
Adjuvant Therapy for Elderly Breast Cancer Patients after Breast-Conserving Surgery: Outcomes in Real World Practice

 , , ,
, , ,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Study Population
2.3. Statistical Analyses and Endpoints
3. Results
3.1. Patient Characteristics
3.2. Outcome
3.3. Factors Associated with the Use of Postoperative Radiotherapy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Darby, S.; McGale, P.; Correa, C.; Taylor, C.; Arriagada, R.; Clarke, M.; Cutter, D.; Davies, C.; Ewertz, M.; Godwin, J.; et al. Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: Meta-analysis of individual patient data for 10 801 women in 17 randomised trials. Lancet 2011, 378, 1707–1716. [Google Scholar] [CrossRef]
- Hutchins, L.F.; Unger, J.M.; Crowley, J.J.; Coltman, C.A.J.; Albain, K.S. Underrepresentation of Patients 65 Years of Age or Older in Cancer-Treatment Trials. N. Engl. J. Med. 2008, 341, 2061–2067. [Google Scholar] [CrossRef]
- Kemeny, M.M.; Peterson, B.L.; Kornblith, A.B.; Muss, H.B.; Wheeler, J.; Levine, E.; Bartlett, N.; Fleming, G.; Cohen, H.J. Barriers to clinical trial participation by older women with breast cancer. J. Clin. Oncol. 2003, 21, 2268–2275. [Google Scholar] [CrossRef]
- Fyles, A.W.; McCready, D.R.; Manchul, L.A.; Trudeau, M.E.; Merante, P.; Pintilie, M.; Weir, L.M.; Olivotto, I.A. Tamoxifen with or without Breast Irradiation in Women 50 Years of Age or Older with Early Breast Cancer. N. Engl. J. Med. 2004, 351, 963–970. [Google Scholar] [CrossRef]
- Blamey, R.W.; Bates, T.; Chetty, U.; Duffy, S.W.; Ellis, I.O.; George, D.; Mallon, E.; Mitchell, M.J.; Monypenny, I.; Morgan, D.A.L.; et al. Radiotherapy or tamoxifen after conserving surgery for breast cancers of excellent prognosis: British Association of Surgical Oncology (BASO) II trial. Eur. J. Cancer 2013, 49, 2294–2302. [Google Scholar] [CrossRef] [PubMed]
- Hughes, K.S.; Schnaper, L.A.; Bellon, J.R.; Cirrincione, C.T.; Berry, D.A.; McCormick, B.; Muss, H.B.; Smith, B.L.; Hudis, C.A.; Winer, E.P.; et al. Lumpectomy plus tamoxifen with or without irradiation in women age 70 years or older with early breast cancer: Long-term follow-up of CALGB 9343. J. Clin. Oncol. 2013, 31, 2382–2387. [Google Scholar] [CrossRef] [PubMed]
- Fastner, G.; Sedlmayer, F.; Widder, J.; Metz, M.; Geinitz, H.; Kapp, K.; Fesl, C.; Sölkner, L.; Greil, R.; Jakesz, R.; et al. Endocrine therapy with or without whole breast irradiation in low-risk breast cancer patients after breast-conserving surgery: 10-year results of the Austrian Breast and Colorectal Cancer Study Group 8A trial. Eur. J. Cancer 2020, 127, 12–20. [Google Scholar] [CrossRef]
- Kunkler, I.H.; Williams, L.J.; Jack, W.J.L.; Cameron, D.A.; Dixon, J.M. Breast-Conserving Surgery with or without Irradiation in Early Breast Cancer. N. Engl. J. Med. 2023, 388, 585–594. [Google Scholar] [CrossRef]
- Joseph, K.; Zebak, S.; Alba, V.; Mah, K.; Au, C.; Vos, L.; Ghosh, S.; Abraham, A.; Chafe, S.; Wiebe, E.; et al. Adjuvant breast radiotherapy, endocrine therapy, or both after breast conserving surgery in older women with low-risk breast cancer: Results from a population-based study. Radiother. Oncol. 2021, 154, 93–100. [Google Scholar] [CrossRef]
- Murphy, C.T.; Li, T.; Wang, L.S.; Obeid, E.I.; Bleicher, R.J.; Eastwick, G.; Johnson, M.E.; Hayes, S.B.; Weiss, S.E.; Anderson, P.R. Comparison of Adjuvant Radiation Therapy Alone Versus Radiation Therapy and Endocrine Therapy in Elderly Women with Early-Stage, Hormone Receptor-Positive Breast Cancer Treated with Breast-Conserving Surgery. Clin. Breast Cancer 2015, 15, 381–389. [Google Scholar] [CrossRef] [PubMed]
- Fisher, B.; Bryant, J.; Dignam, J.J.; Wickerham, D.L.; Mamounas, E.P.; Fisher, E.R.; Margolese, R.G.; Nesbitt, L.; Paik, S.; Pisansky, T.M.; et al. Tamoxifen, radiation therapy, or both for prevention of ipsilateral breast tumor recurrence after lumpectomy in women with invasive breast cancers of one centimeter or less. J. Clin. Oncol. 2002, 20, 4141–4149. [Google Scholar] [CrossRef] [PubMed]
- Sedrak, M.S.; Freedman, R.A.; Cohen, H.J.; Muss, H.B.; Jatoi, A.; Klepin, H.D.; Wildes, T.M.; Le-Rademacher, J.G.; Kimmick, G.G.; Tew, W.P.; et al. Older adult participation in cancer clinical trials: A systematic review of barriers and interventions. CA. Cancer J. Clin. 2021, 71, 78–92. [Google Scholar] [CrossRef] [PubMed]
- MCR. Munich Cancer Registry. Available online: https://www.tumorregister-muenchen.de/ (accessed on 1 October 2022).
- Lyman, G.H.; Levine, M. Comparative effectiveness research in oncology: An overview. J. Clin. Oncol. 2012, 30, 4181–4184. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, K. Methods in comparative effectiveness research. J. Clin. Oncol. 2012, 30, 4208–4214. [Google Scholar] [CrossRef]
- Matuschek, C.; Bölke, E.; Haussmann, J.; Mohrmann, S.; Nestle-Krämling, C.; Gerber, P.A.; Corradini, S.; Orth, K.; Kammers, K.; Budach, W. The benefit of adjuvant radiotherapy after breast conserving surgery in older patients with low risk breast cancer- a meta-analysis of randomized trials. Radiat. Oncol. 2017, 12, 60. [Google Scholar] [CrossRef]
- Nekhlyudov, L.; Li, L.; Ross-Degnan, D.; Wagner, A.K. Five-year patterns of adjuvant hormonal therapy use, persistence, and adherence among insured women with early-stage breast cancer. Breast Cancer Res. Treat. 2011, 130, 681–689. [Google Scholar] [CrossRef] [PubMed]
- Hershman, D.L.; Kushi, L.H.; Shao, T.; Buono, D.; Kershenbaum, A.; Tsai, W.Y.; Fehrenbacher, L.; Lin Gomez, S.; Miles, S.; Neugut, A.I. Early discontinuation and nonadherence to adjuvant hormonal therapy in a cohort of 8,769 early-stage breast cancer patients. J. Clin. Oncol. 2010, 28, 4120–4128. [Google Scholar] [CrossRef]
- Owusu, C.; Buist, D.S.M.; Field, T.S.; Lash, T.L.; Thwin, S.S.; Geiger, A.M.; Quinn, V.P.; Frost, F.; Prout, M.; Yood, M.U.; et al. Predictors of tamoxifen discontinuation among older women with estrogen receptor-positive breast cancer. J. Clin. Oncol. 2008, 26, 549–555. [Google Scholar] [CrossRef]
- Barron, T.I.; Connolly, R.M.; Bennett, K.; Feely, J.; Kennedy, M.J. Early discontinuation of tamoxifen: A lesson for oncologists. Cancer 2007, 109, 832–839. [Google Scholar] [CrossRef]
- Partridge, A.H.; Wang, P.S.; Winer, E.P.; Avorn, J. Nonadherence to adjuvant tamoxifen therapy in women with primary breast cancer. J. Clin. Oncol. 2003, 21, 602–606. [Google Scholar] [CrossRef]
- Corradini, S.; Bauerfeind, I.; Belka, C.; Braun, M.; Combs, S.E.; Eckel, R.; Harbeck, N.; Hölzel, D.; Kiechle, M.; Niyazi, M.; et al. Trends in use and outcome of postoperative radiotherapy following mastectomy: A population-based study. Radiother. Oncol. 2017, 122, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Corradini, S.; Niyazi, M.; Niemoeller, O.M.; Li, M.; Roeder, F.; Eckel, R.; Schubert-Fritschle, G.; Scheithauer, H.R.; Harbeck, N.; Engel, J.; et al. Adjuvant radiotherapy after breast conserving surgery—A comparative effectiveness research study. Radiother. Oncol. 2015, 114, 28–34. [Google Scholar] [CrossRef] [PubMed]
- McGale, P.; Cutter, D.; Darby, S.C.; Henson, K.E.; Jagsi, R.; Taylor, C.W. Can observational data replace randomized trials? J. Clin. Oncol. 2016, 34, 3355–3356. [Google Scholar] [CrossRef] [PubMed]
- Giordano, S.H.; Kuo, Y.F.; Duan, Z.; Hortobagyi, G.N.; Freeman, J.; Goodwin, J.S. Limits of observational data in determining outcomes from cancer therapy. Cancer 2008, 112, 2456–2466. [Google Scholar] [CrossRef] [PubMed]
- Salas, M.; Hofman, A.; Stricker, B.H. Confounding by indication: An example of variation in the use of epidemiologic terminology. Am. J. Epidemiol. 1999, 149, 981–983. [Google Scholar] [CrossRef]


{kind=link}
| BCS Alone | BCS + RT | p-Value | |||
|---|---|---|---|---|---|
| n | (%) | n | (%) | ||
| All | 572 | (18.0) | 2599 | (82.0) | |
| Age at diagnosis | <0.001 | ||||
| 65–69 years | 141 | (24.7) | 1267 | (48.7) | |
| 70–75 years | 122 | (21.3) | 523 | (32.8) | |
| >75 years | 309 | (54.0) | 479 | (18.4) | |
| median (years) | 76.5 | 70.9 | |||
| Lateralisation | 0.799 | ||||
| right | 268 | (46.9) | 1233 | (47.4) | |
| left | 304 | (53.1) | 1366 | (52.6) | |
| Tumor size | <0.001 | ||||
| pTis | 116 | (20.3) | 176 | (6.8) | |
| pT1 | 239 | (41.8) | 1534 | (59.0) | |
| pT2 | 170 | (29.7) | 697 | (26.8) | |
| pT3 | 3 | (0.5) | 24 | (0.9) | |
| pT4 | 10 | (1.7) | 7 | (0.3) | |
| unknown/pTx | 34 | (5.9) | 161 | (6.2) | |
| Nodal status | <0.001 | ||||
| pN0 | 178 | (31.1) | 1584 | (60.9) | |
| pN1 | 64 | (11.2) | 506 | (19.5) | |
| pN2 | 17 | (3.0) | 83 | (3.2) | |
| pN3 | 6 | (1.0) | 35 | (1.3) | |
| unknow/pNx | 307 | (53.7) | 391 | (15.0) | |
| Grade | 0.709 | ||||
| G1 | 77 | (16.8) | 432 | (17.7) | |
| G2 | 276 | (60.4) | 1492 | (61.2) | |
| G3 | 104 | (22.8) | 515 | (21.1) | |
| Axillary surgery | <0.001 | ||||
| None | 289 | (50.5) | 246 | (9.5) | |
| ALND | 111 | (19.4) | 696 | (26.8) | |
| SNB + ALND | 49 | (8.6) | 408 | (15.7) | |
| SNB alone | 105 | (18.4) | 1139 | (43.8) | |
| other | 18 | (3.1) | 110 | (4.2) | |
| Resection status | <0.001 | ||||
| R0 | 425 | (70.7) | 2173 | (83.6) | |
| R1/R2 | 22 | (3.1) | 57 | (2.2) | |
| Rx | 125 | (26.2) | 369 | (14.2) | |
| Hormone receptor | 0.505 | ||||
| positive | 452 | (89.3) | 2298 | (90.3) | |
| negative | 54 | (10.7) | 247 | (9.7) | |
| Chemotherapy | <0.001 | ||||
| no | 534 | (93.4) | 2105 | (81.0) | |
| yes | 38 | (6.6) | 494 | (19.0) | |
| Endocrine therapy | <0.001 | ||||
| no | 358 | (62.6) | 1240 | (47.7) | |
| yes | 214 | (37.4) | 1359 | (52.3) | |
| <70 Years | 70–75 Years | >75 Years | p-Value | ||||
|---|---|---|---|---|---|---|---|
| n | (%) | n | (%) | n | (%) | ||
| All | 1155 | (43.0) | 815 | (30.4) | 714 | (26.6) | |
| Axillary surgery | <0.001 | ||||||
| yes | 1132 | (98.0) | 772 | (94.7) | 513 | (71.8) | |
| no | 23 | (2.0) | 43 | (5.3) | 201 | (28.2) | |
| Radiation Therapy | <0.001 | ||||||
| yes | 1072 | (92.8) | 744 | (91.3) | 446 | (62.5) | |
| none | 83 | (7.2) | 71 | (8.7) | 268 | (37.5) | |
| Chemotherapy | <0.001 | ||||||
| yes | 270 | (23.4) | 105 | (12.9) | 30 | (4.2) | |
| no | 885 | (76.6) | 710 | (87.1) | 684 | (95.8) | |
| Endocrine therapy | 0.238 | ||||||
| yes | 617 | (53.4) | 456 | (56.0) | 369 | (51.7) | |
| no | 538 | (46.6) | 359 | (44.0) | 345 | (48.3) | |
| Adjuvant therapy | <0.001 | ||||||
| ET alone | 26 | (2.3) | 28 | (3.4) | 138 | (19.3) | |
| ET + RT | 591 | (51.2) | 428 | (52.5) | 231 | (32.4) | |
| RT alone | 481 | (41.6) | 316 | (38.8) | 215 | (30.1) | |
| No adj. therapy | 57 | (4.9) | 43 | (5.3) | 130 | (18.2) | |
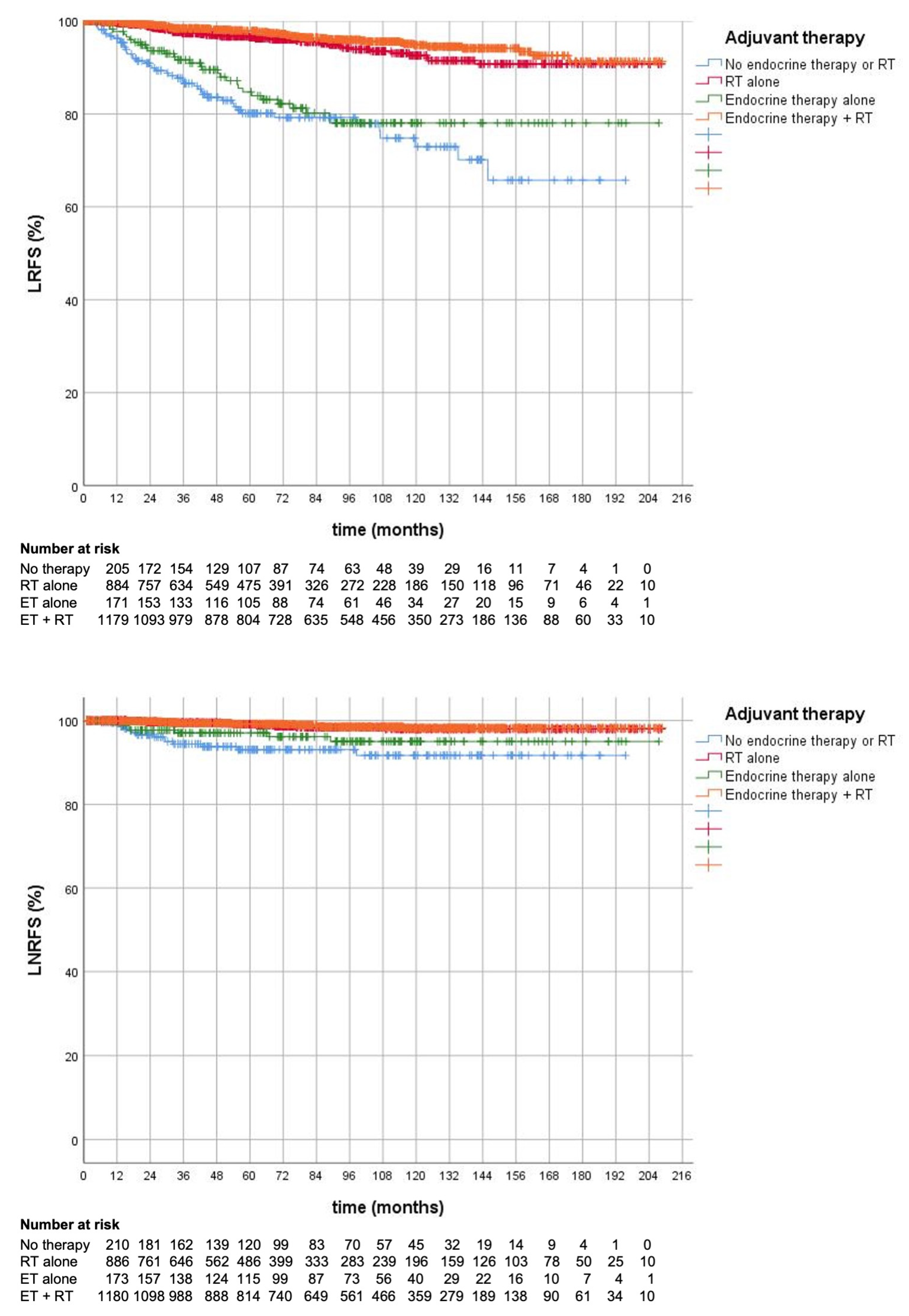
| 5 y (%) | 10 y (%) | p-Value | ||
|---|---|---|---|---|
| LRFS | ||||
| RT | BCS + RT | 97.3 | 94.0 | <0.001 |
| BCS alone | 81.8 | 75.1 | ||
| Adjuvant Therapy | ET alone | 84.7 | 78.1 | |
| ET + RT | 97.9 | 94.8 | <0.001 | |
| RT alone | 96.5 | 92.6 | <0.001 | |
| No adj. therapy | 80.1 | 72.9 | 0.240 | |
| LNRFS | ||||
| RT | BCS + RT | 99.2 | 98.1 | <0.001 |
| BCS alone | 94.9 | 93.1 | ||
| Adjuvant Therapy | ET alone | 97.0 | 95.0 | |
| ET + RT | 99.2 | 98.2 | 0.003 | |
| RT alone | 99.1 | 98.0 | 0.014 | |
| No adj. therapy | 93.0 | 91.6 | 0.215 | |
| DMFS | ||||
| BCS + RT | 93.5 | 89.0 | <0.001 | |
| BCS alone | 84.8 | 76.6 | ||
| Adjuvant Therapy | ET alone | 81.8 | 73.1 | |
| ET + RT | 93.0 | 88.3 | <0.001 | |
| RT alone | 94.4 | 90.2 | <0.001 | |
| No adj. therapy | 87.4 | 79.8 | 0.130 | |
| OS | ||||
| BCS + RT | 91.7 | 76.4 | <0.001 | |
| BCS alone | 71.2 | 39.3 | ||
| Adjuvant Therapy | ET alone | 69.3 | 36.0 | |
| ET + RT | 92.0 | 76.8 | <0.001 | |
| RT alone | 91.4 | 75.0 | <0.001 | |
| No adj. therapy | 72.8 | 41.7 | 0.383 |
| LRFS | LNRFS | DMRFS | OS | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p |
| Age | 0.507 | 0.156 | 0.012 | <0.001 | ||||||||
| <70 years | 1 | 1 | 1 | 1 | ||||||||
| 70–74 years | 1.135 | 0.706–1.826 | 2.462 | 0.985–6.154 | 1.213 | 0.841–1.750 | 1.726 | 1.339–2.224 | ||||
| ≥75 years | 1.338 | 0.820–2.183 | 1.717 | 0.608–4.853 | 1.824 | 1.226–2.715 | 3.513 | 2.702–4.568 | ||||
| Tumor size | 0.097 | <0.001 | <0.001 | <0.001 | ||||||||
| pT1 | 1 | 1 | 1 | 1 | ||||||||
| pT2 | 1.537 | 1.022–2.311 | 2.476 | 1.052–5.830 | 2.389 | 1.700–3.357 | 1.534 | 1.234–1.906 | ||||
| pT3–4 | 0.700 | 0.093–5.277 | 15.355 | 4.059–58.081 | 4.310 | 2.123–8.748 | 1.933 | 0.96–3.878 | ||||
| Nodal status | 0.156 | 0.132 | <0.001 | <0.001 | ||||||||
| pN0 | 1 | 1 | 1 | 1 | ||||||||
| pN+ (<3 LN) | 1.504 | 0.976–2.318 | 2.320 | 1.022–5.264 | 2.295 | 1.621–3.250 | 1.608 | 1.280–2.019 | ||||
| pN+ (≥4 LN) | 0.938 | 0.392–2.245 | 1.677 | 0.414–6.792 | 3.788 | 2.383–6.021 | 1.898 | 1.280–2.813 | ||||
| Grade | 0.219 | 0.474 | <0.001 | 0.001 | ||||||||
| 1 | 1 | 1 | 1 | 1 | ||||||||
| 2 | 1.499 | 0.796–2.821 | 0.838 | 0.229–3.070 | 1.376 | 0.759–2.494 | 1.195 | 0.877–1.628 | ||||
| 3 | 1.934 | 0.920–4.065 | 1.436 | 0.347–6.175 | 3.116 | 1.666–5.830 | 1.898 | 1.266–2.603 | ||||
| Resection status | 0.478 | 0.408 | 0.455 | 0.331 | ||||||||
| R0 | 1 | 1 | 1 | 1 | ||||||||
| R1/2 | 0.656 | 0.205–2.102 | 0.399 | 0.045–3.519 | 1.288 | 0.662–2.506 | 1.271 | 0.784–2.063 | ||||
| Hormone receptor status | 0.123 | 0.009 | 0.338 | 0.755 | ||||||||
| negative | 1 | 1 | 1 | 1 | ||||||||
| positive | 0.601 | 0.315–1.149 | 0.214 | 0.068–0.676 | 0.766 | 0.444–1.321 | 1.063 | 0.726–1.556 | ||||
| Radiotherapy | <0.001 | 0.008 | 0.042 | <0.001 | ||||||||
| no | 1 | 1 | 1 | 1 | ||||||||
| yes | 0.180 | 0.119–0.275 | 0.306 | 0.129–0.729 | 0.655 | 0.436–0.984 | 0.613 | 0.469–0.801 | ||||
| Chemotherapy | 0.091 | 0.102 | 0.627 | 0.611 | ||||||||
| no | 1 | 1 | 1 | 1 | ||||||||
| yes | 0.591 | 0.322–1.088 | 0.380 | 0.119–1.213 | 0.907 | 0.612–1.344 | 0.926 | 0.689–1.245 | ||||
| Endocrine Therapy | 0.125 | 0.819 | 0.240 | 0.010 | ||||||||
| no | 1 | 1 | 1 | 1 | ||||||||
| yes | 0.710 | 0.459–1.099 | 0.892 | 0.336–2.366 | 1.250 | 0.862–1.815 | 0.735 | 0.583–0.928 |
| BCS | |||
|---|---|---|---|
| Variable | OR | 95% CI | p-Value |
| Age | <0.001 | ||
| <70 years | 1 | ||
| 70–74 years | 1.001 | 0.665–1.506 | |
| ≥75 years | 0.310 | 0.215–0.446 | |
| Tumor size | 0.142 | ||
| pT1 | 1 | ||
| pT2 | 0.713 | 0.509–0.997 | |
| pT3-4 | 0.807 | 0.263–2.471 | |
| Nodal status | 0.002 | ||
| pN0 | 1 | ||
| pN+ (<3 LN) | 0.762 | 0.528–1.098 | |
| pN+ (≥4 LN) | 0.353 | 0.198–0.630 | |
| Grade | 0.274 | ||
| 1 | 1 | ||
| 2 | 0.751 | 0.474–1.190 | |
| 3 | 0.628 | 0.355–1.110 | |
| Resection status | 0.230 | ||
| R0 | 1 | ||
| R1/2 | 0.623 | 0.288–1.349 | |
| Hormone receptor status | 0.529 | ||
| negative | 1 | ||
| positive | 1.196 | 0.685–2.087 | |
| Chemotherapy | 0.001 | ||
| no | 1 | ||
| yes | 2.484 | 1.435–4.299 | |
| Endocrine Therapy | <0.001 | ||
| no | 1 | ||
| yes | 1.928 | 1.394–2.665 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rogowski, P.; Schönecker, S.; Konnerth, D.; Schäfer, A.; Pazos, M.; Gaasch, A.; Niyazi, M.; Boelke, E.; Matuschek, C.; Haussmann, J.; et al. Adjuvant Therapy for Elderly Breast Cancer Patients after Breast-Conserving Surgery: Outcomes in Real World Practice. Cancers 2023, 15, 2334. https://doi.org/10.3390/cancers15082334
Rogowski P, Schönecker S, Konnerth D, Schäfer A, Pazos M, Gaasch A, Niyazi M, Boelke E, Matuschek C, Haussmann J, et al. Adjuvant Therapy for Elderly Breast Cancer Patients after Breast-Conserving Surgery: Outcomes in Real World Practice. Cancers. 2023; 15(8):2334. https://doi.org/10.3390/cancers15082334
Chicago/Turabian StyleRogowski, Paul, Stephan Schönecker, Dinah Konnerth, Annemarie Schäfer, Montserrat Pazos, Aurélie Gaasch, Maximilian Niyazi, Edwin Boelke, Christiane Matuschek, Jan Haussmann, and et al. 2023. "Adjuvant Therapy for Elderly Breast Cancer Patients after Breast-Conserving Surgery: Outcomes in Real World Practice" Cancers 15, no. 8: 2334. https://doi.org/10.3390/cancers15082334
APA StyleRogowski, P., Schönecker, S., Konnerth, D., Schäfer, A., Pazos, M., Gaasch, A., Niyazi, M., Boelke, E., Matuschek, C., Haussmann, J., Braun, M., Pölcher, M., Würstlein, R., Harbeck, N., Belka, C., & Corradini, S. (2023). Adjuvant Therapy for Elderly Breast Cancer Patients after Breast-Conserving Surgery: Outcomes in Real World Practice. Cancers, 15(8), 2334. https://doi.org/10.3390/cancers15082334