

Metastatic Breast Cancer: Review of Emerging Nanotherapeutics



Abstract
:Simple Summary
Abstract
1. Background
2. Metastatic Breast Cancer
2.1. Nature and Pathophysiology
2.2. Current Treatment Regime for Metastatic BC and Drawbacks
3. Nanotherapeutics for Breast Cancer Bone Metastasis
3.1. Alendronate Functionalized Nanocarriers
3.2. Zoledronic Acid-Functionalized Nanocarriers
3.3. Other Nanocarriers
4. Nanotherapeutics for Brain Metastasis
4.1. Liposome-Based Delivery Carriers
4.2. Photothermal and Photodynamic Therapies
4.3. Polymeric Nanoparticles
4.4. Other Drug Delivery Carriers
5. Lung Metastasis of Breast Cancer
5.1. Biomimetic Delivery Systems
5.2. Multifunctional Polymeric Nanoparticles
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Liang, Y.; Zhang, H.; Song, X.; Yang, Q. Metastatic Heterogeneity of Breast Cancer: Molecular Mechanism and Potential Therapeutic Targets. Semin. Cancer Biol. 2020, 60, 14–27. [Google Scholar] [CrossRef] [PubMed]
- Giaquinto, A.N.; Sung, H.; Miller, K.D.; Kramer, J.L.; Newman, L.A.; Minihan, A.; Jemal, A.; Siegel, R.L. Breast Cancer Statistics, 2022. CA Cancer J. Clin. 2022, 72, 524–541. [Google Scholar] [CrossRef] [PubMed]
- Mariotto, A.B.; Etzioni, R.; Hurlbert, M.; Penberthy, L.; Mayer, M. Estimation of the Number of Women Living with Metastatic Breast Cancer in the United States. Cancer Epidemiol. Biomark. Prev. 2017, 26, 809–815. [Google Scholar] [CrossRef]
- Wang, L.; Zhang, S.; Wang, X. The Metabolic Mechanisms of Breast Cancer Metastasis. Front. Oncol. 2021, 10, 602416. [Google Scholar] [CrossRef] [PubMed]
- Fares, J.; Fares, M.Y.; Khachfe, H.H.; Salhab, H.A.; Fares, Y. Molecular Principles of Metastasis: A Hallmark of Cancer Revisited. Signal Transduct. Target. Ther. 2020, 5, 28. [Google Scholar] [CrossRef] [PubMed]
- Tulotta, C.; Ottewell, P. The Role of IL-1B in Breast Cancer Bone Metastasis. Endocr. Relat. Cancer 2018, 25, R421–R434. [Google Scholar] [CrossRef]
- Xiong, Z.; Deng, G.; Huang, X.; Li, X.; Xie, X.; Wang, J.; Shuang, Z.; Wang, X. Bone Metastasis Pattern in Initial Metastatic Breast Cancer: A Population-Based Study. Cancer Manag. Res. 2018, 10, 287–295. [Google Scholar] [CrossRef]
- Smid, M.; Wang, Y.; Zhang, Y.; Sieuwerts, A.M.; Yu, J.; Klijn, J.G.M.; Foekens, J.A.; Martens, J.W.M. Subtypes of Breast Cancer Show Preferential Site of Relapse. Cancer Res. 2008, 68, 3108–3114. [Google Scholar] [CrossRef]
- Prasad, M.; Lambe, U.P.; Brar, B.; Shah, I.; Manimegalai, J.; Ranjan, K.; Rao, R.; Kumar, S.; Mahant, S.; Khurana, S.K.; et al. Nanotherapeutics: An Insight into Healthcare and Multi-Dimensional Applications in Medical Sector of the Modern World. Biomed. Pharmacother. 2018, 97, 1521–1537. [Google Scholar] [CrossRef]
- Thakkar, S.; Sharma, D.; Kalia, K.; Tekade, R.K. Tumor Microenvironment Targeted Nanotherapeutics for Cancer Therapy and Diagnosis: A Review. Acta Biomater. 2020, 101, 43–68. [Google Scholar] [CrossRef]
- Krishnan, S.R.; George, S.K. Nanotherapeutics in Cancer Prevention, Diagnosis and Treatment. In Pharmacology and Therapeutics; IntechOpen: London, UK, 2014. [Google Scholar] [CrossRef]
- Hamidi, H.; Ivaska, J. Every Step of the Way: Integrins in Cancer Progression and Metastasis. Nat. Rev. Cancer 2018, 18, 533–548. [Google Scholar] [CrossRef] [PubMed]
- Guan, X. Cancer Metastases: Challenges and Opportunities. Acta Pharm. Sin. B 2015, 5, 402–418. [Google Scholar] [CrossRef]
- Semenza, G.L. Molecular Mechanisms Mediating Metastasis of Hypoxic Breast Cancer Cells. Trends Mol. Med. 2012, 18, 534–543. [Google Scholar] [CrossRef]
- Savagner, P. The Epithelial-Mesenchymal Transition (EMT) Phenomenon. Ann. Oncol. 2010, 21, vii89–vii92. [Google Scholar] [CrossRef] [PubMed]
- Diepenbruck, M.; Christofori, G. Epithelial-Mesenchymal Transition (EMT) and Metastasis: Yes, No, Maybe? Curr. Opin. Cell Biol. 2016, 43, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Lamouille, S.; Xu, J.; Derynck, R. Fakultas Psikologi Dan Sosial Budaya Universitas Islam Indonesia Yogyakarta. Nat. Rev. Mol. Cell Biol. 2014, 15, 178–196. [Google Scholar] [CrossRef] [PubMed]
- Niveria, K.; Yadav, M.; Dangi, K.; Verma, A.K. Overcoming Challenges to Enable Targeting of Metastatic Breast Cancer Tumour Microenvironment with Nano-Therapeutics: Current Status and Future Perspectives. OpenNano 2022, 8, 100083. [Google Scholar] [CrossRef]
- Kim, M.Y. Breast Cancer Metastasis. Adv. Exp. Med. Biol. 2021, 1187, 183–204. [Google Scholar] [CrossRef]
- Cairns, R.; Khokha, R.; Hill, R. Molecular Mechanisms of Tumor Invasion and Metastasis: An Integrated View. Curr. Mol. Med. 2005, 3, 659–671. [Google Scholar] [CrossRef]
- Chen, Y.C.; Sosnoski, D.M.; Mastro, A.M. Breast Cancer Metastasis to the Bone: Mechanisms of Bone Loss. Breast Cancer Res. 2010, 12, 215. [Google Scholar] [CrossRef]
- Leone, J.P.; Leone, B.A. Breast Cancer Brain Metastases: The Last Frontier. Exp. Hematol. Oncol. 2015, 4, 33. [Google Scholar] [CrossRef]
- Karaman, S.; Detmar, M. Mechanisms of Lymphatic Metastasis. J. Clin. Investig. 2014, 124, 922–928. [Google Scholar] [CrossRef] [PubMed]
- DeSantis, C.E.; Ma, J.; Gaudet, M.M.; Newman, L.A.; Miller, K.D.; Goding Sauer, A.; Jemal, A.; Siegel, R.L. Breast Cancer Statistics, 2019. CA Cancer J. Clin. 2019, 69, 438–451. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.S.; Zhao, Z.; Yang, Z.N.; Xu, F.; Lu, H.J.; Zhu, Z.Y.; Shi, W.; Jiang, J.; Yao, P.P.; Zhu, H.P. Risk Factors and Preventions of Breast Cancer. Int. J. Biol. Sci. 2017, 13, 1387–1397. [Google Scholar] [CrossRef] [PubMed]
- Bale, R.; Putzer, D.; Schullian, P. Local Treatment of Breast Cancer Liver Metastasis. Cancers 2019, 11, 1341. [Google Scholar] [CrossRef] [PubMed]
- Rajput, A.; Goodman, M.; Bangiyev, L. Brain Metastases. In PET/MR Imaging A Case-Based Approach; Springer: Cham, Switzerland, 2017; pp. 337–338. [Google Scholar] [CrossRef]
- Zehr, K.R. Diagnosis and Treatment of Breast Cancer in Men. Radiol. Technol. 2019, 91, 51M–63M. [Google Scholar] [PubMed]
- Tong, C.W.S.; Wu, M.; Cho, W.C.S.; To, K.K.W. Recent Advances in the Treatment of Breast Cancer. Front. Oncol. 2018, 8, 227. [Google Scholar] [CrossRef]
- García-Aranda, M.; Redondo, M. Immunotherapy: A Challenge of Breast Cancer Treatment. Cancers 2019, 11, 1822. [Google Scholar] [CrossRef]
- Behravan, N.; Zahedipour, F.; Jaafari, M.R.; Johnston, T.P.; Sahebkar, A. Lipid-Based Nanoparticulate Delivery Systems for HER2-Positive Breast Cancer Immunotherapy. Life Sci. 2022, 291, 120294. [Google Scholar] [CrossRef]
- Chang, D.Y.; Ma, W.L.; Lu, Y.S. Role of Alpelisib in the Treatment of Pik3ca-Mutated Breast Cancer: Patient Selection and Clinical Perspectives. Ther. Clin. Risk Manag. 2021, 17, 193–207. [Google Scholar] [CrossRef]
- Yang, J.; Nie, J.; Ma, X.; Wei, Y.; Peng, Y.; Wei, X. Targeting PI3K in Cancer: Mechanisms and Advances in Clinical Trials 06 Biological Sciences 0601 Biochemistry and Cell Biology. Mol. Cancer 2019, 18, 26. [Google Scholar] [CrossRef] [PubMed]
- Ren, Y.; Song, J.; Li, X.; Luo, N. Rationale and Clinical Research Progress on PD-1/PD-L1-Based Immunotherapy for Metastatic Triple-Negative Breast Cancer. Int. J. Mol. Sci. 2022, 23, 8878. [Google Scholar] [CrossRef] [PubMed]
- Oner, G.; Önder, S.; Karatay, H.; Ak, N.; Tükenmez, M.; Müslümanoğlu, M.; İğci, A.; Dincçağ, A.; Özmen, V.; Aydiner, A.; et al. Clinical Impact of PD-L1 Expression in Triple-Negative Breast Cancer Patients with Residual Tumor Burden after Neoadjuvant Chemotherapy. World J. Surg. Oncol. 2021, 19, 264. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Pettaway, C.A.; Pagliaro, L.C. Treatment for Metastatic Penile Cancer After First-Line Chemotherapy Failure: Analysis of Response and Survival Outcomes. Urology 2015, 85, 1104–1110. [Google Scholar] [CrossRef] [PubMed]
- Gradishar, W.J. Taxanes for the Treatment of Metastatic Breast Cancer. Breast Cancer Basic Clin. Res. 2012, 6, 159–171. [Google Scholar] [CrossRef] [PubMed]
- Anastasiadi, Z.; Lianos, G.D.; Ignatiadou, E.; Harissis, H.V.; Mitsis, M. Breast Cancer in Young Women: An Overview. Updat. Surg. 2017, 69, 313–317. [Google Scholar] [CrossRef]
- Kemp, J.A.; Kwon, Y.J. Cancer Nanotechnology: Current Status and Perspectives. Nano Converg. 2021, 8, 34. [Google Scholar] [CrossRef]
- Rodríguez, F.; Caruana, P.; De la Fuente, N.; Español, P.; Gámez, M.; Balart, J.; Llurba, E.; Rovira, R.; Ruiz, R.; Martín-Lorente, C.; et al. Nano-Based Approved Pharmaceuticals for Cancer Treatment: Present and Future Challenges. Biomolecules 2022, 12, 784. [Google Scholar] [CrossRef]
- Schmid, P.; Adams, S.; Rugo, H.S.; Schneeweiss, A.; Barrios, C.H.; Iwata, H.; Diéras, V.; Hegg, R.; Im, S.-A.; Shaw Wright, G.; et al. Atezolizumab and Nab-Paclitaxel in Advanced Triple-Negative Breast Cancer. N. Engl. J. Med. 2018, 379, 2108–2121. [Google Scholar] [CrossRef]
- Gadi, V.; Gupta, D.; Shetty, S. Emerging Potentials of Nanotherapeutics in Breast Cancer Microenvironment Targeting. OpenNano 2022, 8, 100101. [Google Scholar] [CrossRef]
- Thakur, V.; Kutty, R.V. Recent Advances in Nanotheranostics for Triple Negative Breast Cancer Treatment. J. Exp. Clin. Cancer Res. 2019, 38, 430. [Google Scholar] [CrossRef]
- López-dolado, E. Engineering Biomaterials for Neural Applications; Springer: Cham, Switzerland, 2022; ISBN 9783031114090. [Google Scholar]
- Luo, X.; Zhang, Q.; Chen, H.; Hou, K.; Zeng, N.; Wu, Y. Smart Nanoparticles for Breast Cancer Treatment Based on the Tumor Microenvironment. Front. Oncol. 2022, 12, 2355. [Google Scholar] [CrossRef] [PubMed]
- Behzadi, P.; Sameer, A.S.; Nissar, S.; Banday, M.Z.; Gajdács, M.; García-Perdomo, H.A.; Akhtar, K.; Pinheiro, M.; Magnusson, P.; Sarshar, M.; et al. The Interleukin-1 (IL-1) Superfamily Cytokines and Their Single Nucleotide Polymorphisms (SNPs). J. Immunol. Res. 2022, 2022, 2054431. [Google Scholar] [CrossRef] [PubMed]
- Brook, N.; Brook, E.; Dharmarajan, A.; Dass, C.R.; Chan, A. Breast Cancer Bone Metastases: Pathogenesis and Therapeutic Targets. Int. J. Biochem. Cell Biol. 2018, 96, 63–78. [Google Scholar] [CrossRef] [PubMed]
- Guise, T.A. Molecular Mechanism of Osteolytic Bone Metastases. Cancer 2000, 88, 2892–2898. [Google Scholar] [CrossRef]
- Berenson, J.R.; Rajdev, L.; Broder, M. Pathophysiology of Bone Metastases. Cancer Biol. Ther. 2006, 5, 1078–1081. [Google Scholar] [CrossRef]
- Coleman, R.E. Metastatic Bone Disease: Clinical Features, Pathophysiology and Treatment Strategies. Cancer Treat. Rev. 2001, 27, 165–176. [Google Scholar] [CrossRef]
- Wang, M.; Xia, F.; Wei, Y.; Wei, X. Molecular Mechanisms and Clinical Management of Cancer Bone Metastasis. Bone Res. 2020, 8, 30. [Google Scholar] [CrossRef]
- Suvannasankha, A.; Chirgwin, J.M. Role of Bone-Anabolic Agents in the Treatment of Breast Cancer Bone Metastases. Breast Cancer Res. 2014, 16, 484. [Google Scholar] [CrossRef]
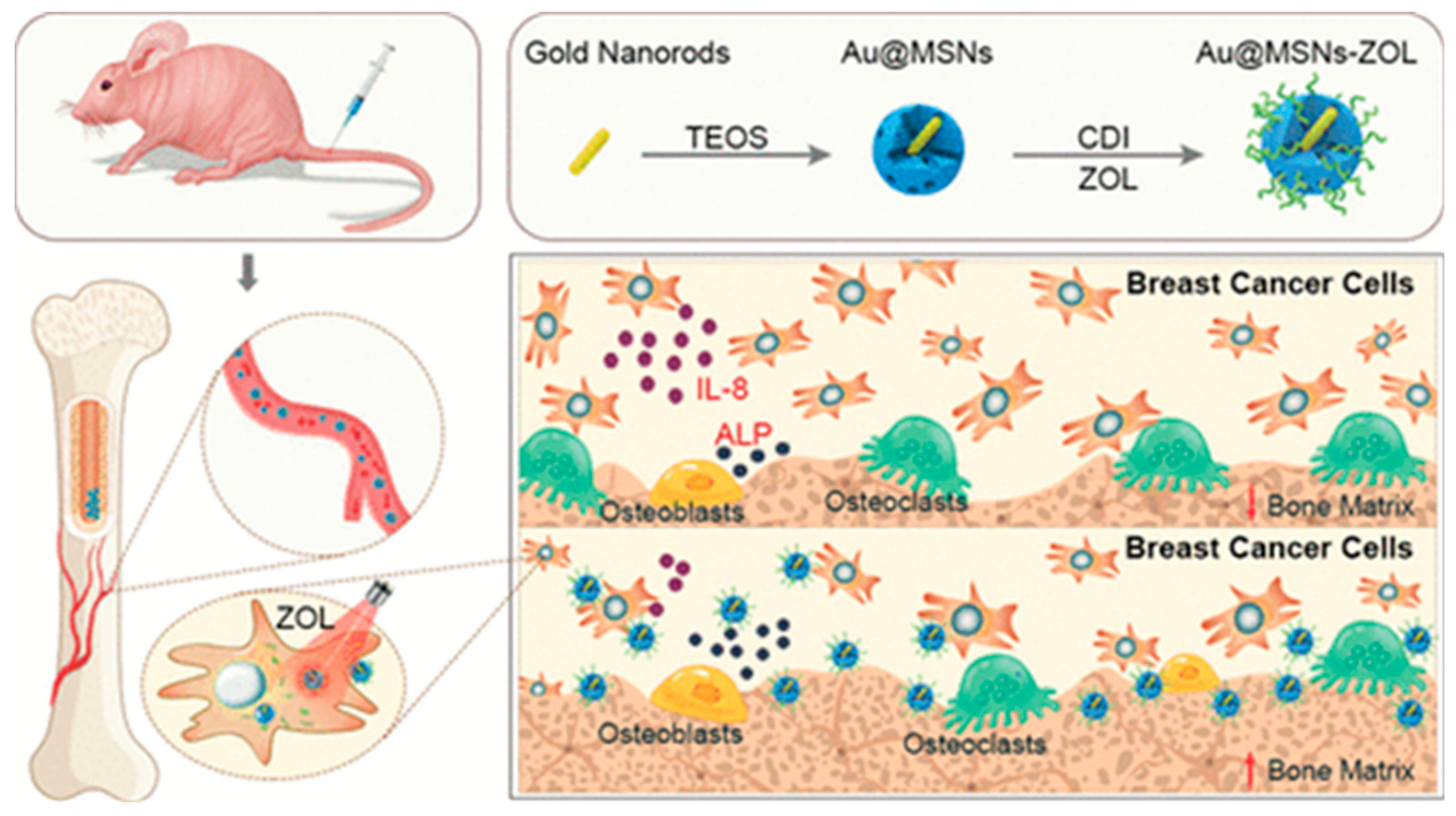
- Sun, W.; Ge, K.; Jin, Y.; Han, Y.; Zhang, H.; Zhou, G.; Yang, X.; Liu, D.; Liu, H.; Liang, X.J.; et al. Bone-Targeted Nanoplatform Combining Zoledronate and Photothermal Therapy to Treat Breast Cancer Bone Metastasis. ACS Nano 2019, 13, 7556–7567. [Google Scholar] [CrossRef]
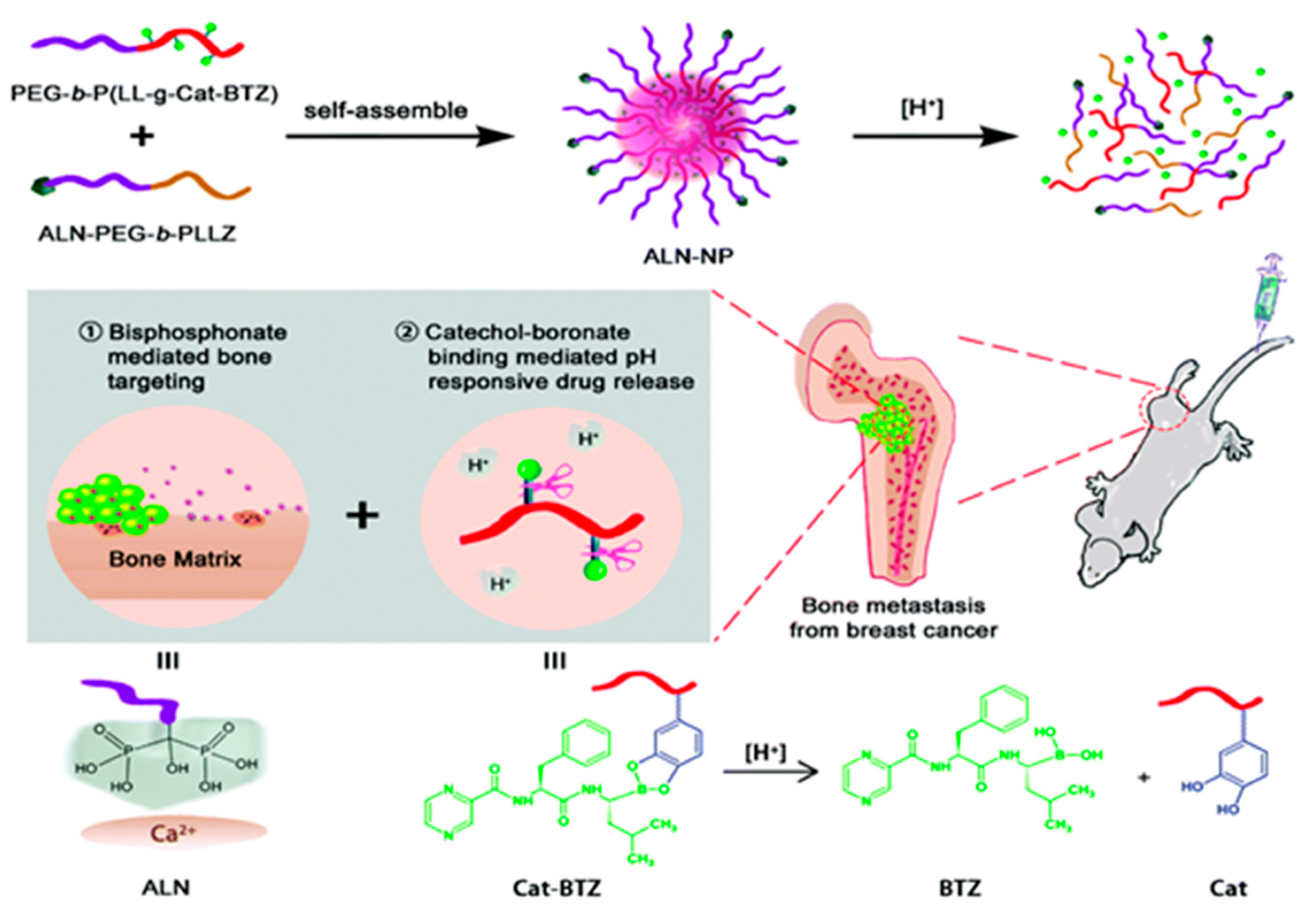
- Zhu, J.; Huo, Q.; Xu, M.; Yang, F.; Li, Y.; Shi, H.; Niu, Y.; Liu, Y. Bortezomib-Catechol Conjugated Prodrug Micelles: Combining Bone Targeting and Aryl Boronate-Based PH-Responsive Drug Release for Cancer Bone-Metastasis Therapy. Nanoscale 2018, 10, 18387–18397. [Google Scholar] [CrossRef]
- Katsumi, H.; Yamashita, S.; Morishita, M.; Yamamoto, A. Bone-Targeted Drug Delivery Systems and Strategies for Treatment of Bone Metastasis. Chem. Pharm. Bull. 2020, 68, 560–566. [Google Scholar] [CrossRef]
- Shao, H.; Varamini, P. Breast Cancer Bone Metastasis: A Narrative Review of Emerging Targeted Drug Delivery Systems. Cells 2022, 11, 388. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Cai, X.; Yang, J.; Wang, C.; Tong, L.; Xiao, J.; Li, L. A Targeted and PH-Responsive Bortezomib Nanomedicine in the Treatment of Metastatic Bone Tumors. ACS Appl. Mater. Interfaces 2018, 10, 41003–41011. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Huang, Y.; Huang, Z.; Jiang, Y.; Sun, X.; Shen, Y.; Chu, W.; Zhao, C. Bisphosphonate-Functionalized Coordination Polymer Nanoparticles for the Treatment of Bone Metastatic Breast Cancer. J. Control. Release 2017, 264, 76–88. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.H.; Liu, T.I.; Chuang, C.L.; Chen, H.H.; Chiang, W.H.; Chiu, H.C. Alendronate/Folic Acid-Decorated Polymeric Nanoparticles for Hierarchically Targetable Chemotherapy against Bone Metastatic Breast Cancer. J. Mater. Chem. B 2020, 8, 3789–3800. [Google Scholar] [CrossRef] [PubMed]
- Kang, N.W.; Lee, J.Y.; Kim, D.D. Hydroxyapatite-Binding Albumin Nanoclusters for Enhancing Bone Tumor Chemotherapy. J. Control. Release 2022, 342, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Dong, X.; Zou, S.; Guo, C.; Wang, K.; Zhao, F.; Fan, H.; Yin, J.; Chen, D. Multifunctional Redox-Responsive and CD44 Receptor Targeting Polymer-Drug Nanomedicine Based Curcumin and Alendronate: Synthesis, Characterization and in Vitro Evaluation. Artif. Cells Nanomed. Biotechnol. 2018, 46, 168–177. [Google Scholar] [CrossRef]
- Wang, K.; Guo, C.; Dong, X.; Yu, Y.; Wang, B.; Liu, W.; Chen, D. In Vivo Evaluation of Reduction-Responsive Alendronate-Hyaluronan-Curcumin Polymer-Drug Conjugates for Targeted Therapy of Bone Metastatic Breast Cancer. Mol. Pharm. 2018, 15, 2764–2769. [Google Scholar] [CrossRef] [PubMed]
- Wen, W.; Guo, P.; Xue, H.Y.; Lun Wong, H. Development of Local Injectable, Bone-Targeting Nanocarriers of Triptolide for Treatment of Bone-Only Metastasis. Int. J. Pharm. 2022, 625, 122092. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Romanova, S.; Wang, S.; Hyun, M.A.; Zhang, C.; Cohen, S.M.; Singh, R.K.; Bronich, T.K. Alendronate-Modified Polymeric Micelles for the Treatment of Breast Cancer Bone Metastasis. Mol. Pharm. 2019, 16, 2872–2883. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.P.; Ye, W.L.; Liu, D.Z.; Cui, H.; Cheng, Y.; Liu, M.; Zhang, B.L.; Mei, Q.B.; Zhou, S.Y. Redox and PH Dual Sensitive Bone Targeting Nanoparticles to Treat Breast Cancer Bone Metastases and Inhibit Bone Resorption. Nanoscale 2017, 9, 6264–6277. [Google Scholar] [CrossRef] [PubMed]
- Pham, T.T.; Nguyen, H.T.; Phung, C.D.; Pathak, S.; Regmi, S.; Ha, D.H.; Kim, J.O.; Yong, C.S.; Kim, S.K.; Choi, J.E.; et al. Targeted Delivery of Doxorubicin for the Treatment of Bone Metastasis from Breast Cancer Using Alendronate-Functionalized Graphene Oxide Nanosheets. J. Ind. Eng. Chem. 2019, 76, 310–317. [Google Scholar] [CrossRef]
- Huang, Y.; Xiao, Z.; Guan, Z.; Shen, Y.; Jiang, Y.; Xu, X.; Huang, Z.; Zhao, C. A Light-Triggered Self-Reinforced Nanoagent for Targeted Chemo-Photodynamic Therapy of Breast Cancer Bone Metastases via ER Stress and Mitochondria Mediated Apoptotic Pathways. J. Control. Release 2020, 319, 119–134. [Google Scholar] [CrossRef]
- Vanderburgh, J.; Hill, J.L.; Gupta, M.K.; Kwakwa, K.A.; Wang, S.K.; Moyer, K.; Bedingfield, S.K.; Merkel, A.R.; D’Arcy, R.; Guelcher, S.A.; et al. Tuning Ligand Density to Optimize Pharmacokinetics of Targeted Nanoparticles for Dual Protection against Tumor-Induced Bone Destruction. ACS Nano 2020, 14, 311–327. [Google Scholar] [CrossRef]
- Caraglia, M.; Marra, M.; Naviglio, S.; Botti, G.; Addeo, R.; Abbruzzese, A. Zoledronic Acid: An Unending Tale for an Antiresorptive Agent. Expert Opin. Pharmacother. 2010, 11, 141–154. [Google Scholar] [CrossRef]
- Chaudhari, K.R.; Kumar, A.; Khandelwal, V.K.M.; Mishra, A.K.; Monkkonen, J.; Murthy, R.S.R. Targeting Efficiency and Biodistribution of Zoledronate Conjugated Docetaxel Loaded Pegylated Pbca Nanoparticles for Bone Metastasis. Adv. Funct. Mater. 2012, 22, 4101–4114. [Google Scholar] [CrossRef]
- Jiang, Z.; Li, J.; Chen, S.; Guo, Q.; Jing, Z.; Huang, B.; Pan, Y.; Wang, L.; Hu, Y. Zoledronate and SPIO Dual-Targeting Nanoparticles Loaded with ICG for Photothermal Therapy of Breast Cancer Tibial Metastasis. Sci. Rep. 2020, 10, 13675. [Google Scholar] [CrossRef]
- Pang, Y.; Fu, Y.; Li, C.; Wu, Z.; Cao, W.; Hu, X.; Sun, X.; He, W.; Cao, X.; Ling, D.; et al. Metal-Organic Framework Nanoparticles for Ameliorating Breast Cancer-Associated Osteolysis. Nano Lett. 2020, 20, 829–840. [Google Scholar] [CrossRef] [PubMed]
- Ross, M.H.; Esser, A.K.; Fox, G.C.; Schmieder, A.H.; Yang, X.; Hu, G.; Pan, D.; Su, X.; Xu, Y.; Novack, D.V.; et al. Bone-Induced Expression of Integrin B3 Enables Targeted Nanotherapy of Breast Cancer Metastases. Cancer Res. 2017, 77, 6299–6312. [Google Scholar] [CrossRef]
- Rostami, R.; Mittal, S.; Rostami, P.; Tavassoli, F.; Jabbari, B. Brain Metastasis in Breast Cancer: A Comprehensive Literature Review. J. Neurooncol. 2016, 127, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Cheng, X.; Hung, M.C. Breast Cancer Brain Metastases. Cancer Metastasis Rev. 2007, 26, 635–643. [Google Scholar] [CrossRef]
- Gavrilovic, I.T.; Posner, J.B. Brain Metastases: Epidemiology and Pathophysiology. J. Neurooncol. 2005, 75, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Arshad, F.; Wang, L.; Sy, C.; Avraham, S.; Avraham, H.K. Blood-Brain Barrier Integrity and Breast Cancer Metastasis to the Brain. Patholog. Res. Int. 2011, 2011, 920509. [Google Scholar] [CrossRef] [PubMed]
- Lorger, M.; Felding-Habermann, B. Capturing Changes in the Brain Microenvironment during Initial Steps of Breast Cancer Brain Metastasis. Am. J. Pathol. 2010, 176, 2958–2971. [Google Scholar] [CrossRef]
- Tosoni, A.; Ermani, M.; Brandes, A.A. The Pathogenesis and Treatment of Brain Metastases: A Comprehensive Review. Crit. Rev. Oncol. Hematol. 2004, 52, 199–215. [Google Scholar] [CrossRef]
- Eichler, A.F.; Chung, E.; Kodack, D.P.; Loeffler, J.S.; Fukumura, D.; Jain, R.K. The Biology of Brain Metastases-Translation to New Therapies. Nat. Rev. Clin. Oncol. 2011, 8, 344–356. [Google Scholar] [CrossRef]
- Bryan, S.; Witzel, I.; Borgmann, K.; Oliveira-Ferrer, L. Molecular Mechanisms Associated with Brain Metastases in Her2-Positive and Triple Negative Breast Cancers. Cancers 2021, 13, 4137. [Google Scholar] [CrossRef]
- Watase, C.; Shiino, S.; Shimoi, T.; Noguchi, E.; Kaneda, T.; Yamamoto, Y.; Yonemori, K.; Takayama, S.; Suto, A. Breast Cancer Brain Metastasis—Overview of Disease State, Treatment Options and Future Perspectives. Cancers 2021, 13, 1078. [Google Scholar] [CrossRef]
- Cao, K.I.; Lebas, N.; Gerber, S.; Levy, C.; Le Scodan, R.; Bourgier, C.; Pierga, J.Y.; Gobillion, A.; Savignoni, A.; Kirova, Y.M. Phase II Randomized Study of Whole-Brain Radiation Therapy with or without Concurrent Temozolomide for Brain Metastases from Breast Cancer. Ann. Oncol. 2015, 26, 89–94. [Google Scholar] [CrossRef]
- Bailleux, C.; Eberst, L.; Bachelot, T. Treatment Strategies for Breast Cancer Brain Metastases. Br. J. Cancer 2021, 124, 142–155. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, S.R.; Mishra, P.; Abraham, J. Neratinib, A Novel HER2-Targeted Tyrosine Kinase Inhibitor. Clin. Breast Cancer 2016, 16, 344–348. [Google Scholar] [CrossRef] [PubMed]
- Moy, B.; Kirkpatrick, P.; Kar, S.; Goss, P. Lapatinib. Nat. Rev. Drug Discov. 2007, 6, 431–432. [Google Scholar] [CrossRef]
- Tsang, R.Y.; Sadeghi, S.; Finn, R.S. Lapatinib, a Dual-Targeted Small Molecule Inhibitor of EGFR and HER2, in HER2-Amplified Breast Cancer: From Bench to Bedside. Clin. Med. Insights Ther. 2011, 3, 1–13. [Google Scholar] [CrossRef]
- Barok, M.; Joensuu, H.; Isola, J. Trastuzumab Emtansine: Mechanisms of Action and Drug Resistance. Breast Cancer Res. 2014, 16, 209. [Google Scholar] [CrossRef] [PubMed]
- Leone, J.P.; Trippa, L.; Milisits, L.; Andrews, C.; Ligibel, J.; Parsons, H.; Bi, W.; Zhao, J.; Winer, E.; Lin, N. TRLS-03. Phase II Trial of GDC-0084 in Combination with Trastuzumab for Patients with HER2-Positive Breast Cancer Brain Metastases (BCBM). Neurooncol. Adv. 2019, 1, 9. [Google Scholar] [CrossRef]
- Jerusalem, G.; Fasolo, A.; Dieras, V.; Cardoso, F.; Bergh, J.; Vittori, L.; Zhang, Y.; Massacesi, C.; Sahmoud, T.; Gianni, L. Phase i Trial of Oral MTOR Inhibitor Everolimus in Combination with Trastuzumab and Vinorelbine in Pre-Treated Patients with HER2-Overexpressing Metastatic Breast Cancer. Breast Cancer Res. Treat. 2011, 125, 447–455. [Google Scholar] [CrossRef]
- Doheny, D.; Manore, S.; Sirkisoon, S.R.; Zhu, D.; Aguayo, N.R.; Harrison, A.; Najjar, M.; Anguelov, M.; Cox, A.O.; Furdui, C.M.; et al. An FDA-Approved Antifungal, Ketoconazole, and Its Novel Derivative Suppress TGLI1-Mediated Breast Cancer Brain Metastasis by Inhibiting the DNA-Binding Activity of Brain Metastasis-Promoting Transcription Factor TGLI1. Cancers 2022, 14, 4256. [Google Scholar] [CrossRef] [PubMed]
- Brandl, M. Liposomes as Drug Carriers: A Technological Approach. Biotechnol. Annu. Rev. 2001, 7, 59–85. [Google Scholar] [CrossRef]
- Belhadj, Z.; Ying, M.; Cao, X.; Hu, X.; Zhan, C.; Wei, X.; Gao, J.; Wang, X.; Yan, Z.; Lu, W. Design of Y-Shaped Targeting Material for Liposome-Based Multifunctional Glioblastoma-Targeted Drug Delivery. J. Control. Release 2017, 255, 132–141. [Google Scholar] [CrossRef]
- Luo, Z.; Wu, S.; Zhou, J.; Xu, W.; Xu, Q.; Lu, L.; Xie, C.; Liu, Y.; Lu, W. All-Stage Targeted Therapy for the Brain Metastasis from Triple-Negative Breast Cancer. Acta Pharm. Sin. B 2022, 13, 359–371. [Google Scholar] [CrossRef] [PubMed]
- Du, J.; Shao, Y.; Hu, Y.; Chen, Y.; Cang, J.; Chen, X.; Pei, W.; Miao, F.; Shen, Y.; Muddassir, M.; et al. Multifunctional Liposomes Enable Active Targeting and Twinfilin 1 Silencing to Reverse Paclitaxel Resistance in Brain Metastatic Breast Cancer. ACS Appl. Mater. Interfaces 2021, 13, 23396–23409. [Google Scholar] [CrossRef] [PubMed]
- Mohammad, A.S.; Griffith, J.I.; Adkins, C.E.; Shah, N.; Sechrest, E.; Dolan, E.L.; Terrell-Hall, T.B.; Hendriks, B.S.; Lee, H.; Lockman, P.R. Liposomal Irinotecan Accumulates in Metastatic Lesions, Crosses the Blood-Tumor Barrier (BTB), and Prolongs Survival in an Experimental Model of Brain Metastases of Triple Negative Breast Cancer. Pharm. Res. 2018, 35, 31. [Google Scholar] [CrossRef] [PubMed]
- Koukouraki, S.; Fezoulidis, I.; Kelekis, N.; Kyrias, G.; Archimandritis, S.; Karkavitsas, N. High Intratumoural Accumulation of Stealth¨ Liposomal Doxorubicin (Caelyx¨) in Glioblastomas and in Metastatic Brain Tumours. Br. J. Cancer 2000, 83, 1281–1286. [Google Scholar] [CrossRef]
- Caraglia, M.; Addeo, R.; Costanzo, R.; Montella, L.; Faiola, V.; Marra, M.; Abbruzzese, A.; Palmieri, G.; Budillon, A.; Grillone, F.; et al. Phase II Study of Temozolomide plus Pegylated Liposomal Doxorubicin in the Treatment of Brain Metastases from Solid Tumours. Cancer Chemother. Pharmacol. 2006, 57, 34–39. [Google Scholar] [CrossRef]
- Wu, S.K.; Chiang, C.F.; Hsu, Y.H.; Lin, T.H.; Liou, H.C.; Fu, W.M.; Lin, W.L. Short-Time Focused Ultrasound Hyperthermia Enhances Liposomal Doxorubicin Delivery and Antitumor Efficacy for Brain Metastasis of Breast Cancer. Int. J. Nanomed. 2014, 9, 4485–4494. [Google Scholar] [CrossRef]
- Le Rhun, E.; Wallet, J.; Mailliez, A.; Le Deley, M.C.; Rodrigues, I.; Boulanger, T.; Lorgis, V.; Barrière, J.; Robin, Y.M.; Weller, M.; et al. Intrathecal Liposomal Cytarabine plus Systemic Therapy versus Systemic Chemotherapy Alone for Newly Diagnosed Leptomeningeal Metastasis from Breast Cancer. Neuro Oncol. 2020, 22, 524–538. [Google Scholar] [CrossRef]
- Doughty, A.C.V.; Hoover, A.R.; Layton, E.; Murray, C.K.; Howard, E.W.; Chen, W.R. Nanomaterial Applications in Photothermal Therapy for Cancer. Materials 2019, 12, 779. [Google Scholar] [CrossRef]
- Alamdari, S.G.; Amini, M.; Jalilzadeh, N.; Baradaran, B.; Mohammadzadeh, R.; Mokhtarzadeh, A.; Oroojalian, F. Recent Advances in Nanoparticle-Based Photothermal Therapy for Breast Cancer. J. Control. Release 2022, 349, 269–303. [Google Scholar] [CrossRef]
- Salimi, M.; Mosca, S.; Gardner, B.; Palombo, F.; Matousek, P.; Stone, N. Nanoparticle-Mediated Photothermal Therapy Limitation in Clinical Applications Regarding Pain Management. Nanomaterials 2022, 12, 922. [Google Scholar] [CrossRef]
- Tong, F.; Hu, H.; Xu, Y.; Zhou, Y.; Xie, R.; Lei, T.; Du, Y.; Yang, W.; He, S.; Huang, Y.; et al. Sensitized Photothermal Therapy of Breast Cancer and Brain Metastases. Acta Pharm. Sin. B 2022. [Google Scholar] [CrossRef]
- Carney, C.P.; Kapur, A.; Anastasiadis, P.; Ritzel, R.M.; Chen, C.; Woodworth, G.F.; Winkles, J.A.; Kim, A.J. Fn14-Directed DART Nanoparticles Selectively Target Neoplastic Cells in Preclinical Models of Triple-Negative Breast Cancer Brain Metastasis. Mol. Pharm. 2023, 20, 314–330. [Google Scholar] [CrossRef]
- Zhang, T.; Lip, H.; He, C.; Cai, P.; Wang, Z.; Henderson, J.T.; Rauth, A.M.; Wu, X.Y. Multitargeted Nanoparticles Deliver Synergistic Drugs across the Blood–Brain Barrier to Brain Metastases of Triple Negative Breast Cancer Cells and Tumor-Associated Macrophages. Adv. Healthc. Mater. 2019, 8, 1900543. [Google Scholar] [CrossRef] [PubMed]
- Wyatt, E.A.; Davis, M.E. Method of Establishing Breast Cancer Brain Metastases Affects Brain Uptake and Efficacy of Targeted, Therapeutic Nanoparticles. Bioeng. Transl. Med. 2019, 4, 30–37. [Google Scholar] [CrossRef]
- McAtee, C.O.; Barycki, J.J.; Simpson, M.A. Emerging Roles for Hyaluronidase in Cancer Metastasis and Therapy. Adv. Cancer Res. 2014, 123, 1–34. [Google Scholar] [CrossRef]
- Ju, X.; Chen, H.; Miao, T.; Ni, J.; Han, L. Prodrug Delivery Using Dual-Targeting Nanoparticles to Treat Breast Cancer Brain Metastases. Mol. Pharm. 2021, 18, 2694–2702. [Google Scholar] [CrossRef] [PubMed]
- Collet, G.; Grillon, C.; Nadim, M.; Kieda, C. Trojan Horse at Cellular Level for Tumor Gene Therapies. Gene 2013, 525, 208–216. [Google Scholar] [CrossRef]
- Levy, O.; Brennen, W.N.; Han, E.; Rosen, D.M.; Musabeyezu, J.; Safaee, H.; Ranganath, S.; Ngai, J.; Heinelt, M.; Milton, Y.; et al. A Prodrug-Doped Cellular Trojan Horse for the Potential Treatment of Prostate Cancer. Biomaterials 2016, 91, 140–150. [Google Scholar] [CrossRef]
- Choi, M.R.; Bardhan, R.; Stanton-Maxey, K.J.; Badve, S.; Nakshatri, H.; Stantz, K.M.; Cao, N.; Halas, N.J.; Clare, S.E. Delivery of Nanoparticles to Brain Metastases of Breast Cancer Using a Cellular Trojan Horse. Cancer Nanotechnol. 2012, 3, 47–54. [Google Scholar] [CrossRef]
- Hainfeld, J.F.; Ridwan, S.M.; Stanishevskiy, F.Y.; Smilowitz, H.M. Iodine Nanoparticle Radiotherapy of Human Breast Cancer Growing in the Brains of Athymic Mice. Sci. Rep. 2020, 10, 15627. [Google Scholar] [CrossRef]
- Lu, H.; Chen, T.; Wang, Y.; He, Y.; Pang, Z.; Wang, Y. Dual Targeting Micelles Loaded with Paclitaxel and Lapatinib for Combinational Therapy of Brain Metastases from Breast Cancer. Sci. Rep. 2022, 12, 2610. [Google Scholar] [CrossRef] [PubMed]
- Ngamcherdtrakul, W.; Bejan, D.S.; Cruz-Muñoz, W.; Reda, M.; Zaidan, H.Y.; Siriwon, N.; Marshall, S.; Wang, R.; Nelson, M.A.; Rehwaldt, J.P.C.; et al. Targeted Nanoparticle for Co-Delivery of HER2 SiRNA and a Taxane to Mirror the Standard Treatment of HER2+ Breast Cancer: Efficacy in Breast Tumor and Brain Metastasis. Small 2022, 18, 2107550. [Google Scholar] [CrossRef] [PubMed]
- Kennecke, H.; Yerushalmi, R.; Woods, R.; Cheang, M.C.U.; Voduc, D.; Speers, C.H.; Nielsen, T.O.; Gelmon, K. Metastatic Behavior of Breast Cancer Subtypes. J. Clin. Oncol. 2010, 28, 3271–3277. [Google Scholar] [CrossRef]
- Welter, S.; Jacobs, J.; Krbek, T.; Tötsch, M.; Stamatis, G. Pulmonary Metastases of Breast Cancer. When Is Resection Indicated? Eur. J. Cardio-Thorac. Surg. 2008, 34, 1228–1234. [Google Scholar] [CrossRef] [PubMed]
- Läubli, H.; Borsig, L. Selectins Promote Tumor Metastasis. Semin. Cancer Biol. 2010, 20, 169–177. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, I.C.; Groom, A.C.; Chambers, A.F. Cancer Spread and Micrometastasis Development: Quantitative Approaches for in Vivo Models. BioEssays 2002, 24, 885–893. [Google Scholar] [CrossRef] [PubMed]
- Medeiros, B.; Allan, A.L. Molecular Mechanisms of Breast Cancer Metastasis to the Lung: Clinical and Experimental Perspectives. Int. J. Mol. Sci. 2019, 20, 2272. [Google Scholar] [CrossRef]
- Padua, D.; Zhang, X.H.F.; Wang, Q.; Nadal, C.; Gerald, W.L.; Gomis, R.R.; Massagué, J. TGFβ Primes Breast Tumors for Lung Metastasis Seeding through Angiopoietin-like 4. Cell 2008, 133, 66–77. [Google Scholar] [CrossRef]
- Jin, L.; Han, B.; Siegel, E.; Cui, Y.; Giuliano, A.; Cui, X. Breast Cancer Lung Metastasis: Molecular Biology and Therapeutic Implications. Cancer Biol. Ther. 2018, 19, 858–868. [Google Scholar] [CrossRef]
- Zarychta, E.; Ruszkowska-Ciastek, B. Cooperation between Angiogenesis, Vasculogenesis, Chemotaxis, and Coagulation in Breast Cancer Metastases Development: Pathophysiological Point of View. Biomedicines 2022, 10, 300. [Google Scholar] [CrossRef]
- Torres, K.E.; Ravi, V.; Kin, K.; Yi, M.; Guadagnolo, B.A.; May, C.D.; Arun, B.K.; Hunt, K.K.; Lam, R.; Lahat, G.; et al. Long-Term Outcomes in Patients with Radiation-Associated Angiosarcomas of the Breast Following Surgery and Radiotherapy for Breast Cancer. Ann. Surg. Oncol. 2013, 20, 1267–1274. [Google Scholar] [CrossRef]
- Garrastazu Pereira, G.; Lawson, A.J.; Buttini, F.; Sonvico, F. Loco-Regional Administration of Nanomedicines for the Treatment of Lung Cancer. Drug Deliv. 2016, 23, 2881–2896. [Google Scholar] [CrossRef] [PubMed]
- Sukumar, U.K.; Bhushan, B.; Dubey, P.; Matai, I.; Sachdev, A.; Packirisamy, G. Emerging Applications of Nanoparticles for Lung Cancer Diagnosis and Therapy. Int. Nano Lett. 2013, 3, 45. [Google Scholar] [CrossRef]
- Guido, C.; Maiorano, G.; Cortese, B.; D’amone, S.; Palamà, I.E. Biomimetic Nanocarriers for Cancer Target Therapy. Bioengineering 2020, 7, 111. [Google Scholar] [CrossRef]
- Fu, J.; Wang, D.; Mei, D.; Zhang, H.; Wang, Z.; He, B.; Dai, W.; Zhang, H.; Wang, X.; Zhang, Q. Macrophage Mediated Biomimetic Delivery System for the Treatment of Lung Metastasis of Breast Cancer. J. Control. Release 2015, 204, 11–19. [Google Scholar] [CrossRef]
- Zhao, H.; Li, L.; Zhang, J.; Zheng, C.; Ding, K.; Xiao, H.; Wang, L.; Zhang, Z. C-C Chemokine Ligand 2 (CCL2) Recruits Macrophage-Membrane-Camouflaged Hollow Bismuth Selenide Nanoparticles to Facilitate Photothermal Sensitivity and Inhibit Lung Metastasis of Breast Cancer. ACS Appl. Mater. Interfaces 2018, 10, 31124–31135. [Google Scholar] [CrossRef]
- Cao, H.; Dan, Z.; He, X.; Zhang, Z.; Yu, H.; Yin, Q.; Li, Y. Liposomes Coated with Isolated Macrophage Membrane Can Target Lung Metastasis of Breast Cancer. ACS Nano 2016, 10, 7738–7748. [Google Scholar] [CrossRef]
- Gong, C.; Yu, X.; You, B.; Wu, Y.; Wang, R.; Han, L.; Wang, Y.; Gao, S.; Yuan, Y. Macrophage-Cancer Hybrid Membrane-Coated Nanoparticles for Targeting Lung Metastasis in Breast Cancer Therapy. J. Nanobiotechnol. 2020, 18, 92. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Su, J.; Meng, Q.; Yin, Q.; Chen, L.; Gu, W.; Zhang, Z.; Yu, H.; Zhang, P.; Wang, S.; et al. Cancer Cell Membrane-Coated Gold Nanocages with Hyperthermia-Triggered Drug Release and Homotypic Target Inhibit Growth and Metastasis of Breast Cancer. Adv. Funct. Mater. 2017, 27, 1604300. [Google Scholar] [CrossRef]
- Li, Y.; Yan, T.; Chang, W.; Cao, C.; Deng, D. Fabricating an Intelligent Cell-like Nano-Prodrug: Via Hierarchical Self-Assembly Based on the DNA Skeleton for Suppressing Lung Metastasis of Breast Cancer. Biomater. Sci. 2019, 7, 3652–3661. [Google Scholar] [CrossRef]
- Su, J.; Sun, H.; Meng, Q.; Yin, Q.; Tang, S.; Zhang, P.; Chen, Y.; Zhang, Z.; Yu, H.; Li, Y. Long Circulation Red-Blood-Cell-Mimetic Nanoparticles with Peptide-Enhanced Tumor Penetration for Simultaneously Inhibiting Growth and Lung Metastasis of Breast Cancer. Adv. Funct. Mater. 2016, 26, 1243–1252. [Google Scholar] [CrossRef]
- Dan, Z.; Cao, H.; He, X.; Zhang, Z.; Zou, L.; Zeng, L.; Xu, Y.; Yin, Q.; Xu, M.; Zhong, D.; et al. A PH-Responsive Host-Guest Nanosystem Loading Succinobucol Suppresses Lung Metastasis of Breast Cancer. Theranostics 2016, 6, 435–445. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Hu, H.; Zhang, H.; Dai, W.; Weng, X.; Wang, X.; Zhang, Q. Effects of PEGylated Paclitaxel Nanocrystals on Breast Cancer and Its Lung Metastasis. Nanoscale 2015, 7, 10790–10800. [Google Scholar] [CrossRef] [PubMed]
- Cao, H.; Zhang, Z.; Zhao, S.; He, X.; Yu, H.; Yin, Q.; Zhang, Z.; Gu, W.; Chen, L.; Li, Y. Hydrophobic Interaction Mediating Self-Assembled Nanoparticles of Succinobucol Suppress Lung Metastasis of Breast Cancer by Inhibition of VCAM-1 Expression. J. Control. Release 2015, 205, 162–171. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.; Meng, Q.; Sun, H.; Su, J.; Yin, Q.; Zhang, Z.; Yu, H.; Chen, L.; Chen, Y.; Gu, W.; et al. Tumor-Microenvironment-Adaptive Nanoparticles Codeliver Paclitaxel and SiRNA to Inhibit Growth and Lung Metastasis of Breast Cancer. Adv. Funct. Mater. 2016, 26, 6033–6046. [Google Scholar] [CrossRef]
- Yin, J.; Lang, T.; Cun, D.; Zheng, Z.; Huang, Y.; Yin, Q.; Yu, H. PH-Sensitive Nano-Complexes Overcome Drug Resistance and Inhibit Metastasis of Breast Cancer by Silencing Akt Expression. Theranostics 2017, 7, 4204. [Google Scholar] [CrossRef] [PubMed]
- Shi, X.; Yang, X.; Liu, M.; Wang, R.; Qiu, N.; Liu, Y.; Yang, H.; Ji, J.; Zhai, G. Chondroitin Sulfate-Based Nanoparticles for Enhanced Chemo-Photodynamic Therapy Overcoming Multidrug Resistance and Lung Metastasis of Breast Cancer. Carbohydr. Polym. 2021, 254, 117459. [Google Scholar] [CrossRef]
- Liu, Y.; Xie, X.; Hou, X.; Shen, J.; Shi, J.; Chen, H.; He, Y.; Wang, Z.; Feng, N. Functional Oral Nanoparticles for Delivering Silibinin and Cryptotanshinone against Breast Cancer Lung Metastasis. J. Nanobiotechnol. 2020, 18, 83. [Google Scholar] [CrossRef]
- Xiao, J.; Duan, X.; Yin, Q.; Zhang, Z.; Yu, H.; Li, Y. Nanodiamonds-Mediated Doxorubicin Nuclear Delivery to Inhibit Lung Metastasis of Breast Cancer. Biomaterials 2013, 34, 9648–9656. [Google Scholar] [CrossRef]
- Xu, J.; Sun, J.; Ho, P.Y.; Luo, Z.; Ma, W.; Zhao, W.; Rathod, S.B.; Fernandez, C.A.; Venkataramanan, R.; Xie, W.; et al. Creatine Based Polymer for Codelivery of Bioengineered MicroRNA and Chemodrugs against Breast Cancer Lung Metastasis. Biomaterials 2019, 210, 25–40. [Google Scholar] [CrossRef]
- Hu, C.; Liu, X.; Ran, W.; Meng, J.; Zhai, Y.; Zhang, P.; Yin, Q.; Yu, H.; Zhang, Z.; Li, Y. Regulating Cancer Associated Fibroblasts with Losartan-Loaded Injectable Peptide Hydrogel to Potentiate Chemotherapy in Inhibiting Growth and Lung Metastasis of Triple Negative Breast Cancer. Biomaterials 2017, 144, 60–72. [Google Scholar] [CrossRef]
- Liu, R.; Xiao, W.; Hu, C.; Xie, R.; Gao, H. Theranostic Size-Reducible and No Donor Conjugated Gold Nanocluster Fabricated Hyaluronic Acid Nanoparticle with Optimal Size for Combinational Treatment of Breast Cancer and Lung Metastasis. J. Control. Release 2018, 278, 127–139. [Google Scholar] [CrossRef]
- Yu, W.; He, X.; Yang, Z.; Yang, X.; Xiao, W.; Liu, R.; Xie, R.; Qin, L.; Gao, H. Sequentially Responsive Biomimetic Nanoparticles with Optimal Size in Combination with Checkpoint Blockade for Cascade Synergetic Treatment of Breast Cancer and Lung Metastasis. Biomaterials 2019, 217, 119309. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Yang, F.; Wu, D.; Liu, Y.; Gao, Y.; Lian, H.; Zhang, H.; Yin, Z.; Wu, A.; Zeng, L. Ce6-Conjugated and Polydopamine-Coated Gold Nanostars with Enhanced Photoacoustic Imaging and Photothermal/Photodynamic Therapy to Inhibit Lung Metastasis of Breast Cancer. Nanoscale 2020, 12, 22173–22184. [Google Scholar] [CrossRef] [PubMed]
- Al Faraj, A.; Shaik, A.S.; Halwani, R.; Alfuraih, A. Magnetic Targeting and Delivery of Drug-Loaded SWCNTs Theranostic Nanoprobes to Lung Metastasis in Breast Cancer Animal Model: Noninvasive Monitoring Using Magnetic Resonance Imaging. Mol. Imaging Biol. 2016, 18, 315–324. [Google Scholar] [CrossRef]
- Qin, Y.; Chen, K.; Gu, W.; Dong, X.; Lei, R.; Chang, Y.; Bai, X.; Xia, S.; Zeng, L.; Zhang, J.; et al. Small Size Fullerenol Nanoparticles Suppress Lung Metastasis of Breast Cancer Cell by Disrupting Actin Dynamics. J. Nanobiotechnol. 2018, 16, 54. [Google Scholar] [CrossRef]
- Zhang, X.; Huang, Y.; Song, H.; Canup, B.S.B.; Gou, S.; She, Z.; Dai, F.; Ke, B.; Xiao, B. Inhibition of Growth and Lung Metastasis of Breast Cancer by Tumor-Homing Triple-Bioresponsive Nanotherapeutics. J. Control. Release 2020, 328, 454–469. [Google Scholar] [CrossRef]
- Zhang, T.; Liu, H.; Li, Y.; Li, C.; Wan, G.; Chen, B.; Li, C.; Wang, Y. A PH-Sensitive Nanotherapeutic System Based on a Marine Sulfated Polysaccharide for the Treatment of Metastatic Breast Cancer through Combining Chemotherapy and COX-2 Inhibition. Acta Biomater. 2019, 99, 412–425. [Google Scholar] [CrossRef] [PubMed]
- Lao, J.; Madani, J.; Puértolas, T.; Álvarez, M.; Hernández, A.; Pazo-Cid, R.; Artal, Á.; Antón Torres, A. Liposomal Doxorubicin in the Treatment of Breast Cancer Patients: A Review. J. Drug Deliv. 2013, 2013, 456409. [Google Scholar] [CrossRef]
- Perez, A.T.; Domenech, G.H.; Frankel, C.; Vogel, C.L. Pegylated Liposomal Doxorubicin (Doxil®) for Metastatic Breast Cancer: The Cancer Research Network, Inc., Experience. Cancer Investig. 2002, 20, 22–29. [Google Scholar] [CrossRef]
- Zhu, R.; Lang, T.; Yin, Q.; Li, Y. Nano Drug Delivery Systems Improve Metastatic Breast Cancer Therapy. Med. Rev. 2021, 1, 244–274. [Google Scholar] [CrossRef]
- Park, I.H.; Sohn, J.H.; Kim, S.B.; Lee, K.S.; Chung, J.S.; Lee, S.H.; Kim, T.Y.; Jung, K.H.; Cho, E.K.; Kim, Y.S.; et al. An Open-Label, Randomized, Parallel, Phase III Trial Evaluating the Efficacy and Safety of Polymeric Micelle-Formulated Paclitaxel Compared to Conventional Cremophor EL-Based Paclitaxel for Recurrent or Metastatic HER2-Negative Breast Cancer. Cancer Res. Treat. 2017, 49, 569–577. [Google Scholar] [CrossRef] [PubMed]
- Yuan, H.; Guo, H.; Luan, X.; He, M.; Li, F.; Burnett, J.; Truchan, N.; Sun, D. Albumin Nanoparticle of Paclitaxel (Abraxane) Decreases While Taxol Increases Breast Cancer Stem Cells in Treatment of Triple Negative Breast Cancer. Mol. Pharm. 2020, 17, 2275–2286. [Google Scholar] [CrossRef] [PubMed]
- De Luca, R.; Profita, G.; Cicero, G. Nab-Paclitaxel in Pretreated Metastatic Breast Cancer: Evaluation of Activity, Safety, and Quality of Life. OncoTargets Ther. 2019, 12, 1621–1627. [Google Scholar] [CrossRef] [PubMed]
- Đorđević, S.; Gonzalez, M.M.; Conejos-Sánchez, I.; Carreira, B.; Pozzi, S.; Acúrcio, R.C.; Satchi-Fainaro, R.; Florindo, H.F.; Vicent, M.J. Current Hurdles to the Translation of Nanomedicines from Bench to the Clinic. Drug Deliv. Transl. Res. 2022, 12, 500–525. [Google Scholar] [CrossRef]
- Zhang, P.; Xiao, Y.; Sun, X.; Lin, X.; Koo, S.; Yaremenko, A.V.; Qin, D.; Kong, N.; Farokhzad, O.C.; Tao, W. Cancer Nanomedicine toward Clinical Translation: Obstacles, Opportunities, and Future Prospects. Med 2023, 4, 147–167. [Google Scholar] [CrossRef] [PubMed]
- Guo, D.; Ji, X.; Luo, J. Rational Nanocarrier Design towards Clinical Translation of Cancer Nanotherapy. Biomed. Mater. 2021, 16, 032005. [Google Scholar] [CrossRef]
- Parodi, A.; Kolesova, E.P.; Voronina, M.V.; Frolova, A.S.; Kostyushev, D.; Trushina, D.B.; Akasov, R.; Pallaeva, T.; Zamyatnin, A.A. Anticancer Nanotherapeutics in Clinical Trials: The Work behind Clinical Translation of Nanomedicine. Int. J. Mol. Sci. 2022, 23, 13368. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Nanoparticle | Composition | Special Features/Advantages | Targeting Agent | Payload | Ref |
|---|---|---|---|---|---|
| Nanotherapeutics for bone metastasis | |||||
| Coordination polymer | Inner core—DSP and Zn Outer stealth—ALN PEG conjugate |
| ALN | Cisplatin prodrug (DSP) | [58] |
| Polymeric | PLGA |
| ALN and FA | Paclitaxel (PTX) | [59] |
| Nanocluster | Human serum albumin |
| ALN | Doxorubicin (DOX) | [60] |
| Micelles | Oligosaccharide hyaluronan |
| ALN | curcumin | [61] |
| Polymeric | PLGA |
| ALN | Curcumin and bortezomib | [62] |
| Micelles | PEG and polylysine (PEG-b-PLL) |
| ALN | bortezomib | [54] |
| Lipid/oil | Triptolide |
| ALN | PTX or Docetaxel (DOT) | [63] |
| Micelles | PEG, PGlu, and PPhA copolymer |
| ALN | DOT | [64] |
| Polymeric | PEG–hyaluronic acid and poly(aspartic acid) |
| ALN | DOX | [65] |
| GO nanosheet | Graphene oxide |
| ALN | DOX | [66] |
| Nanoparticle | Zinc phthalocyanine |
| ALN | Bortezomib | [67] |
| Polymeric | Amphiphilic deblock copolymers |
| ALN | GANT58 | [68] |
| Polymeric | PEGylated polybutyl cyanoacrylate |
| ZLA | DOT | [70] |
| MSN | Gold nanorod-loaded MSN |
| ZLA | - | [53] |
| Nanoparticle | Fe3O4 and ICG-entrapped PLGA |
| ZLA | - | [71] |
| Nanoparticle | Metal–organic framework |
| ZLA | Cytosine–phosphate–guanosine | [72] |
| Dendrimer | Poly(amidoamine) |
| RGD and cRGD | Bortezomib | [57] |
| Micelles | Phospholipid/polysorbate 80 |
| αvβ3-targeted quinolone nonpeptide | DOT | [73] |
| Nanotherapeutics for brain metastasis | |||||
| Liposome | Lecithin, cholesterol, DSPE–PEG3400–pVAP and platelet membrane |
| ‘Y’-shaped peptide | Cabazitaxel | [93] |
| Liposome | Cholesterol and DSPC |
| BRBP1 linear dodecapeptide | PTX and siRNA for TWF1 | [95] |
| Liposome | DSPC, cholesterol, and PEG–DSPE |
| - | Irinotecan | [96] |
| Liposome | PEG (Stealth®) |
| - | DOX (Caelyx®) | [96] |
| Liposome | PEG (Stealth®) |
| - | Temozolamide and DOX | [98] |
| Liposome | PEG, phospholipid, cholesterol |
| - | DOX | [99] |
| Liposome | DEPOSEIN® |
| - | DOX | [100] |
| Hallow nanoparticle | PEG–lauric acid conjugate copper sulfide |
| - | Stress granule inhibitor (ISRIB) | [104] |
| Polymeric | PLGA–PEG |
| Fn14-specific antibody | PTX | [105] |
| Nanoparticle | Terpolymer and polysorbate80 |
| iRGD | DOX and mitomycin | [106] |
| Polymeric | Mucic acid polymer |
| Transferrin | Camptothecin | [107] |
| Polymeric | Poly(lactic-co-glycolic acid)–poly(ε-carbobenzoxy-L-lysine) |
| Hyaluronic acid transcytosis-targeting peptide | DOX | [109] |
| Nanoparticle | Iodine |
| - | - | [113] |
| Micelles | PEG and PLA |
| Angiopep-2 | PTX and Iapatinib | [114] |
| MSN | Silica |
| Trastuzumab | PTX and siHER2 | [115] |
| Nanotherapeutics for lung metastasis | |||||
| Biomimetic intact cell | RAW264.7 cell |
| - | DOX | [128] |
| Biomimetic-Membrane | Macrophage membrane-camouflaged quercetin-loaded bismuth selenide nanoparticle |
| - | Quercetin | [129] |
| Biomimetic membrane-coated liposome | RAW264.7 macrophage membrane, DSPE–PEG, and DOPE |
| - | Emtansine | [130] |
| Biomimetic membrane-coated polymeric NP | RAW264.7 and 4T1 membrane, and PLGA |
| - | DOX | [131] |
| Biomimetic membrane-coated nanocage | 4T1 membrane and gold nanocage |
| - | DOX | [132] |
| Biomimetic membrane-coated liposome | RAW264.7 membrane and DNA tetrahedron dendrimers |
| - | DOX | [133] |
| Biomimetic membrane-coated polymeric NP | RBC membrane and PCL |
| iRGD | PTX | [134] |
| Polymeric NP | βCD–DPA and mPEG-Ad |
| - | Succinobucol | [135] |
| Polymeric NP | Triblock copolymer poloxamer |
| - | Succinobucol | [137] |
| Core–shell polymeric NP | PEI–PDHA core and PEG–PDHA shell |
| - | PTX and Twist-targeting siRNA | [138] |
| Polymeric NP | BDP |
| - | PTX and Akt-specific siRNA | [139] |
| Polymeric NP | Chondroitin sulfate |
| Quercetin, chlorin e6, and PTX | [140] | |
| Lipid-Polymeric NP | pHPMA and wheat germ agglutin-modified phosphatidylcholine |
| - | Silibinin and cryptotanshinone | [141] |
| Nanodiamond | DSPE–PEG-coated nanodiamond |
| - | DOX | [142] |
| Micelles | POEG–VBC, creatine |
| - | miRNA prodrug and DOX | [143] |
| Nanocluster | Hyaluronic acid and BSA-coated gold nanocluster |
| - | PTX | [145] |
| Nanocluster | Hyaluronic acid-coated gold nanocluster |
| PTX prodrug | [146] | |
| Nano star | Chlorin e6 and PDA-coated gold nano star |
| - | - | [147] |
| Nanotube | Iron oxide NP-incorporated single-wall carbon nanotube |
| Anti-CD105 | DOX | [148] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dissanayake, R.; Towner, R.; Ahmed, M. Metastatic Breast Cancer: Review of Emerging Nanotherapeutics. Cancers 2023, 15, 2906. https://doi.org/10.3390/cancers15112906
Dissanayake R, Towner R, Ahmed M. Metastatic Breast Cancer: Review of Emerging Nanotherapeutics. Cancers. 2023; 15(11):2906. https://doi.org/10.3390/cancers15112906
Chicago/Turabian StyleDissanayake, Ranga, Rheal Towner, and Marya Ahmed. 2023. "Metastatic Breast Cancer: Review of Emerging Nanotherapeutics" Cancers 15, no. 11: 2906. https://doi.org/10.3390/cancers15112906
APA StyleDissanayake, R., Towner, R., & Ahmed, M. (2023). Metastatic Breast Cancer: Review of Emerging Nanotherapeutics. Cancers, 15(11), 2906. https://doi.org/10.3390/cancers15112906