
Deep Learning for the Diagnosis of Esophageal Cancer in Endoscopic Images: A Systematic Review and Meta-Analysis

 , ,
, ,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Research Design
2.2. Search Methods for Identification of Studies
Electronic Database Search
2.3. Inclusion and Exclusion Criteria
2.4. Data Extraction
2.5. Quality Assessment
2.6. Statistical Analysis
3. Results
3.1. Study Selection
3.2. Study Characteristics
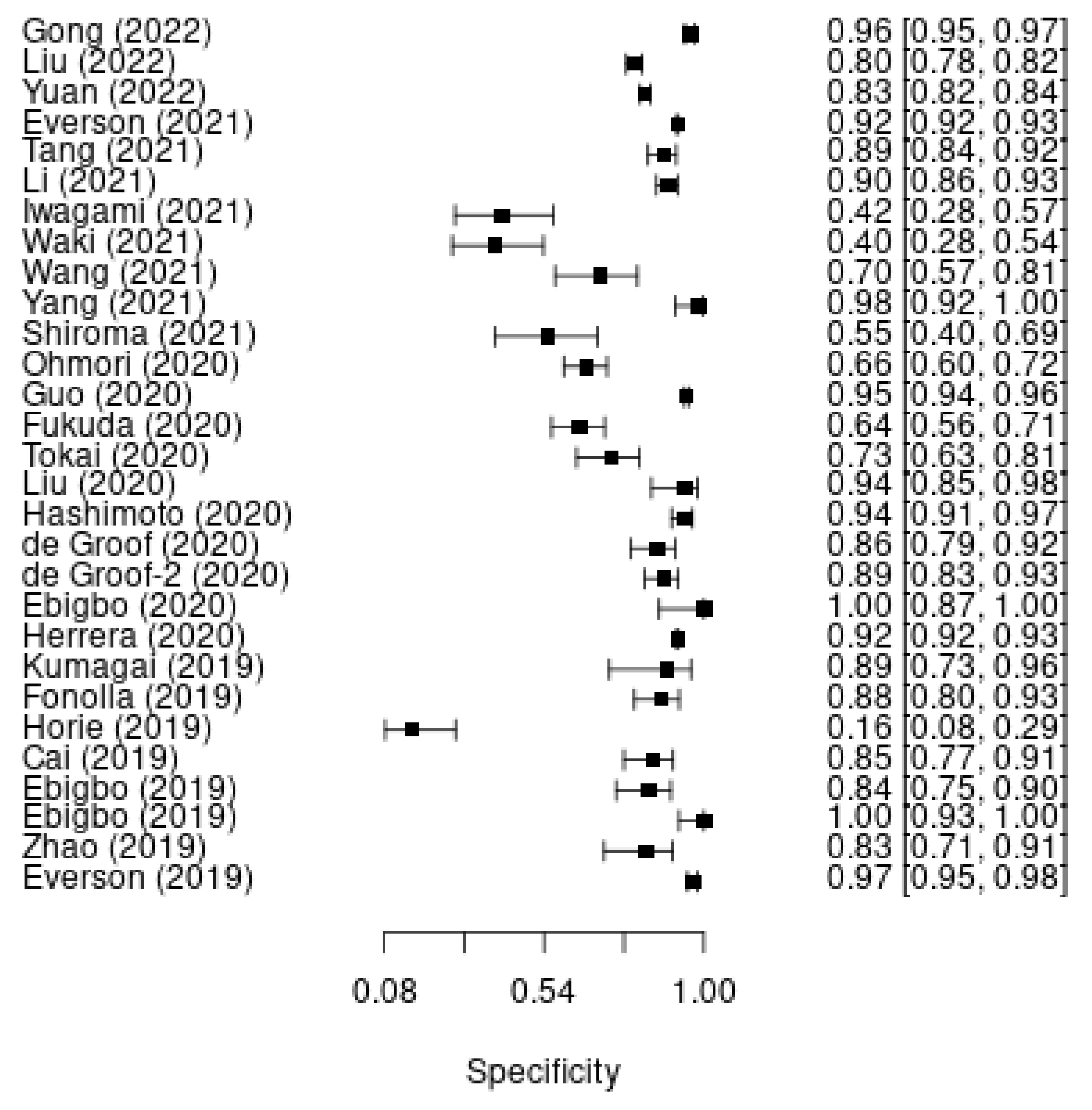
3.3. Deep Learning Model for Esophageal Cancer Diagnosis
3.4. Subgroup Analysis
3.5. External Validation
3.6. Performance Comparison between DL and Endoscopists
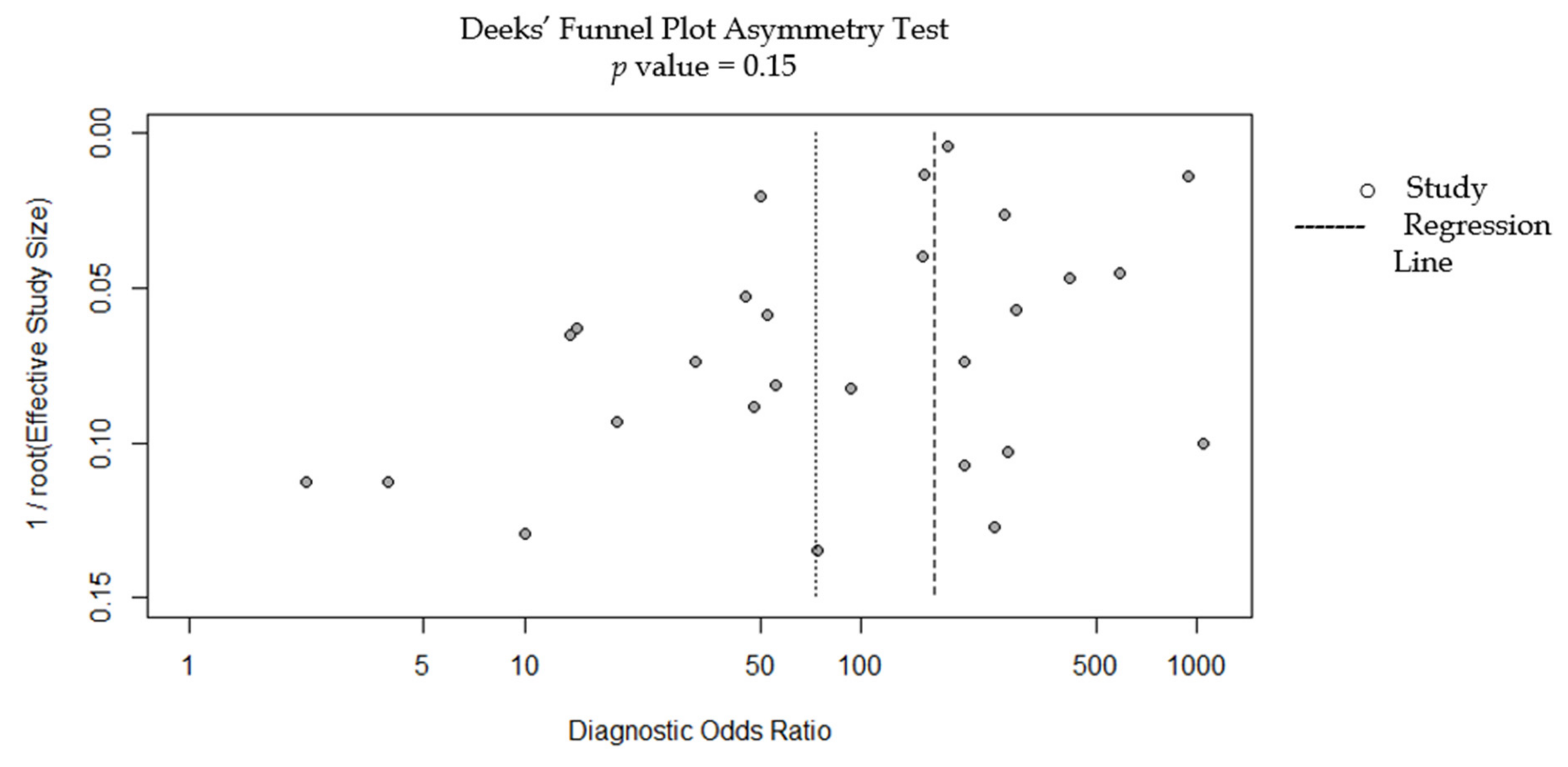
3.7. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Huang, J.; Koulaouzidis, A.; Marlicz, W.; Lok, V.; Chu, C.; Ngai, C.H.; Zhang, L.; Chen, P.; Wang, S.; Yuan, J. Global Burden, Risk Factors, and Trends of Esophageal Cancer: An Analysis of Cancer Registries from 48 Countries. Cancers 2021, 13, 141. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rock, C.L.; Thomson, C.; Gansler, T.; Gapstur, S.M.; McCullough, M.L.; Patel, A.V.; Andrews, K.S.; Bandera, E.V.; Spees, C.K.; Robien, K. American Cancer Society guideline for diet and physical activity for cancer prevention. CA Cancer J. Clin. 2020, 70, 245–271. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Zhang, S.; Li, H.; Hassan, M.O.O.; Lu, T.; Zhao, J.; Zhang, L. Lung Metastases in Newly Diagnosed Esophageal Cancer: A Population-Based Study. Front. Oncol. 2021, 11, 119. [Google Scholar] [CrossRef] [PubMed]
- Uhlenhopp, D.J.; Then, E.O.; Sunkara, T.; Gaduputi, V. Epidemiology of esophageal cancer: Update in global trends, etiology and risk factors. Clin. J. Gastroenterol. 2020, 13, 1010–1021. [Google Scholar] [CrossRef] [PubMed]
- Lepage, C.; Rachet, B.; Jooste, V.; Faivre, J.; Coleman, M.P. Continuing rapid increase in esophageal adenocarcinoma in England and Wales. Off. J. Am. Coll. Gastroenterol. 2008, 103, 2694–2699. [Google Scholar] [CrossRef]
- Ilson, D.H.; van Hillegersberg, R. Management of patients with adenocarcinoma or squamous cancer of the esophagus. Gastroenterology 2018, 154, 437–451. [Google Scholar] [CrossRef]
- Hou, H.; Meng, Z.; Zhao, X.; Ding, G.; Sun, M.; Wang, W.; Wang, Y. Survival of esophageal cancer in China: A pooled analysis on hospital-based studies from 2000 to 2018. Front. Oncol. 2019, 9, 548. [Google Scholar] [CrossRef] [Green Version]
- Qin, J.; Zhu, H.; Guo, J.; Ni, C.; Wu, P.; Xu, H.; Mao, A.; Lu, J.; Su, C.; Teng, G. Factors associated with overall survival and relief of dysphagia in advanced esophageal cancer patients after 125I seed-loaded stent placement: A multicenter retrospective analysis. Dis. Esophagus 2019, 32, doz012. [Google Scholar] [CrossRef]
- Kountouras, J.; Doulberis, M.; Papaefthymiou, A.; Polyzos, S.A.; Vardaka, E.; Tzivras, D.; Dardiotis, E.; Deretzi, G.; Giartza-Taxidou, E.; Grigoriadis, S. A perspective on risk factors for esophageal adenocarcinoma: Emphasis on Helicobacter pylori infection. Ann. N. Y. Acad. Sci. 2019, 1452, 12–17. [Google Scholar] [CrossRef]
- Kambhampati, S.; Tieu, A.H.; Luber, B.; Wang, H.; Meltzer, S.J. Risk factors for progression of Barrett’s esophagus to High Grade Dysplasia and esophageal Adenocarcinoma. Sci. Rep. 2020, 10, 4899. [Google Scholar] [CrossRef] [Green Version]
- Abnet, C.C.; Arnold, M.; Wei, W.-Q. Epidemiology of esophageal squamous cell carcinoma. Gastroenterology 2018, 154, 360–373. [Google Scholar] [CrossRef]
- Coleman, H.G.; Xie, S.-H.; Lagergren, J. The epidemiology of esophageal adenocarcinoma. Gastroenterology 2018, 154, 390–405. [Google Scholar] [CrossRef]
- Pickens, A.; Orringer, M.B. Geographical distribution and racial disparity in esophageal cancer. Ann. Thorac. Surg. 2003, 76, S1367–S1369. [Google Scholar] [CrossRef]
- Arnal, M.J.D.; Arenas, Á.F.; Arbeloa, Á.L. Esophageal cancer: Risk factors, screening and endoscopic treatment in Western and Eastern countries. World J. Gastroenterol. 2015, 21, 7933. [Google Scholar] [CrossRef]
- Minashi, K.; Nihei, K.; Mizusawa, J.; Takizawa, K.; Yano, T.; Ezoe, Y.; Tsuchida, T.; Ono, H.; Iizuka, T.; Hanaoka, N. Efficacy of endoscopic resection and selective chemoradiotherapy for stage I esophageal squamous cell carcinoma. Gastroenterology 2019, 157, 382–390.e383. [Google Scholar] [CrossRef] [Green Version]
- Defize, I.; Van Der Horst, S.; Bülbul, M.; Mohammad, N.H.; Mook, S.; Meijer, G.; Brosens, L.; Ruurda, J.; van Hillegersberg, R. Salvage robot-assisted minimally invasive esophagectomy (RAMIE) for T4b esophageal cancer after definitive chemoradiotherapy. Ann. Surg. Oncol. 2021, 28, 2730–2738. [Google Scholar] [CrossRef]
- Ebi, M.; Shimura, T.; Yamada, T.; Mizushima, T.; Itoh, K.; Tsukamoto, H.; Tsuchida, K.; Hirata, Y.; Murakami, K.; Kanie, H. Multicenter, prospective trial of white-light imaging alone versus white-light imaging followed by magnifying endoscopy with narrow-band imaging for the real-time imaging and diagnosis of invasion depth in superficial esophageal squamous cell carcinoma. Gastrointest. Endosc. 2015, 81, 1355–1361.e2. [Google Scholar] [CrossRef]
- Muto, M.; Minashi, K.; Yano, T.; Saito, Y.; Oda, I.; Nonaka, S.; Omori, T.; Sugiura, H.; Goda, K.; Kaise, M. Early detection of superficial squamous cell carcinoma in the head and neck region and esophagus by narrow band imaging: A multicenter randomized controlled trial. J. Clin. Oncol. 2010, 28, 1566. [Google Scholar] [CrossRef] [Green Version]
- Chung, C.S.; Lo, W.C.; Lee, Y.C.; Wu, M.S.; Wang, H.P.; Liao, L.J. Image-enhanced endoscopy for detection of second primary neoplasm in patients with esophageal and head and neck cancer: A systematic review and meta-analysis. Head Neck 2016, 38, E2343–E2349. [Google Scholar] [CrossRef]
- Ishihara, R.; Takeuchi, Y.; Chatani, R.; Kidu, T.; Inoue, T.; Hanaoka, N.; Yamamoto, S.; Higashino, K.; Uedo, N.; Iishi, H. Prospective evaluation of narrow-band imaging endoscopy for screening of esophageal squamous mucosal high-grade neoplasia in experienced and less experienced endoscopists. Dis. Esophagus 2010, 23, 480–486. [Google Scholar] [CrossRef]
- Horie, Y.; Yoshio, T.; Aoyama, K.; Yoshimizu, S.; Horiuchi, Y.; Ishiyama, A.; Hirasawa, T.; Tsuchida, T.; Ozawa, T.; Ishihara, S. Diagnostic outcomes of esophageal cancer by artificial intelligence using convolutional neural networks. Gastrointest. Endosc. 2019, 89, 25–32. [Google Scholar] [CrossRef]
- McInnes, M.D.; Moher, D.; Thombs, B.D.; McGrath, T.A.; Bossuyt, P.M.; Clifford, T.; Cohen, J.F.; Deeks, J.J.; Gatsonis, C.; Hooft, L. Preferred reporting items for a systematic review and meta-analysis of diagnostic test accuracy studies: The PRISMA-DTA statement. JAMA 2018, 319, 388–396. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Suh, C.H.; Park, S.H. Successful publication of systematic review and meta-analysis of studies evaluating diagnostic test accuracy. Korean J. Radiol. 2016, 17, 5–6. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.W.; Lee, J.; Choi, S.H.; Huh, J.; Park, S.H. Systematic review and meta-analysis of studies evaluating diagnostic test accuracy: A practical review for clinical researchers-part I. General guidance and tips. Korean J. Radiol. 2015, 16, 1175–1187. [Google Scholar] [CrossRef] [Green Version]
- Reitsma, J.B.; Glas, A.S.; Rutjes, A.W.; Scholten, R.J.; Bossuyt, P.M.; Zwinderman, A.H. Bivariate analysis of sensitivity and specificity produces informative summary measures in diagnostic reviews. J. Clin. Epidemiol. 2005, 58, 982–990. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.M.; Yang, H.-C.; Poly, T.N.; Jian, W.-S.; Li, Y.-C.J. Deep learning algorithms for detection of diabetic retinopathy in retinal fundus photographs: A systematic review and meta-analysis. Comput. Methods Programs Biomed. 2020, 191, 105320. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.; Poly, T.N.; Walther, B.A.; Yang, H.C.; Li, Y.-C.J. Artificial intelligence in ophthalmology: A meta-analysis of deep learning models for retinal vessels segmentation. J. Clin. Med. 2020, 9, 1018. [Google Scholar] [CrossRef] [PubMed]
- Gong, E.J.; Bang, C.S.; Jung, K.; Kim, S.J.; Kim, J.W.; Seo, S.I.; Lee, U.; Maeng, Y.B.; Lee, Y.J.; Lee, J.I. Deep-Learning for the Diagnosis of Esophageal Cancers and Precursor Lesions in Endoscopic Images: A Model Establishment and Nationwide Multicenter Performance Verification Study. J. Pers. Med. 2022, 12, 1052. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Yuan, X.; Guo, L.; Pan, F.; Wu, C.; Sun, Z.; Tian, F.; Yuan, C.; Zhang, W.; Bai, S. Artificial Intelligence for Detecting and Delineating Margins of Early ESCC Under WLI Endoscopy. Clin. Transl. Gastroenterol. 2022, 13, e00433. [Google Scholar] [CrossRef] [PubMed]
- Yuan, X.L.; Guo, L.J.; Liu, W.; Zeng, X.H.; Mou, Y.; Bai, S.; Pan, Z.G.; Zhang, T.; Pu, W.F.; Wen, C. Artificial intelligence for detecting superficial esophageal squamous cell carcinoma under multiple endoscopic imaging modalities: A multicenter study. J. Gastroenterol. Hepatol. 2022, 37, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Everson, M.A.; Garcia-Peraza-Herrera, L.; Wang, H.-P.; Lee, C.-T.; Chung, C.-S.; Hsieh, P.-H.; Chen, C.-C.; Tseng, C.-H.; Hsu, M.-H.; Vercauteren, T. A clinically interpretable convolutional neural network for the real-time prediction of early squamous cell cancer of the esophagus: Comparing diagnostic performance with a panel of expert European and Asian endoscopists. Gastrointest. Endosc. 2021, 94, 273–281. [Google Scholar] [CrossRef]
- Tang, D.; Wang, L.; Jiang, J.; Liu, Y.; Ni, M.; Fu, Y.; Guo, H.; Wang, Z.; An, F.; Zhang, K. A novel deep learning system for diagnosing early esophageal squamous cell carcinoma: A multicenter diagnostic study. Clin. Transl. Gastroenterol. 2021, 12, e00393. [Google Scholar] [CrossRef]
- Li, B.; Cai, S.-L.; Tan, W.-M.; Li, J.-C.; Yalikong, A.; Feng, X.-S.; Yu, H.-H.; Lu, P.-X.; Feng, Z.; Yao, L.-Q. Comparative study on artificial intelligence systems for detecting early esophageal squamous cell carcinoma between narrow-band and white-light imaging. World J. Gastroenterol. 2021, 27, 281. [Google Scholar] [CrossRef]
- Iwagami, H.; Ishihara, R.; Aoyama, K.; Fukuda, H.; Shimamoto, Y.; Kono, M.; Nakahira, H.; Matsuura, N.; Shichijo, S.; Kanesaka, T. Artificial intelligence for the detection of esophageal and esophagogastric junctional adenocarcinoma. J. Gastroenterol. Hepatol. 2021, 36, 131–136. [Google Scholar] [CrossRef]
- Waki, K.; Ishihara, R.; Kato, Y.; Shoji, A.; Inoue, T.; Matsueda, K.; Miyake, M.; Shimamoto, Y.; Fukuda, H.; Matsuura, N. Usefulness of an artificial intelligence system for the detection of esophageal squamous cell carcinoma evaluated with videos simulating overlooking situation. Dig. Endosc. 2021, 33, 1101–1109. [Google Scholar] [CrossRef]
- Wang, Y.-K.; Syu, H.-Y.; Chen, Y.-H.; Chung, C.-S.; Tseng, Y.S.; Ho, S.-Y.; Huang, C.-W.; Wu, I.-C.; Wang, H.-C. Endoscopic images by a single-shot multibox detector for the identification of early cancerous lesions in the esophagus: A pilot study. Cancers 2021, 13, 321. [Google Scholar] [CrossRef]
- Yang, X.X.; Li, Z.; Shao, X.J.; Ji, R.; Qu, J.Y.; Zheng, M.Q.; Sun, Y.N.; Zhou, R.C.; You, H.; Li, L.X. Real-time artificial intelligence for endoscopic diagnosis of early esophageal squamous cell cancer (with video). Dig. Endosc. 2021, 33, 1075–1084. [Google Scholar] [CrossRef]
- Shiroma, S.; Yoshio, T.; Kato, Y.; Horie, Y.; Namikawa, K.; Tokai, Y.; Yoshimizu, S.; Yoshizawa, N.; Horiuchi, Y.; Ishiyama, A. Ability of artificial intelligence to detect T1 esophageal squamous cell carcinoma from endoscopic videos and the effects of real-time assistance. Sci. Rep. 2021, 11, 7759. [Google Scholar] [CrossRef] [PubMed]
- Ohmori, M.; Ishihara, R.; Aoyama, K.; Nakagawa, K.; Iwagami, H.; Matsuura, N.; Shichijo, S.; Yamamoto, K.; Nagaike, K.; Nakahara, M. Endoscopic detection and differentiation of esophageal lesions using a deep neural network. Gastrointest. Endosc. 2020, 91, 301–309.e1. [Google Scholar] [CrossRef] [PubMed]
- Guo, L.; Xiao, X.; Wu, C.; Zeng, X.; Zhang, Y.; Du, J.; Bai, S.; Xie, J.; Zhang, Z.; Li, Y. Real-time automated diagnosis of precancerous lesions and early esophageal squamous cell carcinoma using a deep learning model (with videos). Gastrointest. Endosc. 2020, 91, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, H.; Ishihara, R.; Kato, Y.; Matsunaga, T.; Nishida, T.; Yamada, T.; Ogiyama, H.; Horie, M.; Kinoshita, K.; Tada, T. Comparison of performances of artificial intelligence versus expert endoscopists for real-time assisted diagnosis of esophageal squamous cell carcinoma (with video). Gastrointest. Endosc. 2020, 92, 848–855. [Google Scholar] [CrossRef]
- Tokai, Y.; Yoshio, T.; Aoyama, K.; Horie, Y.; Yoshimizu, S.; Horiuchi, Y.; Ishiyama, A.; Tsuchida, T.; Hirasawa, T.; Sakakibara, Y. Application of artificial intelligence using convolutional neural networks in determining the invasion depth of esophageal squamous cell carcinoma. Esophagus 2020, 17, 250–256. [Google Scholar] [CrossRef]
- Liu, G.; Hua, J.; Wu, Z.; Meng, T.; Sun, M.; Huang, P.; He, X.; Sun, W.; Li, X.; Chen, Y. Automatic classification of esophageal lesions in endoscopic images using a convolutional neural network. Ann. Transl. Med. 2020, 8, 486. [Google Scholar] [CrossRef]
- Hashimoto, R.; Requa, J.; Dao, T.; Ninh, A.; Tran, E.; Mai, D.; Lugo, M.; Chehade, N.E.-H.; Chang, K.J.; Karnes, W.E. Artificial intelligence using convolutional neural networks for real-time detection of early esophageal neoplasia in Barrett’s esophagus (with video). Gastrointest. Endosc. 2020, 91, 1264–1271.e1. [Google Scholar] [CrossRef] [PubMed]
- De Groof, A.J.; Struyvenberg, M.R.; van der Putten, J.; van der Sommen, F.; Fockens, K.N.; Curvers, W.L.; Zinger, S.; Pouw, R.E.; Coron, E.; Baldaque-Silva, F. Deep-learning system detects neoplasia in patients with Barrett’s esophagus with higher accuracy than endoscopists in a multistep training and validation study with benchmarking. Gastroenterology 2020, 158, 915–929.e4. [Google Scholar] [CrossRef] [PubMed]
- De Groof, A.J.; Struyvenberg, M.R.; Fockens, K.N.; van der Putten, J.; van der Sommen, F.; Boers, T.G.; Zinger, S.; Bisschops, R.; Peter, H.; Pouw, R.E. Deep learning algorithm detection of Barrett’s neoplasia with high accuracy during live endoscopic procedures: A pilot study (with video). Gastrointest. Endosc. 2020, 91, 1242–1250. [Google Scholar] [CrossRef] [PubMed]
- Ebigbo, A.; Mendel, R.; Probst, A.; Manzeneder, J.; de Souza, L.A., Jr.; Papa, J.P.; Palm, C.; Messmann, H. Computer-aided diagnosis using deep learning in the evaluation of early oesophageal adenocarcinoma. Gut 2019, 68, 1143–1145. [Google Scholar] [CrossRef]
- García-Peraza-Herrera, L.C.; Everson, M.; Lovat, L.; Wang, H.-P.; Wang, W.L.; Haidry, R.; Stoyanov, D.; Ourselin, S.; Vercauteren, T. Intrapapillary capillary loop classification in magnification endoscopy: Open dataset and baseline methodology. Int. J. Comput. Assist. Radiol. Surg. 2020, 15, 651–659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumagai, Y.; Takubo, K.; Kawada, K.; Aoyama, K.; Endo, Y.; Ozawa, T.; Hirasawa, T.; Yoshio, T.; Ishihara, S.; Fujishiro, M. Diagnosis using deep-learning artificial intelligence based on the endocytoscopic observation of the esophagus. Esophagus 2019, 16, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Fonollà, R.; Scheeve, T.; Struyvenberg, M.R.; Curvers, W.L.; de Groof, A.J.; van der Sommen, F.; Schoon, E.J.; Bergman, J.J.; de With, P.H. Ensemble of deep convolutional neural networks for classification of early Barrett’s neoplasia using volumetric laser endomicroscopy. Appl. Sci. 2019, 9, 2183. [Google Scholar] [CrossRef] [Green Version]
- Cai, S.-L.; Li, B.; Tan, W.-M.; Niu, X.-J.; Yu, H.-H.; Yao, L.-Q.; Zhou, P.-H.; Yan, B.; Zhong, Y.-S. Using a deep learning system in endoscopy for screening of early esophageal squamous cell carcinoma (with video). Gastrointest. Endosc. 2019, 90, 745–753.e2. [Google Scholar] [CrossRef]
- Ebigbo, A.; Mendel, R.; Probst, A.; Manzeneder, J.; Prinz, F.; de Souza, L.A., Jr.; Papa, J.; Palm, C.; Messmann, H. Real-time use of artificial intelligence in the evaluation of cancer in Barrett’s oesophagus. Gut 2020, 69, 615–616. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.-Y.; Xue, D.-X.; Wang, Y.-L.; Zhang, R.; Sun, B.; Cai, Y.-P.; Feng, H.; Cai, Y.; Xu, J.-M. Computer-assisted diagnosis of early esophageal squamous cell carcinoma using narrow-band imaging magnifying endoscopy. Endoscopy 2019, 51, 333–341. [Google Scholar] [CrossRef]
- Everson, M.; Herrera, L.G.P.; Li, W.; Luengo, I.M.; Ahmad, O.; Banks, M.; Magee, C.; Alzoubaidi, D.; Hsu, H.; Graham, D. Artificial intelligence for the real-time classification of intrapapillary capillary loop patterns in the endoscopic diagnosis of early oesophageal squamous cell carcinoma: A proof-of-concept study. United Eur. Gastroenterol. J. 2019, 7, 297–306. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.M.; Wang, Y.J.; Zhang, S.T. Accuracy of artificial intelligence-assisted detection of esophageal cancer and neoplasms on endoscopic images: A systematic review and meta-analysis. J. Dig. Dis. 2021, 22, 318–328. [Google Scholar] [CrossRef]
- Lui, T.K.; Tsui, V.W.; Leung, W.K. Accuracy of artificial intelligence–assisted detection of upper GI lesions: A systematic review and meta-analysis. Gastrointest. Endosc. 2020, 92, 821–830.e9. [Google Scholar] [CrossRef]
- Bang, C.S.; Lee, J.J.; Baik, G.H. Computer-aided diagnosis of esophageal cancer and neoplasms in endoscopic images: A systematic review and meta-analysis of diagnostic test accuracy. Gastrointest. Endosc. 2021, 93, 1006–1015.e3. [Google Scholar] [CrossRef]
- Mohan, B.P.; Khan, S.R.; Kassab, L.L.; Ponnada, S.; Dulai, P.S.; Kochhar, G.S. Accuracy of convolutional neural network-based artificial intelligence in diagnosis of gastrointestinal lesions based on endoscopic images: A systematic review and meta-analysis. Endosc. Int. Open 2020, 8, E1584–E1594. [Google Scholar] [CrossRef] [PubMed]
- Jemal, A.; Ward, E.M.; Johnson, C.J.; Cronin, K.A.; Ma, J.; Ryerson, A.B.; Mariotto, A.; Lake, A.J.; Wilson, R.; Sherman, R.L. Annual report to the nation on the status of cancer, 1975–2014, featuring survival. J. Natl. Cancer Inst. 2017, 109, djx030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaise, M. Advanced endoscopic imaging for early gastric cancer. Best Pract. Res. Clin. Gastroenterol. 2015, 29, 575–587. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.-Q.; Jiao, G.-G.; Chang, F.-B.; Fang, W.-H.; Song, J.-X.; Lu, N.; Lin, D.-M.; Xie, Y.-Q.; Yang, L. Long-term results of operation for 420 patients with early squamous cell esophageal carcinoma discovered by screening. Ann. Thorac. Surg. 2004, 77, 1740–1744. [Google Scholar] [CrossRef]
- Abe, H.; Hatta, W.; Ogata, Y.; Koike, T.; Saito, M.; Jin, X.; Nakagawa, K.; Kanno, T.; Uno, K.; Asano, N. Prevention of delayed bleeding with vonoprazan in upper gastrointestinal endoscopic treatment. J. Gastroenterol. 2021, 56, 640–650. [Google Scholar] [CrossRef]
- Hatta, W.; Koike, T.; Abe, H.; Ogata, Y.; Saito, M.; Jin, X.; Kanno, T.; Uno, K.; Asano, N.; Imatani, A. Recent approach for preventing complications in upper gastrointestinal endoscopic submucosal dissection. DEN Open 2022, 2, e60. [Google Scholar] [CrossRef]
- Takayanagi, D.; Cho, H.; Machida, E.; Kawamura, A.; Takashima, A.; Wada, S.; Tsunoda, T.; Kohno, T.; Shiraishi, K. Update on Epidemiology, Diagnosis, and Biomarkers in Gastroenteropancreatic Neuroendocrine Neoplasms. Cancers 2022, 14, 1119. [Google Scholar] [CrossRef]
- Ay, B.; Turker, C.; Emre, E.; Ay, K.; Aydin, G. Automated classification of nasal polyps in endoscopy video-frames using handcrafted and CNN features. Comput. Biol. Med. 2022, 147, 105725. [Google Scholar] [CrossRef]
- Wolfson, P.; Ho, K.M.A.; Wilson, A.; McBain, H.; Hogan, A.; Lipman, G.; Dunn, J.; Haidry, R.; Novelli, M.; Olivo, A. Endoscopic eradication therapy for Barrett’s Esophagus related neoplasia. A final 10 year report from the United Kingdom National Halo Radiofrequency Ablation Registry. Gastrointest. Endosc. 2022, 96, 223–233. [Google Scholar] [CrossRef]
- Tsai, C.-L.; Mukundan, A.; Chung, C.-S.; Chen, Y.-H.; Wang, Y.-K.; Chen, T.-H.; Tseng, Y.-S.; Huang, C.-W.; Wu, I.-C.; Wang, H.-C. Hyperspectral Imaging Combined with Artificial Intelligence in the Early Detection of Esophageal Cancer. Cancers 2021, 13, 4593. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Study Type | Country/ Region | Modality | Model | Total Images | Total Patient | Number of Endoscopists | Real-Time | Compare with Endoscopist | External Validation | Video Validation | Target | Quality |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Gong | 2022 | RE | Korea | WLI | CNN | 5162 | NR | NR | No | No | Yes | No | EC | H |
| Liu | 2022 | RE | China | WLI | CNN | 13,083 | 1239 | 14 | No | Yes | Yes | No | ESCC | H |
| Yuan | 2022 | RE | China | WLI, NBI | CNN | 53,933 | 2621 | 11 | Yes | Yes | Yes | Yes | ESCC | H |
| Everson | 2021 | RE | Taiwan | NBI | CNN | 67,742 | NR | 3 | No | Yes | No | No | ESCC | H |
| Tang | 2021 | RE | China | WLI | CNN | 4002 | 1078 | 10 | Yes | Yes | Yes | Yes | ESCC | H |
| Li | 2021 | RE | China | WLI, NBI | CNN | 4735 | NR | 20 | No | Yes | No | No | ESCC | H |
| Iwagami | 2021 | RE | Japan | WLI, NBI | CNN | 232 | 79 | 15 | Yes | Yes | Yes | No | EAC | L |
| Waki | 2021 | RE | Japan | NBI/BLI | CNN | 17,336 | NR | 21 | Yes | Yes | No | Yes | ESCC | H |
| Wang | 2021 | RE | Taiwan | WLI, NBI | CNN | 935 | NR | NR | No | No | No | No | ESCC | L |
| Yang | 2021 | RE | China | WLI, NBI | CNN | 13,297 | 6130 | 6 | Yes | Yes | Yes | Yes | ESCC | H |
| Shiroma | 2021 | RE | Japan | NBI, WLI | CNN | 8428 | NR | 18 | Yes | Yes | No | Yes | ESCC | H |
| Ohmori | 2020 | RE | Japan | NBI, WLI, BLI | CNN | 135 | 102 | 15 | No | Yes | No | No | ESCC | H |
| Guo | 2020 | RE | China | NBI | CNN | 6671 | NR | NR | Yes | No | Yes | Yes | ESCC | H |
| Fukuda | 2020 | RE | Japan | NBI, BLI | CNN | 238 | NR | 13 | Yes | Yes | Yes | Yes | ESSC | L |
| Tokai | 2020 | RE | Japan | NBI, WLI | CNN | 279 | NR | 13 | No | Yes | No | No | ESCC | H |
| Liu | 2020 | RE | China | WLI | CNN | 127 | NR | NR | No | No | No | No | ESCC/EAC | H |
| Hashimoto | 2020 | RE | Japan | NBI, WLI | CNN | 458 | 39 | NR | Yes | No | No | No | BE | H |
| de Groof | 2020 | PR | Netherlands | WLI | CNN | 144 | 20 | NR | No | No | No | No | BE | H |
| de Groof | 2020 | RE | Netherlands | WLI | CNN | 494,364 | 15,286 | 53 | No | Yes | Yes | No | BE | L |
| Ebigbo | 2020 | RE | Europe | WLI | CNN | 62 | 14 | NR | No | No | No | No | BE | L |
| Herrera | 2020 | RE | Asia | NBI | CNN | 67,742$ | 114 | NR | NR | NR | No | No | ESCC | H |
| Kumagai | 2019 | RE | Japan | ECS | CNN | 1520 | 55 | NR | No | No | No | No | ESCC | H |
| Fonolla | 2019 | PR | Europe | VLI | CNN | 141 | NR | NR | No | No | No | No | BE | L |
| Horie | 2019 | RE | Japan | NBI, WLI | CNN | 1118 | 97 | NR | Yes | No | No | No | ESCC/EAC | H |
| Cai | 2019 | RE | China | WLI | CNN | 187 | 52 | 16 | No | Yes | No | No | ESCC | H |
| Ebigbo | 2019 | RE | Germany | NBI, WLI | CNN | 148 | NR | NR | No | No | No | No | BE/EAC | H |
| Ebigbo # | 2019 | RE | Germany | WLI | CNN | 100 | NR | NR | No | No | No | No | BE | H |
| Zhao | 2019 | RE | China | NBI | CNN | 1383 | NR | 9 | No | Yes | No | No | ESCC | H |
| Everson | 2019 | RE | Taiwan | NBI | CNN | 7046 | 17 | NR | No | No | No | No | ESCC | L |
| Subgroup | Studies (n) | Sensitivity (95%CI) | Specificity (95%CI) | Positive Predictive Value (95%CI) | Negative Predictive Value (95%CI) | Accuracy (95%CI) | Disease Prevalence |
|---|---|---|---|---|---|---|---|
| All | 28 | 93.80 (93.64–93.96) | 91.73 (91.52–91.94) | 93.62 (93.47–93.77) | 91.97 (91.77–92.15) | 92.90 (92.77–93.03) | 56.38 (56.14–56.63) |
| Region | |||||||
| Asia | 23 | 93.82 (93.66–93.98) | 91.75 (91.55–91.96) | 93.66 (93.51–93.80) | 91.97 (91.77–92.16) | 92.92 (92.80–93.05) | 56.48 (56.23–56.72) |
| West | 5 | 88.20 (84.39–91.36) | 88.99 (86.03–91.51) | 84.18 (80.66–87.16) | 91.91 (89.51–93.79) | 88.68 (86.41–90.68) | 39.91 (36.68–43.21) |
| Study design | |||||||
| Retrospective | 25 | 93.82 (93.66–93.98) | 91.75 (91.55–91.96) | 93.65 (93.50–93.80) | 91.97 (91.77–92.15) | 92.92 (92.79–93.05) | 56.46 (56.22–56.71) |
| Prospective | 3 | 85.78 (80.23–90.27) | 87.83 (84.10–90.95) | 79.19 (74.26–83.38) | 91.97 (89.08–94.14) | 87.11 (84.12–89.73) | 35.05 (31.17–39.08) |
| Endoscopy type | |||||||
| WLI | 9 | 92.60 (91.39–93.69) | 86.95 (85.58–88.25) | 85.42 (84.11–86.64) | 93.44 (92.44–94.32) | 89.51 (88.59–90.38) | 45.22 (43.78 46.67) |
| NBI | 5 | 93.73 (93.56–93.89) | 92.66 (92.45–92.86) | 94.39 (94.24–94.54) | 91.81 (91.61–92.01) | 93.27 (93.14–93.39) | 56.85 (56.60–57.11) |
| Mixed (WLI + NBI) | 11 | 95.70 (95.09–96.26) | 80.99 (79.72–82.21) | 86.15 (85.35–86.91) | 93.85 (93.03–94.58) | 89.12 (88.45–89.77) | 55.27 (54.21–56.32) |
| VLE/BLI/ECS | 3 | 88.24 (81.05–93.42) | 74.58 (67.50–80.81) | 70.00 (64.26–75.18) | 90.41 (85.12–93.95) | 80.07 (75.06–84.47) | 40.20 (34.57–46.03) |
| Histological type | |||||||
| ESCC | 18 | 93.81 (93.65–93.97) | 91.79 (91.58–92.00) | 93.74 (93.59–93.89) | 91.88 (91.69–92.07) | 92.94 (92.81–93.06) | 56.72 (56.47–56.96) |
| BE | 6 | 90.87 (88.05–93.22) | 91.41 (89.06–93.40) | 88.80 (86.12–91.02) | 93.04 (91.04–94.61) | 91.18 (89.43–92.72) | 42.85 (40.03–45.70) |
| EAC, including ESCC | 4 | 95.80 (90.47–98.62) | 52.38 (43.99–60.67) | 61.96 (57.79–65.96) | 93.90 (86.56–97.36) | 71.80 (65.99–77.13) | 44.74 (38.66–50.93) |
| Methodological quality | |||||||
| High | 21 | 93.85 (93.69–94.01) | 91.80 (91.59–92.01) | 93.68 (93.53–93.83 | 92.02 (91.82–92.21) | 92.96 (92.83–93.09) | 56.44 (56.19–56.69) |
| Low | 7 | 90.40 (88.70–91.93) | 87.75 (85.75–89.57) | 89.27 (87.71–90.65) | 89.03 (87.30–90.55) | 89.16 (87.88–90.35) | 52.98 (51.0–54.94) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Islam, M.M.; Poly, T.N.; Walther, B.A.; Yeh, C.-Y.; Seyed-Abdul, S.; Li, Y.-C.; Lin, M.-C. Deep Learning for the Diagnosis of Esophageal Cancer in Endoscopic Images: A Systematic Review and Meta-Analysis. Cancers 2022, 14, 5996. https://doi.org/10.3390/cancers14235996
Islam MM, Poly TN, Walther BA, Yeh C-Y, Seyed-Abdul S, Li Y-C, Lin M-C. Deep Learning for the Diagnosis of Esophageal Cancer in Endoscopic Images: A Systematic Review and Meta-Analysis. Cancers. 2022; 14(23):5996. https://doi.org/10.3390/cancers14235996
Chicago/Turabian StyleIslam, Md. Mohaimenul, Tahmina Nasrin Poly, Bruno Andreas Walther, Chih-Yang Yeh, Shabbir Seyed-Abdul, Yu-Chuan (Jack) Li, and Ming-Chin Lin. 2022. "Deep Learning for the Diagnosis of Esophageal Cancer in Endoscopic Images: A Systematic Review and Meta-Analysis" Cancers 14, no. 23: 5996. https://doi.org/10.3390/cancers14235996
APA StyleIslam, M. M., Poly, T. N., Walther, B. A., Yeh, C. -Y., Seyed-Abdul, S., Li, Y. -C., & Lin, M. -C. (2022). Deep Learning for the Diagnosis of Esophageal Cancer in Endoscopic Images: A Systematic Review and Meta-Analysis. Cancers, 14(23), 5996. https://doi.org/10.3390/cancers14235996