
Expression of Membranous CD155 Is Associated with Aggressive Phenotypes and a Poor Prognosis in Patients with Bladder Cancer

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Data Collection
2.2. Immunohistochemistry for CD155
2.3. Statistical Analyses
3. Results
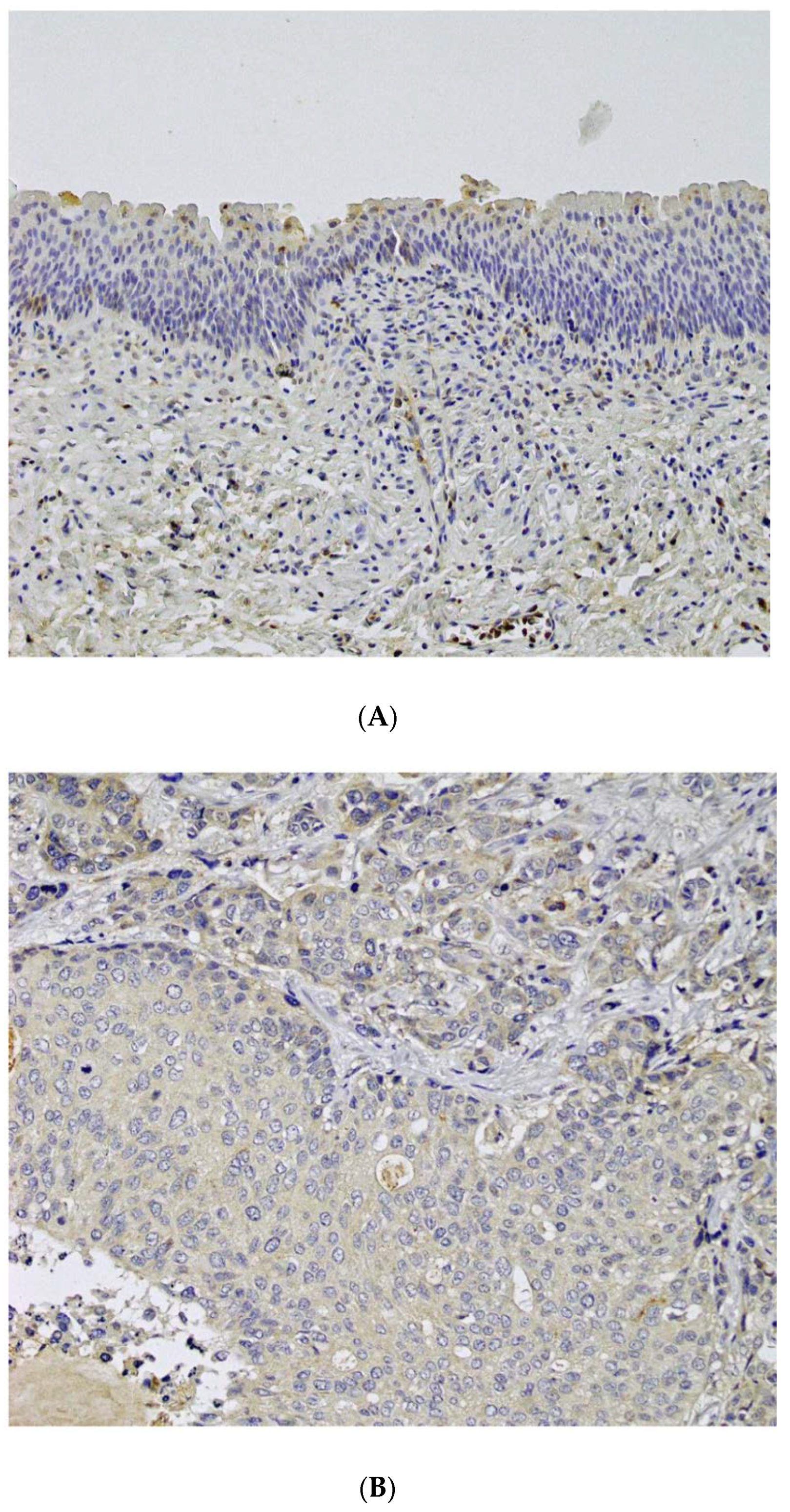
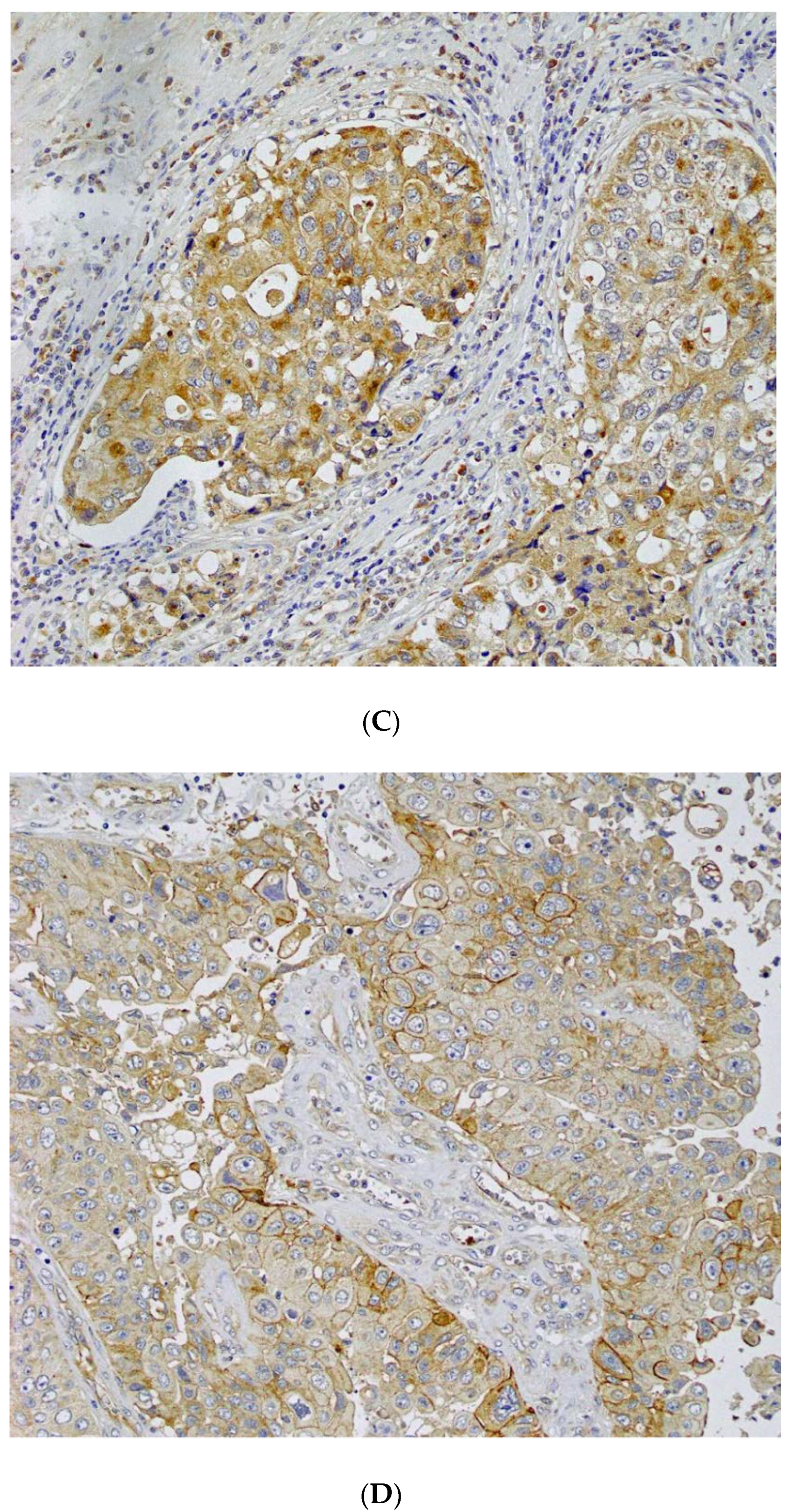
3.1. Immunohistochemistry Analysis of CD155
3.2. Association of Clinicopathological Characteristics with CD155 Expression
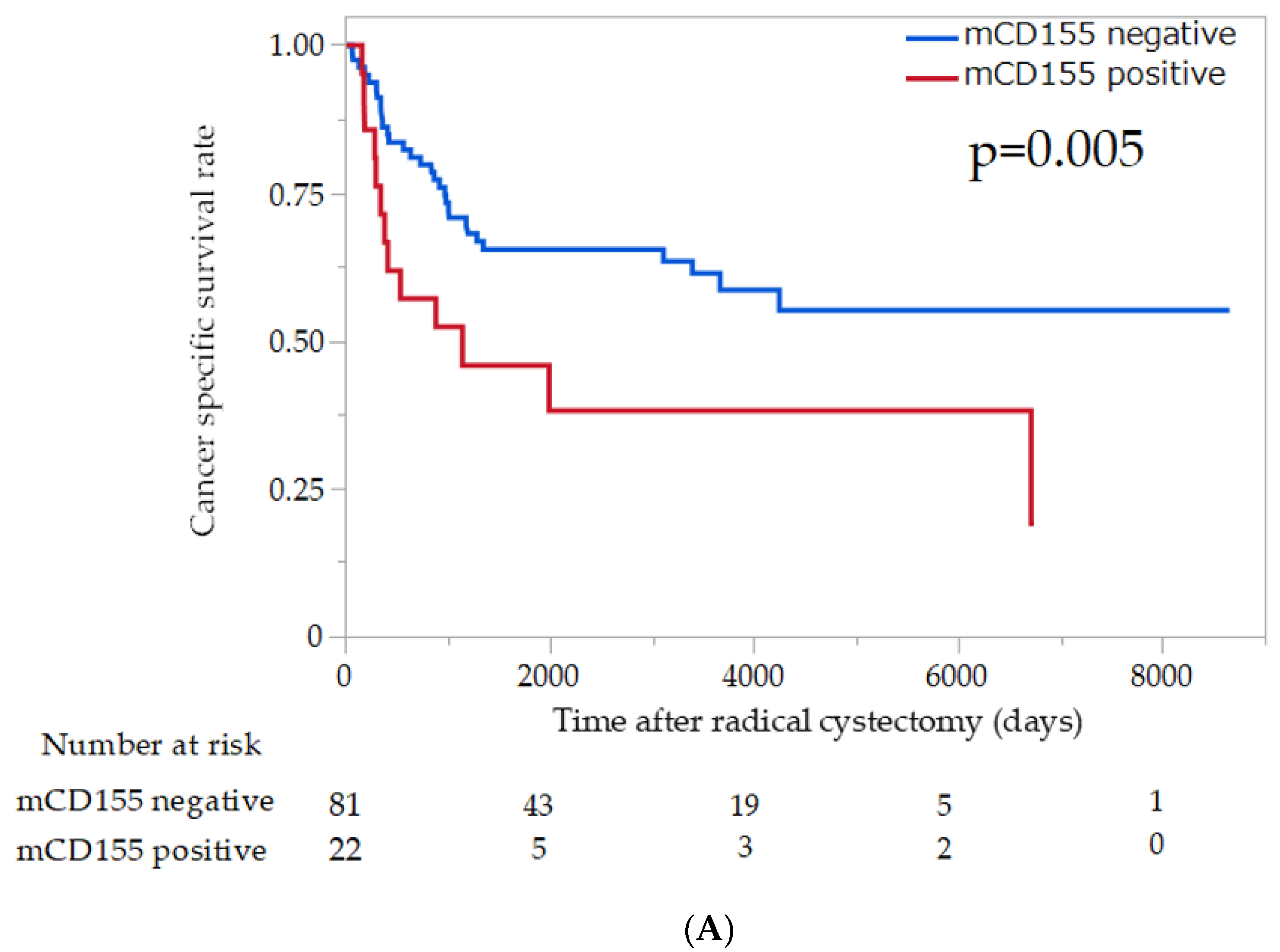
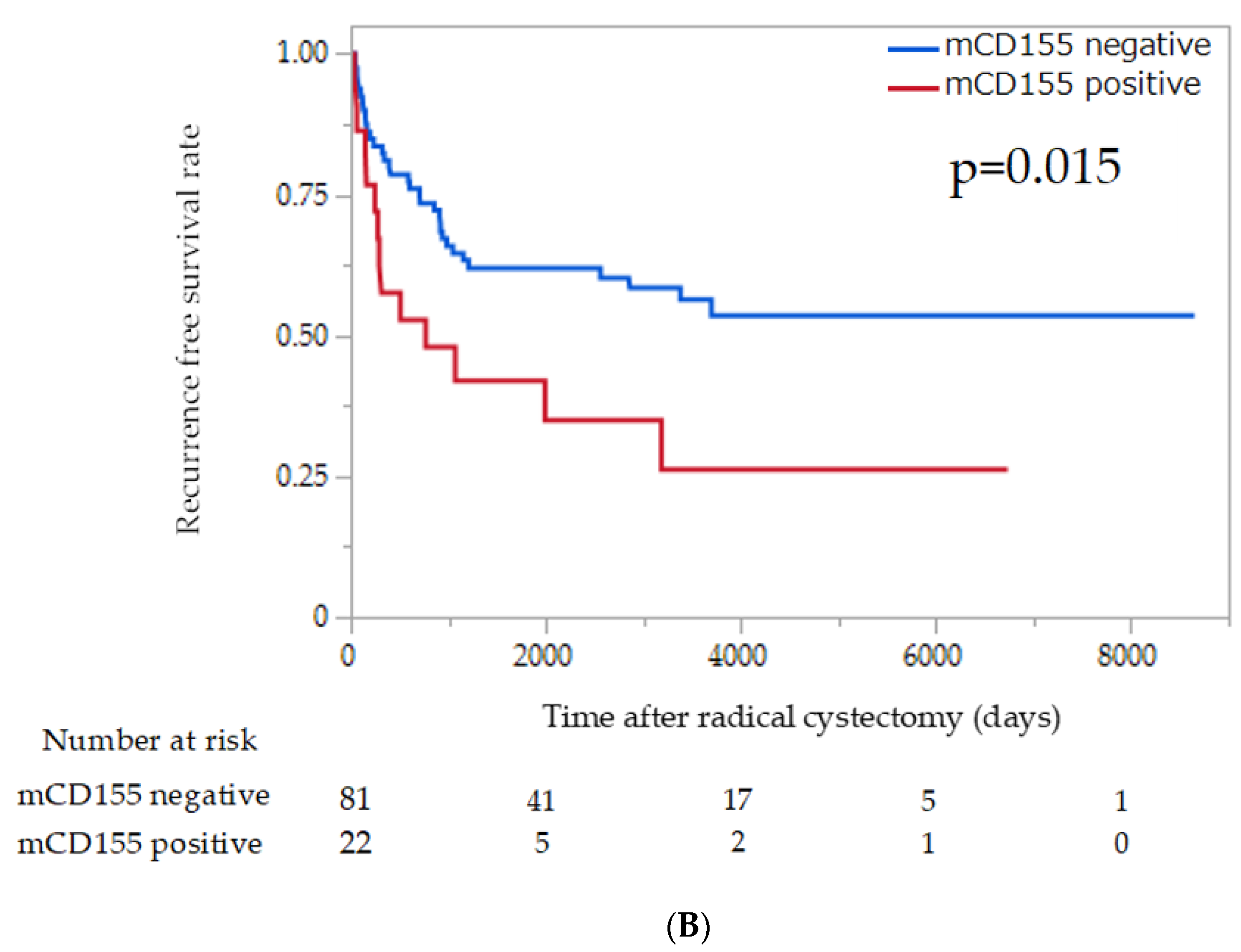
3.3. Association of Survival Outcomes with CD155 Expression
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antoni, S.; Ferlay, J.; Soerjomataram, I.; Znaor, A.; Jemal, A.; Bray, F. Bladder Cancer Incidence and Mortality: A Global Overview and Recent Trends. Eur. Urol. 2017, 71, 96–108. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, K.; Tabata, K.; Hirayama, T.; Shimura, S.; Nishi, M.; Fujita, T.; Iwamura, M. Robot-assisted laparoscopic radical cystectomy is a safe and effective procedure for patients with bladder cancer compared to laparoscopic and open surgery: Perioperative outcomes of a single-center experience. Asian J. Surg. 2019, 42, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Xylinas, E.; Cha, E.K.; Sun, M.; Rink, M.; Trinh, Q.D.; Novara, G.; Green, D.A.; Pycha, A.; Fradet, Y.; Daneshmand, S.; et al. Risk stratification of pT1-3N0 patients after radical cystectomy for adjuvant chemotherapy counselling. Br. J. Cancer. 2012, 107, 1826–1832. [Google Scholar] [CrossRef] [Green Version]
- Oughton, J.B.; Poad, H.; Twiddy, M.; Collinson, M.; Hiley, V.; Gordon, K.; Jhonson, M.; Jain, S.; Noon, A.P.; Chahal, R.; et al. Radical cystectomy (bladder removal) against intravesical BCG immunotherapy for high-risk non-muscle invasive bladder cancer (BRAVO): A protocol for a randomised controlled feasibility study. BMJ Open 2017, 7, e017913. [Google Scholar] [CrossRef]
- Bajorin, D.F.; Witjes, J.A.; Gschwend, J.E.; Schenker, M.; Valderrama, B.P.; Tomita, Y.; Bamias, Y.; Lebret, T.; Shariat, S.F.; Park, S.H.; et al. Adjuvant Nivolumab versus Placebo in Muscle-Invasive Urothelial Carcinoma. N. Engl. J. Med. 2021, 384, 2102–2114. [Google Scholar] [CrossRef]
- Yong, H.; Cheng, R.; Li, X.; Gao, G.; Jiang, X.; Cheng, H.; Zhou, X.; Zhao, W. CD155 expression and its prognostic value in postoperative patients with breast cancer. Biomed. Pharmacother. 2019, 115, 108884. [Google Scholar] [CrossRef]
- Zheng, Q.; Gao, J.; Yin, P.; Wang, W.; Wang, B.; Li, Y.; Zhao, C. CD155 contributes to the mesenchymal phenotype of triple-negative breast cancer. Cancer Sci. 2020, 111, 383–394. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Luo, J.; Chen, Y.; Cui, J.; Lei, Y.; Cui, Y.; Jiang, N.; Jiang, W.; Chen, L.; Chen, Y.; et al. Combined evaluation of the expression status of CD155 and TIGIT plays an important role in the prognosis of LUAD (lung adenocarcinoma). Int. Immunopharmacol. 2020, 80, 106198. [Google Scholar] [CrossRef]
- Nakai, R.; Maniwa, Y.; Tanaka, Y.; Nishio, W.; Yoshimura, M.; Okita, Y.; Onbayashi, C.; Satoh, N.; Ogita, H.; Takai, Y.; et al. Overexpression of Necl-5 correlates with unfavorable prognosis in patients with lung adenocarcinoma. Cancer Sci. 2010, 101, 1326–1330. [Google Scholar] [CrossRef]
- Smazynski, J.; Hamilton, P.T.; Thornton, S.; Miline, K.; Wouters, M.C.A.; Webb, J.R.; Nelson, B.H. The immune suppressive factors CD155 and PD-L1 show contrasting expression patterns and immune correlates in ovarian and other cancers. Gynecol. Oncol. 2020, 158, 167–177. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Ma, J.; Lei, T.; Ma, W.; Zhang, M. The bispecific anti-CD3 × anti-CD155 antibody mediates T cell immunotherapy for human prostate cancer. Investig. New Drugs 2019, 37, 810–817. [Google Scholar] [CrossRef] [PubMed]
- Okumura, G.; Iguchi-Manaka, A.; Murata, R.; Yamashita-Kanemaru, Y.; Shibuya, A.; Shibuya, K. Tumor-derived soluble CD155 inhibits DNAM-1-mediated antitumor activity of natural killer cells. J. Exp. Med. 2020, 217, e20191290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, L.; Gai, J.; Qiao, P.; Li, Y.; Li, X.; Zhu, M.; Li, G.; Wan, Y. A Novel Bispecific Nanobody with PD-L1/TIGIT Dual Immune Checkpoint Blockade. Biochem. Biophys. Res. Commun. 2020, 531, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Mao, L.; Xiao, Y.; Yang, Q.C.; Yang, S.C.; Yang, L.L.; Sun, Z.J. TIGIT/CD155 Blockade Enhances Anti-PD-L1 Therapy in Head and Neck Squamous Cell Carcinoma by Targeting Myeloid-Derived Suppressor Cells. Oral Oncol. 2021, 121, 105472. [Google Scholar] [CrossRef] [PubMed]
- Murakami, Y.; Matsumoto, K.; Shimizu, Y.; Ikeda, M.; Amano, N.; Shimura, S.; Ishii, D.; Sato, Y.; Iwamura, M. PD-L1 expression in tumor-infiltrating lymphocytes (TILs) as an independent predictor of prognosis in patients with pN0 bladder cancer undergoing radical cystectomy. Urol. Oncol. 2020, 39, 195.e15–195.e23. [Google Scholar] [CrossRef]
- Mendelsohn, C.L.; Wimmer, E.; Racaniello, V.R. Cellular receptor for poliovirus: Molecular cloning, nucleotide sequence, and expression of a new member of the immunoglobulin superfamily. Cell 1989, 56, 855–865. [Google Scholar] [CrossRef]
- Luo, C.; Ye, W.; Hu, J.; Othmance, B.; Li, H.; Chen, J.; Zu, X. A Poliovirus Receptor (CD155)-Related Risk Signature Predicts the Prognosis of Bladder Cancer. Front Oncol. 2021, 11, 660273. [Google Scholar] [CrossRef]
- Zhang, J.; Zhu, Y.; Wang, Q.; Kong, Y.; Guo, J.; Xu, J.; Dai, B. Poliovirus receptor CD155 is up-regulated in muscle-invasive bladder cancer and predicts poor prognosis. Urol. Oncol. 2020, 38, 41.e11–41.e18. [Google Scholar] [CrossRef]
- Minami, Y.; Ikeda, W.; Kajita, M.; Fujito, T.; Amano, H.; Tamaru, Y.; Kuramitsu, K.; Sakamoto, Y.; Monden, M.; Takai, Y. Necl-5/poliovirus receptor interacts in cis with integrin alphaVbeta3 and regulates its clustering and focal complex formation. J. Biol. Chem. 2007, 282, 18481–18496. [Google Scholar] [CrossRef] [Green Version]
- Kakunaga, S.; Ikeda, W.; Shingai, T.; Fujito, T.; Yamada, A.; Minami, Y.; Imai, T.; Takai, Y. Enhancement of serum- and platelet-derived growth factor-induced cell proliferation by Necl-5/Tage4/poliovirus receptor/CD155 through the Ras-Raf-MEK-ERK signaling. J. Biol. Chem. 2004, 279, 36419–36425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, R.B.; Li, Y.C.; Zhou, Q.; Lv, S.Z.; Yuan, K.Y.; Wu, J.P.; Zhao, Y.J.; Song, Q.K.; Zhu, B. Overexpression of CD155 is associated with PD-1 and PD-L1 expression on immune cells, rather than tumor cells in the breast cancer microenvironment. World J. Clin. Cases 2020, 8, 5935–5943. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Guo, Q.; Fu, H.; Yu, J.; Wang, L.; Sun, Y.; ZHang, J.; Duan, Y. Asynchronous blockade of PD-L1 and CD155 by polymeric nanoparticles inhibits triple-negative breast cancer progression and metastasis. Biomaterials 2021, 275, 120988. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Harden, K.; Gonzalez, L.C.; Francesco, M.; Chiang, E.; Irving, B.; Tom, I.; Ivelja, S.; Refino, C.J.; Clark, H.; et al. The surface protein TIGIT suppresses T cell activation by promoting the generation of mature immunoregulatory dendritic cells. Nat. Immunol. 2009, 10, 48–57. [Google Scholar] [CrossRef]
- Rodriguez-Abreu, D.; Johnson, M.L.; Hussein, M.A.; Cobo, M.; Patel, A.J.; Secen, N.M.; Lee, K.H.; Massuti, B.; Hiret, S.; Yang, J.C.; et al. Primary analysis of a randomized, double-blind, phase II study of the anti-TIGIT antibody tiragolumab (tira) plus atezolizumab (atezo) versus placebo plus atezo as first-line (1L) treatment in patients with PD-L1-selected NSCLC (CITYSCAPE). J. Clin. Orthod. 2020, 38, 9503. [Google Scholar] [CrossRef]
- Attalla, K.; Farkas, A.M.; Anastos, H.; Andenet, F.; Galsky, M.D.; Bhardwaj, N.; Sfakianos, J.P. TIM-3 and TIGIT are possible immune checkpoint targets in patients with bladder cancer. Urol. Oncol. Semin. Orig. Investig. 2020, in press. [Google Scholar] [CrossRef]
- Caruso, C. Tiragolumab Impresses in Multiple Trials. Cancer Discov. 2020, 10, 1086–1087. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CD155 Expression | |||||||
|---|---|---|---|---|---|---|---|
| Characteristics | mCD155 | cCD155 | |||||
| Total No. | negative | positive | p | negative | positive | p | |
| Total (%) | 103 | 81 | 22 | 79 | 24 | ||
| Age, years | |||||||
| ≤65 | 48 | 38 | 10 | 0.9 | 36 | 12 | 0.81 |
| ≥65 | 55 | 43 | 12 | 43 | 12 | ||
| SEX | |||||||
| Male | 86 | 69 | 17 | 0.35 | 66 | 20 | 0.98 |
| Female | 17 | 12 | 5 | 13 | 4 | ||
| Tumor stage | |||||||
| ≤pT2 | 52 | 45 | 7 | 0.04 | 39 | 13 | 0.82 |
| ≥pT3 | 51 | 36 | 15 | 40 | 11 | ||
| Pathologic grade | |||||||
| Grade 1 and 2 | 32 | 30 | 2 | 0.02 | 25 | 7 | 0.81 |
| Grade 3 | 71 | 51 | 20 | 54 | 17 | ||
| Carcinoma in situ | |||||||
| Present | 19 | 14 | 5 | 0.54 | 14 | 5 | 0.77 |
| Absent | 84 | 67 | 17 | 65 | 19 | ||
| LVI | |||||||
| Present | 54 | 39 | 15 | 0.22 | 38 | 16 | 0.08 |
| Absent | 37 | 31 | 6 | 32 | 5 | ||
| Nodal status | |||||||
| pN0 | 76 | 65 | 11 | <0.01 | 57 | 19 | 0.61 |
| pN+ | 27 | 16 | 11 | 22 | 5 | ||
| PD-L1 expression in tumor cell | |||||||
| Negative | 54 | 43 | 11 | 0.47 | 43 | 11 | 0.83 |
| Positive | 13 | 9 | 4 | 10 | 3 | ||
| PD-L1 expression in TILs | |||||||
| Negative | 42 | 34 | 8 | 0.55 | 32 | 10 | 0.54 |
| Positive | 25 | 18 | 7 | 21 | 4 | ||
| Adjuvant chemotherapy | |||||||
| Yes | 14 | 11 | 3 | 0.98 | 10 | 4 | 0.73 |
| No | 89 | 71 | 18 | 69 | 20 | ||
| Salvage chemotherapy | |||||||
| Responder | 4 | 3 | 1 | 0.71 | 3 | 1 | 0.56 |
| Non-responder | 9 | 7 | 2 | 4 | 5 | ||
| Recurrence | |||||||
| Yes | 48 | 34 | 14 | 0.09 | 35 | 13 | 0.49 |
| No | 55 | 47 | 8 | 44 | 11 | ||
| Cancer-specific death | |||||||
| No | 63 | 50 | 13 | 0.81 | 52 | 11 | 0.09 |
| Yes | 40 | 31 | 9 | 27 | 13 |
| CSS (Cancer-Specific Survival) | ||||||
|---|---|---|---|---|---|---|
| Univariate | Multivariate | |||||
| HR | 95% CI | p-value | HR | 95% CI | p-value | |
| mCD155 positive | 2.43 | 1.26–4.69 | <0.01 | 1.35 | 0.65–2.79 | 0.42 |
| pN+ | 2.94 | 0.16–5.41 | <0.01 | 2.43 | 1.17–5.1 | 0.02 |
| Grade3 | 2.08 | 1.01–4.27 | 0.04 | 1.1 | 0.51–2.42 | 0.81 |
| LVI present | 1.71 | 0.84–3.46 | 0.13 | 1.1 | 0.53–2.35 | 0.76 |
| pT3-4 | 2.8 | 1.50–5.22 | <0.01 | 1.79 | 0.85–3.74 | 0.12 |
| RFS (Recurrence-Free Survival) | ||||||
| Univariate | Multivariate | |||||
| HR | 95% CI | p-value | HR | 95% CI | p-value | |
| mCD155 positive | 2.13 | 1.14–4.01 | <0.01 | 1.26 | 0.63–2.52 | 0.52 |
| pN+ | 3.89 | 2.18–6.93 | <0.01 | 3.6 | 1.73–7.44 | <0.01 |
| Grade3 | 1.92 | 0.98–3.77 | 0.04 | 1.43 | 0.68–3.14 | 0.34 |
| LVI present | 1.48 | 0.79–2.78 | 0.21 | 0.65 | 0.31–1.39 | 0.27 |
| pT3-4 | 2.43 | 1.35–4.37 | <0.01 | 1.78 | 0.99–3.95 | 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mori, K.; Matsumoto, K.; Amano, N.; Koguchi, D.; Shimura, S.; Hagiwara, M.; Shimizu, Y.; Ikeda, M.; Sato, Y.; Iwamura, M. Expression of Membranous CD155 Is Associated with Aggressive Phenotypes and a Poor Prognosis in Patients with Bladder Cancer. Cancers 2022, 14, 1576. https://doi.org/10.3390/cancers14061576
Mori K, Matsumoto K, Amano N, Koguchi D, Shimura S, Hagiwara M, Shimizu Y, Ikeda M, Sato Y, Iwamura M. Expression of Membranous CD155 Is Associated with Aggressive Phenotypes and a Poor Prognosis in Patients with Bladder Cancer. Cancers. 2022; 14(6):1576. https://doi.org/10.3390/cancers14061576
Chicago/Turabian StyleMori, Kohei, Kazumasa Matsumoto, Noriyuki Amano, Dai Koguchi, Soichiro Shimura, Masahiro Hagiwara, Yuriko Shimizu, Masaomi Ikeda, Yuichi Sato, and Masatsugu Iwamura. 2022. "Expression of Membranous CD155 Is Associated with Aggressive Phenotypes and a Poor Prognosis in Patients with Bladder Cancer" Cancers 14, no. 6: 1576. https://doi.org/10.3390/cancers14061576
APA StyleMori, K., Matsumoto, K., Amano, N., Koguchi, D., Shimura, S., Hagiwara, M., Shimizu, Y., Ikeda, M., Sato, Y., & Iwamura, M. (2022). Expression of Membranous CD155 Is Associated with Aggressive Phenotypes and a Poor Prognosis in Patients with Bladder Cancer. Cancers, 14(6), 1576. https://doi.org/10.3390/cancers14061576