

CD3+ and CD8+ T-Cell-Based Immune Cell Score and PD-(L)1 Expression in Pulmonary Metastases of Microsatellite Stable Colorectal Cancer

 , , , , , , ,
, , , , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
2.1. Study Design
2.2. Data Collection
2.3. Tissue Microarrays
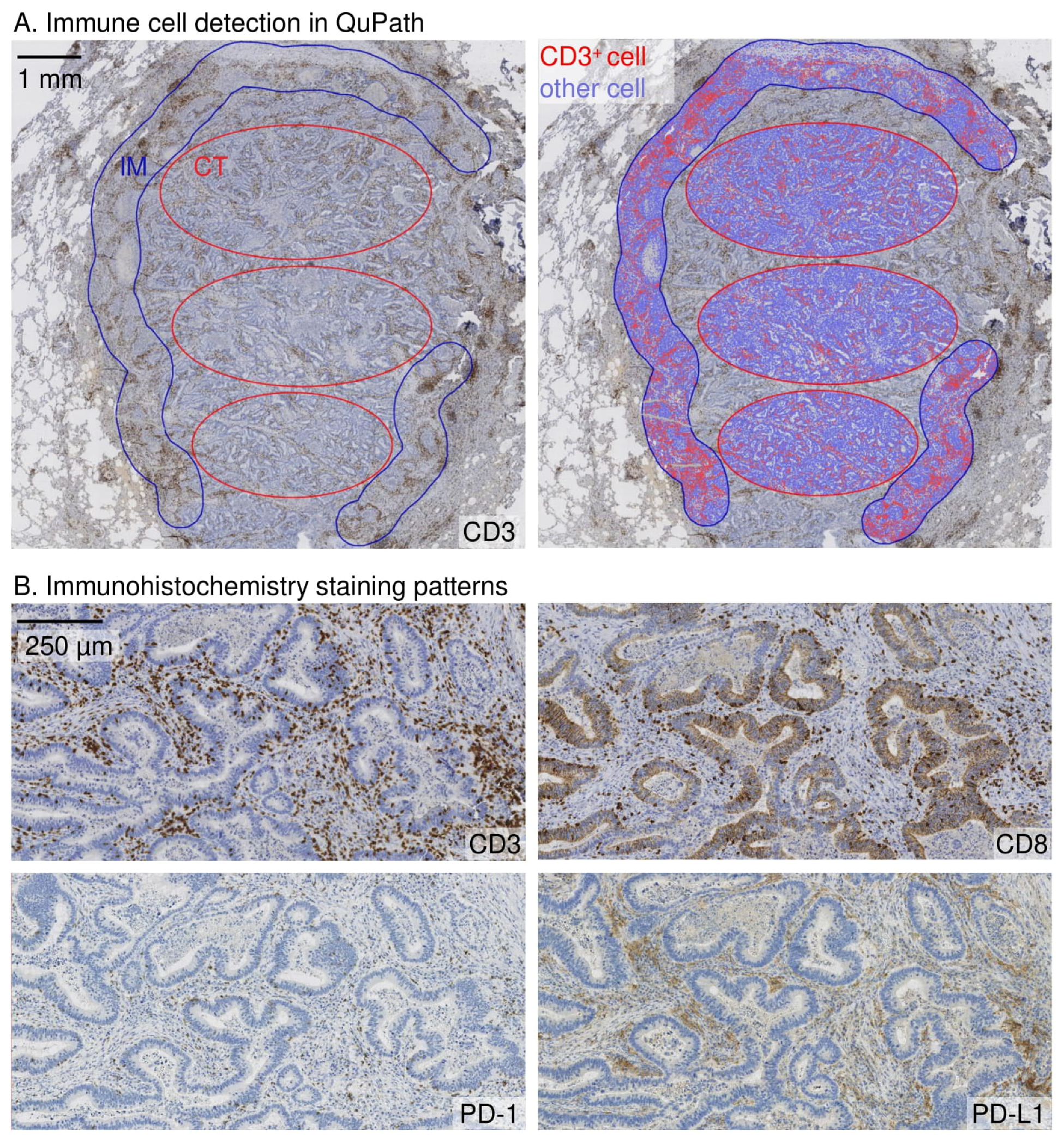
2.4. Immunohistochemistry
2.5. Scoring
2.6. Outcomes and Definitions
2.7. Statistical Analysis
2.8. Ethical Aspects
3. Results
3.1. Patient Characteristics
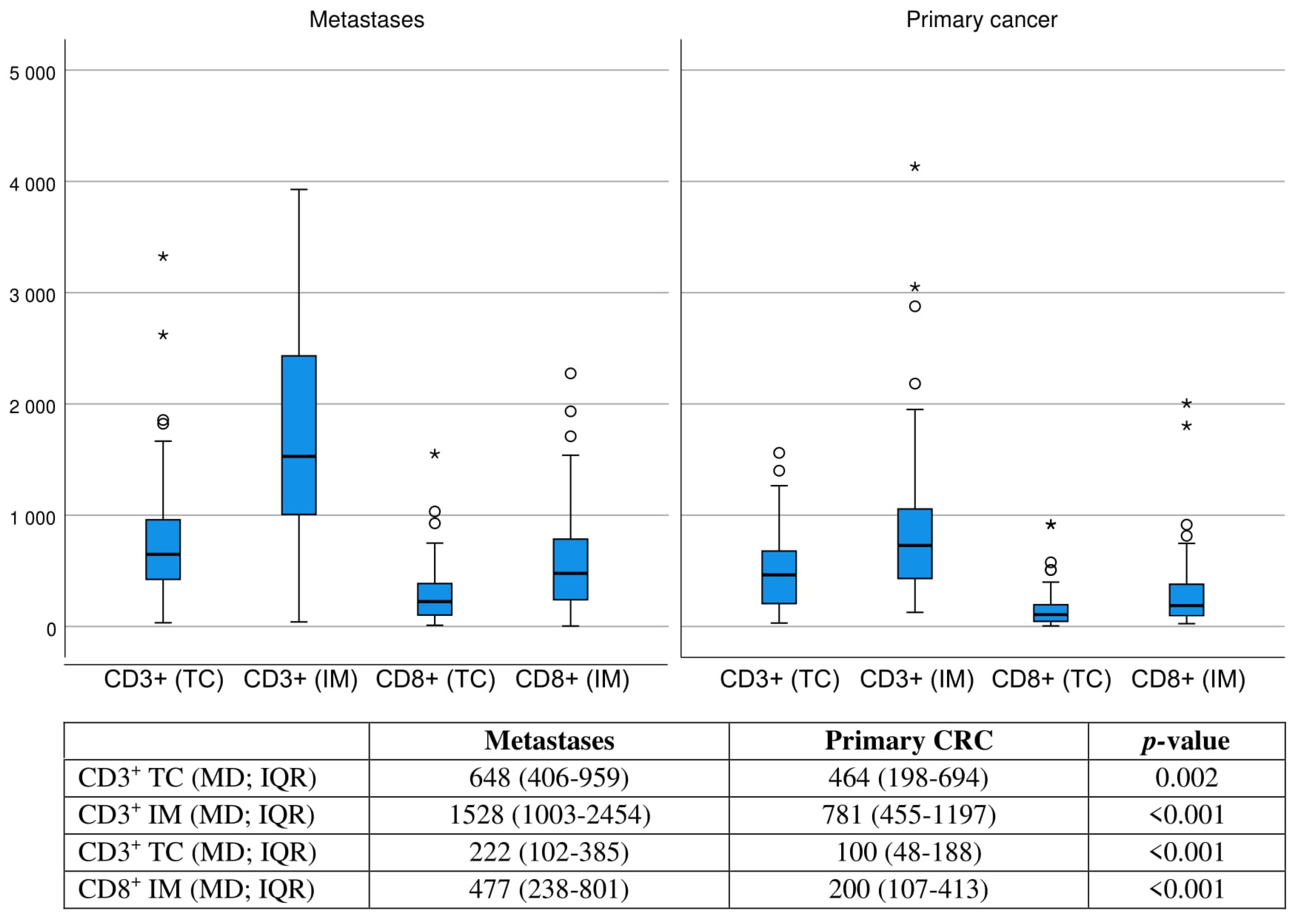
3.2. Immune Cell Score
3.3. Immune Cell Score and Survival
3.4. PD-1/PD-L1 and Survival
3.5. Post Hoc Analysis of Immune Cell Score
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2020, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Mitry, E.; Guiu, B.; Cosconea, S.; Jooste, V.; Faivre, J.; Bouvier, A.M. Epidemiology, Management and Prognosis of Colorectal Cancer with Lung Metastases: A 30-Year Population-Based Study. Gut 2010, 59, 1383–1388. [Google Scholar] [CrossRef] [PubMed]
- Colorectal Cancer Survival Rates|Colorectal Cancer Prognosis. Available online: https://www.cancer.org/cancer/colon-rectal-cancer/detection-diagnosis-staging/survival-rates.html (accessed on 20 September 2022).
- Gonzalez, H.; Hagerling, C.; Werb, Z. Roles of the Immune System in Cancer: From Tumor Initiation to Metastatic Progression. Genes Dev. 2018, 32, 1267–1284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagès, F.; Mlecnik, B.; Marliot, F.; Bindea, G.; Ou, F.-S.; Bifulco, C.; Lugli, A.; Zlobec, I.; Rau, T.T.; Berger, M.D.; et al. International Validation of the Consensus Immunoscore for the Classification of Colon Cancer: A Prognostic and Accuracy Study. Lancet 2018, 391, 2128–2139. [Google Scholar] [CrossRef] [PubMed]
- Mlecnik, B.; Bindea, G.; Kirilovsky, A.; Angell, H.K.; Obenauf, A.C.; Tosolini, M.; Church, S.E.; Maby, P.; Vasaturo, A.; Angelova, M.; et al. The Tumor Microenvironment and Immunoscore Are Critical Determinants of Dissemination to Distant Metastasis. Sci. Transl. Med. 2016, 8, 26–40. [Google Scholar] [CrossRef]
- Mlecnik, B.; van den Eynde, M.; Bindea, G.; Church, S.E.; Vasaturo, A.; Fredriksen, T.; Lafontaine, L.; Haicheur, N.; Marliot, F.; Debetancourt, D.; et al. Comprehensive Intrametastatic Immune Quantification and Major Impact of Immunoscore on Survival. J. Natl. Cancer Inst. 2018, 110, 97–108. [Google Scholar] [CrossRef] [Green Version]
- Baldin, P.; van den Eynde, M.; Mlecnik, B.; Bindea, G.; Beniuga, G.; Carrasco, J.; Haicheur, N.; Marliot, F.; Lafontaine, L.; Fredriksen, T.; et al. Prognostic Assessment of Resected Colorectal Liver Metastases Integrating Pathological Features, RAS Mutation and Immunoscore. Clin. Res. J. Pathol Clin. Res. 2021, 7, 27–41. [Google Scholar] [CrossRef]
- Ahtiainen, M.; Elomaa, H.; Väyrynen, J.P.; Wirta, E.V.; Kuopio, T.; Helminen, O.; Seppälä, T.T.; Kellokumpu, I.; Mecklin, J.P. Immune Contexture of MMR-Proficient Primary Colorectal Cancer and Matched Liver and Lung Metastases. Cancers 2021, 13, 1530. [Google Scholar] [CrossRef] [PubMed]
- Pardoll, D.M. The Blockade of Immune Checkpoints in Cancer Immunotherapy. Nat. Rev. Cancer 2012, 12, 252–264. [Google Scholar] [CrossRef] [Green Version]
- Topalian, S.L.; Taube, J.M.; Anders, R.A.; Pardoll, D.M. Mechanism-Driven Biomarkers to Guide Immune Checkpoint Blockade in Cancer Therapy. Nat. Rev. Cancer 2016, 16, 275–287. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Liang, L.; Dai, W.; Cai, G.; Xu, Y.; Li, X.; Li, Q.; Cai, S. Prognostic Impact of Programed Cell Death-1 (PD-1) and PD-Ligand 1 (PD-L1) Expression in Cancer Cells and Tumor Infiltrating Lymphocytes in Colorectal Cancer. Mol. Cancer 2016, 15, 55–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuai, W.; Xu, X.; Yan, J.; Zhao, W.; Li, Y.; Wang, B.; Yuan, N.; Li, Z.; Jia, Y. Prognostic Impact of PD-1 and Tim-3 Expression in Tumor Tissue in Stage I-III Colorectal Cancer. Biomed. Res. Int. 2020, 2020, 5294043. [Google Scholar] [CrossRef] [PubMed]
- Azcue, P.; Encío, I.; Setas, D.G.; Alecha, J.S.; Galbete, A.; Mercado, M.; Vera, R.; Gomez-Dorronsoro, M.L. PD-L1 as a Prognostic Factor in Early-Stage Colon Carcinoma within the Immunohistochemical Molecular Subtype Classification. Cancers 2021, 13, 1943. [Google Scholar] [CrossRef] [PubMed]
- Zengin, M.; Zergeroğlu, S.; Okcu, O.; Benek, S. PD-1 and PD-L2 Expression Predict Relapse Risk and Poor Survival in Patients with Stage III Colorectal Cancer. Cell Oncol. 2021, 44, 423–432. [Google Scholar] [CrossRef] [PubMed]
- Alterio, C.D.; Nasti, G.; Polimeno, M.; Ottaiano, A.; Conson, M.; Circelli, L.; Botti, G.; Scognamiglio, G.; Santagata, S.; de Divitiis, C.; et al. CXCR4-CXCL12-CXCR7, TLR2-TLR4, and PD-1/ PD-L1 in Colorectal Cancer Liver Metastases from Neoadjuvant-Treated Patients CXCR4-CXCL12-CXCR7, TLR2-TLR4, and PD-1/PD-L1 in Colorectal Cancer Liver Metastases from Neoadjuvant-Treated Patients. Oncoimmunology 2016, 5, e1254313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takasu, C.; Yamashita, S.; Morine, Y.; Yoshikawa, K.; Tokunaga, T.; Nishi, M.; Kashihara, H.; Yoshimoto, T.; Shimada, M. The Role of the Immunoescape in Colorectal Cancer Liver Metastasis. PLoS ONE 2021, 16, e0259940. [Google Scholar] [CrossRef]
- Yang, L.; Xue, R.; Pan, C. Prognostic and Clinicopathological Value of PD-L1 in Colorectal Cancer: A Systematic Review and Meta-Analysis. Onco. Targets Ther. 2019, 12, 3671–3682. [Google Scholar] [CrossRef]
- Han, Y.; Liu, D.; Li, L. PD-1/PD-L1 Pathway: Current Researches in Cancer. Am. J. Cancer Res. 2020, 10, 727–742. [Google Scholar]
- Overman, M.J.; McDermott, R.; Leach, J.L.; Lonardi, S.; Lenz, H.J.; Morse, M.A.; Desai, J.; Hill, A.; Axelson, M.; Moss, R.A.; et al. Nivolumab in Patients with Metastatic DNA Mismatch Repair-Deficient or Microsatellite Instability-High Colorectal Cancer (CheckMate 142): An Open-Label, Multicentre, Phase 2 Study. Lancet Oncol. 2017, 18, 1182–1191. [Google Scholar] [CrossRef]
- Le, D.T.; Uram, J.N.; Wang, H.; Bartlett, B.R.; Kemberling, H.; Eyring, A.D.; Skora, A.D.; Luber, B.S.; Azad, N.S.; Laheru, D.; et al. PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. N. Engl. J. Med. 2015, 372, 2509–2520. [Google Scholar] [CrossRef] [Green Version]
- Johnson, B.; Haymaker, C.L.; Parra, E.R.; Maren, L.; Soto, S.; Wang, X.; Thomas, J.V.; Dasari, A.; Morris, V.K.; Raghav, K.; et al. Phase II Study of Durvalumab (Anti-PD-L1) and Trametinib (MEKi) in Microsatellite Stable (MSS) Metastatic Colorectal Cancer (MCRC). J. Immunother. Cancer 2022, 12, 5332–5343. [Google Scholar] [CrossRef] [PubMed]
- Chalabi, M.; Fanchi, L.F.; Dijkstra, K.K.; van den Berg, J.G.; Aalbers, A.G.; Sikorska, K.; Lopez-Yurda, M.; Grootscholten, C.; Beets, G.L.; Snaebjornsson, P.; et al. Neoadjuvant Immunotherapy Leads to Pathological Responses in MMR-Proficient and MMR-Deficient Early-Stage Colon Cancers. Nat. Med. 2020, 26, 566–576. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Edge, S.; Greene, F.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. AJCC Cancer Staging Manual, 8th ed.; Springer Cham: New York, NY, USA, 2017; ISBN 9783319406176. [Google Scholar]
- Bankhead, P.; Loughrey, M.B.; Fernández, J.A.; Dombrowski, Y.; McArt, D.G.; Dunne, P.D.; McQuaid, S.; Gray, R.T.; Murray, L.J.; Coleman, H.G.; et al. QuPath: Open Source Software for Digital Pathology Image Analysis. Sci. Rep. 2017, 7, 16878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Marchi, P.; Leal, L.F.; Duval Da Silva, V.; da Silva, E.C.A.; Cordeiro De Lima, V.C.; Reis, R.M. PD-L1 Expression by Tumor Proportion Score (TPS) and Combined Positive Score (CPS) Are Similar in Non-Small Cell Lung Cancer (NSCLC). J. Clin. Pathol. 2021, 74, 735–740. [Google Scholar] [CrossRef] [PubMed]
- Armitage, J.N.; van der Meulen, J.H. Identifying Co-Morbidity in Surgical Patients Using Administrative Data with the Royal College of Surgeons Charlson Score. Br. J. Surg. 2010, 97, 772–781. [Google Scholar] [CrossRef]
- van den Eynde, M.; Mlecnik, B.; Bindea, G.; Fredriksen, T.; Church, S.E.; Lafontaine, L.; Haicheur, N.; Marliot, F.; Angelova, M.; Vasaturo, A.; et al. The Link between the Multiverse of Immune Microenvironments in Metastases and the Survival of Colorectal Cancer Patients. Cancer Cell 2018, 34, 1012–1026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, L.H.; Cavalcanti, M.S.; Segal, N.H.; Hechtman, J.F.; Weiser, M.R.; Smith, J.J.; Garcia-Aguilar, J.; Sadot, E.; Ntiamoah, P.; Markowitz, A.J.; et al. Patterns and Prognostic Relevance of PD-1 and PD-L1 Expression in Colorectal Carcinoma. Mod. Pathol. 2016, 29, 1433–1442. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.E.; Kim, J.H.; Kim, S.Y.; Cho, H.; Ryu, Y.M.; Hong, Y.S.; Kim, S.Y.; Kim, T.W. Immune Profile of BRAF-Mutated Metastatic Colorectal Tumors with Good Prognosis after Palliative Chemotherapy. Cancers 2022, 14, 2383. [Google Scholar] [CrossRef]
- Ko, Y.S.; Pyo, J.S. Clinicopathological Significance and Prognostic Role of Tumor-Infiltrating Lymphocytes in Colorectal Cancer. Int. J. Biol. Markers 2019, 34, 132–138. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.B.; Yao, H.; Li, C.S.; Liang, L.X.; Zhang, Y.; Chen, Y.X.; Fang, J.-Y.; Xu, J. Rise of PD-L1 Expression during Metastasis of Colorectal Cancer: Implications for Immunotherapy. J. Dig. Dis. 2017, 18, 574–581. [Google Scholar] [CrossRef] [Green Version]
- Meng, X.; Huang, Z.; Teng, F.; Xing, L.; Yu, J. Predictive Biomarkers in PD-1/PD-L1 Checkpoint Blockade Immunotherapy. Cancer Treat. Rev. 2015, 41, 868–876. [Google Scholar] [CrossRef] [PubMed]
- Cervantes, A.; Adam, R.; Roselló, S.; Arnold, D.; Normanno, N.; Taïeb, J.; Seligmann, J.; de Baere, T.; Osterlund, P.; Yoshino, T.; et al. Metastatic Colorectal Cancer: ESMO Clinical Practice Guideline for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2022, 43, 10–32. [Google Scholar] [CrossRef] [PubMed]
- Schmoll, H.J.; van Cutsem, E.; Stein, A.; Valentini, V.; Glimelius, B.; Haustermans, K.; Nordlinger, B.; van de Velde, C.J.; Balmana, J.; Regula, J.; et al. ESMO Consensus Guidelines for Management of Patients with Colon and Rectal Cancer. A Personalized Approach to Clinical Decision Making. Ann. Oncol. 2012, 23, 2479–2516. [Google Scholar] [CrossRef] [PubMed]
- Ou, L.; Lu, G.; Cao, M.; Hu, M. Lung Metastases after Liver Cancer Resection Cured by Immunotherapy: Case Report and Literature Review. Anti-Cancer Drugs 2023, 34, e1. [Google Scholar] [CrossRef]
- Gong, T.J.; Tang, F.; Zheng, C.X.; Wang, J.; Wang, Y.T.; Zhang, Y.H.; Luo, Y.; Zhou, Y.; Min, L.; Tu, C.Q. Case Report: Pulmonary Metastases From Epithelioid Sarcoma in Extremity Favourably Responding to Immunotherapy With Camrelizumab. Front. Oncol. 2021, 11, 4070. [Google Scholar] [CrossRef]
- Stephens, A.J.; Burgess-Brown, N.A.; Jiang, S. Beyond Just Peptide Antigens: The Complex World of Peptide-Based Cancer Vaccines. Front. Immunol. 2021, 12, 696791. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.; Kumar, A.B.; Finnes, H.; Markovic, S.N.; Park, S.; Dronca, R.S.; Dong, H. Combining Immune Checkpoint Inhibitors With Conventional Cancer Therapy. Front. Immunol. 2018, 9, 1739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaumaya, P.T.P.; Guo, L.; Overholser, J.; Penichet, M.L.; Bekaii-Saab, T. Immunogenicity and Antitumor Efficacy of a Novel Human PD-1 B-Cell Vaccine (PD1-Vaxx) and Combination Immunotherapy with Dual Trastuzumab/Pertuzumab-like HER-2 B-Cell Epitope Vaccines (B-Vaxx) in a Syngeneic Mouse Model. OncoImmunology 2020, 9, e1818437. [Google Scholar] [CrossRef]
- Guo, L.; Overholser, J.; Darby, H.; Ede, N.J.; Kaumaya, P.T.P. A Newly Discovered PD-L1 B-Cell Epitope Peptide Vaccine (PDL1-Vaxx) Exhibits Potent Immune Responses and Effective Anti-Tumor Immunity in Multiple Syngeneic Mice Models and (Synergizes) in Combination with a Dual HER-2 B-Cell Vaccine (B-Vaxx). Oncoimmunology 2022, 11, 2127691. [Google Scholar] [CrossRef]
- Guo, L.; Overholser, J.; Good, A.J.; Ede, N.J.; Kaumaya, P.T.P. Preclinical Studies of a Novel Human PD-1 B-Cell Peptide Cancer Vaccine PD1-Vaxx From BALB/c Mice to Beagle Dogs and to Non-Human Primates (Cynomolgus Monkeys). Front. Oncol. 2022, 12, 1989–2004. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ICS 1 | ICS 1 | ICS 2 | p-Value | |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | ||
| 10 | 40 | 17 | ||
| Sex | 0.615 | |||
| Female | 5 (50.0%) | 22 (55.0%) | 7 (41.2%) | |
| Male | 5 (50.0%) | 18 (45.0%) | 10 (58.8%) | |
| Age (M, SD) | 68.5 (10.5) | 66.8 (11.3) | 69.2 (9.6) | 0.622 |
| CCI | 0.748 | |||
| 1 | 7 (70.0%) | 25 (62.5%) | 8 (47.1%) | |
| 2 | 2 (20.0%) | 8 (20.0%) | 6 (35.3%) | |
| ≥3 | 1 (10.0%) | 7 (17.5%) | 3 (17.6%) | |
| CRC stage | 0.548 | |||
| 1–2 | 2 (20.0%) | 17 (42.5%) | 4 (23.5%) | |
| 3 | 5 (50.0%) | 13 (32.5%) | 8 (47.1%) | |
| 4 | 3 (30.0%) | 10 (25.0%) | 5 (29.4%) | |
| CRC location | 0.255 | |||
| Colon | 6 (60.0%) | 17 (42.5%) | 11 (64.7%) | |
| Rectum | 4 (40.0%) | 23 (57.5%) | 6 (35.3%) | |
| Former CRC liver metastasectomy | 0.154 | |||
| No | 5 (50.0%) | 25 (62.5%) | 6 (35.3%) | |
| Yes | 5 (50.0%) | 15 (37.5%) | 11 (64.7%) | |
| Neoadjuvant | 0.883 | |||
| No | 5 (50.0%) | 24 (60.0%) | 10 (58.8%) | |
| Chemotherapy | 5 (50.0%) | 16 (40.0%) | 7 (41.2%) | |
| DFI (d; MD; IQR) | 645.5 (0–925) | 363.5 (0–793) | 309.0 (0–738) | 0.922 |
| Synchronicity | 0.533 | |||
| Synchronous | 2 (20.0%) | 10 (25.0%) | 2 (11.8%) | |
| Metachronous | 8 (80.0%) | 30 (75.0%) | 15 (88.2%) | |
| No of PM at diagnosis | 0.369 | |||
| 1 | 5 (50.0%) | 25 (62.5%) | 13 (76.5%) | |
| ≥1 | 5 (50.0%) | 15 (37.5%) | 4 (23.5%) | |
| Size of largest PM (MD; IQR) | 2.8 (1.3–4.0) | 2.2 (1.1–3.1) | 2.0 (1.3–3.5) | 0.691 |
| Laterality of PM | 0.392 | |||
| Unilateral | 8 (80.0%) | 31 (77.5%) | 16 (94.1%) | |
| Bilateral | 2 (20.0%) | 9 (22.5%) | 1 (5.9%) | |
| BRAF | >0.999 | |||
| Wild-type | 10 (100.0%) | 36 (94.7%) | 17 (100.0%) | |
| Mutant | 0 (0.0%) | 2 (5.3%) | 0 (0.0%) | |
| met PD-1 (TC) | <0.001 * | |||
| Low | 10 (100.0%) | 27 (67.5%) | 2 (11.8%) | |
| High | 0 (0.0%) | 13 (32.5%) | 15 (88.2%) | |
| met PD-1 (IM) | <0.001 * | |||
| Low | 10 (100.0%) | 23 (63.9%) | 2 (11.8%) | |
| High | 0 (0.0%) | 13 (36.1%) | 15 (88.2%) | |
| met PD-L1 (TCe) | 0.156 | |||
| Low | 10 (100.0%) | 38 (95.0%) | 14 (82.4%) | |
| High | 0 (0.0%) | 2 (5.0%) | 3 (17.6%) | |
| met PD-L1 (IC) | 0.003 * | |||
| Low | 5 (50.0%) | 6 (15.4%) | 0 (0.0%) | |
| High | 5 (50.0%) | 33 (84.6%) | 17 (100.0%) | |
| prim PD-1 (TC) | 0.008 * | |||
| Low | 8 (88.9%) | 19 (54.3%) | 4 (25.0%) | |
| High | 1 (11.1%) | 17 (45.7%) | 12 (75.0%) | |
| prim PD-1 (IM) | 0.073 | |||
| Low | 7 (77.8%) | 19 (54.3%) | 5 (31.3%) | |
| High | 2 (22.2%) | 16 (45.7%) | 11 (68.8%) | |
| prim PD-L1 (TCe) | 0.074 | |||
| Low | 9 (100.0%) | 34 (97.1%) | 13 (81.3%) | |
| High | 0 (0.0%) | 1 (2.9%) | 3 (18.7%) | |
| prim PD-L1 (IC) | >0.999 | |||
| Low | 7 (77.8%) | 25 (71.4%) | 11 (68.8%) | |
| High | 2 (22.2%) | 10 (28.6%) | 5 (31.3%) | |
| ICS primary tumour | 0.074 | |||
| Low | 4 (44.4%) | 5 (13.9%) | 4 (25.0%) | |
| Intermediate | 5 (55.6%) | 23 (63.9%) | 6 (37.5%) | |
| High | 0 (0.0%) | 8 (22.2%) | 6 (37.5%) |
| n | ICS 0 | ICS 1 | ICS 2 | p-value | |
| Metastases | 67 | 10.0% | 25.5% | 47.0% | 0.046 * |
| Primary tumours | 62 | 11.1% | 41.9% | 0.0% | 0.152 |
| n | PD-1 (TC) low | PD-1 (TC), high | p | ||
| Metastases | 67 | 23.5% | 33.6% | 0.114 | |
| Primary tumours | 61 | 29.3% | 27.2% | 0.726 | |
| n | PD-1 (IM) low | PD-1 (IM), high | p | ||
| Metastases | 63 | 23.8% | 39.7% | 0.066 | |
| Primary tumours | 60 | 20.7% | 42.5% | 0.328 | |
| n | PD-L1 (TCe) low | PD-L1 (TCe), high | p | ||
| Metastases | 67 | 23.3% | 100.0% | 0.024 | |
| Primary tumours | 60 | 28.2% | 0.0% | 0.328 | |
| n | PD-L1 (IC) low | PD-L1 (IC), high | p | ||
| Metastases | 66 | 27.3% | 27.7% | 0.943 | |
| Primary tumours | 60 | 32.4% | 13.9% | 0.086 |
| n | ICS 0, HR (95%CI) | ICS 1, HR (95%CI) | ICS 2, HR (95%CI) | |
|---|---|---|---|---|
| Metastases | ||||
| Crude | 67 | 1.00 (reference) | 0.48 (0.22–1.03, p = 0.058) | 0.31 (0.12–0.84, p = 0.022) |
| Adjusted * | 67 | 1.00 (reference) | 0.31 (0.13–0.74, p = 0.008) | 0.25 (0.09–0.75, p = 0.013) |
| Primary Tumours | ||||
| Crude | 62 | 1.00 (reference) | 0.63 (0.29–1.35, p = 0.233) | 1.31 (0.53–3.24, p = 0.558) |
| Adjusted ** | 62 | 1.00 (reference) | 0.69 (0.28–1.67, p = 0.406) | 1.35 (0.41–4.42, p = 0.625) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karjula, T.; Elomaa, H.; Niskakangas, A.; Mustonen, O.; Puro, I.; Kuopio, T.; Ahtiainen, M.; Mecklin, J.-P.; Seppälä, T.T.; Wirta, E.-V.; et al. CD3+ and CD8+ T-Cell-Based Immune Cell Score and PD-(L)1 Expression in Pulmonary Metastases of Microsatellite Stable Colorectal Cancer. Cancers 2023, 15, 206. https://doi.org/10.3390/cancers15010206
Karjula T, Elomaa H, Niskakangas A, Mustonen O, Puro I, Kuopio T, Ahtiainen M, Mecklin J-P, Seppälä TT, Wirta E-V, et al. CD3+ and CD8+ T-Cell-Based Immune Cell Score and PD-(L)1 Expression in Pulmonary Metastases of Microsatellite Stable Colorectal Cancer. Cancers. 2023; 15(1):206. https://doi.org/10.3390/cancers15010206
Chicago/Turabian StyleKarjula, Topias, Hanna Elomaa, Anne Niskakangas, Olli Mustonen, Iiris Puro, Teijo Kuopio, Maarit Ahtiainen, Jukka-Pekka Mecklin, Toni T. Seppälä, Erkki-Ville Wirta, and et al. 2023. "CD3+ and CD8+ T-Cell-Based Immune Cell Score and PD-(L)1 Expression in Pulmonary Metastases of Microsatellite Stable Colorectal Cancer" Cancers 15, no. 1: 206. https://doi.org/10.3390/cancers15010206
APA StyleKarjula, T., Elomaa, H., Niskakangas, A., Mustonen, O., Puro, I., Kuopio, T., Ahtiainen, M., Mecklin, J. -P., Seppälä, T. T., Wirta, E. -V., Sihvo, E., Väyrynen, J. P., Yannopoulos, F., & Helminen, O. (2023). CD3+ and CD8+ T-Cell-Based Immune Cell Score and PD-(L)1 Expression in Pulmonary Metastases of Microsatellite Stable Colorectal Cancer. Cancers, 15(1), 206. https://doi.org/10.3390/cancers15010206