
Circulating Tumor Cells as Biomarkers for Renal Cell Carcinoma: Ready for Prime Time?




Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
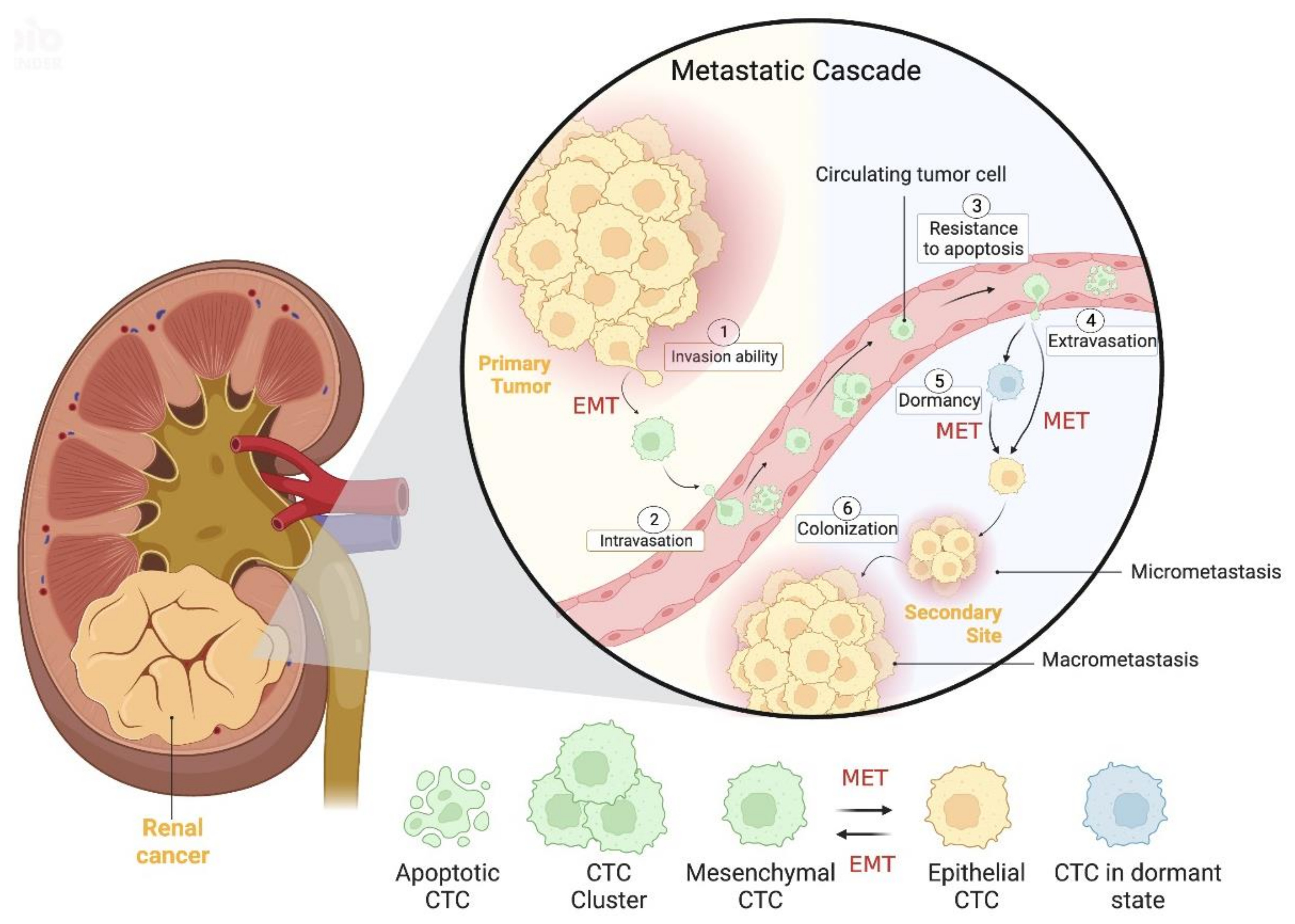
3. CTCs Biology and Clinical Significance: An Overview
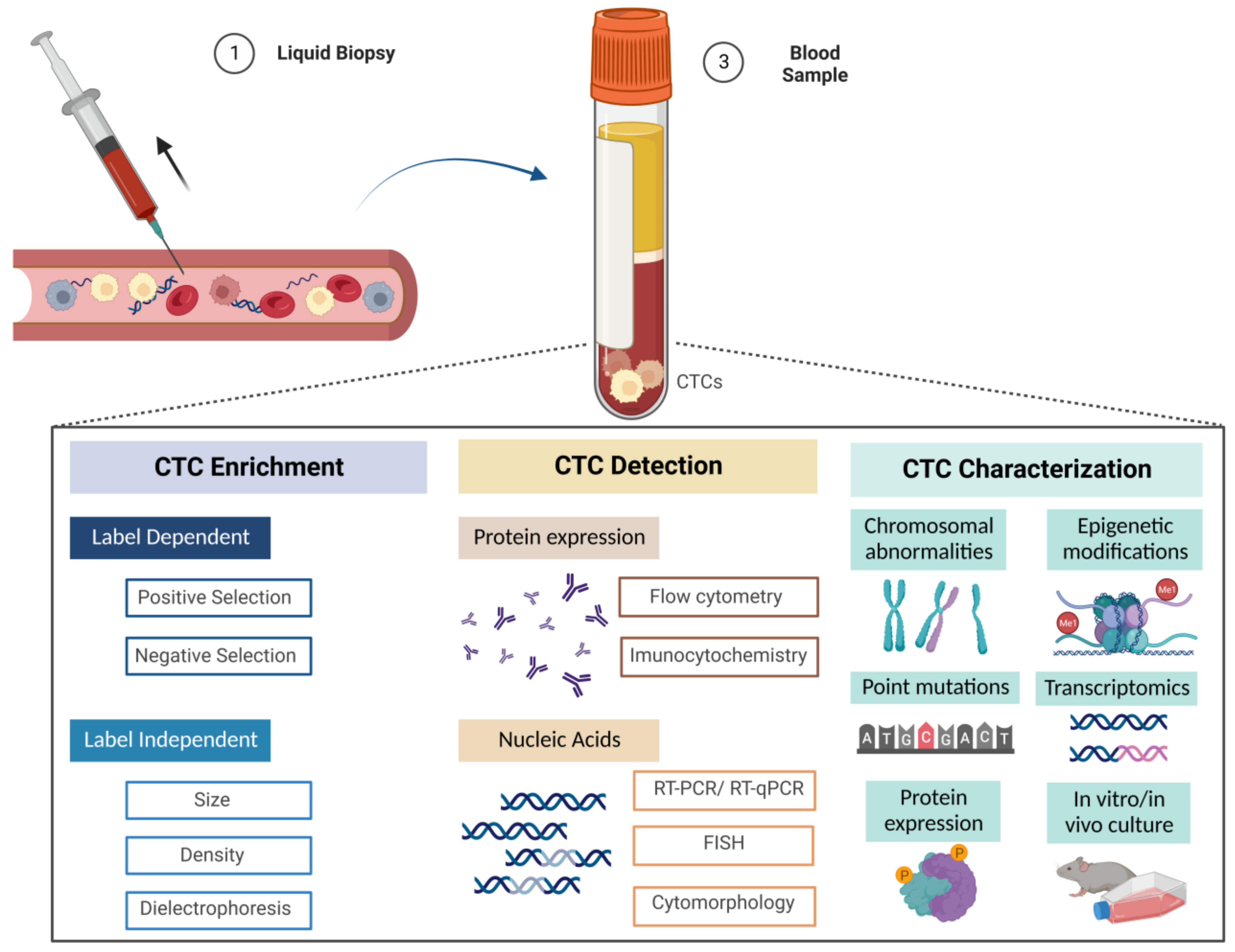
4. Enrichment and Detection Techniques for CTCs
5. Enrichment Techniques
5.1. Label-Dependent Methodologies
5.1.1. Positive Selection Strategy
5.1.2. Negative Selection Strategy
5.2. Label-Independent Methodologies
5.2.1. Size- and Deformability-Based Enrichment
Membrane Filtration
Microfluidic Chips
5.2.2. Density Based Enrichment
5.2.3. Differential Electric Charge-Based Enrichment
5.3. Detection Techniques
5.3.1. Protein Expression-Based Strategies
Flow Cytometry
5.3.2. Immunocytochemistry
Immunofluorescence
5.3.3. Nucleic Acids-Based Strategies
PCR
RNA In Situ Hybridization
Sequencing
5.3.4. Combined Strategies
5.4. Emerging Techniques for mRCC

{kind=link}
{kind=link}
{kind=link}
| Technology | Characteristics | Reference |
|---|---|---|
| SE- iFISH | Based on subtraction enrichment (SE) and combined with immunofluorescence in situ hybridization (iFISH) | [65,80,81] |
| NE-iFISH | Based on negative enrichment (NE) and combined with immunofluorescence in situ hybridization (iFISH) | [51] |
| Tapered-slit filter platform | Based on size and deformability properties | [82] |
| CelSee® + On-chip Sort® + BD FACSCalibur™ system | Based on microfluidics and sorted by combination with anti-G250 antibodies Based on flow cytometry detection | [83] |
| SERS platform and Raman spectroscopy (SHINERS) | Based on nanomaterials (silver) combined with photovoltaic and microfluidic devices and spectroscopy | [84] |
| Nanobiointerface chips | Based on nanomaterials (silica) combined with nanochips | [85] |
| Capture platform | Based on dendrimers, biomimetic cell rolling and a combination of antibodies | [86] |
| Hydrogel-based cell blocks | Based on cell blocks formation (label-free) combined with immunocytochemistry | [87] |
| CellCollector® | Based on EpCam expression In vivo and ex vivo method | [12] |
6. Models for RCC Investigation
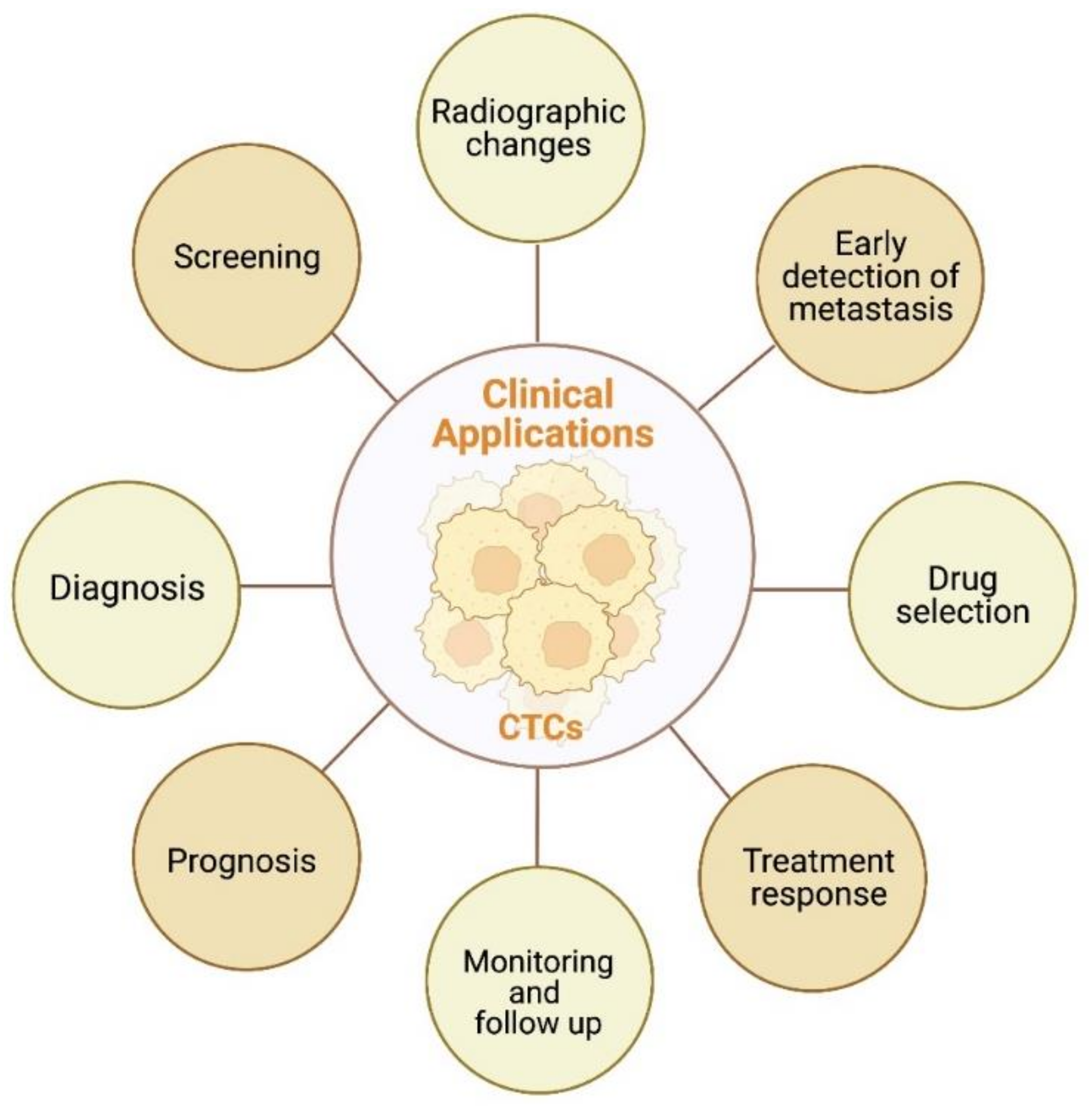
7. Clinical Applications of CTCs
7.1. Early Detection of Metastasis

7.2. Prognostic Value
7.3. Prediction of Response to Therapy
7.4. Screening
7.5. Monitoring and Follow-Up
7.6. Radiological Impact
8. Future Directions
9. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Rossi, S.H.; Blick, C.; Handforth, C.; Brown, J.E.; Stewart, G.D.; Renal Cancer Gap Analysis, C. Essential Research Priorities in Renal Cancer: A Modified Delphi Consensus Statement. Eur. Urol. Focus. 2020, 6, 991–998. [Google Scholar] [CrossRef] [PubMed]
- Rosiello, G.; Larcher, A.; Montorsi, F.; Capitanio, U. Renal cancer: Overdiagnosis and overtreatment. World J. Urol. 2021, 39, 2821–2823. [Google Scholar] [CrossRef] [PubMed]
- Padala, S.A.; Barsouk, A.; Thandra, K.C.; Saginala, K.; Mohammed, A.; Vakiti, A.; Rawla, P.; Barsouk, A. Epidemiology of Renal Cell Carcinoma. World J. Oncol. 2020, 11, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Moch, H.; Amin, M.B.; Berney, D.M.; Comperat, E.M.; Gill, A.J.; Hartmann, A.; Menon, S.; Raspollini, M.R.; Rubin, M.A.; Srigley, J.R.; et al. The 2022 World Health Organization Classification of Tumours of the Urinary System and Male Genital Organs-Part A: Renal, Penile, and Testicular Tumours. Eur. Urol. 2022, 82, 458–468. [Google Scholar] [CrossRef] [PubMed]
- Archard, N.; Vargiamidou, A.; Beggan, C.; Ho-Yen, C.M. Pathological Classification and Biomarkers. In Renal Cancer: Current Status and Innovations; Anderson, C., Afshar, M., Eds.; Springer International Publishing: Cham, Switzerland, 2022; pp. 53–68. [Google Scholar] [CrossRef]
- Bradley, A.J.; Maskell, G.F.; Mannava, A.; Pollard, A.; Welsh, T. Routes to diagnosis and missed opportunities in the detection of renal cancer. Clin. Radiol. 2021, 76, 129–134. [Google Scholar] [CrossRef]
- Yin, Q.; Xu, H.; Zhong, Y.; Ni, J.; Hu, S. Diagnostic performance of MRI, SPECT, and PET in detecting renal cell carcinoma: A systematic review and meta-analysis. BMC Cancer 2022, 22, 163. [Google Scholar] [CrossRef]
- O’Connor, S.D.; Silverman, S.G.; Cochon, L.R.; Khorasani, R.K. Renal cancer at unenhanced CT: Imaging features, detection rates, and outcomes. Abdom. Radiol. 2018, 43, 1756–1763. [Google Scholar] [CrossRef]
- Vig, S.V.L.; Zan, E.; Kang, S.K. Imaging for Metastatic Renal Cell Carcinoma. Urol. Clin. North Am. 2020, 47, 281–291. [Google Scholar] [CrossRef]
- Capitanio, U.; Bensalah, K.; Bex, A.; Boorjian, S.A.; Bray, F.; Coleman, J.; Gore, J.L.; Sun, M.; Wood, C.; Russo, P. Epidemiology of Renal Cell Carcinoma. Eur. Urol. 2019, 75, 74–84. [Google Scholar] [CrossRef]
- Bialek, J.; Wencker, A.; Kawan, F.; Yankulov, S.; Fornara, P.; Theil, G. Potential Use of CTCs as Biomarkers in Renal Cancer Patients. Life 2022, 12, 89. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.-F.; Wu, L.; Liu, S.-P.; Jiang, M.-M.; Hu, B.; Zhou, K.-Q.; Guo, W.; Xu, Y.; Zhong, Y.; Zhou, X.-R.; et al. Dissecting spatial heterogeneity and the immune-evasion mechanism of CTCs by single-cell RNA-seq in hepatocellular carcinoma. Nat. Commun. 2021, 12, 4091. [Google Scholar] [CrossRef]
- Su, Z.; Wang, Z.; Ni, X.; Duan, J.; Gao, Y.; Zhuo, M.; Li, R.; Zhao, J.; Ma, Q.; Bai, H.; et al. Inferring the Evolution and Progression of Small-Cell Lung Cancer by Single-Cell Sequencing of Circulating Tumor Cells. Clin. Cancer Res. 2019, 25, 5049–5060. [Google Scholar] [CrossRef] [PubMed]
- Lim, M.; Park, S.; Jeong, H.-O.; Park, S.H.; Kumar, S.; Jang, A.; Lee, S.; Kim, D.U.; Cho, Y.-K. Circulating Tumor Cell Clusters Are Cloaked with Platelets and Correlate with Poor Prognosis in Unresectable Pancreatic Cancer. Cancers 2021, 13, 5272. [Google Scholar] [CrossRef]
- Jiang, M.; Jin, S.; Han, J.; Li, T.; Shi, J.; Zhong, Q.; Li, W.; Tang, W.; Huang, Q.; Zong, H. Detection and clinical significance of circulating tumor cells in colorectal cancer. Biomark. Res. 2021, 9, 85. [Google Scholar] [CrossRef] [PubMed]
- Mendelaar, P.A.J.; Kraan, J.; Van, M.; Zeune, L.L.; Terstappen, L.W.M.M.; Oomen-De Hoop, E.; Martens, J.W.M.; Sleijfer, S. Defining the dimensions of circulating tumor cells in a large series of breast, prostate, colon, and bladder cancer patients. Mol. Oncol. 2021, 15, 116–125. [Google Scholar] [CrossRef]
- Guan, Y.; Xu, F.; Tian, J.; Chen, H.; Yang, C.; Huang, S.; Gao, K.; Wan, Z.; Li, M.; He, M.; et al. Pathology of circulating tumor cells and the available capture tools (Review). Oncol. Rep. 2020, 43, 1355–1364. [Google Scholar] [CrossRef]
- Yeo, D.; Bastian, A.; Strauss, H.; Saxena, P.; Grimison, P.; Rasko, J.E.J. Exploring the Clinical Utility of Pancreatic Cancer Circulating Tumor Cells. Int. J. Mol. Sci. 2022, 23, 1671. [Google Scholar] [CrossRef]
- Lin, D.; Shen, L.; Luo, M.; Zhang, K.; Li, J.; Yang, Q.; Zhu, F.; Zhou, D.; Zheng, S.; Chen, Y.; et al. Circulating tumor cells: Biology and clinical significance. Signal Transduct Target 2021, 6, 404. [Google Scholar] [CrossRef]
- Menyailo, M.E.; Bokova, U.A.; Ivanyuk, E.E.; Khozyainova, A.A.; Denisov, E.V. Metastasis Prevention: Focus on Metastatic Circulating Tumor Cells. Mol. Diagn 2021, 25, 549–562. [Google Scholar] [CrossRef]
- Lowes, L.E.; Allan, A.L. Circulating Tumor Cells and Implications of the Epithelial-to-Mesenchymal Transition. Adv. Clin. Chem. 2018, 83, 121–181. [Google Scholar] [CrossRef] [PubMed]
- Werner, S.; Stenzl, A.; Pantel, K.; Todenhofer, T. Expression of Epithelial Mesenchymal Transition and Cancer Stem Cell Markers in Circulating Tumor Cells. Adv. Exp. Med. Biol. 2017, 994, 205–228. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Li, H.; Yuan, Y.; Hao, T.; Zou, B.; Yu, B.; Li, S.; Zhang, J. A preliminary study on the association between epithelial-mesenchymal transition and circulating tumor cells in renal cell carcinoma. Transl. Androl. Urol. 2022, 11, 460–471. [Google Scholar] [CrossRef] [PubMed]
- Lowes, L.E.; Goodale, D.; Xia, Y.; Postenka, C.; Piaseczny, M.M.; Paczkowski, F.; Allan, A.L. Epithelial-to-mesenchymal transition leads to disease-stage differences in circulating tumor cell detection and metastasis in pre-clinical models of prostate cancer. Oncotarget 2016, 7, 76125–76139. [Google Scholar] [CrossRef] [Green Version]
- Guan, X.; Ma, F.; Liu, S.; Wu, S.; Xiao, R.; Yuan, L.; Sun, X.; Yi, Z.; Yang, H.; Xu, B. Analysis of the hormone receptor status of circulating tumor cell subpopulations based on epithelial-mesenchymal transition: A proof-of-principle study on the heterogeneity of circulating tumor cells. Oncotarget 2016, 7, 65993–66002. [Google Scholar] [CrossRef] [Green Version]
- Carneiro, A.; Piairo, P.; Teixeira, A.; Ferreira, D.; Cotton, S.; Rodrigues, C.; Chicharo, A.; Abalde-Cela, S.; Santos, L.L.; Lima, L.; et al. Discriminating Epithelial to Mesenchymal Transition Phenotypes in Circulating Tumor Cells Isolated from Advanced Gastrointestinal Cancer Patients. Cells 2022, 11, 376. [Google Scholar] [CrossRef]
- Wu, F.; Zhu, J.; Mao, Y.; Li, X.; Hu, B.; Zhang, D. Associations between the Epithelial-Mesenchymal Transition Phenotypes of Circulating Tumor Cells and the Clinicopathological Features of Patients with Colorectal Cancer. Dis. Mrk. 2017, 2017, 9474532. [Google Scholar] [CrossRef] [Green Version]
- Xia, Q.-D.; Zhang, Y.; Li, L.-S.; Lu, J.-L.; Xun, Y.; Sun, J.-X.; Xu, J.-Z.; Liu, C.-Q.; Lu, Y.-C.; He, D.; et al. Identification of a Twelve Epithelial-Mesenchymal Transition-Related lncRNA Prognostic Signature in Kidney Clear Cell Carcinoma. Dis. Mrk. 2022, 2022, 8131007. [Google Scholar] [CrossRef]
- Nel, I.; Gauler, T.C.; Bublitz, K.; Lazaridis, L.; Goergens, A.; Giebel, B.; Schuler, M.; Hoffmann, A.C. Circulating Tumor Cell Composition in Renal Cell Carcinoma. PLoS ONE 2016, 11, e0153018. [Google Scholar] [CrossRef]
- Hassan, S.; Blick, T.; Thompson, E.W.; Williams, E.D. Diversity of Epithelial-Mesenchymal Phenotypes in Circulating Tumour Cells from Prostate Cancer Patient-Derived Xenograft Models. Cancers 2021, 13, 2750. [Google Scholar] [CrossRef]
- Zhao, X.H.; Wang, Z.R.; Chen, C.L.; Di, L.; Bi, Z.F.; Li, Z.H.; Liu, Y.M. Molecular detection of epithelial-mesenchymal transition markers in circulating tumor cells from pancreatic cancer patients: Potential role in clinical practice. World J. Gastroenterol. 2019, 25, 138–150. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Liu, S.; Liu, Z.; Huang, J.; Pu, X.; Li, J.; Yang, D.; Deng, H.; Yang, N.; Xu, J. Classification of circulating tumor cells by epithelial-mesenchymal transition markers. PLoS ONE 2015, 10, e0123976. [Google Scholar] [CrossRef] [PubMed]
- Cappelletti, V.; Verzoni, E.; Ratta, R.; Vismara, M.; Silvestri, M.; Montone, R.; Miodini, P.; Reduzzi, C.; Claps, M.; Sepe, P.; et al. Analysis of Single Circulating Tumor Cells in Renal Cell Carcinoma Reveals Phenotypic Heterogeneity and Genomic Alterations Related to Progression. Int. J. Mol. Sci. 2020, 21, 1475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wen, L.; Guo, L.; Zhang, W.; Li, Y.; Jiang, W.; Di, X.; Ma, J.; Feng, L.; Zhang, K.; Shou, J. Cooperation Between the Inflammation and Coagulation Systems Promotes the Survival of Circulating Tumor Cells in Renal Cell Carcinoma Patients. Front. Oncol. 2019, 9, 504. [Google Scholar] [CrossRef] [PubMed]
- Guan, Y.; Xu, F.; Tian, J.; Wang, Y.; Guo, N.; Wan, Z.; He, M.; Gao, M.; Gao, K.; Chong, T. Prognostic value of circulating tumor cells and immune-inflammatory cells in patients with renal cell carcinoma. Urol. Oncol. 2022, 40, 167.e121–167.e132. [Google Scholar] [CrossRef]
- Hu, J.; Chen, Z.; Bao, L.; Zhou, L.; Hou, Y.; Liu, L.; Xiong, M.; Zhang, Y.; Wang, B.; Tao, Z.; et al. Single-Cell Transcriptome Analysis Reveals Intratumoral Heterogeneity in ccRCC, which Results in Different Clinical Outcomes. Mol. Ther. 2020, 28, 1658–1672. [Google Scholar] [CrossRef]
- Shen, C.; Hu, G.; Zhang, S.; Ao, X.; Zhou, Q.; Xiao, P.; Zhong, Y. Immunophenotypic characterization of sphere-forming cells derived from the human renal cell carcinoma cell line 786-O. Am. J. Transl. Res. 2018, 10, 3978–3990. [Google Scholar]
- Balcik-Ercin, P.; Cayrefourcq, L.; Soundararajan, R.; Mani, S.A.; Alix-Panabieres, C. Epithelial-to-Mesenchymal Plasticity in Circulating Tumor Cell Lines Sequentially Derived from a Patient with Colorectal Cancer. Cancers 2021, 13, 5408. [Google Scholar] [CrossRef]
- Lozar, T.; Gersak, K.; Cemazar, M.; Kuhar, C.G.; Jesenko, T. The biology and clinical potential of circulating tumor cells. Radiol. Oncol. 2019, 53, 131–147. [Google Scholar] [CrossRef] [Green Version]
- Friberg, S.; Nystrom, A. Cancer Metastases: Early Dissemination and Late Recurrences. Cancer Growth Metastasis 2015, 8, 43–49. [Google Scholar] [CrossRef]
- Dianat-Moghadam, H.; Azizi, M.; Eslami, S.Z.; Cortes-Hernandez, L.E.; Heidarifard, M.; Nouri, M.; Alix-Panabieres, C. The Role of Circulating Tumor Cells in the Metastatic Cascade: Biology, Technical Challenges, and Clinical Relevance. Cancers 2020, 12, 867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, Z.; Wu, J.; Lu, Y.; Chan, Y.T.; Zhang, C.; Wang, D.; Luo, D.; Huang, Y.; Feng, Y.; Wang, N. Circulating tumor cells in the early detection of human cancers. Int. J. Biol. Sci. 2022, 18, 3251–3265. [Google Scholar] [CrossRef] [PubMed]
- Dudani, S.; de Velasco, G.; Wells, J.C.; Gan, C.L.; Donskov, F.; Porta, C.; Fraccon, A.; Pasini, F.; Lee, J.L.; Hansen, A.; et al. Evaluation of Clear Cell, Papillary, and Chromophobe Renal Cell Carcinoma Metastasis Sites and Association With Survival. JAMA Netw. Open 2021, 4, e2021869. [Google Scholar] [CrossRef] [PubMed]
- Aceto, N. Bring along your friends: Homotypic and heterotypic circulating tumor cell clustering to accelerate metastasis. Biomed. J. 2020, 43, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Castro-Giner, F.; Aceto, N. Tracking cancer progression: From circulating tumor cells to metastasis. Genome. Med. 2020, 12, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiu, Y.; Zhang, X.; Deng, X.; Zhang, R.; Cai, Z.; Zhang, Z.; Liu, H. Circulating tumor cell-associated white blood cell cluster is associated with poor survival of patients with gastric cancer following radical gastrectomy. Eur. J. Surg. Oncol. 2022, 48, 1039–1045. [Google Scholar] [CrossRef] [PubMed]
- Suo, Y.; Xie, C.; Zhu, X.; Fan, Z.; Yang, Z.; He, H.; Wei, X. Proportion of circulating tumor cell clusters increases during cancer metastasis. Cytom. A 2017, 91, 250–253. [Google Scholar] [CrossRef] [Green Version]
- Turajlic, S.; Xu, H.; Litchfield, K.; Rowan, A.; Chambers, T.; Lopez, J.I.; Nicol, D.; O’Brien, T.; Larkin, J.; Horswell, S.; et al. Tracking Cancer Evolution Reveals Constrained Routes to Metastases: TRACERx Renal. Cell 2018, 173, 581–594 e512. [Google Scholar] [CrossRef] [Green Version]
- Turajlic, S.; Xu, H.; Litchfield, K.; Rowan, A.; Horswell, S.; Chambers, T.; O’Brien, T.; Lopez, J.I.; Watkins, T.B.K.; Nicol, D.; et al. Deterministic Evolutionary Trajectories Influence Primary Tumor Growth: TRACERx Renal. Cell 2018, 173, 595–610.e511. [Google Scholar] [CrossRef] [Green Version]
- Ye, Z.; Ding, Y.; Chen, Z.; Li, Z.; Ma, S.; Xu, Z.; Cheng, L.; Wang, X.; Zhang, X.; Ding, N.; et al. Detecting and phenotyping of aneuploid circulating tumor cells in patients with various malignancies. Cancer Biol. 2019, 20, 546–551. [Google Scholar] [CrossRef]
- Zhang, X.; Guo, X.; Zong, Y.; Xu, C.; Wang, J.; Zhang, B.; Liu, C.; Gong, Y.; Xue, L.; Ma, L.; et al. CTCs detection from intraoperative salvaged blood in RCC-IVC thrombus patients by negative enrichment and iFISH identification: A preliminary study. BMC Urol. 2021, 21, 89. [Google Scholar] [CrossRef] [PubMed]
- Guan, Y.; Xu, F.; Wang, Y.; Tian, J.; Wan, Z.; Wang, Z.; Chong, T. Identification of key genes and functions of circulating tumor cells in multiple cancers through bioinformatic analysis. BMC Med. Genom. 2020, 13, 140. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.-M.; Yoo, J.-S.; Moon, H.W.; Hur, K.J.; Choi, J.B.; Hong, S.-H.; Lee, J.Y.; Ha, U.S. Distinct mutation profiles between primary bladder cancer and circulating tumor cells warrant the use of circulating tumors cells as cellular resource for mutation follow-up. BMC Cancer 2020, 20, 1203. [Google Scholar] [CrossRef] [PubMed]
- Davis, A.A.; Zhang, Q.; Gerratana, L.; Shah, A.N.; Zhan, Y.; Qiang, W.; Finkelman, B.S.; Flaum, L.; Behdad, A.; Gradishar, W.J.; et al. Association of a novel circulating tumor DNA next-generating sequencing platform with circulating tumor cells (CTCs) and CTC clusters in metastatic breast cancer. Breast Cancer Res. 2019, 21, 137. [Google Scholar] [CrossRef]
- Khan, M.I.; Czarnecka, A.M.; Lewicki, S.; Helbrecht, I.; Brodaczewska, K.; Koch, I.; Zdanowski, R.; Krol, M.; Szczylik, C. Comparative Gene Expression Profiling of Primary and Metastatic Renal Cell Carcinoma Stem Cell-Like Cancer Cells. PLoS ONE 2016, 11, e0165718. [Google Scholar] [CrossRef] [Green Version]
- Shi, D.; Che, J.; Yan, Y.; Peng, B.; Yao, X.; Guo, C. Expression and clinical value of CD105 in renal cell carcinoma based on data mining in The Cancer Genome Atlas. Exp. Med. 2019, 17, 4499–4505. [Google Scholar] [CrossRef] [Green Version]
- Fiedorowicz, M.; Khan, M.I.; Strzemecki, D.; Orzel, J.; Welniak-Kaminska, M.; Sobiborowicz, A.; Wieteska, M.; Rogulski, Z.; Cheda, L.; Wargocka-Matuszewska, W.; et al. Renal carcinoma CD105-/CD44- cells display stem-like properties in vitro and form aggressive tumors in vivo. Sci. Rep. 2020, 10, 5379. [Google Scholar] [CrossRef] [Green Version]
- Palmela Leitao, T.; Miranda, M.; Polido, J.; Morais, J.; Corredeira, P.; Alves, P.; Oliveira, T.; Pereira, E.S.R.; Fernandes, R.; Ferreira, J.; et al. Circulating tumor cell detection methods in renal cell carcinoma: A systematic review. Crit. Rev. Oncol. Hematol. 2021, 161, 103331. [Google Scholar] [CrossRef]
- Hu, M.; Wang, Z.; Wu, Z.; Ding, P.; Pei, R.; Wang, Q.; Xing, C. Circulating tumor cells in colorectal cancer in the era of precision medicine. J. Mol. Med. 2022, 100, 197–213. [Google Scholar] [CrossRef]
- Rushton, A.J.; Nteliopoulos, G.; Shaw, J.A.; Coombes, R.C. A Review of Circulating Tumour Cell Enrichment Technologies. Cancers 2021, 13, 970. [Google Scholar] [CrossRef]
- Basso, U.; Facchinetti, A.; Rossi, E.; Maruzzo, M.; Conteduca, V.; Aieta, M.; Massari, F.; Fraccon, A.P.; Mucciarini, C.; Sava, T.; et al. Prognostic Role of Circulating Tumor Cells in Metastatic Renal Cell Carcinoma: A Large, Multicenter, Prospective Trial. Oncology 2021, 26, 740–750. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Tian, Z.; Zhang, L.; Hou, S.; Hu, S.; Wu, J.; Jing, Y.; Sun, H.; Yu, F.; Zhao, L.; et al. Combined cell surface carbonic anhydrase 9 and CD147 antigens enable high-efficiency capture of circulating tumor cells in clear cell renal cell carcinoma patients. Oncotarget 2016, 7, 59877–59891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bade, R.M.; Schehr, J.L.; Emamekhoo, H.; Gibbs, B.K.; Rodems, T.S.; Mannino, M.C.; Desotelle, J.A.; Heninger, E.; Stahlfeld, C.N.; Sperger, J.M.; et al. Development and initial clinical testing of a multiplexed circulating tumor cell assay in patients with clear cell renal cell carcinoma. Mol. Oncol. 2021, 15, 2330–2344. [Google Scholar] [CrossRef] [PubMed]
- Tian, D.; Zhang, M.; Zheng, G.; Zhang, Y.; Li, Y.; Lin, P.; Li, H.; Jiao, W.; Niu, H. Clinical significance of phenotyping and karyotyping of detecting circulating tumor cells in renal cell carcinoma using subtraction enrichment and immunostaining-fluorescence in situ hybridization (SE-iFISH). Int. Urol. Nephrol. 2020, 52, 2281–2287. [Google Scholar] [CrossRef]
- Habli, Z.; AlChamaa, W.; Saab, R.; Kadara, H.; Khraiche, M.L. Circulating Tumor Cell Detection Technologies and Clinical Utility: Challenges and Opportunities. Cancers 2020, 12, 1930. [Google Scholar] [CrossRef]
- Coumans, F.A.W.; Van Dalum, G.; Beck, M.; Terstappen, L.W.M.M. Filtration Parameters Influencing Circulating Tumor Cell Enrichment from Whole Blood. PLoS ONE 2013, 8, e61774. [Google Scholar] [CrossRef] [Green Version]
- Bai, M.; Zou, B.; Wang, Z.; Li, P.; Wang, H.; Ou, Y.; Cui, K.; Bian, J.; Li, S.; Xu, X. Comparison of two detection systems for circulating tumor cells among patients with renal cell carcinoma. Int. Urol. Nephrol. 2018, 50, 1801–1809. [Google Scholar] [CrossRef]
- Takagi, H.; Dong, L.; Kuczler, M.D.; Lombardo, K.; Hirai, M.; Amend, S.R.; Pienta, K.J. Analysis of the Circulating Tumor Cell Capture Ability of a Slit Filter-Based Method in Comparison to a Selection-Free Method in Multiple Cancer Types. Int. J. Mol. Sci. 2020, 21, 9031. [Google Scholar] [CrossRef]
- Guan, Y.; Xu, F.; Tian, J.; Gao, K.; Wan, Z.; Wang, Y.; Gao, M.; Wang, Z.; Chong, T. The prognostic value of circulating tumour cells (CTCs) and CTC white blood cell clusters in patients with renal cell carcinoma. BMC Cancer 2021, 21, 826. [Google Scholar] [CrossRef]
- Zhang, P.; Wang, Z.; Yang, X.; Gao, K.; Li, M.; Chong, T. The Significance of Detection of Circulating Tumor Cells and Beclin1 in Peripheral Blood of Patients with Renal Cell Carcinoma. Crit. Rev. Eukaryot. Gene Expr. 2020, 30, 483–492. [Google Scholar] [CrossRef]
- Wang, Z.L.; Zhang, P.; Li, H.C.; Yang, X.J.; Zhang, Y.P.; Li, Z.L.; Xue, L.; Xue, Y.Q.; Li, H.L.; Chen, Q.; et al. Dynamic changes of different phenotypic and genetic circulating tumor cells as a biomarker for evaluating the prognosis of RCC. Cancer Biol. 2019, 20, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Bobek, V.; Kolostova, K. Isolation and Characterization of CTCs from Patients with Cancer of a Urothelial Origin. Methods Mol. Biol. 2018, 1655, 275–286. [Google Scholar] [CrossRef] [PubMed]
- De Alwis, R.; Hansson, J.; Lindgren, D.; Schoch, S.; Tejera, A.; Scholtz, B.; Elfving, P.; Moller, C.; Nilsson, H.; Johansson, M.; et al. Size-based isolation and detection of renal carcinoma cells from whole blood. Mol. Clin. Oncol. 2022, 16, 101. [Google Scholar] [CrossRef] [PubMed]
- Russo, G.I.; Musso, N.; Romano, A.; Caruso, G.; Petralia, S.; Lanzano, L.; Broggi, G.; Camarda, M. The Role of Dielectrophoresis for Cancer Diagnosis and Prognosis. Cancers 2021, 14, 198. [Google Scholar] [CrossRef] [PubMed]
- Staudte, S.; Klinghammer, K.; Jurmeister, P.S.; Jank, P.; Blohmer, J.U.; Liebs, S.; Rhein, P.; Hauser, A.E.; Tinhofer, I. Multiparametric Phenotyping of Circulating Tumor Cells for Analysis of Therapeutic Targets, Oncogenic Signaling Pathways and DNA Repair Markers. Cancers 2022, 14, 2810. [Google Scholar] [CrossRef]
- Broncy, L.; Njima, B.B.; Méjean, A.; Béroud, C.; Ben Romdhane, K.; Ilie, M.; Hofman, V.; Muret, J.; Hofman, P.; Chaabouni Bouhamed, H.; et al. Single-cell genetic analysis validates cytopathological identification of circulating cancer cells in patients with clear cell renal cell carcinoma. Oncotarget 2018, 9, 20058–20074. [Google Scholar] [CrossRef] [Green Version]
- Glennon, K.I.; Maralani, M.; Abdian, N.; Paccard, A.; Montermini, L.; Nam, A.J.; Arseneault, M.; Staffa, A.; Jandaghi, P.; Meehan, B.; et al. Rational Development of Liquid Biopsy Analysis in Renal Cell Carcinoma. Cancers 2021, 13, 5825. [Google Scholar] [CrossRef]
- Nayak, B.; Panaiyadiyan, S.; Singh, P.; Karmakar, S.; Kaushal, S.; Seth, A. Role of circulating tumor cells in patients with metastatic clear-cell renal cell carcinoma. Urol. Oncol. 2021, 39, 135.e139–135.e115. [Google Scholar] [CrossRef]
- Ge, L.; Song, Y.; Yang, F.; Zhao, G.; Lu, M.; Zhang, S.; Ma, L. Clinical significance of circulating tumor cells detection in renal cell carcinoma with thrombus: A STROBE-compliant study. Medicine 2020, 99, e20615. [Google Scholar] [CrossRef]
- Wu, C.; Xu, C.; Wang, G.; Zhang, D.; Zhao, X. Noninvasive circulating tumor cell and urine cellular XPC (rs2228001, A2815C) and XRCC1 (rs25487, G1196A) polymorphism detection as an effective screening panel for genitourinary system cancers. Transl. Cancer Res. 2019, 8, 2803–2812. [Google Scholar] [CrossRef]
- Kim, T.H. Detection of circulating tumour cells and their potential use as a biomarker for advanced renal cell carcinoma. Can. Urol. Assoc. J. 2019, 13, E285–E291. [Google Scholar] [CrossRef] [PubMed]
- Naoe, M.; Kusaka, C.; Ohta, M.; Hasebe, Y.; Unoki, T.; Shimoyama, H.; Nakasato, T.; Oshinomi, K.; Morita, J.; Fuji, K.; et al. Development of a Highly Sensitive Technique for Capturing Renal Cell Cancer Circulating Tumor Cells. Diagnostics 2019, 9, 96. [Google Scholar] [CrossRef] [Green Version]
- Nicinski, K.; Krajczewski, J.; Kudelski, A.; Witkowska, E.; Trzcinska-Danielewicz, J.; Girstun, A.; Kaminska, A. Detection of circulating tumor cells in blood by shell-isolated nanoparticle-enhanced Raman spectroscopy (SHINERS) in microfluidic device. Sci. Rep. 2019, 9, 9267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xing, T.; Wang, B.; Song, Y.; Zhang, S.; Ma, L. Candle soot-templated silica nanobiointerface chip for detecting circulating tumour cells from patients with urologic malignancies. RSC Adv. 2018, 8, 34566–34572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bu, J.; Nair, A.; Kubiatowicz, L.J.; Poellmann, M.J.; Jeong, W.J.; Reyes-Martinez, M.; Armstrong, A.J.; George, D.J.; Wang, A.Z.; Zhang, T.; et al. Surface engineering for efficient capture of circulating tumor cells in renal cell carcinoma: From nanoscale analysis to clinical application. Biosens Bioelectron 2020, 162, 112250. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.T.; Kim, Y.J.; Lee, T.H.; Cho, Y.H.; Chang, H.J.; Lee, H.M. Cytopathological Study of the Circulating Tumor Cells filtered from the Cancer Patients’ Blood using Hydrogel-based Cell Block Formation. Sci. Rep. 2018, 8, 15218. [Google Scholar] [CrossRef] [Green Version]
- Shapiro, D.D.; Virumbrales-Munoz, M.; Beebe, D.J.; Abel, E.J. Models of Renal Cell Carcinoma Used to Investigate Molecular Mechanisms and Develop New Therapeutics. Front. Oncol. 2022, 12, 871252. [Google Scholar] [CrossRef]
- Yang, X.; Zhang, D.; Chong, T.; Li, Y.; Wang, Z.; Zhang, P. Expression of CK19, CD105 and CD146 are associated with early metastasis in patients with renal cell carcinoma. Oncol. Lett. 2018, 15, 4229–4234. [Google Scholar] [CrossRef]
- Arai, T.; Sazuka, T.; Sato, H.; Kato, M.; Kamada, S.; Katsura, S.; Seito, A.; Miyamoto, S.; Wakai, K.; Takeuchi, N.; et al. A clinical investigation of recurrence and lost follow-up after renal cell carcinoma surgery: A single-center, long-term, large cohort, retrospective study. Int. J. Clin. Oncol. 2022, 27, 1467–1476. [Google Scholar] [CrossRef]
- Kim, S.H.; Park, B.; Hwang, E.C.; Hong, S.-H.; Jeong, C.W.; Kwak, C.; Byun, S.S.; Chung, J. A Retrospective, Multicenter, Long-Term Follow-Up Analysis of the Prognostic Characteristics of Recurring Non-Metastatic Renal Cell Carcinoma After Partial or Radical Nephrectomy. Front. Oncol. 2021, 11, 653002. [Google Scholar] [CrossRef]
- Jiang, H.; Gu, X.; Zuo, Z.; Tian, G.; Liu, J. Prognostic value of circulating tumor cells in patients with bladder cancer: A meta-analysis. PLoS ONE 2021, 16, e0254433. [Google Scholar] [CrossRef] [PubMed]
- Klezl, P.; Pospisilova, E.; Kolostova, K.; Sonsky, J.; Maly, O.; Grill, R.; Pawlak, I.; Bobek, V. Detection of Circulating Tumor Cells in Renal Cell Carcinoma: Disease Stage Correlation and Molecular Characterization. J. Clin. Med. 2020, 9, 1372. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Yu, Z.; Dong, B.; Zhu, M.; Guo, X.; Ma, Y.; Zhao, S.; Yang, T. Clinical significance of circulating tumour cells and Ki-67 in renal cell carcinoma. World J. Surg. Oncol. 2021, 19, 156. [Google Scholar] [CrossRef] [PubMed]
- Haga, N.; Onagi, A.; Koguchi, T.; Hoshi, S.; Ogawa, S.; Akaihata, H.; Hata, J.; Hiraki, H.; Honda, R.; Tanji, R.; et al. Perioperative Detection of Circulating Tumor Cells in Radical or Partial Nephrectomy for Renal Cell Carcinoma. Ann. Surg. Oncol. 2020, 27, 1272–1281. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Zhang, P.; Chong, Y.; Xue, Y.; Yang, X.; Li, H.; Wang, L.; Zhang, Y.; Chen, Q.; Li, Z.; et al. Perioperative Circulating Tumor Cells (CTCs), MCTCs, and CTC-White Blood Cells Detected by a Size-Based Platform Predict Prognosis in Renal Cell Carcinoma. Dis. Mrk. 2021, 2021, 9956142. [Google Scholar] [CrossRef] [PubMed]
- Andersson-Evelonn, E.; Vidman, L.; Kallberg, D.; Landfors, M.; Liu, X.; Ljungberg, B.; Hultdin, M.; Ryden, P.; Degerman, S. Combining epigenetic and clinicopathological variables improves specificity in prognostic prediction in clear cell renal cell carcinoma. J. Transl. Med. 2020, 18, 435. [Google Scholar] [CrossRef]
- Flores, B.C.T.; Correia, M.P.; Rodriguez, J.G.; Henrique, R.; Jeronimo, C. Bridging the Gaps between Circulating Tumor Cells and DNA Methylation in Prostate Cancer. Cancers 2021, 13, 4209. [Google Scholar] [CrossRef]
- Geertsen, L.; Koldby, K.M.; Thomassen, M.; Kruse, T.; Lund, L. Circulating Tumor DNA in Patients with Renal Cell Carcinoma. A Systematic Review of the Literature. Eur. Urol. Open Sci. 2022, 37, 27–35. [Google Scholar] [CrossRef]
- Tan, Z.; Yue, C.; Ji, S.; Zhao, C.; Jia, R.; Zhang, Y.; Liu, R.; Li, D.; Yu, Q.; Li, P.; et al. Assessment of PD-L1 Expression on Circulating Tumor Cells for Predicting Clinical Outcomes in Patients with Cancer Receiving PD-1/PD-L1 Blockade Therapies. Oncologist 2021, 26, e2227–e2238. [Google Scholar] [CrossRef]
- Chen, B.H.; Kao, C.C.; Xu, T.; Yang, Y.N.; Cha, T.L.; Tsai, Y.T.; Liu, S.Y.; Wu, S.T.; Meng, E.; Tsao, C.W.; et al. Determining programmed cell death ligand 1 expression in circulating tumor cells of patients with clear cell renal cell carcinoma and its correlation with response to programmed cell death protein 1 inhibitors. Int. J. Urol. 2022, 29, 947–954. [Google Scholar] [CrossRef]
- Chiang, P.J.; Xu, T.; Cha, T.L.; Tsai, Y.T.; Liu, S.Y.; Wu, S.T.; Meng, E.; Tsao, C.W.; Kao, C.C.; Chen, C.L.; et al. Programmed Cell Death Ligand 1 Expression in Circulating Tumor Cells as a Predictor of Treatment Response in Patients with Urothelial Carcinoma. Biology 2021, 10, 674. [Google Scholar] [CrossRef] [PubMed]
- Nagaya, N.; Kanayama, M.; Nagata, M.; Horie, S. The Surge in the Number of Circulating Tumor Cells Following Treatment with Sunitinib for Metastatic Renal Cell Carcinoma. Intern. Med. 2018, 57, 2695–2700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bootsma, M.; McKay, R.R.; Emamekhoo, H.; Bade, R.M.; Schehr, J.L.; Mannino, M.C.; Singh, A.; Wolfe, S.K.; Schultz, Z.D.; Sperger, J.; et al. Longitudinal Molecular Profiling of Circulating Tumor Cells in Metastatic Renal Cell Carcinoma. J. Clin. Oncol. 2022, 40, 3633–3641. [Google Scholar] [CrossRef] [PubMed]
- Mao, X.; Mei, R.; Yu, S.; Shou, L.; Zhang, W.; Li, K.; Qiu, Z.; Xie, T.; Sui, X. Emerging Technologies for the Detection of Cancer Micrometastasis. Technol. Cancer Res. Treat. 2022, 21, 15330338221100355. [Google Scholar] [CrossRef]
- Moon, D.H.; Lindsay, D.P.; Hong, S.; Wang, A.Z. Clinical indications for, and the future of, circulating tumor cells. Adv. Drug. Deliv. Rev. 2018, 125, 143–150. [Google Scholar] [CrossRef]
- Rousset, X.; Maillet, D.; Grolleau, E.; Barthelemy, D.; Calattini, S.; Brevet, M.; Balandier, J.; Raffin, M.; Geiguer, F.; Garcia, J.; et al. Embryonated Chicken Tumor Xenografts Derived from Circulating Tumor Cells as a Relevant Model to Study Metastatic Dissemination: A Proof of Concept. Cancers 2022, 14, 4085. [Google Scholar] [CrossRef]
- Bu, J.; Lee, T.H.; Poellmann, M.J.; Rawding, P.A.; Jeong, W.J.; Hong, R.S.; Hyun, S.H.; Eun, H.S.; Hong, S. Tri-modal liquid biopsy: Combinational analysis of circulating tumor cells, exosomes, and cell-free DNA using machine learning algorithm. Clin. Transl. Med. 2021, 11, e499. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Couto-Cunha, A.; Jerónimo, C.; Henrique, R. Circulating Tumor Cells as Biomarkers for Renal Cell Carcinoma: Ready for Prime Time? Cancers 2023, 15, 287. https://doi.org/10.3390/cancers15010287
Couto-Cunha A, Jerónimo C, Henrique R. Circulating Tumor Cells as Biomarkers for Renal Cell Carcinoma: Ready for Prime Time? Cancers. 2023; 15(1):287. https://doi.org/10.3390/cancers15010287
Chicago/Turabian StyleCouto-Cunha, Anabela, Carmen Jerónimo, and Rui Henrique. 2023. "Circulating Tumor Cells as Biomarkers for Renal Cell Carcinoma: Ready for Prime Time?" Cancers 15, no. 1: 287. https://doi.org/10.3390/cancers15010287
APA StyleCouto-Cunha, A., Jerónimo, C., & Henrique, R. (2023). Circulating Tumor Cells as Biomarkers for Renal Cell Carcinoma: Ready for Prime Time? Cancers, 15(1), 287. https://doi.org/10.3390/cancers15010287