1. Introduction
In recent decades, basal cell carcinoma (BCC) has progressed towards being the most frequently occurring type of skin cancer [
1,
2]. The diagnostic gold standard includes a biopsy or excision of the suspicious lesion and histopathological examination, resulting in a cost- and time-intensive process [
3,
4]. Treatment depends mainly on the histopathological subtype, with deep and nodular or infiltrating BCCs requiring a complete surgical excision, while superficial tumors can benefit from cryotherapy, lasers, or topical drugs such as imiquimod [
2,
3]. Therefore, the bedside diagnosis and subtyping of BCC are crucial for treatment planning. Clinical and dermoscopical examinations are commonly used in the daily clinical practice to diagnose BCCs, but non-invasive optical diagnostic methods, such as optical coherence tomography (OCT) and reflectance confocal microscopy (RCM), have shown a high potential in early detection of clinically unclear BCCs, with diagnostic sensitivity and specificity over 90% [
5,
6,
7]. Additionally, the new line-field confocal OCT (LC-OCT), with higher penetration depth than RCM (500 µm compared to 250 µm) and higher resolution than OCT (1 µm compared to 7.5–10 µm) [
8,
9], has recently been used to detect BCCs non-invasively according to morphological criteria in preliminary studies [
10,
11,
12]. However, there are no studies focused on clinically unclear lesions.
The aims of this study were: to verify in a real-life setting the diagnostic value of LC-OCT for clinically unclear BCC cases and to test for the ability to distinguish between superficial and other BCC subtypes, compared to dermoscopy and histopathology. Moreover, we reviewed morphological LC-OCT criteria for BCCs and provide an overview of the main diagnostic pitfalls.
2. Materials and Methods
This prospective study was performed at the Departments of Dermatology of the University of Munich and the University of Augsburg in Germany between November 2019 and February 2021. We prospectively recruited 182 clinically unclear lesions of 154 patients that were referred to our imaging departments from the general outpatient and inpatient departments and from external specialists in order to confirm or to rule out BCC prior to biopsy or excision. Clinical, dermoscopic (FotoFinder GmbH, Germany and Dermogenius-Dermoscan GmbH, Regensburg, Germany), and LC-OCT images of the cases were acquired and analyzed by two blinded imaging experts (CR, CG). Discordant cases were reviewed by a third expert (ES, SS, or JW). After the non-invasive imaging, surgical excision followed by histopathological examination was performed in all lesions.
For every case, the patient’s age, sex, and the anatomical site of the lesion were registered. Afterwards, dermoscopy was performed and a dermoscopic diagnosis was registered together with a confidence level ranging from 1 = high (>75% confidence) to 2 = intermediate (>50% confidence) to 3 = low (<50% confidence). Finally, the lesions were scanned with the LC-OCT device (DAMAE Medical, Paris), which uses a class 1 supercontinuum laser with a central wavelength of 800 nm to create various A-scans up to a depth of approximately 500 µm. Three imaging modalities are available: vertical or en-coupe, horizontal or en-face, and a 3D reconstruction either in a vertical or horizontal field of view. Details are described elsewhere [
8,
9].
The following features were registered: LC-OCT diagnosis, confidence, image quality, and whether LC-OCT could rule out a BCC diagnosis or not. LC-OCT image quality was scored from 1 (high: perfect image, no artefacts) to 2 (low: lower resolution, minor artefacts) to 3 (insufficient: major artefacts, unreadable). Confidence level was measured as described above for dermoscopy.
We calculated the frequency of the main descriptive morphological parameters used for the identification of BCCs in LC-OCT and their frequency as previously described in published studies [
11] (
Table 1). Key features useful for differentiating BCCs from non-BCCs and to differentiate between superficial BCC and other subtypes were identified by logistic regression.
To assess the LC-OCT performance, diagnostic accuracy, sensitivity, and specificity for BCCs compared to dermoscopy and to the gold standard histology were calculated using McNemar’s tests. Calculation was performed for all lesions and additionally in the subgroup of cases with a confidence level rated as “high” by at least one of the observers.
The study was approved by the ethical committee of the LMU Munich (Protocol Number 17-699).
3. Results
3.1. Population
A total of 182 lesions clinically suspicious for BCC in 154 patients were included in this study; 113 (62.1%) were confirmed histopathologically as BCCs and 69 (37.9%) as non-BCCs. The histopathological analysis entailed 35 (19.2%) completely excised lesions, 132 (72.5%) lesions acquired by punch biopsy, and 15 (8.2%) shave biopsies. Among the 113 BCCs, the nodular BCC subtype was seen most frequently in 52 (46%) lesions, followed by the superficial subtype in 35 (31%) and 4 (3.5%) infiltrative cases. Among the non-BCC cases, actinic keratosis (AK) was the most common diagnosis with a total of 24 lesions equaling a prevalence of 34.8%. Additional diagnoses included: squamous cell carcinoma (SCC), Bowen’s disease, nevus, melanoma, sebaceous hyperplasia, scar tissue/fibrous papule, dermatofibroma, lentigo solaris/seborrheic keratosis, eczema, clear cell acanthoma, molluscum contagiosum, trichoblastoma, angioma, atypical fibroxanthoma, and granuloma (
Figure 1,
Figure 2,
Figure 3,
Figure 4 and
Figure 5) (
Table 2).
3.2. Image Quality and Diagnostic Confidence
Average LC-OCT image quality was rated as high in 162 cases (89%) and as low in 20 cases (11%); no image was considered unreadable (image quality 3).
A high diagnostic confidence (1) by at least one observer was only scored in 48% of the dermoscopic images, compared to 70% of the LC-OCT cases. The interobserver agreement on the confidence level was very good. With LC-OCT, this was the case in 173 out of 182 (95%) of the observations (weighted kappa = 0.90 (95% CI, 8.84 to 0.97), p0). For dermoscopy, the number of interobserver agreements was 177 out of 182 (97.3%) observations (weighted kappa = 0.96 (95% CI, 0.92 to 0.99), p).
Our average diagnostic confidence with LC-OCT was 1.7; if we consider the subgroup of lesions with high image quality (1), we reported a confidence level of 1.1 (limbs) and 1.2 (head, trunk); in the subgroup of lesions with low image quality (2), diagnostic confidence sank to 2.3 (trunk), 2.5 (head), and 2.8 (limbs). Diagnostic confidence was therefore influenced by image quality but not by anatomical site.
3.3. Diagnostic Performance
Diagnostic accuracy of dermoscopy and LC-OCT for ruling out BCCs in suspicious lesions was 88% and 91%, respectively. Concerning sensitivity and specificity compared to the gold standard histology, dermoscopy scored a sensitivity of 90% and a specificity of 86%, while LC-OCT showed a high sensitivity (98%) and a good but lower specificity (80%). Sensitivity and specificity slightly increased when image quality was high, to 93% and 99%, respectively. If considering the subgroup of LC-OCT images with a high diagnostic confidence, however (70% of the lesions), the LC-OCT performance increased significantly, with a sensitivity of 100% and a specificity of 97% compared to the gold standard histology (p = 1, McNemar’s test).
In daily clinical practice, the combination of dermoscopy and LC-OCT enables the clinician to confidently make an almost perfect diagnosis at the bedside. The combination of both reaches an accuracy of 92.9% in all cases and an accuracy of 98.2% in confident cases, providing a certain security for the clinician and guiding further steps in the treatment process.
3.4. BCC Subtype
The diagnostic accuracy of LC-OCT for all BCC subtypes was 90%; we reported an overall sensitivity of 77% and a specificity of 96%. When only looking at cases with either a high LC-OCT quality (n = 101, 11% of the lesions) or lesions with a high LC-OCT confidence level (n = 93, 84% of the lesions), the performance of LC-OCT showed no significant difference to histology for all subtypes (
p > 0.05, McNemar’s test). Diagnostic accuracy, sensitivity, and specificity for each subtype were: superficial BCC, 90%, 77%, 96%; nodular BCC, 88%, 96%, 82%; mixed BCC, 90%, 67%, 96%. This values slightly increased when selecting only high image quality (
Table 3).
If we consider only pure BCC subtypes (86 lesions), the diagnostic accuracy increased to 92%. Sensitivity and specificity were for superficial BCCs 82% and 100%, for nodular BCCs 100% and 81%, and for fibrosing BCCs 75% and 100%, respectively.
3.5. Diagnostic Criteria
The following nine parameters were entered in the first model of the logistic regression: vertical parameters: hyperkeratosis, thinning of the epidermis, poorly defined DEJ, hyporeflective ovoid structures, dark rim/clefting; horizontal parameters: polarization of nuclei in the epidermis, palisading, clefting, and tumor nests. Through a backward elimination approach, non-significant parameters were removed one by one so that the three most impactful parameters to discriminate between BCC and non-BCC were: poorly defined DEJ, dark rim/clefting, and hyporeflective ovoid structures. These findings were in line with previous work [
10,
11].
Concerning BCC subtypes, following parameters were inserted in the logistic regression: thinning of the epidermis, shoal of fish pattern of the lobules, and string of pearls pattern of the lobules. After logistic regression, thinning of the epidermis and string of pearls were the most impactful key criteria to influence the distinction between superficial BCC and other BCC subtypes (
Figure 1,
Figure 2 and
Figure 3).
3.6. Other Diagnoses
With dermoscopy, 10 lesions were mistakenly classified as BCC: two AK, two sebaceous hyperplasias (
Figure 5), one Bowen’s disease, one SCC, one nevus, one dermatofibroma, one molluscum contagiosum (
Figure 1), and one pyogenic granuloma. Eleven BCCs were instead classified as: five SCC, two AK, one lentigo maligna/melanoma, one nevus, one scar, and one dermatofibroma. Using LC-OCT, we reported 14 false positive cases: eight AK, two seborrheic keratosis, one Bowen’s disease, one sebaceous hyperplasia, one molluscum contagiosum, and one pyogenic granuloma. Two cases of nodular BCCs were mistakenly diagnosed as a scar and an SCC.
Keratinocyte skin cancer (KC), consisting of actinic keratoses (AKs), squamous cell carcinoma (SCC), and Bowen carcinomas (BCs), made up 38 of the 182 suspicious lesions. The performance of LC-OCT differed on KC compared to BCCs, showing a change in sensitivity, specificity, and confidence. Compared to dermoscopy, LC-OCT was more specific but less sensitive (N = 182, McNemar’s p value = 0.02).
4. Discussion
In this study, we aimed to analyze the diagnostic performance of LC-OCT for BCCs among clinically unclear lesions, which can be missed with dermoscopy since they display unspecific patterns. We determined our diagnostic confidence and our diagnostic accuracy, sensitivity, and specificity in comparison to dermoscopy and to the gold standard histology. Being in a real-life setting, we also focused on our capability of distinguishing superficial BCCs from other subtypes using LC-OCT, since this has a direct influence on the choice of the therapy. Moreover, we tried to identify morphological criteria specific for BCC compared to other non-BCC differential diagnoses, which could be helpful to avoid unnecessary biopsies in the case of a benign diagnosis and to direct the patient to the correct therapeutic path in the case of malignant lesions other than BCC.
4.1. BCC Morphologic Criteria and Comparison with Histology
While clinical examination and dermoscopy are able to diagnose most clear-cut BCCs, equivocal lesions are a special target of non-invasive diagnostic techniques [
5]. To date, a few preliminary studies have described morphological criteria for diagnosing BCC using the novel device LC-OCT, with good histopathological correlations [
10,
11]. Suppa et al. examined 89 BCCs and described tumor lobules, with (in superficial BCCs) or without connection (in nodular BCCs) to the epidermis and branched lobules (in infiltrative BCCs). In our previous study [
11], we reported overlapping findings and defined, analogously to OCT terminology, the presence of a string of pearls pattern in superficial BCCs and of a shoal of fish pattern in infiltrative BCCs. Moreover, we reported an overall BCC subtype agreement between LC-OCT and histology of 90.4%, with a sensitivity of 82% and a specificity of 100% for superficial BCCs.
4.2. Diagnostic Accuracy, Sensitivity, and Specificity
Our diagnostic accuracy for BCCs was very high with both dermoscopy (88%) and LC-OCT (91%); compared to the gold standard histology, LC-OCT reached a high sensitivity (98%) but a slightly lower specificity (80%) in contrast to dermoscopy (86%).
Nevertheless, LC-OCT’s specificity was higher than shown in recent studies on the use of other diagnostic techniques: OCT (range: 73–75%) or RCM (range: 38–59%). Such tools have been used in similar studies to better characterize unclear lesions. Ulrich et al., for example, analyzed the sensitivity and specificity of OCT for the assisted diagnosis of non-pigmented BCC in a similar way in a previous observational study [
13]. The additional use of OCT resulted in a specificity of 75.3% (LC-OCT: 80%), a sensitivity of 95.7% (LC-OCT: 98%), and an accuracy of 87.4% (LC-OCT: 92.9%).
The combination of dermoscopy and LC-OCT reached, in our study, an accuracy of 92.9% in all cases and of 98.2% in confident cases, providing a certain security for the clinician and guiding further steps in the treatment process. Using both tools in clinical practice enables the clinician to confidently make a very accurate diagnosis at the bedside.
Dermoscopy alone scored a lower sensitivity (90%) than expected [
14]. This was probably due to the setting of clinically equivocal lesions, further supported by the fact that for only 48% of the lesions examined, the clinicians had a high level of confidence in their diagnosis with dermoscopy. This finding supports the fact that the enrolled lesions were equivocal. Our confidence improved markedly (70%) using LC-OCT.
Interestingly, if we consider only lesions with a high level of diagnostic confidence with LC-OCT (the majority), sensitivity and specificity values for the diagnosis of BCC reach those of the gold standard histology (100% and 97%, McNemar’s p value = 1).
4.3. Diagnostic Confidence
The abovementioned findings point out that the clinician can significantly increase diagnostic confidence after dermoscopy based on LC-OCT images and avoid a potentially unnecessary biopsy if reassured by high confidence (which was the case in most lesions in our study). The potential practical consequences are the reduction in pain and discomfort for the patient and surgery related costs and complications.
Our diagnostic confidence was not influenced by the anatomical site of the examined lesions, but was negatively influenced by the image quality. In fact, diagnostic confidence was significantly lower (1.2 vs. 2.5) in the subgroup of high vs. low image quality. This emphasizes the value of correct and standardized image acquisition protocols and required training for imaging performing personnel.
4.4. BCC Subtyping
After correctly diagnosing a BCC out of clinically equivocal lesions, the next step requires its classification into the superficial or non-superficial subtypes; in fact, a superficial BCC can be easily treated with topical drugs or further local treatments, while other more invasive subtypes should be referred to (micrographically controlled) surgery.
We identified the absence of the thinning of the epidermis and a string of pearls pattern with lobules connected to the DEJ as the most useful criteria for diagnosing superficial BCCs. The string of pearls pattern, present in 80% of our superficial BCCs, was described as hemispheric lobules (63%) or lobules connected to the epidermis (100%) in Suppa et al.’s findings. We demonstrated that we are able to use LC-OCT to distinguish between superficial and non-superficial BCC subtypes with high diagnostic accuracy. We reached a sensitivity and specificity for diagnosing superficial BCCs of 77% and 96%, respectively, increasing to 82% and 100% when considering only pure subtypes [
11].
Mixed BCC subtypes are a diagnostic challenge, since their components vary in their amount and can be easily missed. However, when nodular or fibrosing components are present, the BCC becomes a surgery candidate and should not be (except for very superficial nodular components) treated with less invasive methods. Therefore, superficial BCCs could be treated non-invasively after LC-OCT without histopathological examination.
For nodular BCC detection, LC-OCT showed the highest sensitivity with 100%, whereas specificity was highest for superficial (100%) and infiltrating (100%) BCCs. However, it needs to be mentioned that for the infiltrating BCC subtype, only a few lesions (n = 4) were collected in the real-life setting and the category classified as mixed subtype includes nodular superficial, nodular fibrosing, and other mixed subtypes. This may be seen as a limitation of this study.
Again, the performance of LC-OCT for all subtypes including mixed subtypes showed no significant difference to histology for all subtypes (p > 0.05, McNemar’s test) when only looking at cases with either a high LC-OCT quality (n = 101, 11% of the lesions) or lesions with a high LC-OCT confidence level (n = 93, 84% of the lesions).
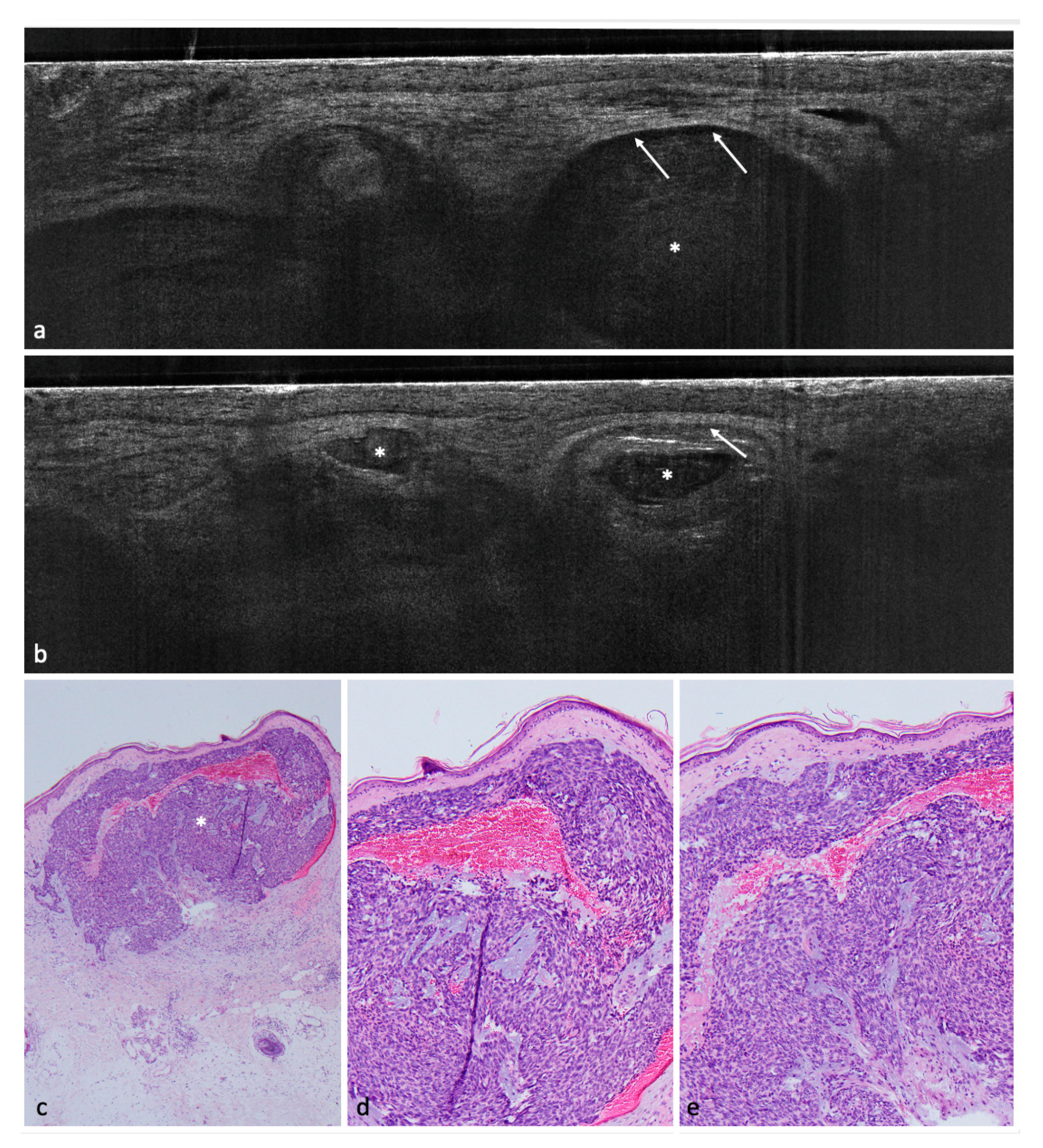
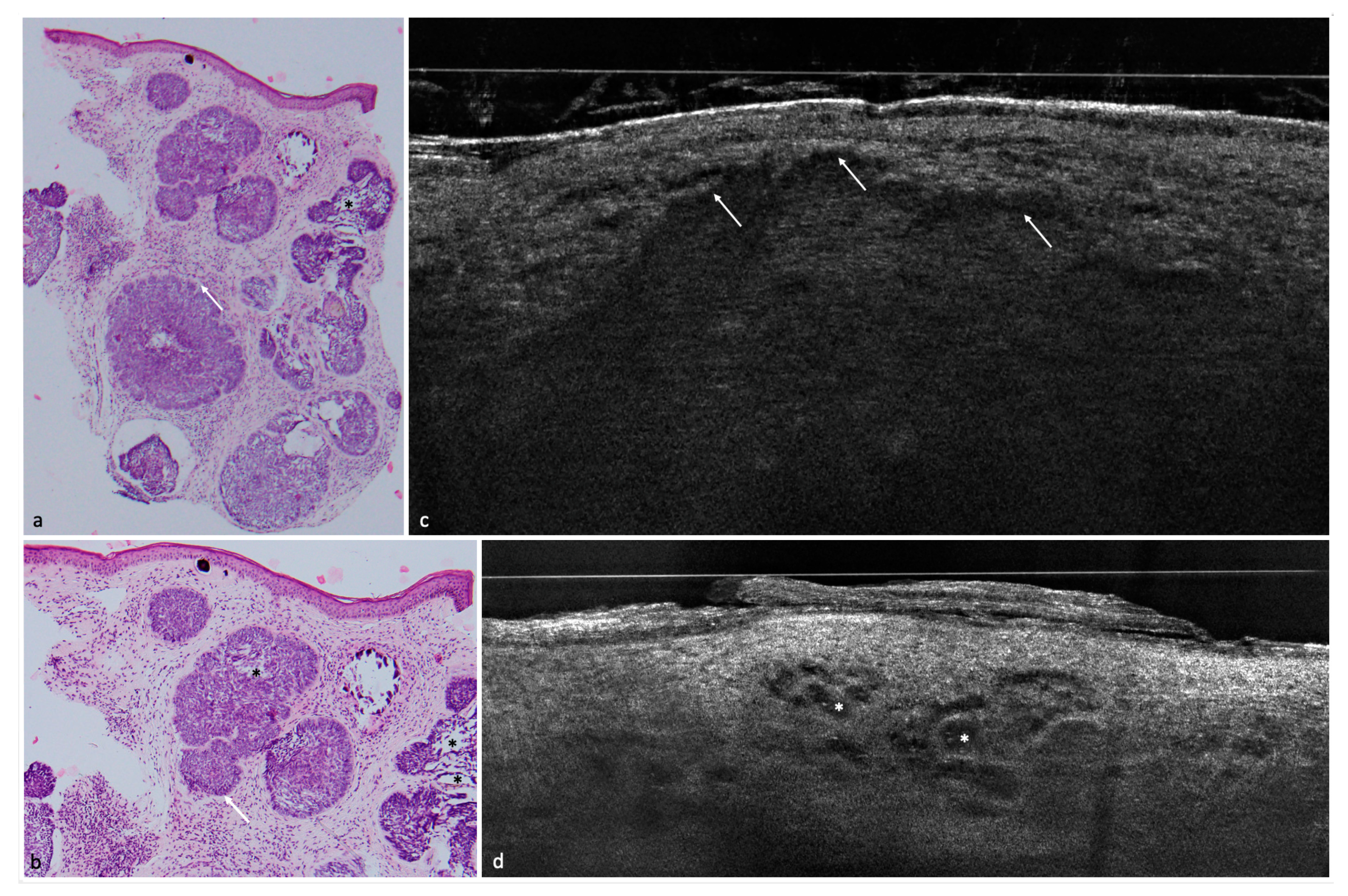
In a second step, we tried to identify with the help of logistic regressions a few key criteria able to distinguish between BCC and non-BCCs; these were: poorly defined DEJ, hyporeflective ovoid structures or nests/lobules (
Figure 3), and dark rim/clefting (
Figure 1). These criteria were consistent with previous findings [
10,
11].
4.5. Differential Diagnosis and Related Pitfalls
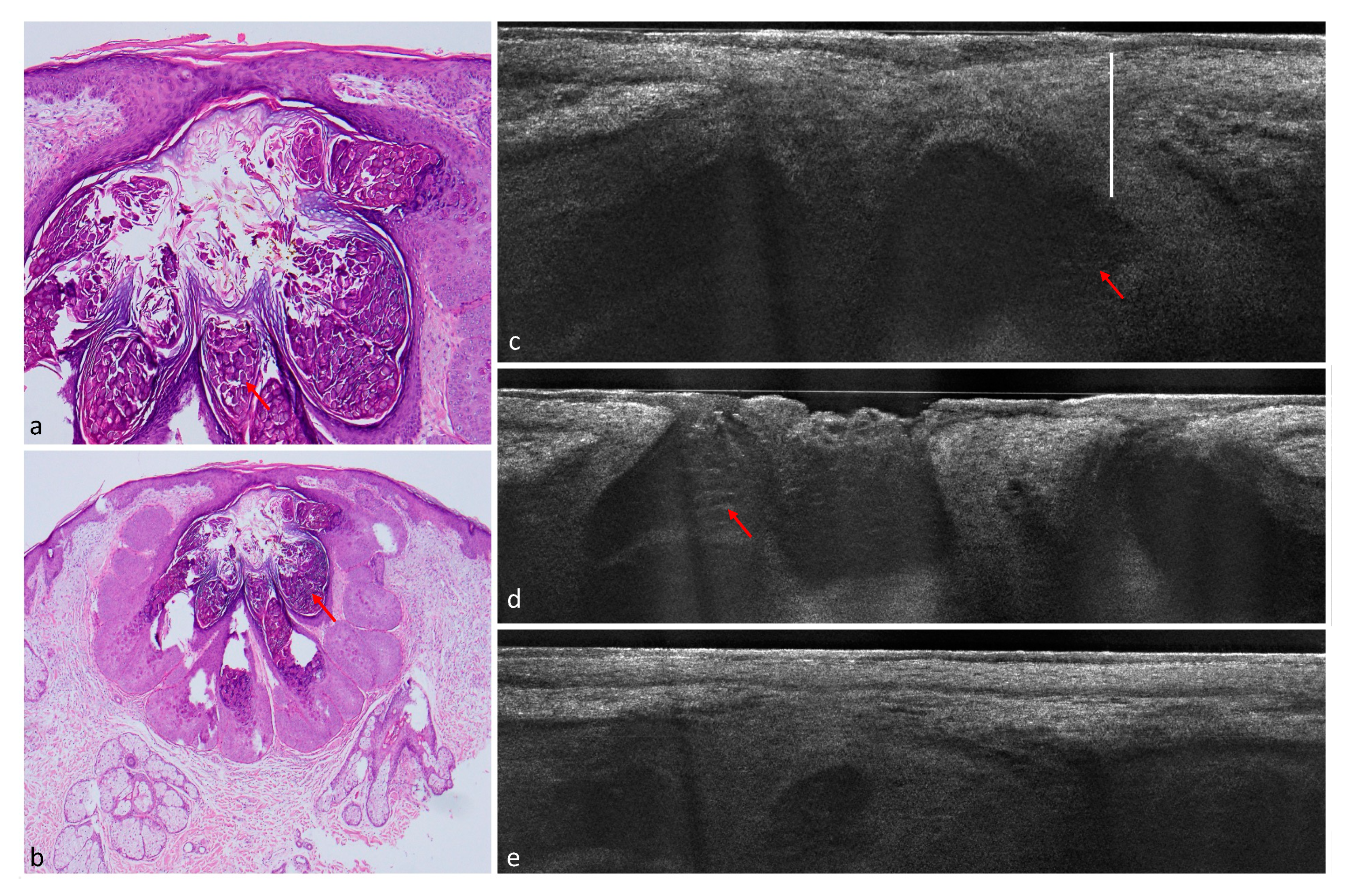
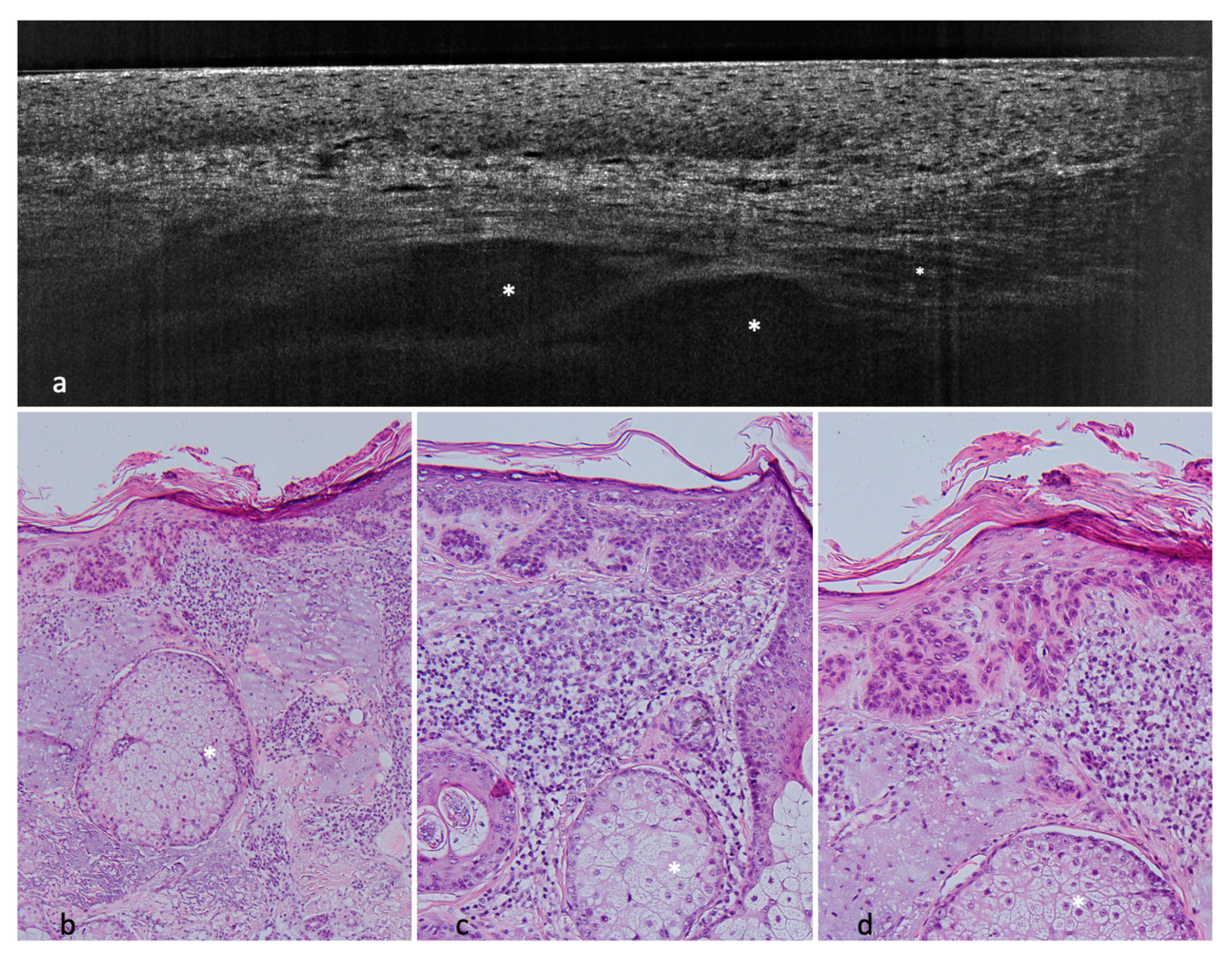
Although LC-OCT is a promising tool for the bedside differential diagnosis of BCC, there still remain pitfalls. Fourteen lesions (eight actinic keratosis, two lentigo solaris/seborrheic keratosis, one Bowen’s disease, one sebaceous hyperplasia, one molluscum contagiosum, one pyogenic granuloma) were misdiagnosed as BCCs.
The actinic keratosis belonged to the bowenoid subtype, causing a roundish contour of the epidermis with atypical keratinocytes that can be confounded with a string of pearls pattern. In this case, the expert observer should pay attention to the bright hyperkeratosis and continuity of the DEJ, Analogously, tumor lobules can be easily caused by granulomas, sebaceous lobules [
15], and even molluscum bodies [
16]. In such cases, the roundish or polycyclic dermal lobules are very well defined and sharply contoured, and usually contain brighter granular structures (
Figure 4: molluscum contagiosum,
Figure 5: sebaceous hyperplasia) or fibrotic–calcific tissue (granuloma). Furthermore, the DEJ is usually preserved and is overlined by a normal epidermis, which can, however, be thinned by the dermal structures. Sebaceous hyperplasia is also usually connected to hair follicles.
One case of BCC was misdiagnosed as a scar, probably due to the hyperreflective connective tissue masking the presence of tumor lobules, while another one was classified as an SCC due to the surrounding field cancerization in an elderly patient with hyperkeratosis, keratinocyte atypia, elastosis, and collagen alterations. For this reason, particular attention is needed in such patients when performing a bedside mapping of multiple suspicious lesions.
5. Conclusions
To sum up, we were able to reach a very good diagnostic confidence and performance in distinguishing BCCs from other BCC-suspicious lesions compared to dermoscopy and the gold standard histology. The study had limitations such as the small number of non-BCC lesions and the presence of only histologically confirmed lesions. Nevertheless, we believe LC-OCT is able to support the clinician in the process of diagnosing and subtyping BCC, as a key role to optimize the diagnostic approach and the treatment. It is particularly useful to screen BCCs in the context of clinically equivocal lesions, which can be difficult to diagnose with dermoscopy only. Moreover, it is possible to screen for superficial BCCs to be treated with less invasive methods than surgery. Larger studies on specific lesion subgroups such as facial papules are needed to gain more experience in this interesting field of dermatology.
Author Contributions
Conceptualization, J.W., C.R. and E.C.S.; methodology, J.W., C.R., E.C.S. and S.S.; validation, J.W., C.R., E.C.S., S.S. and D.H.; formal analysis, J.W., C.R., E.C.S., S.S., D.H., C.G. and F.D.; investigation, J.W., C.R., E.C.S., S.S., D.H., C.G. and F.D.; resources, C.R., E.C.S., J.W. and L.E.F.; data curation, C.R., S.S. and C.G.; writing—original draft preparation, C.G. and C.R.; writing—review and editing, E.C.S., S.S., D.H., C.G., C.R., F.D. and L.E.F.; supervision, J.W. and E.C.S.; project administration, J.W., C.R., E.C.S. and S.S.; funding acquisition, C.R. All authors have read and agreed to the published version of the manuscript.
Funding
The study was partially funded by the FöFoLe, a Funding program for research and teaching and Research Grant of the medical faculty of the Ludwig Maximilian University of Munich, protocol number 10-22.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of the LMU Munich (Protocol Number 17-699).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Fully anonymized data are available on motivated request.
Acknowledgments
The authors thank DAMAE Medical together with Maxime Cazalas and Melanie Pedrazzani for providing the device needed for this study and for their constant professional assistance.
Conflicts of Interest
The authors declare no relevant conflict of interest. The prototype of the LC-OCT device was made available for the study free of charge by DAMAE at both centers.
References
- Lomas, A.; Leonardi-Bee, J.; Bath-Hextall, F. A systematic review of worldwide incidence of nonmelanoma skin cancer. Br. J. Dermatol. 2012, 166, 1069–1080. [Google Scholar] [CrossRef] [PubMed]
- Peris, K.; Fargnoli, M.C.; Garbe, C.; Kaufmann, R.; Bastholt, L.; Seguin, N.B.; Bataille, V.; Marmol, V.D.; Dummer, R.; Harwood, C.A.; et al. Diagnosis and treatment of basal cell carcinoma: European consensus-based interdisciplinary guidelines. Eur. J. Cancer 2019, 118, 10–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, B.M.; Balermpas, P.; Bauer, A.; Blum, A.; Brölsch, G.F.; Dirschka, T.; Follmann, M.; Frank, J.; Frerich, B.; Fritz, K.; et al. S2k Guidelines for Cutaneous Basal Cell Carcinoma—Part 2: Treatment, Prevention and Follow-up. J. Dtsch. Dermatol. Ges. 2019, 17, 214–230. [Google Scholar] [CrossRef] [PubMed]
- Heppt, M.V.; Leiter, U.; Steeb, T.; Amaral, T.; Bauer, A.; Becker, J.C.; Breitbart, E.; Breuninger, H.; Diepgen, T.; Dirschka, T.; et al. S3 guideline for actinic keratosis and cutaneous squamous cell carcinoma—Short version, part 1: Diagnosis, interventions for actinic keratoses, care structures and quality-of-care indicators. J. Dtsch. Dermatol. Ges. 2020, 18, 275–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrante di Ruffano, L.; Dinnes, J.; Deeks, J.J.; Chuchu, N.; Bayliss, S.E.; Davenport, C.; Takwoingi, Y.; Godfrey, K.; O’Sullivan, C.; Matin, R.N.; et al. Optical coherence tomography for diagnosing skin cancer in adults. Cochrane Database Syst. Rev. 2018, 12, Cd013189. [Google Scholar] [CrossRef] [PubMed]
- Dinnes, J.; Deeks, J.J.; Chuchu, N.; Saleh, D.; Bayliss, S.E.; Takwoingi, Y.; Davenport, C.; Patel, L.; Matin, R.N.; O’Sullivan, C.; et al. Reflectance confocal microscopy for diagnosing keratinocyte skin cancers in adults. Cochrane Database Syst. Rev. 2018, 12, Cd013191. [Google Scholar] [CrossRef] [PubMed]
- Longo, C.; Lallas, A.; Kyrgidis, A.; Rabinovitz, H.; Moscarella, E.; Ciardo, S.; Zalaudek, I.; Oliviero, M.; Losi, A.; Gonzalez, S.; et al. Classifying distinct basal cell carcinoma subtype by means of dermatoscopy and reflectance confocal microscopy. J. Am. Acad. Dermatol. 2014, 71, 716–724.e711. [Google Scholar] [CrossRef] [PubMed]
- Ogien, J.; Levecq, O.; Azimani, H.; Dubois, A. Dual-mode line-field confocal optical coherence tomography for ultrahigh-resolution vertical and horizontal section imaging of human skin. Biomed. Opt. Express 2020, 11, 1327–1335. [Google Scholar] [CrossRef] [PubMed]
- Dubois, A.; Xue, W.; Levecq, O.; Bulkin, P.; Coutrot, A.L.; Ogien, J. Mirau-based line-field confocal optical coherence tomography. Opt. Express 2020, 28, 7918–7927. [Google Scholar] [CrossRef]
- Suppa, M.; Fontaine, M.; Dejonckheere, G.; Cinotti, E.; Yelamos, O.; Diet, G.; Tognetti, L.; Miyamoto, M.; Orte Cano, C.; Perez-Anker, J.; et al. Line-field confocal optical coherence tomography of basal cell carcinoma: A descriptive study. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 1099–1110. [Google Scholar] [CrossRef] [PubMed]
- Ruini, C.; Schuh, S.; Gust, C.; Kendziora, B.; Frommherz, L.; French, L.E.; Hartmann, D.; Welzel, J.; Sattler, E. Line-field optical coherence tomography: In vivo diagnosis of basal cell carcinoma subtypes compared to histopathology. Clin. Exp. Dermatol. 2021, 46, 1471–1481. [Google Scholar] [CrossRef]
- Ruini, C.; Schuh, S.; Sattler, E.; Welzel, J. Line-field confocal optical coherence tomography-Practical applications in dermatology and comparison with established imaging methods. Ski. Res. Technol. 2021, 27, 340–352. [Google Scholar] [CrossRef]
- Ulrich, M.; von Braunmuehl, T.; Kurzen, H.; Dirschka, T.; Kellner, C.; Sattler, E.; Berking, C.; Welzel, J.; Reinhold, U. The sensitivity and specificity of optical coherence tomography for the assisted diagnosis of nonpigmented basal cell carcinoma: An observational study. Br. J. Dermatol. 2015, 173, 428–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altamura, D.; Menzies, S.W.; Argenziano, G.; Zalaudek, I.; Soyer, H.P.; Sera, F.; Avramidis, M.; DeAmbrosis, K.; Fargnoli, M.C.; Peris, K. Dermatoscopy of basal cell carcinoma: Morphologic variability of global and local features and accuracy of diagnosis. J. Am. Acad. Dermatol. 2010, 62, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Lenoir, C.; Diet, G.; Cinotti, E.; Tognetti, L.; Orte Cano, C.; Rocq, L.; Trepant, A.L.; Monnier, J.; Perez-Anker, J.; Rubegni, P.; et al. Line-field confocal optical coherence tomography of sebaceous hyperplasia: A case series. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e509–e511. [Google Scholar] [CrossRef] [PubMed]
- Verzi, A.E.; Micali, G.; Lacarrubba, F. Line-field confocal optical coherence tomography in molluscum contagiosum: A case series. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e934–e936. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}