
External Validation of the RETREAT Score for Prediction of Hepatocellular Carcinoma Recurrence after Liver Transplantation



Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Post-Transplant Follow-Up and Diagnosis of HCC Recurrence
2.3. Milan Criteria on Explant and RETREAT Score
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. HCC Recurrence
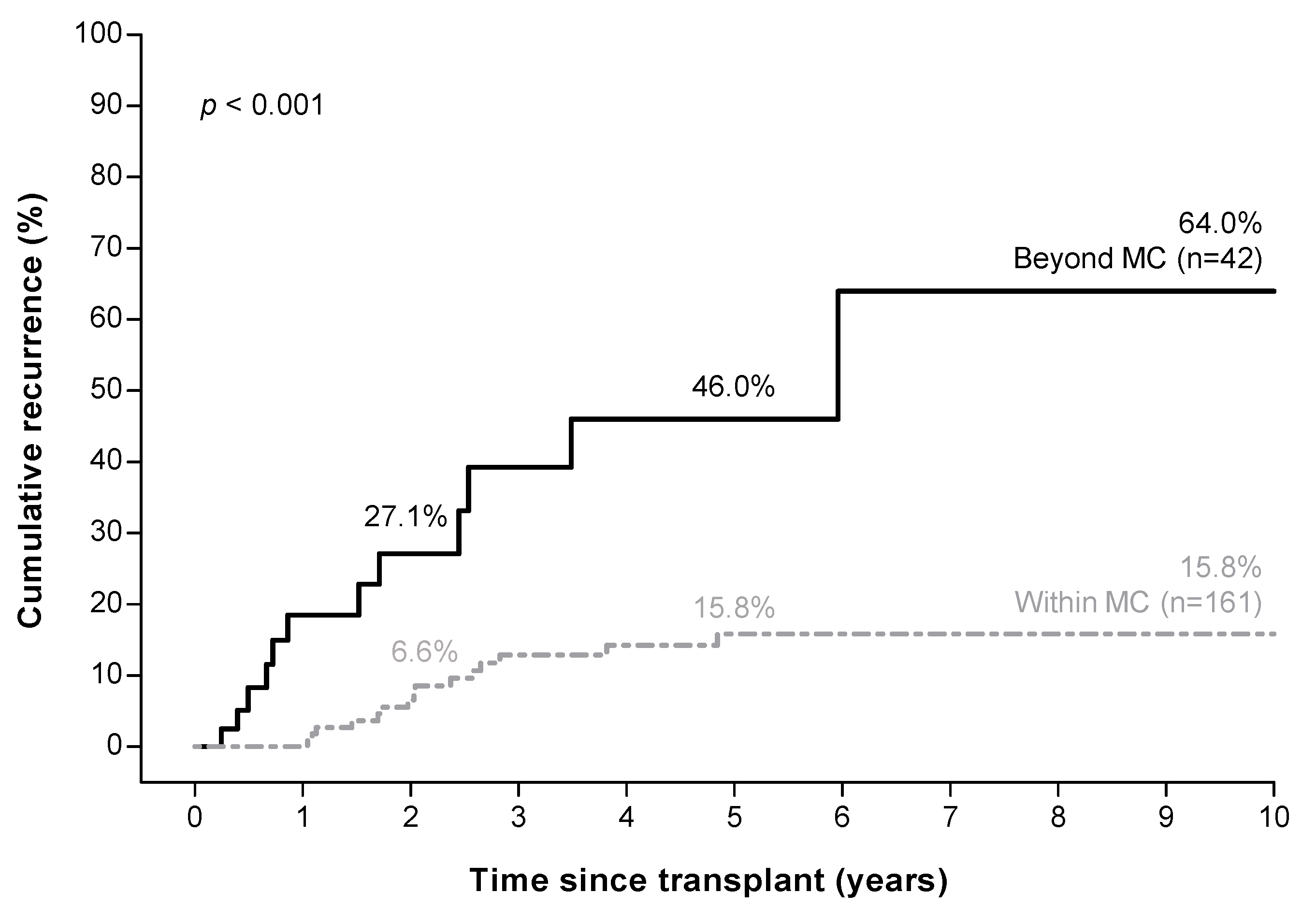
3.3. Higher Recurrence Rate in Patients beyond Milan Criteria on Explant
3.4. RETREAT Score Predicts HCC Recurrence
3.5. RETREAT Score Stratifies HCC Recurrence Risk in Patients within the Milan Criteria
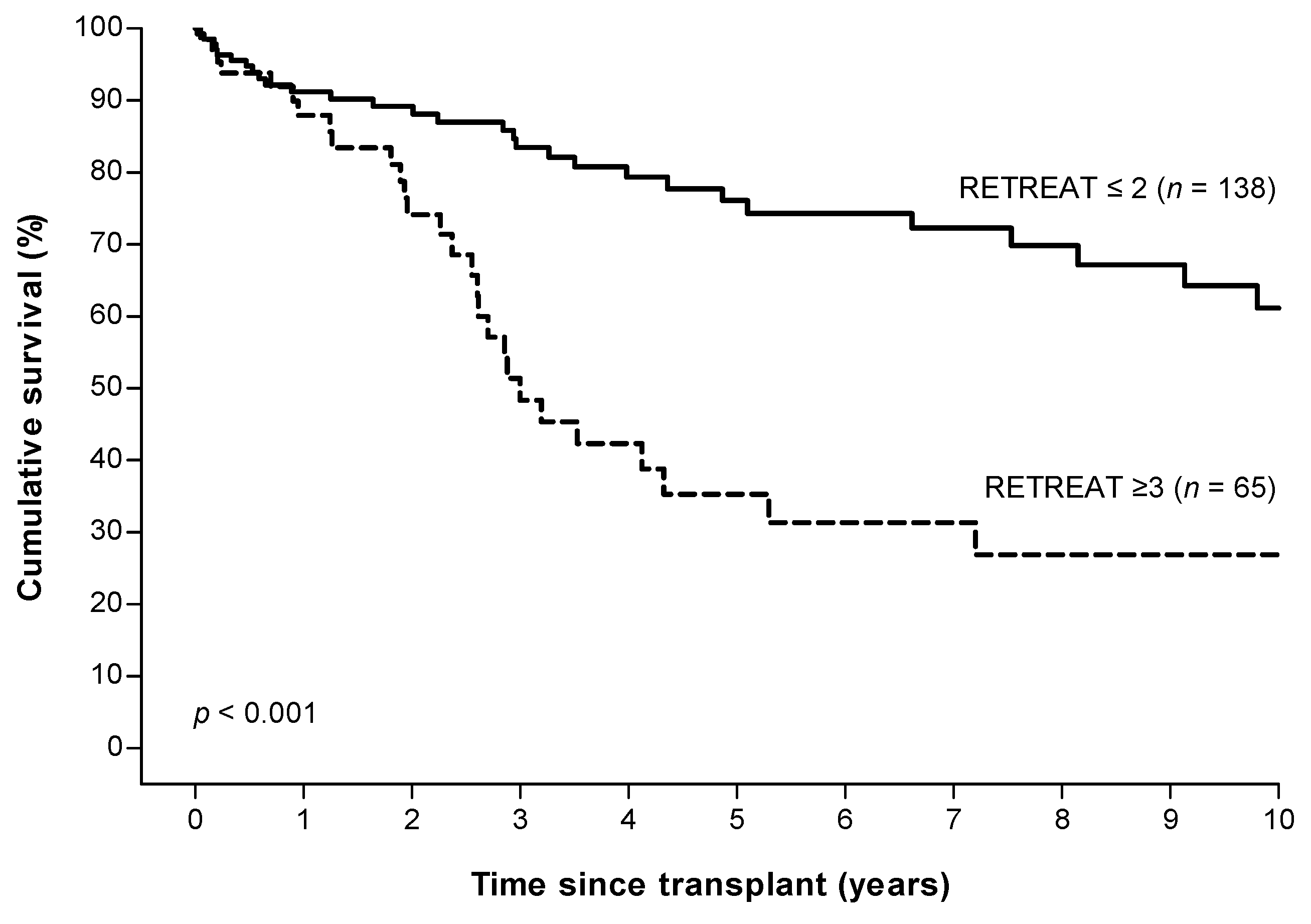
3.6. Overall Survival after Liver Transplantation Stratified by RETREAT
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Santopaolo, F.; Lenci, I.; Milana, M.; Manzia, T.M.; Baiocchi, L. Liver transplantation for hepatocellular carcinoma: Where do we stand? World J. Gastroenterol. 2019, 25, 2591–2602. [Google Scholar] [CrossRef] [PubMed]
- Clavien, P.A.; Lesurtel, M.; Bossuyt, P.M.; Gores, G.J.; Langer, B.; Perrier, A.; Group, O.L.T.f.H.C. Recommendations for liver transplantation for hepatocellular carcinoma: An international consensus conference report. Lancet Oncol. 2012, 13, e11–e22. [Google Scholar] [CrossRef] [Green Version]
- Mazzaferro, V.; Regalia, E.; Doci, R.; Andreola, S.; Pulvirenti, A.; Bozzetti, F.; Montalto, F.; Ammatuna, M.; Morabito, A.; Gennari, L. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N. Engl. J. Med. 1996, 334, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Filgueira, N.A. Hepatocellular carcinoma recurrence after liver transplantation: Risk factors, screening and clinical presentation. World J. Hepatol. 2019, 11, 261–272. [Google Scholar] [CrossRef] [PubMed]
- Bodzin, A.S.; Lunsford, K.E.; Markovic, D.; Harlander-Locke, M.P.; Busuttil, R.W.; Agopian, V.G. Predicting mortality in patients developing recurrent hepatocellular carcinoma after liver transplantation: Impact of treatment modality and recurrence characteristics. Ann. Surg. 2017, 266, 118–125. [Google Scholar] [CrossRef]
- de’Angelis, N.; Landi, F.; Carra, M.C.; Azoulay, D. Managements of recurrent hepatocellular carcinoma after liver transplantation: A systematic review. World J. Gastroenterol. 2015, 21, 11185–11198. [Google Scholar] [CrossRef]
- Sotiropoulos, G.C.; Molmenti, E.P.; Losch, C.; Beckebaum, S.; Broelsch, C.E.; Lang, H. Meta-analysis of tumor recurrence after liver transplantation for hepatocellular carcinoma based on 1198 cases. Eur. J. Med. Res. 2007, 12, 527–534. [Google Scholar]
- Pommergaard, H.C.; Burcharth, J.; Rosenberg, J.; Rasmussen, A. Serologic and molecular biomarkers for recurrence of hepatocellular carcinoma after liver transplantation: A systematic review and meta-analysis. Transplant. Rev. 2016, 30, 171–177. [Google Scholar] [CrossRef]
- Al-Ameri, A.A.M.; Wei, X.; Wen, X.; Wei, Q.; Guo, H.; Zheng, S.; Xu, X. Systematic review: Risk prediction models for recurrence of hepatocellular carcinoma after liver transplantation. Transplant. Int. 2020, 33, 697–712. [Google Scholar] [CrossRef]
- Mehta, N.; Heimbach, J.; Harnois, D.M.; Sapisochin, G.; Dodge, J.L.; Lee, D.; Burns, J.M.; Sanchez, W.; Greig, P.D.; Grant, D.R.; et al. Validation of a risk estimation of tumor recurrence after transplant (retreat) score for hepatocellular carcinoma recurrence after liver transplant. JAMA Oncol. 2017, 3, 493–500. [Google Scholar] [CrossRef]
- Mehta, N.; Dodge, J.L.; Roberts, J.P.; Yao, F.Y. Validation of the prognostic power of the retreat score for hepatocellular carcinoma recurrence using the unos database. Am. J. Transplant. 2018, 18, 1206–1213. [Google Scholar] [CrossRef] [PubMed]
- Hasan, B.; Colak, Y.; Khalid, R.A.; Castillo, M.; Castaneda, D.; Tandon, K.; Shaw, J.J.; Erim, T.; Zervos, X.B.; Castro, F.J.; et al. Early detection of hepatocellular carcinoma recurrence in the posttransplant population: A comparison of retreat and cleveland clinic florida scoring system. Transplant. Proc. 2021, 53, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Ma, K.W.; She, W.H.; Chan, A.C.Y.; Cheung, T.T.; Fung, J.Y.Y.; Dai, W.C.; Lo, C.M.; Chok, K.S.H. Validated model for prediction of recurrent hepatocellular carcinoma after liver transplantation in asian population. World J. Gastrointest. Oncol. 2019, 11, 322–334. [Google Scholar] [CrossRef] [PubMed]
- Reddy, S.H.S.; Mehta, N.; Dodge, J.L.; Hakeem, A.R.; Khorsandi, S.E.; Jassem, W.; Vilca-Melendez, H.; Cortes-Cerisuelo, M.; Srinivasan, P.; Prachalias, A.; et al. Liver transplantation for hcc: Validation of prognostic power of the retreat score for recurrence in a uk cohort. HPB 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Roayaie, S.; Schwartz, J.D.; Sung, M.W.; Emre, S.H.; Miller, C.M.; Gondolesi, G.E.; Krieger, N.R.; Schwartz, M.E. Recurrence of hepatocellular carcinoma after liver transplant: Patterns and prognosis. Liver Transplant. 2004, 10, 534–540. [Google Scholar] [CrossRef] [PubMed]
- Sapisochin, G.; Goldaracena, N.; Astete, S.; Laurence, J.M.; Davidson, D.; Rafael, E.; Castells, L.; Sandroussi, C.; Bilbao, I.; Dopazo, C.; et al. Benefit of treating hepatocellular carcinoma recurrence after liver transplantation and analysis of prognostic factors for survival in a large euro-american series. Ann. Surg. Oncol. 2015, 22, 2286–2294. [Google Scholar] [CrossRef] [PubMed]
- Villanueva, A. Hepatocellular carcinoma. N. Engl. J. Med. 2019, 380, 1450–1462. [Google Scholar] [CrossRef] [Green Version]
- European Association for the Study of the Liver. Electronic address, e.e.e. Easl clinical practice guidelines: Liver transplantation. J. Hepatol. 2016, 64, 433–485. [Google Scholar] [CrossRef]
- Aggarwal, A.; Te, H.S.; Verna, E.C.; Desai, A.P. A national survey of hepatocellular carcinoma surveillance practices following liver transplantation. Transplant. Direct 2021, 7, e638. [Google Scholar] [CrossRef]
- Herden, U.; Schoening, W.; Pratschke, J.; Manekeller, S.; Paul, A.; Linke, R.; Lorf, T.; Lehner, F.; Braun, F.; Stippel, D.L.; et al. Accuracy of pretransplant imaging diagnostic for hepatocellular carcinoma: A retrospective german multicenter study. Can. J. Gastroenterol. Hepatol. 2019, 2019, 8747438. [Google Scholar] [CrossRef] [Green Version]
- Pommergaard, H.C.; Rostved, A.A.; Adam, R.; Thygesen, L.C.; Salizzoni, M.; Gomez Bravo, M.A.; Cherqui, D.; Filipponi, F.; Boudjema, K.; Mazzaferro, V.; et al. Vascular invasion and survival after liver transplantation for hepatocellular carcinoma: A study from the european liver transplant registry. HPB 2018, 20, 768–775. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | n = 203 |
|---|---|
| Median follow up time (months) (IQR) | 26.8 (7.2–60.7) |
| Median age at LT (years), (IQR) | 61.2 (54.8–65.2) |
| Male sex, % | 162 (79.8) |
| Median waiting time to LT (months), (IQR) | 7.7 (3.8–10.8) |
| Median lab MELD Score on LT, (IQR) (n = 188) | 11 (8–15) |
| LRT pre LT a, % | 153 (75.4) |
| Resection pre LT, % | 17 (8.4) |
| RFA | 95 (46.8) |
| TACE/TARE | 71 (35.0) |
| MWA | 20 (9.9) |
| PEI | 5 (2.5) |
| ILC | 3 (1.5) |
| Stereotactic radiotherapy | 2 (1.0) |
| Etiology of liver disease, % | |
| Hepatitis B | 28 (13.8) |
| Hepatitis C | 42 (20.7) |
| NAFLD | 25 (12.3) |
| Alcoholic Liver Disease | 33 (16.3) |
| Others & cryptogenic liver disease | 48 (23.6) |
| Combined etiology | 26 (12.8) |
| Predictor | RETREAT Points | Overall (n = 203) (%) | Recurrence (n = 27) (%) | No Recurrence (n = 176) (%) |
|---|---|---|---|---|
| Last AFP pre LT (µg/L) | ||||
| 0–20 | 0 | 160 (78.8) | 15 (55.6) | 145 (82.4) |
| 21–99 | 1 | 19 (9.4) | 1 (3.7) | 18 (10.2) |
| 100–999 | 2 | 19 (9.4) | 7 (25.9) | 12 (6.8) |
| ≥1000 | 3 | 5 (2.5) | 4 (14.8) | 1 (0.6) |
| Microvascular invasion | 2 | 45 (22.2) | 16 (59.3) | 29 (16.5) |
| Largest viable tumor diameter (cm) plus number of viable tumors | ||||
| 0 * | 0 | 40 (19.7) | 0 (0.0) | 40 (22.7) |
| 1.1–4.9 | 1 | 105 (51.7) | 10 (37.0) | 95 (54.0) |
| 5.0–9.9 | 2 | 53 (26.1) | 14 (51.9) | 39 (22.2) |
| ≥10 | 3 | 5 (2.5) | 3 (11.1) | 2 (1.1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Hooff, M.C.; Sonneveld, M.J.; Ijzermans, J.N.; Doukas, M.; Sprengers, D.; Metselaar, H.J.; den Hoed, C.M.; de Man, R.A. External Validation of the RETREAT Score for Prediction of Hepatocellular Carcinoma Recurrence after Liver Transplantation. Cancers 2022, 14, 630. https://doi.org/10.3390/cancers14030630
van Hooff MC, Sonneveld MJ, Ijzermans JN, Doukas M, Sprengers D, Metselaar HJ, den Hoed CM, de Man RA. External Validation of the RETREAT Score for Prediction of Hepatocellular Carcinoma Recurrence after Liver Transplantation. Cancers. 2022; 14(3):630. https://doi.org/10.3390/cancers14030630
Chicago/Turabian Stylevan Hooff, Maria C., Milan J. Sonneveld, Jan N. Ijzermans, Michail Doukas, Dave Sprengers, Herold J. Metselaar, Caroline M. den Hoed, and Robert A. de Man. 2022. "External Validation of the RETREAT Score for Prediction of Hepatocellular Carcinoma Recurrence after Liver Transplantation" Cancers 14, no. 3: 630. https://doi.org/10.3390/cancers14030630
APA Stylevan Hooff, M. C., Sonneveld, M. J., Ijzermans, J. N., Doukas, M., Sprengers, D., Metselaar, H. J., den Hoed, C. M., & de Man, R. A. (2022). External Validation of the RETREAT Score for Prediction of Hepatocellular Carcinoma Recurrence after Liver Transplantation. Cancers, 14(3), 630. https://doi.org/10.3390/cancers14030630