N/a | N/a | N/a | N/a | N/a | N/a | None |
| Matsumoto; 2021 [26] | 89.% vs. 74% | 84.9% vs. 74% | 43.4% vs. 15.4% | 43.4% vs. 0 | 12 (52.2) vs. 9 (81.8) | N/a | N/a | N/a |
| Feng; 2020 [27] | 70.3% vs. 67% | 38.7% vs. 60.3% | 25.9% vs. 32.8% | 21.6% vs. 9.8% | N/a | N/a | 4 (8.3) vs. 1 (2) | None |
| Lu; 2020 [29] | 81.5% vs. 61% | 71.8% vs. 41.7% | N/a | N/a | 59 (49.1) vs. 69 (57.5) | N/a | 10 (8.3) vs. 5 (4.1) | None |
| Xia; 2020 [30] | 65.8% vs. 52.5% | 43.6% vs. 38.5% | 52.4% vs. 41.7% | 36.2% vs. 30.2% | 73 (60.8) vs. 77 (64.2) | 26 (21.6) vs. 9 (7.5) | 7 (5.8) vs. 2 (1.6) | None |
| Yin; 2019 [31] | 50.5% vs. 50.9% | 29.7% vs. 26% | 39.4% vs. 32.8% | 26.6% vs. 20.4% | 32 (56.1) vs. 40 (78.4) | N/a | N/a | None |
| Sun; 2017 [32] | 82.7% vs. 77.2% | 56.4% vs. 52.6% | 32.1% vs. 26.6% | 28.6% vs. 16.6% | 30 (69.7) vs. 41 (71.9) | 7 (16.3) vs. 4 (7) | 1 (2.3) vs. 0 | 1 (2.3) vs. 0 |
| Wang; 2015 [33] | 84.1% vs. 73.4% | 64.5% vs. 37% | N/a | N/a | N/a | N/a | N/a | N/a |
| Song; 2015 [34] | 88.8% vs. 85.7% | 83.9% vs. 72.1% | 48.5% vs. 45.1% | 43.1% vs. 39.4% | 18 (47.3) vs. 117 (65.7) | N/a | 1 (2.5) vs. 1 (1.2) | 1 (2.5) vs. 0 |
| Ho; 2012 [35] | N/a | 72% vs. 83% | N/a | N/a | N/a | N/a | N/a | N/a |
| Chan; 2011 [36] | 56.5% vs. 68.2 | 35.2% vs. 44.5% | 24.2% vs. 12.4% | 24.2% vs. 9.3% | 21 (72.4) vs. 38 (84.4) | 7 (24.1) vs. 2 (4.4) | 3 (10.3) vs. 1 (2.2) | 0 vs. 1 (2.2) |
| Umeda; 2010 [37] | 66.8% vs. 75.1% | 56.1% vs. 48.3% | N/a | N/a | N/a | N/a | N/a | None |
| Liang; 2008 [38] | 44.5% vs. 48.6% | 27.6% vs. 39.9% | N/a | N/a | 38 (86.3) vs. 52 (78.7) | N/a | N/a | None |
| Outcome | n Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Others | Certainty |
|---|---|---|---|---|---|---|---|---|
| Overall Survival | 17 | Observational studies, n = 16 RCT, n = 1 | Moderate | Low | Low | Moderate | None | ⊕⊕⊕☐ Moderate |
| Disease-Free Survival | 12 | Observational studies, n = 11 RCT, n = 1 | Moderate | Moderate | Low | Moderate | None | ⊕⊕☐☐ Low |
| Second Recurrence | 9 | Observational studies, n = 9 RCT, n = 1 | Moderate | Moderate | Moderate | Moderate | None | ⊕⊕☐☐ Low |
| Morbidity | 5 | Observational studies, n = 4 RCT, n = 1 | Moderate | Moderate | Moderate | Serious | None | ⊕☐☐☐ Very Low |
| Morbidity, CD≥III | 10 | Observational studies, n = 9 RCT, n = 1 | Moderate | Low | Moderate | Moderate | None | ⊕⊕☐☐ Low |
| Mortality | 12 | Observational studies, n = 11 RCT, n = 1 | Moderate | Low | Moderate | Moderate | None | ⊕⊕☐☐ Low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Machairas, N.; Papaconstantinou, D.; Dorovinis, P.; Tsilimigras, D.I.; Keramida, M.D.; Kykalos, S.; Schizas, D.; Pawlik, T.M. Meta-Analysis of Repeat Hepatectomy versus Radiofrequency Ablation for Recurrence of Hepatocellular Carcinoma. Cancers 2022, 14, 5398. https://doi.org/10.3390/cancers14215398
Machairas N, Papaconstantinou D, Dorovinis P, Tsilimigras DI, Keramida MD, Kykalos S, Schizas D, Pawlik TM. Meta-Analysis of Repeat Hepatectomy versus Radiofrequency Ablation for Recurrence of Hepatocellular Carcinoma. Cancers. 2022; 14(21):5398. https://doi.org/10.3390/cancers14215398
Chicago/Turabian StyleMachairas, Nikolaos, Dimitrios Papaconstantinou, Panagiotis Dorovinis, Diamantis I. Tsilimigras, Myrto D. Keramida, Stylianos Kykalos, Dimitrios Schizas, and Timothy M. Pawlik. 2022. "Meta-Analysis of Repeat Hepatectomy versus Radiofrequency Ablation for Recurrence of Hepatocellular Carcinoma" Cancers 14, no. 21: 5398. https://doi.org/10.3390/cancers14215398
APA StyleMachairas, N., Papaconstantinou, D., Dorovinis, P., Tsilimigras, D. I., Keramida, M. D., Kykalos, S., Schizas, D., & Pawlik, T. M. (2022). Meta-Analysis of Repeat Hepatectomy versus Radiofrequency Ablation for Recurrence of Hepatocellular Carcinoma. Cancers, 14(21), 5398. https://doi.org/10.3390/cancers14215398