

Lung-Heart Outcomes and Mortality through the 2020 COVID-19 Pandemic in a Prospective Cohort of Breast Cancer Radiotherapy Patients
 , ,
, ,  , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Description of the Cohort
2.2. Clinical Data Collection
2.3. Toxicity Grades
2.4. Freedom from Adverse Event (fAE) Scores
2.5. Echocardiography Assessment
2.6. Lung Function Assessment
2.7. Interpolation and Handling of Missing Data
2.8. Longitudinal Analysis of Continuous Measurements
2.9. Survival Analysis
2.10. Statistical Implementation
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liu, C.; Zhao, Y.; Okwan-Duodu, D.; Basho, R.; Cui, X. COVID-19 in cancer patients: Risk, clinical features, and management. Cancer Biol. Med. 2020, 17, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, N.P.; Vinh-Hung, V.; Baumert, B.; Zamagni, A.; Arenas, M.; Motta, M.; Lara, P.C.; Myint, A.S.; Bonet, M.; Popescu, T.; et al. Older Cancer Patients during the COVID-19 Epidemic: Practice Proposal of the International Geriatric Radiotherapy Group. Cancers 2020, 12, 1287. [Google Scholar] [CrossRef] [PubMed]
- Rasulo, F.A.; Piva, S.; Latronico, N. Long-term complications of COVID-19 in ICU survivors: What do we know? Minerva Anestesiol. 2022, 88, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Plümper, T.; Neumayer, E. Lockdown policies and the dynamics of the first wave of the Sars-CoV-2 pandemic in Europe. J. Eur. Public Policy 2022, 29, 321–341. [Google Scholar] [CrossRef]
- Park, J.; Kim, S.; Heo, J. Aspects of Psychiatric Comorbidities in Breast Cancer Patients in Tertiary Hospitals Due to COVID-19 Outbreak in South Korea: A Single Center Longitudinal Cohort Study. Medicina 2022, 58, 560. [Google Scholar] [CrossRef]
- De Jaeghere, E.A.; Kanervo, H.; Colman, R.; Schrauwen, W.; West, P.; Vandemaele, N.; De Pauw, A.; Jacobs, C.; Hilderson, I.; Saerens, M.; et al. Mental Health and Quality of Life among Patients with Cancer during the SARS-CoV-2 Pandemic: Results from the Longitudinal ONCOVID Survey Study. Cancers 2022, 14, 1093. [Google Scholar] [CrossRef]
- Garassino, M.C.; Whisenant, J.G.; Huang, L.C.; Trama, A.; Torri, V.; Agustoni, F.; Baena, J.; Banna, G.; Berardi, R.; Bettini, A.C.; et al. COVID-19 in patients with thoracic malignancies (TERAVOLT): First results of an international, registry-based, cohort study. Lancet Oncol. 2020, 21, 914–922. [Google Scholar] [CrossRef]
- Lee, R.J.; Wysocki, O.; Bhogal, T.; Shotton, R.; Tivey, A.; Angelakas, A.; Aung, T.; Banfill, K.; Baxter, M.; Boyce, H.; et al. Longitudinal characterisation of haematological and biochemical parameters in cancer patients prior to and during COVID-19 reveals features associated with outcome. ESMO Open 2021, 6, 100005. [Google Scholar] [CrossRef]
- Ferrari, B.L.; Ferreira, C.G.; Menezes, M.; De Marchi, P.; Canedo, J.; Melo, A.C.; Jacome, A.A.; Reinert, T.; Paes, R.D.; Sodre, B.; et al. Determinants of COVID-19 Mortality in Patients With Cancer From a Community Oncology Practice in Brazil. JCO Glob. Oncol. 2021, 7, 46–55. [Google Scholar] [CrossRef]
- Fendler, A.; Au, L.; Shepherd, S.T.C.; Byrne, F.; Cerrone, M.; Boos, L.A.; Rzeniewicz, K.; Gordon, W.; Shum, B.; Gerard, C.L.; et al. Functional antibody and T cell immunity following SARS-CoV-2 infection, including by variants of concern, in patients with cancer: The CAPTURE study. Nat. Cancer 2021, 2, 1321–1337. [Google Scholar] [CrossRef]
- Madani, M.; Goldstein, D.; Stefanescu, R.; Woodman, S.E.; Rojas-Hernandez, C.M. Characterization of coagulopathy and outcomes in cancer patients with severe COVID-19 illness: Longitudinal changes in hospitalized cancer patients. Cancer Med. 2022, 11, 3771–3785. [Google Scholar] [CrossRef] [PubMed]
- Van de Steene, J.; Soete, G.; Storme, G. Adjuvant radiotherapy for breast cancer significantly improves overall survival: The missing link. Radiother Oncol. 2000, 55, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Van Parijs, H.; Cecilia-Joseph, E.; Gorobets, O.; Storme, G.; Adriaenssens, N.; Heyndrickx, B.; Verschraegen, C.; Nguyen, N.P.; De Ridder, M.; Vinh-Hung, V. Lung-heart toxicity in a randomized clinical trial of hypofractionated image guided radiation therapy for breast cancer. Preprints 2022, 202212, 0214. [Google Scholar] [CrossRef]
- Van Parijs, H.; Vinh-Hung, V.; Fontaine, C.; Storme, G.; Verschraegen, C.; Nguyen, D.M.; Adriaenssens, N.; Nguyen, N.P.; Gorobets, O.; De Ridder, M. Cardiopulmonary-related patient-reported outcomes in a randomized clinical trial of radiation therapy for breast cancer. BMC Cancer 2021, 21, 1177. [Google Scholar] [CrossRef] [PubMed]
- Vinh-Hung, V.; Van Parijs, H. TomoBreast Randomized Clinical Trial’s Lung-Heart Outcomes and Mortality through the 2020 COVID-19 Pandemic: Data and Software. Available online: https://zenodo.org/deposit/5919956 (accessed on 5 December 2022).
- Riera, R.; Bagattini, A.M.; Pacheco, R.L.; Pachito, D.V.; Roitberg, F.; Ilbawi, A. Delays and Disruptions in Cancer Health Care Due to COVID-19 Pandemic: Systematic Review. JCO Glob. Oncol. 2021, 7, 311–323. [Google Scholar] [CrossRef] [PubMed]
- Lazzerini, M.; Barbi, E.; Apicella, A.; Marchetti, F.; Cardinale, F.; Trobia, G. Delayed access or provision of care in Italy resulting from fear of COVID-19. Lancet Child Adolesc. Health 2020, 4, e10–e11. [Google Scholar] [CrossRef] [PubMed]
- Iodice, F.; Cassano, V.; Rossini, P.M. Direct and indirect neurological, cognitive, and behavioral effects of COVID-19 on the healthy elderly, mild-cognitive-impairment, and Alzheimer’s disease populations. Neurol. Sci. 2021, 42, 455–465. [Google Scholar] [CrossRef] [PubMed]
- Kumar, J.; Kumar, P. COVID-19 pandemic and health-care disruptions: Count the most vulnerable. Lancet Glob. Health 2021, 9, e722–e723. [Google Scholar] [CrossRef]
- eHealth-Platform. Wie Zijn Wij? Available online: https://www.ehealth.fgov.be/ehealthplatform/nl/wie-zijn-wij (accessed on 5 December 2022).
- eHealth in Belgium. Available online: https://gnius.esante.gouv.fr/en/decrypting-ehealth-abroad/ehealth-in-belgium (accessed on 5 December 2022).
- Detollenaere, J.; Christiaens, W.; Dossche, D.; Camberlin, C.; Lefèvre, M.; Devriese, S. Barriers and facilitators for eHealth adoption by general practitioners in Belgium. Analysis based on the integrated allowance for GP practices. KCE Rep. 2020, 337, D/2020/10.273/42. Available online: https://kce.fgov.be/sites/default/files/2021-11/KCE_337_eHealth_adoption_in_Belgium_Report_V2.pdf (accessed on 5 December 2022).
- Vray, M.; Hamelin, B.; Jaillon, P.; Round Table No, G.X.X. The respective roles of controlled clinical trials and cohort monitoring studies in the pre- and postmarketing assessment of drugs. Therapie 2005, 60, 345–349. [Google Scholar] [CrossRef] [Green Version]
- Verbanck, S.; Van Parijs, H.; Schuermans, D.; Vinh-Hung, V.; Storme, G.; Fontaine, C.; De Ridder, M.; Verellen, D.; Vanderhelst, E.; Hanon, S. Lung Restriction in Patients With Breast Cancer After Hypofractionated and Conventional Radiation Therapy: A 10-Year Follow-up. Int. J. Radiat. Oncol. Biol. Phys. 2022, 113, 561–569. [Google Scholar] [CrossRef] [PubMed]
- Dixon, W.J. Analysis of Extreme Values. Ann. Math. Stat. 1950, 21, 488–506. [Google Scholar] [CrossRef]
- Stefansky, W. Rejecting Outliers in Factorial Designs. Technometrics 1972, 14, 469–479. [Google Scholar] [CrossRef]
- Kaplan, E.L.; Meier, P. Nonparametric estimation from incomplete observations. J. Am. Stat. Assoc. 1958, 53, 457–481. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Version 4.1.2.; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- Bustos Sierra, N.; Bossuyt, N.; Braeye, T.; Leroy, M.; Moyersoen, I.; Peeters, I.; Scohy, A.; Van der Heyden, J.; Van Oyen, H.; Renard, F. All-cause mortality supports the COVID-19 mortality in Belgium and comparison with major fatal events of the last century. Arch. Public Health 2020, 78, 117. [Google Scholar] [CrossRef]
- Silversmit, G.; Verdoodt, F.; Van Damme, N.; De Schutter, H.; Van Eycken, L. Excess Mortality in a Nationwide Cohort of Cancer Patients during the Initial Phase of the COVID-19 Pandemic in Belgium. Cancer Epidemiol. Biomark. Prev. 2021, 30, 1615–1619. [Google Scholar] [CrossRef]
- Sciensano. Health Status. Mortality and Causes of Death, General mortality. Available online: https://www.healthybelgium.be/en/health-status/mortality-and-causes-of-death/general-mortality (accessed on 7 December 2022).
- Peron, J.; Dagonneau, T.; Conrad, A.; Pineau, F.; Calattini, S.; Freyer, G.; Perol, D.; Sajous, C.; Heiblig, M. COVID-19 Presentation and Outcomes among Cancer Patients: A Matched Case-Control Study. Cancers 2021, 13, 5283. [Google Scholar] [CrossRef]
- Alagoz, O.; Lowry, K.P.; Kurian, A.W.; Mandelblatt, J.S.; Ergun, M.A.; Huang, H.; Lee, S.J.; Schechter, C.B.; Tosteson, A.N.A.; Miglioretti, D.L.; et al. Impact of the COVID-19 Pandemic on Breast Cancer Mortality in the US: Estimates From Collaborative Simulation Modeling. NCI J. Natl. Cancer Inst. 2021, 113, 1484–1494. [Google Scholar] [CrossRef]
- Registry Study Describes COVID-19 Mortality and Hospitalization in Patients with Breast Cancer. Oncologist 2021, 26 (Suppl. S2), S17–S18. [CrossRef]
- Blanco, J.R.; Cobos-Ceballos, M.J.; Navarro, F.; Sanjoaquin, I.; Arnaiz de Las Revillas, F.; Bernal, E.; Buzon-Martin, L.; Viribay, M.; Romero, L.; Espejo-Perez, S.; et al. Pulmonary long-term consequences of COVID-19 infections after hospital discharge. Clin. Microbiol. Infect. 2021, 27, 892–896. [Google Scholar] [CrossRef]
- Ritz, T.; Rosenfield, D.; Steptoe, A. Physical activity, lung function, and shortness of breath in the daily life of individuals with asthma. Chest 2010, 138, 913–918. [Google Scholar] [CrossRef] [PubMed]
- Natalucci, V.; Marini, C.F.; Flori, M.; Pietropaolo, F.; Lucertini, F.; Annibalini, G.; Vallorani, L.; Sisti, D.; Saltarelli, R.; Villarini, A.; et al. Effects of a Home-Based Lifestyle Intervention Program on Cardiometabolic Health in Breast Cancer Survivors during the COVID-19 Lockdown. J. Clin. Med. 2021, 10, 2678. [Google Scholar] [CrossRef] [PubMed]
- Oleszak, F.; Maryniak, A.; Botti, E.; Abrahim, C.; Salifu, M.O.; Youssef, M.; Henglein, V.L.; McFarlane, S.I. Myocarditis Associated With COVID-19. Am. J. Med. Case Rep. 2020, 8, 498–502. [Google Scholar] [CrossRef] [PubMed]
- Luoto, J.; Pihlsgard, M.; Wollmer, P.; Elmstahl, S. Relative and absolute lung function change in a general population aged 60–102 years. Eur. Respir. J. 2019, 53, 1701812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, E.T.; Guppy, M.; Straus, S.E.; Bell, K.J.L.; Glasziou, P. Rate of normal lung function decline in ageing adults: A systematic review of prospective cohort studies. BMJ Open 2019, 9, e028150. [Google Scholar] [CrossRef]
- Zaugg, M.; Lucchinetti, E. Respiratory function in the elderly. Anesthesiol. Clin. N. Am. 2000, 18, 47–58. [Google Scholar] [CrossRef]
- Sherrill, D.L.; Enright, P.L.; Kaltenborn, W.T.; Lebowitz, M.D. Predictors of longitudinal change in diffusing capacity over 8 years. Am. J. Respir. Crit. Care Med. 1999, 160, 1883–1887. [Google Scholar] [CrossRef]
- Dunlay, S.M.; Roger, V.L.; Weston, S.A.; Jiang, R.; Redfield, M.M. Longitudinal changes in ejection fraction in heart failure patients with preserved and reduced ejection fraction. Circ. Heart Fail. 2012, 5, 720–726. [Google Scholar] [CrossRef] [Green Version]
- Cho, D.H.; Joo, H.J.; Kim, M.N.; Kim, H.D.; Lim, D.S.; Park, S.M. Longitudinal Change in Myocardial Function and Clinical Parameters in Middle-Aged Subjects: A 3-Year Follow-up Study. Diabetes Metab. J. 2021, 45, 719–729. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | n (%) | n (%) | |
|---|---|---|---|
| Age (years) | Mastectomy | ||
| <50 | 36 (29.3%) | ||
| ≥50 | 87 (70.7%) | No | 78 (63.4%) |
| Screen-detected | Yes | 45 (36.6%) | |
| No | 55 (45.8%) | ||
| Yes | 65 (54.2%) | Axillary dissection | |
| Smoking history | No | 75 (61.0%) | |
| No | 84 (68.3%) | Yes | 48 (39.0%) |
| Yes | 39 (31.7%) | ||
| Laterality | Nodal irradiation | ||
| Right | 55 (44.7%) | No | 87 (70.7%) |
| Left | 67 (54.5%) | Yes | 36 (29.3%) |
| Bilateral | 1 (0.8%) | ||
| Stage | Chemotherapy | ||
| I | 53 (43.1%) | No | 67 (54.5%) |
| IIA | 57 (46.3%) | Before radiation | 14 (11.4%) |
| IIB | 13 (10.6%) | Concomitant | 42 (34.1%) |
| Progesterone receptor | Hormone therapy | ||
| Negative | 31 (25.2%) | No | 17 (13.8%) |
| Positive | 92 (74.8%) | Yes | 106 (86.2%) |
| Neu score | Trastuzumab | ||
| 0–2 | 100 (82.6%) | No | 110 (89.4%) |
| 3 | 21 (17.4%) | Yes | 13 (10.6%) |
| Year | n Alive in Year | n Died in Year | Case ID | Primary Cause of Death |
|---|---|---|---|---|
| 2007 | 12 | 0 | ||
| 2008 | 47 | 0 | ||
| 2009 | 78 | 0 | ||
| 2010 | 115 | 0 | ||
| 2011 | 123 | 1 | 10 | Metastatic disease |
| 2012 | 122 | 1 | 28 | Metastatic disease |
| 2013 | 121 | 2 | 47 | Metastatic disease + heart failure |
| 63 | Metastatic disease | |||
| 2014 | 119 | 1 | 85 | Renal abscess; cognitive dysfunction; NC |
| 2015 | 118 | 3 | 4 | Metastatic disease |
| 31 | Metastatic disease | |||
| 61 | Metastatic disease (lung cancer) | |||
| 2016 | 115 | 0 | ||
| 2017 | 115 | 2 | 79 | Unspecified; NC |
| 113 | Metastatic disease | |||
| 2018 | 113 | 1 | 73 | Digestive pathology |
| 2019 | 112 | 4 | 65 | Metastatic disease |
| 68 | Digestive pathology; NC | |||
| 76 | Metastatic disease (ovarian cancer) | |||
| 84 | Metastatic disease | |||
| 2020 | 108 | 4 | 16 | Digestive pathology; NC |
| 42 | Liver failure; NC | |||
| 45 | Pulmonary hypertension; bowel obstruction; NC | |||
| 103 | Unspecified (toxic thyroid adenoma?); NC | |||
| 2021 | 104 | 1 | 116 | Pulmonary hypertension (right heart failure); NC |
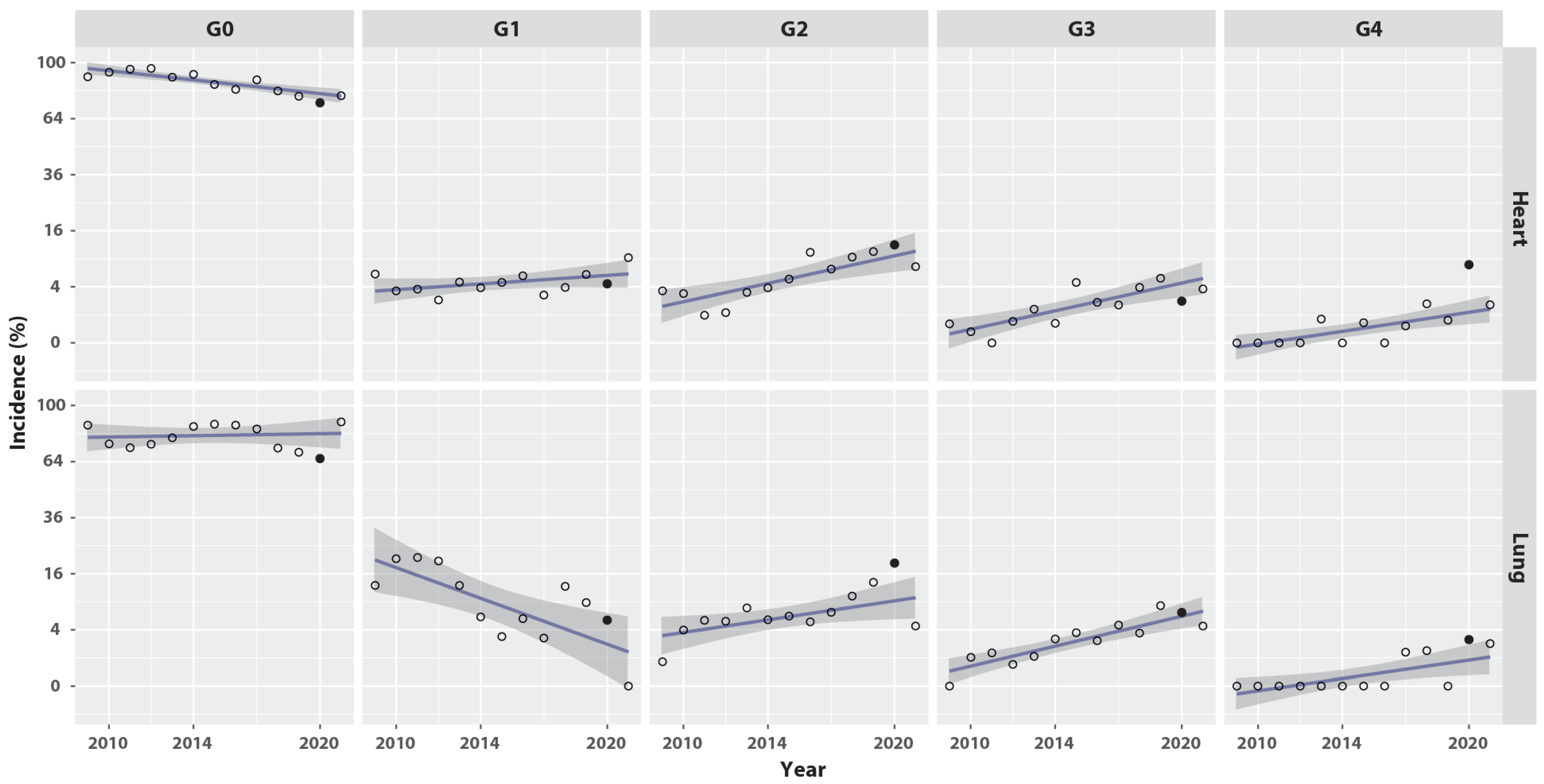
| Year | n Records | Heart | Lung | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n Data | G0 % | G1 % | G2 % | G3 % | G4 % | n Data | G0 % | G1 % | G2 % | G3 % | G4 % | ||
| 2007 * | 70 | 32 | 100.0 | 0.0 | 0.0 | 0.0 | 0.0 | 28 | 82.1 | 14.3 | 3.6 | 0.0 | 0.0 |
| 2008 | 493 | 381 | 97.4 | 2.1 | 0.5 | 0.0 | 0.0 | 360 | 92.2 | 5.0 | 1.7 | 1.1 | 0.0 |
| 2009 | 518 | 433 | 90.1 | 6.0 | 3.5 | 0.5 | 0.0 | 404 | 86.4 | 12.9 | 0.7 | 0.0 | 0.0 |
| 2010 | 687 | 612 | 93.3 | 3.4 | 3.1 | 0.2 | 0.0 | 579 | 74.4 | 20.6 | 4.0 | 1.0 | 0.0 |
| 2011 | 531 | 517 | 95.4 | 3.7 | 1.0 | 0.0 | 0.0 | 512 | 72.3 | 20.9 | 5.5 | 1.4 | 0.0 |
| 2012 | 340 | 340 | 95.9 | 2.4 | 1.2 | 0.6 | 0.0 | 338 | 74.3 | 19.8 | 5.3 | 0.6 | 0.0 |
| 2013 | 279 | 277 | 89.9 | 4.7 | 3.2 | 1.4 | 0.7 | 272 | 78.3 | 12.9 | 7.7 | 1.1 | 0.0 |
| 2014 | 217 | 207 | 91.8 | 3.9 | 3.9 | 0.5 | 0.0 | 215 | 85.6 | 6.0 | 5.6 | 2.8 | 0.0 |
| 2015 | 195 | 193 | 85.0 | 4.7 | 5.2 | 4.7 | 0.5 | 194 | 87.1 | 3.1 | 6.2 | 3.6 | 0.0 |
| 2016 | 194 | 192 | 81.8 | 5.7 | 10.4 | 2.1 | 0.0 | 192 | 86.5 | 5.7 | 5.2 | 2.6 | 0.0 |
| 2017 | 284 | 275 | 88.0 | 2.9 | 6.9 | 1.8 | 0.4 | 276 | 84.1 | 2.9 | 6.9 | 4.7 | 1.4 |
| 2018 | 317 | 256 | 80.9 | 3.9 | 9.4 | 3.9 | 2.0 | 254 | 72.0 | 12.6 | 10.2 | 3.5 | 1.6 |
| 2019 | 220 | 151 | 77.5 | 6.0 | 10.6 | 5.3 | 0.7 | 147 | 69.4 | 8.8 | 13.6 | 8.2 | 0.0 |
| 2020 | 134 | 90 | 73.3 | 4.4 | 12.2 | 2.2 | 7.8 | 73 | 65.8 | 5.5 | 19.2 | 6.8 | 2.7 |
| 2021 * | 168 | 54 | 77.8 | 9.3 | 7.4 | 3.7 | 1.9 | 44 | 88.6 | 0.0 | 4.5 | 4.5 | 2.3 |
| All years | 4647 | 4010 | 90.2 | 4.0 | 4.1 | 1.2 | 0.4 | 3888 | 79.5 | 12.6 | 5.5 | 2.1 | 0.3 |
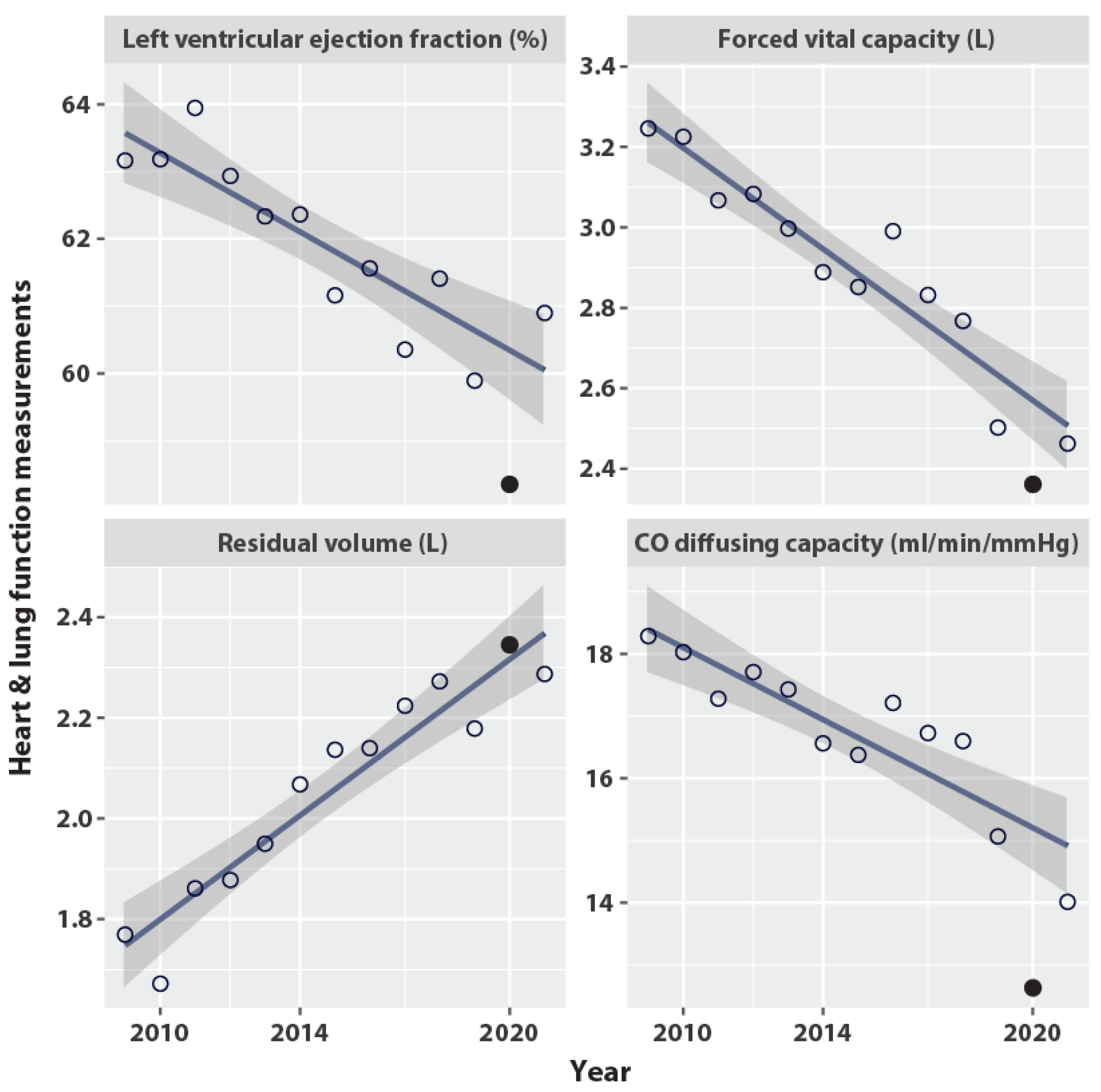
| Year | n Records | LVEF (%) | FVC (L) | RV (L) | DLCO (ml/min/mmHg) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n Data | Mean | SD | n Data | Mean | SD | n Data | Mean | SD | n Data | Mean | SD | ||
| 2007 * | 70 | 62 | 62.3 | 4.7 | 46 | 3.9 | 0.5 | 46 | 1.7 | 0.4 | 46 | 19.8 | 1.9 |
| 2008 | 493 | 446 | 63.8 | 4.4 | 393 | 3.6 | 0.7 | 391 | 1.9 | 0.5 | 391 | 18.5 | 3.3 |
| 2009 | 518 | 467 | 63.2 | 5.1 | 449 | 3.2 | 0.7 | 438 | 1.8 | 0.6 | 446 | 18.3 | 3.5 |
| 2010 | 687 | 587 | 63.2 | 4.5 | 621 | 3.2 | 0.6 | 612 | 1.7 | 0.5 | 612 | 18.0 | 3.2 |
| 2011 | 531 | 441 | 63.9 | 4.9 | 474 | 3.1 | 0.6 | 470 | 1.9 | 0.5 | 469 | 17.3 | 3.3 |
| 2012 | 340 | 216 | 62.9 | 4.4 | 260 | 3.1 | 0.6 | 256 | 1.9 | 0.5 | 256 | 17.7 | 3.4 |
| 2013 | 279 | 152 | 62.3 | 4.8 | 184 | 3.0 | 0.6 | 179 | 1.9 | 0.5 | 179 | 17.4 | 3.5 |
| 2014 | 217 | 121 | 62.4 | 4.6 | 117 | 2.9 | 0.7 | 111 | 2.1 | 0.6 | 113 | 16.6 | 3.6 |
| 2015 | 195 | 116 | 61.2 | 4.7 | 97 | 2.9 | 0.7 | 87 | 2.1 | 0.5 | 92 | 16.4 | 3.6 |
| 2016 | 194 | 104 | 61.6 | 5.7 | 104 | 3.0 | 0.6 | 99 | 2.1 | 0.5 | 101 | 17.2 | 3.8 |
| 2017 | 284 | 103 | 60.4 | 5.2 | 148 | 2.8 | 0.8 | 135 | 2.2 | 0.5 | 140 | 16.7 | 4.4 |
| 2018 | 317 | 104 | 61.4 | 6.8 | 140 | 2.8 | 0.8 | 123 | 2.3 | 0.4 | 127 | 16.6 | 4.0 |
| 2019 | 220 | 78 | 59.9 | 6.9 | 81 | 2.5 | 0.8 | 65 | 2.2 | 0.5 | 68 | 15.1 | 4.8 |
| 2020 | 134 | 44 | 58.4 | 8.2 | 46 | 2.4 | 0.7 | 36 | 2.3 | 0.6 | 43 | 12.6 | 5.0 |
| 2021 * | 168 | 10 | 60.9 | 7.6 | 13 | 2.5 | 0.7 | 10 | 2.3 | 0.5 | 10 | 14.0 | 5.1 |
| All years | 4647 | 3051 | 62.8 | 5.1 | 3173 | 3.1 | 0.7 | 3058 | 1.9 | 0.5 | 3093 | 17.6 | 3.6 |
| Baseline Characteristic | Alive through 2020 n = 103 | Died in 2020–2021 n = 5 | p-Value |
|---|---|---|---|
| Age (years) | 0.004 | ||
| Mean (SD) | 55.3 (10.9) | 70.0 (7.6) | |
| Karnofsky Performance Status | 0.816 | ||
| n missing | 5 | 0 | |
| Mean (SD) | 94.8 (7.4) | 94.0 (8.9) | |
| Weight (kg) | 0.424 | ||
| Mean (SD) | 67.8 (12.1) | 63.4 (10.3) | |
| Smoking history | 0.600 | ||
| No | 71 (68.9%) | 4 (80.0%) | |
| Yes | 32 (31.1%) | 1 (20.0%) | |
| Laterality | 0.474 | ||
| Right | 45 (43.7%) | 3 (60.0%) | |
| Left (1 case bilateral) | 58 (56.3%) | 2 (40.0%) | |
| Stage | 0.805 | ||
| I | 56 (54.4%) | 3 (60.0%) | |
| II | 47 (45.6%) | 2 (40.0%) | |
| Estrogen receptor positive | 0.686 | ||
| No | 14 (13.6%) | 1 (20.0%) | |
| Yes | 89 (86.4%) | 4 (80.0%) | |
| Progesterone receptor positive | 0.864 | ||
| No | 24 (23.3%) | 1 (20.0%) | |
| Yes | 79 (76.7%) | 4 (80.0%) | |
| Mastectomy | 0.442 | ||
| No | 65 (63.1%) | 4 (80.0%) | |
| Yes | 38 (36.9%) | 1 (20.0%) | |
| Axillary Dissection | 0.298 | ||
| No | 65 (63.1%) | 2 (40.0%) | |
| Yes | 38 (36.9%) | 3 (60.0%) | |
| Randomization arm | 0.709 | ||
| Conventional radiotherapy | 53 (51.5%) | 3 (60.0%) | |
| Tomotherapy | 50 (48.5%) | 2 (40.0%) | |
| Radiotherapy (RT) boost | 0.467 | ||
| No (= RT chest wall only) | 37 (35.9%) | 1 (20.0%) | |
| Yes (= RT breast conserving surgery) | 66 (64.1%) | 4 (80.0%) | |
| Nodal irradiation | 0.113 | ||
| No | 75 (72.8%) | 2 (40.0%) | |
| Yes | 28 (27.2%) | 3 (60.0%) | |
| Chemotherapy | 0.277 | ||
| No | 57 (55.3%) | 4 (80.0%) | |
| Yes | 46 (44.7%) | 1 (20.0%) | |
| Hormone therapy | 0.397 | ||
| No | 13 (12.6%) | 0 (0.0%) | |
| Yes | 90 (87.4%) | 5 (100.0%) | |
| Trastuzumab therapy | 0.441 | ||
| No | 92 (89.3%) | 5 (100.0%) | |
| Yes | 11 (10.7%) | 0 (0.0%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vinh-Hung, V.; Gorobets, O.; Adriaenssens, N.; Van Parijs, H.; Storme, G.; Verellen, D.; Nguyen, N.P.; Magne, N.; De Ridder, M. Lung-Heart Outcomes and Mortality through the 2020 COVID-19 Pandemic in a Prospective Cohort of Breast Cancer Radiotherapy Patients. Cancers 2022, 14, 6241. https://doi.org/10.3390/cancers14246241
Vinh-Hung V, Gorobets O, Adriaenssens N, Van Parijs H, Storme G, Verellen D, Nguyen NP, Magne N, De Ridder M. Lung-Heart Outcomes and Mortality through the 2020 COVID-19 Pandemic in a Prospective Cohort of Breast Cancer Radiotherapy Patients. Cancers. 2022; 14(24):6241. https://doi.org/10.3390/cancers14246241
Chicago/Turabian StyleVinh-Hung, Vincent, Olena Gorobets, Nele Adriaenssens, Hilde Van Parijs, Guy Storme, Dirk Verellen, Nam P. Nguyen, Nicolas Magne, and Mark De Ridder. 2022. "Lung-Heart Outcomes and Mortality through the 2020 COVID-19 Pandemic in a Prospective Cohort of Breast Cancer Radiotherapy Patients" Cancers 14, no. 24: 6241. https://doi.org/10.3390/cancers14246241
APA StyleVinh-Hung, V., Gorobets, O., Adriaenssens, N., Van Parijs, H., Storme, G., Verellen, D., Nguyen, N. P., Magne, N., & De Ridder, M. (2022). Lung-Heart Outcomes and Mortality through the 2020 COVID-19 Pandemic in a Prospective Cohort of Breast Cancer Radiotherapy Patients. Cancers, 14(24), 6241. https://doi.org/10.3390/cancers14246241