
Preoperative Prognostic Index for Patients with Brain Metastases—A Population-Based Multi-Centre Study

 ,
,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Statistical Analyses
3. Results
4. Discussion
4.1. Patient Characteristics
4.2. Validity of the Preoperative Prognostic Index
4.3. Clinical Importance
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nieder, C.; Spanne, O.; Mehta, M.P.; Grosu, A.L.; Geinitz, H. Presentation, patterns of care, and survival in patients with brain metastases. Cancer 2011, 117, 2505–2512. [Google Scholar] [CrossRef] [PubMed]
- Wong, J.; Hird, A.; Kirou-Mauro, A.; Napolskikh, J.; Chow, E. Quality of life in brain metastases radiation trials: A literature review. Curr. Oncol. 2008, 15, 25–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winther, R.R.; Vik-Mo, E.O.; Yri, O.E.; Aass, N.; Kaasa, S.; Skovlund, E.; Helseth, E.; Hjermstad, M.J. Surgery for brain metastases—Real-world prognostic factors’ association with survival. Acta Oncol. 2021, 60, 1161–1168. [Google Scholar] [CrossRef] [PubMed]
- Cagney, D.N.; Martin, A.M.; Catalano, P.J.; Redig, A.J.; Lin, N.U.; Lee, E.Q.; Wen, P.Y.; Dunn, I.F.; Bi, W.L.; Weiss, S.E.; et al. Incidence and prognosis of patients with brain metastases at diagnosis of systemic malignancy: A population-based study. Neuro Oncol. 2017, 19, 1511–1521. [Google Scholar] [CrossRef] [Green Version]
- Sperduto, P.W.; Mesko, S.; Li, J.; Cagney, D.; Aizer, A.; Lin, N.U.; Nesbit, E.; Kruser, T.J.; Chan, J.; Braunstein, S.; et al. Survival in Patients with Brain Metastases: Summary Report on the Updated Diagnosis-Specific Graded Prognostic Assessment and Definition of the Eligibility Quotient. J. Clin. Oncol. 2020, 38, 3773. [Google Scholar] [CrossRef] [PubMed]
- Kavouridis, V.K.; Harary, M.; Hulsbergen, A.F.C.; Lo, Y.T.; Reardon, D.A.; Aizer, A.A.; Iorgulescu, J.B.; Smith, T.R. Survival and prognostic factors in surgically treated brain metastases. J. Neurooncol. 2019, 43, 359–367. [Google Scholar] [CrossRef]
- Soffietti, R.; Abacioglu, U.; Baumert, B.; Combs, S.E.; Kinhult, S.; Kros, J.M.; Marosi, C.; Metellus, P.; Radbruch, A.; Villa Freixa, S.S.; et al. Diagnosis and treatment of brain metastases from solid tumors: Guidelines from the European Association of Neuro-Oncology (EANO). Neuro Oncol. 2017, 19, 162–174. [Google Scholar] [CrossRef] [Green Version]
- Olson, J.J.; Kalkanis, S.N.; Ryken, T.C. Congress of Neurological Surgeons Systematic Review and Evidence-Based Guidelines for the Treatment of Adults with Metastatic Brain Tumors: Executive Summary. Neurosurgery 2019, 84, 550–552. [Google Scholar] [CrossRef] [Green Version]
- Long, G.V.; Atkinson, V.; Lo, S.; Sandhu, S.; Guminski, A.D.; Brown, M.P.; Wilmott, J.S.; Edwards, J.; Gonzalez, M.; Scolyer, R.A.; et al. Combination nivolumab and ipilimumab or nivolumab alone in melanoma brain metastases: A multicentre randomised phase 2 study. Lancet Oncol. 2018, 19, 672–681. [Google Scholar] [CrossRef]
- Gaspar, L.E.; Prabhu, R.S.; Hdeib, A.; McCracken, D.J.; Lasker, G.F.; McDermott, M.W.; Kalkanis, S.N.; Olson, J.J. Congress of Neurological Surgeons Systematic Review and Evidence-Based Guidelines on the Role of Whole Brain Radiation Therapy in Adults with Newly Diagnosed Metastatic Brain Tumors. Neurosurgery 2019, 84, E159–E162. [Google Scholar] [CrossRef] [Green Version]
- Brown, P.D.; Ballman, K.V.; Cerhan, J.H.; Anderson, S.K.; Carrero, X.W.; Whitton, A.C.; Greenspoon, J.; Parney, I.F.; Laack, N.N.I.; Ashman, J.B.; et al. Postoperative stereotactic radiosurgery compared with whole brain radiotherapy for resected metastatic brain disease (NCCTG N107C/CEC.3): A multicentre, randomised, controlled, phase 3 trial. Lancet Oncol. 2017, 18, 1049–1060. [Google Scholar] [CrossRef] [PubMed]
- Ayas, A.W.; Grau, S.; Jablonska, K.; Ruess, D.; Ruge, M.; Marnitz, S.; Goldbrunner, R.; Kocher, M. Postoperative local fractionated radiotherapy for resected single brain metastases. Strahlenther. Onkol. 2018, 194, 1163–1170. [Google Scholar] [CrossRef] [PubMed]
- Schapira, E.; Hubbeling, H.; Yeap, B.Y.; Mehan, W.A., Jr.; Shaw, A.T.; Oh, K.; Gainor, J.F.; Shih, H.A. Improved Overall Survival and Locoregional Disease Control with Concurrent PD-1 Pathway Inhibitors and Stereotactic Radiosurgery for Lung Cancer Patients with Brain Metastases. Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 624–629. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, A.; Ahmed, S.; McAleer, M.F.; Weinberg, J.S.; Li, J.; Brown, P.; Settle, S.; Prabhu, S.S.; Lang, F.F.; Levine, N.; et al. Post-operative stereotactic radiosurgery versus observation for completely resected brain metastases: A single-centre, randomised, controlled, phase 3 trial. Lancet Oncol. 2017, 18, 1040–1048. [Google Scholar] [CrossRef]
- Kotecha, R.; Gondi, V.; Ahluwalia, M.S.; Brastianos, P.K.; Mehta, M.P. Recent advances in managing brain metastasis. F1000Research 2018, 7. [Google Scholar] [CrossRef] [Green Version]
- Schmieder, K.; Keilholz, U.; Combs, S. The Interdisciplinary Management of Brain Metastases. Dtsch. Arztebl. Int. 2016, 113, 415–421. [Google Scholar] [CrossRef] [Green Version]
- Patchell, R.A.; Tibbs, P.A.; Walsh, J.W.; Dempsey, R.J.; Maruyama, Y.; Kryscio, R.J.; Markesbery, W.R.; Macdonald, J.S.; Young, B. A randomized trial of surgery in the treatment of single metastases to the brain. N. Engl. J. Med. 1990, 322, 494–500. [Google Scholar] [CrossRef]
- Thon, N.; Kreth, F.W.; Tonn, J.C. The role of surgery for brain metastases from solid tumors. Handb. Clin. Neurol. 2018, 149, 113–121. [Google Scholar] [CrossRef]
- Ferguson, S.D.; Wagner, K.M.; Prabhu, S.S.; McAleer, M.F.; McCutcheon, I.E.; Sawaya, R. Neurosurgical management of brain metastases. Clin. Exp. Metastasis 2017, 34, 377–389. [Google Scholar] [CrossRef]
- D’Andrea, G.; Palombi, L.; Minniti, G.; Pesce, A.; Marchetti, P. Brain Metastases: Surgical Treatment and Overall Survival. World Neurosurg. 2017, 97, 169–177. [Google Scholar] [CrossRef]
- Le Rhun, E.; Guckenberger, M.; Smits, M.; Dummer, R.; Bachelot, T.; Sahm, F.; Galldiks, N.; de Azambuja, E.; Berghoff, A.S.; Metellus, P.; et al. EANO-ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up of patients with brain metastasis from solid tumours. Ann. Oncol. 2021, 32, 1332–1347. [Google Scholar] [CrossRef] [PubMed]
- Moss, N.S.; Beal, K.; Tabar, V. Brain Metastasis—A Distinct Oncologic Disease Best Served by an Integrated Multidisciplinary Team Approach. JAMA Oncol. 2022, 8, 1252–1254. [Google Scholar] [CrossRef]
- Loh, D.; Hogg, F.; Edwards, P.; MacColl, J.; Brogna, C.; Bhangoo, R.; Ashkan, K.; Vergani, F. Two-year experience of multi-disciplinary team (MDT) outcomes for brain metastases in a tertiary neuro-oncology centre. Br. J. Neurosurg. 2018, 32, 53–60. [Google Scholar] [CrossRef]
- Sperduto, P.W.; Berkey, B.; Gaspar, L.E.; Mehta, M.; Curran, W. A new prognostic index and comparison to three other indices for patients with brain metastases: An analysis of 1,960 patients in the RTOG database. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 510–514. [Google Scholar] [CrossRef] [PubMed]
- Gaspar, L.; Scott, C.; Rotman, M.; Asbell, S.; Phillips, T.; Wasserman, T.; McKenna, W.G.; Byhardt, R. Recursive partitioning analysis (RPA) of prognostic factors in three Radiation Therapy Oncology Group (RTOG) brain metastases trials. Int. J. Radiat. Oncol. Biol. Phys. 1997, 37, 745–751. [Google Scholar] [CrossRef] [PubMed]
- Picarelli, H.; Oliveira, M.L.; Marta, G.N.; Solla, D.J.F.; Teixeira, M.J.; Figueiredo, E.G. Mortality, Morbidity, and Prognostic Factors in the Surgical Resection of Brain Metastases: A Contemporary Cohort Study. J. Neurol. Surg. Part A Cent. Eur. Neurosurg. 2020, 81, 279–289. [Google Scholar] [CrossRef]
- Pojskic, M.; Bopp, M.H.A.; Schymalla, M.; Nimsky, C.; Carl, B. Retrospective study of 229 surgically treated patients with brain metastases: Prognostic factors, outcome and comparison of recursive partitioning analysis and diagnosis-specific graded prognostic assessment. Surg. Neurol. Int. 2017, 8, 259. [Google Scholar] [CrossRef]
- Liu, Z.; Lei, B.; Zheng, M.; Li, Z.; Huang, S.; Deng, Y. Prognostic factors in patients treated with surgery for brain metastases: A single-center retrospective analysis of 125 patients. Int. J. Surg. 2017, 44, 204–209. [Google Scholar] [CrossRef]
- Bergqvist, S. Gamma Knife at Karolinska. Available online: https://www.karolinska.se/en/karolinska-university-hospital/medical-areas/gamma-knife-surgery/ (accessed on 9 August 2022).
- Leksell, L. Stereotaxis and Radiosurgery. An Operative System; Charles C Thomas: Springfield, IL, USA, 1971; p. 70. [Google Scholar]
- Lindquist, C.; Kihlström, L. Department of Neurosurgery, Karolinska Institute: 60 years. Neurosurgery 1996, 39, 1016–1021. [Google Scholar] [CrossRef]
- Editorial Group for NOMESCO Health Statistics. Cancer. Available online: https://nhwstat.org/health/cancer (accessed on 12 September 2022).
- Kim, Y.J.; Hui, D.; Zhang, Y.; Park, J.C.; Chisholm, G.; Williams, J.; Bruera, E. Differences in Performance Status Assessment among Palliative Care Specialists, Nurses, and Medical Oncologists. J. Pain Symptom Manag. 2015, 49, 1050–1058.e1052. [Google Scholar] [CrossRef] [Green Version]
- Mulvenna, P.; Nankivell, M.; Barton, R.; Faivre-Finn, C.; Wilson, P.; McColl, E.; Moore, B.; Brisbane, I.; Ardron, D.; Holt, T.; et al. Dexamethasone and supportive care with or without whole brain radiotherapy in treating patients with non-small cell lung cancer with brain metastases unsuitable for resection or stereotactic radiotherapy (QUARTZ): Results from a phase 3, non-inferiority, randomised trial. Lancet 2016, 388, 2004–2014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, P.D.; Jaeckle, K.; Ballman, K.V.; Farace, E.; Cerhan, J.H.; Anderson, S.K.; Carrero, X.W.; Barker, F.G.; Deming, R.; Burri, S.H.; et al. Effect of radiosurgery alone vs. radiosurgery with whole brain radiation therapy on cognitive function in patients with 1 to 3 brain metastases: A randomized clinical trial. JAMA 2016, 316, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.L.; Wefel, J.S.; Hess, K.R.; Allen, P.K.; Lang, F.F.; Kornguth, D.G.; Arbuckle, R.B.; Swint, J.M.; Shiu, A.S.; Maor, M.H.; et al. Neurocognition in patients with brain metastases treated with radiosurgery or radiosurgery plus whole-brain irradiation: A randomised controlled trial. Lancet Oncol. 2009, 10, 1037–1044. [Google Scholar] [CrossRef]
- Lee, C.H.; Kim, D.G.; Kim, J.W.; Han, J.H.; Kim, Y.H.; Park, C.K.; Kim, C.Y.; Paek, S.H.; Jung, H.W. The role of surgical resection in the management of brain metastasis: A 17-year longitudinal study. Acta Neurochir. 2013, 155, 389–397. [Google Scholar] [CrossRef] [PubMed]
- Armocida, D.; Pesce, A.; Palmieri, M.; Cofano, F.; Palmieri, G.; Cassoni, P.; Busceti, C.L.; Biagioni, F.; Garbossa, D.; Fornai, F.; et al. EGFR-Driven Mutation in Non-Small-Cell Lung Cancer (NSCLC) Influences the Features and Outcome of Brain Metastases. J. Clin. Med. 2023, 12, 3372. [Google Scholar] [CrossRef]
- Preusser, M.; Berghoff, A.S.; Ilhan-Mutlu, A.; Magerle, M.; Dinhof, C.; Widhalm, G.; Dieckmann, K.; Marosi, C.; Wöhrer, A.; Hackl, M.; et al. ALK gene translocations and amplifications in brain metastases of non-small cell lung cancer. Lung Cancer 2013, 80, 278–283. [Google Scholar] [CrossRef]
- Italiano, A.; Vandenbos, F.B.; Otto, J.; Mouroux, J.; Fontaine, D.; Marcy, P.Y.; Cardot, N.; Thyss, A.; Pedeutour, F. Comparison of the epidermal growth factor receptor gene and protein in primary non-small-cell-lung cancer and metastatic sites: Implications for treatment with EGFR-inhibitors. Ann. Oncol. 2006, 17, 981–985. [Google Scholar] [CrossRef]
- Rau, K.-M.; Chen, H.-K.; Shiu, L.-Y.; Chao, T.-L.; Lo, Y.-P.; Wang, C.-C.; Lin, M.-C.; Huang, C.-C. Discordance of Mutation Statuses of Epidermal Growth Factor Receptor and K-ras between Primary Adenocarcinoma of Lung and Brain Metastasis. Int. J. Mol. Sci. 2016, 17, 524. [Google Scholar] [CrossRef] [Green Version]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): The TRIPOD Statement. BMC Med. 2015, 13, 1. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Prognostic Variables 1 | B | p-Value | HR (95% CI) |
|---|---|---|---|
| Age ≥ 70? | 0.514 | <0.001 | 1.67 (1.36–2.05) |
| ECOG > 2? | 0.489 | <0.001 | 1.63 (1.31–2.04) |
| Breast cancer? | −0.710 | <0.001 | 0.49 (0.33–0.73) |
| Colorectal cancer? | 0.350 | 0.036 | 1.42 (1.02–197) |
| Progressive extracranial disease 2 or synchronous brain metastases 3 | 0.345 | <0.001 | 1.41 (1.17–1.71) |
| Extracranial metastases present? 4 | 0.394 | <0.001 | 1.48 (1.23–1.79) |
| Previous chemotherapy? | 0.295 | 0.009 | 1.34 (1.08–1.68) |
| Number of BM > 4? | 0.439 | 0.010 | 1.55 (1.11–2.17) |
| Prognostic Index Score | Group | ||
| −1.0–0.0 | 0 | ||
| >0.0–1.0 | 1 | ||
| >1.0–1.4 | 2 | ||
| 1.4–2.9 | 3 | ||
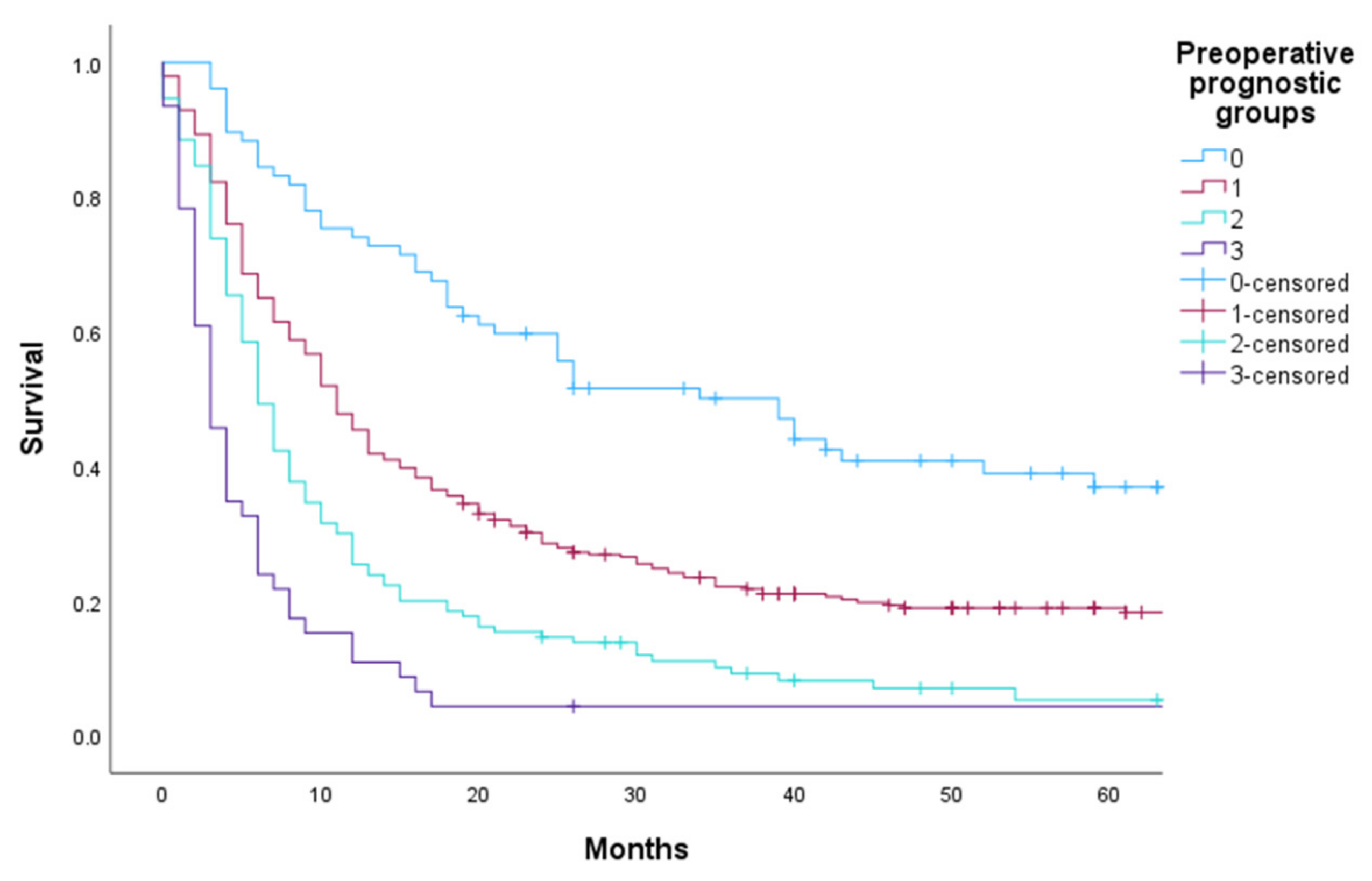
| Prognostic Group | Prognostic Index Score | Total N (%) | Median OS in Months (95% CI) | HR (95% CI) |
|---|---|---|---|---|
| 0 | −1.0–0.0 | 77 (13) | 39 (24–54) | 1 |
| 1 | >0.0–1.0 | 337 (57) | 11 (10–12) | 1.93 (1.42–2.62) |
| 2 | >1.0–1.4 | 130 (22) | 6 (5–7) | 3.1 (2.19–4.32) |
| 3 | >1.4–2.9 | 46 (8) | 3 (2–4) | 5.4 (3.56–8.19) |
| Overall | 590 (100) | 10 (9–11) |
| Oslo University Hospital (590) | Karolinska University Hospital (261) | St.Olavs University Hospital (177) | |
|---|---|---|---|
| Age ≥ 70 | 148 (25%) | 39 (15%) * | 63 (36%) |
| ECOG > 2 | 111 (19%) | 73 (28%) * | 7 (4%) * |
| Breast cancer | 53 (9%) | 54 (21%) * | 25 (14%) * |
| Colorectal cancer | 50 (9%) | 19 (7%) | 23 (13%) |
| Progressive extracranial disease/synchronous BM | 322 (55%) | 112 (43%) * | 98 (55%) |
| Extracranial metastases | 312 (53%) | 133 (51%) | 80 (45%) |
| Previous chemotherapy | 203 (34%) | 155 (59%) * | 98 (55%) * |
| Number of BM > 4 | 43 (7%) | 13 (5%) | 8 (5%) |
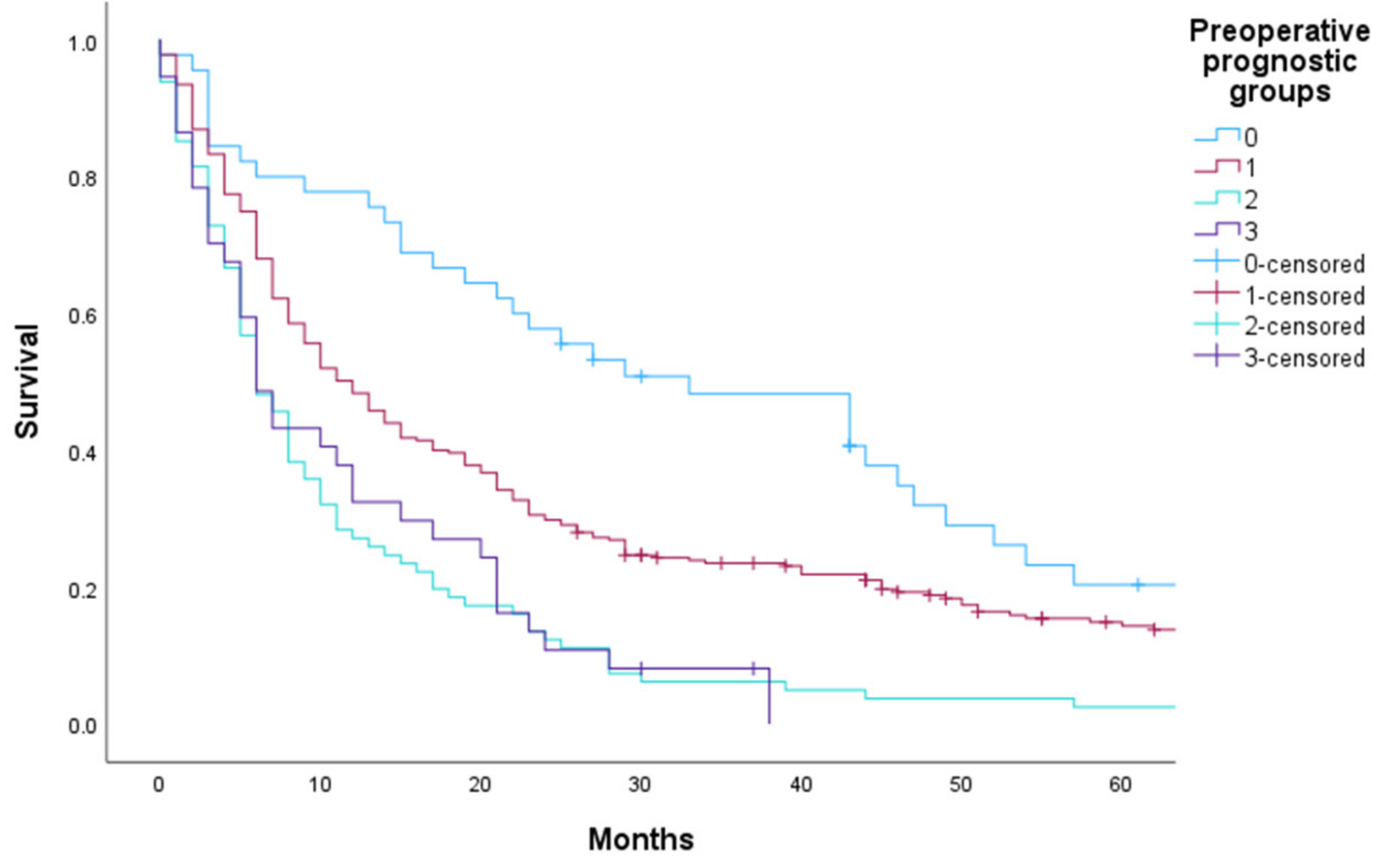
| Prognostic Group | Total N (%) | Median OS in Months (95% CI) | HR (95% CI) |
|---|---|---|---|
| 0 | 45 (10) | 33 (19–47) | |
| 1 | 275 (63) | 12 (9–15) | 1.60 (1.12–2.29) |
| 2 | 81 (18) | 6 (4–8) | 2.85 (1.90–4.28) |
| 3 | 37 (8) | 6 (4–8) | 2.73 (1.70–4.40) |
| Overall | 438 (100) | 10 (8–12) |
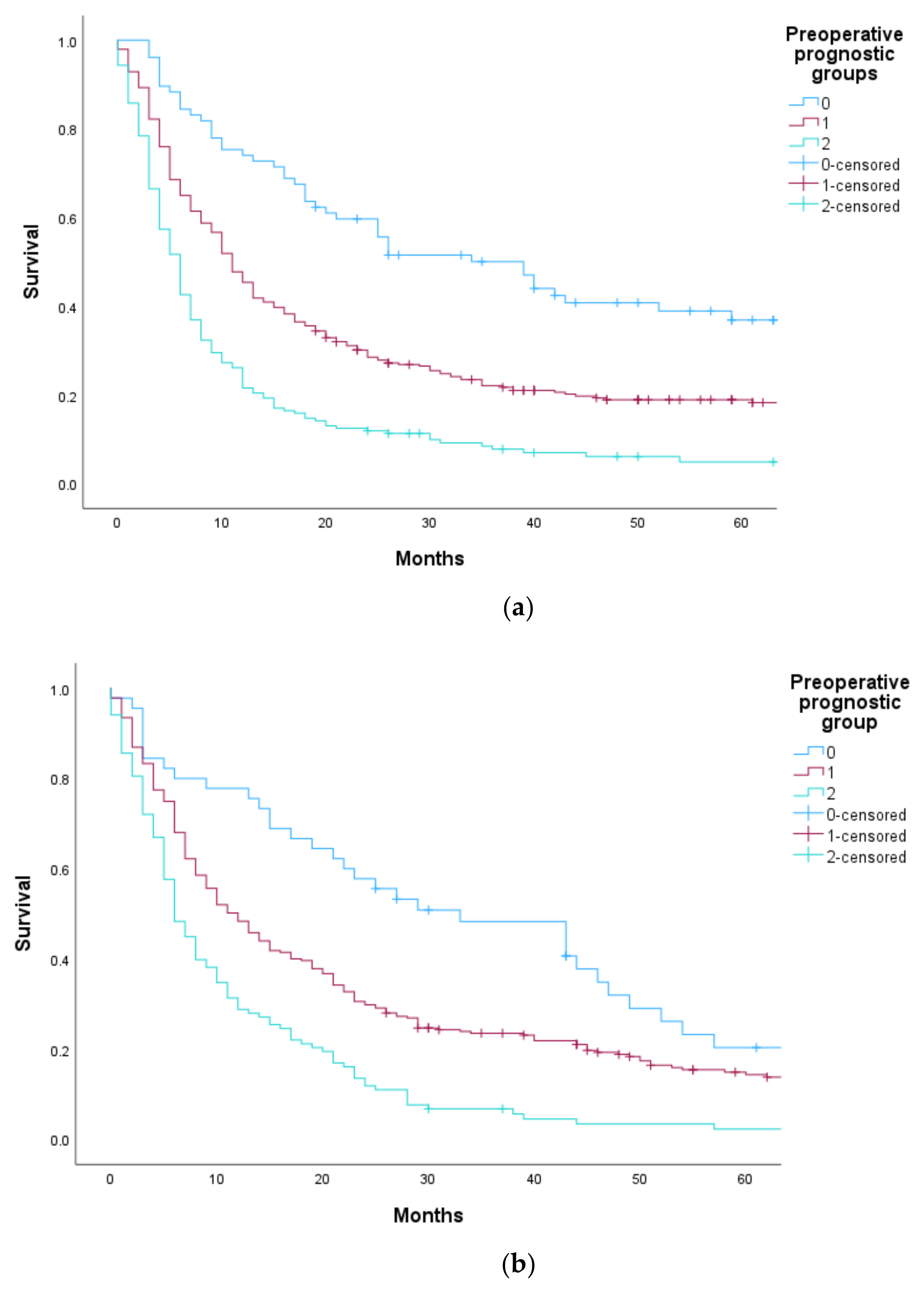
| Prognostic Group | Prognostic Index Score | Oslo University Hospital * | Karolinska/St.Olavs ** | ||||
|---|---|---|---|---|---|---|---|
| Total N (%) | Median OS in Months (95% CI) | HR (95% CI) | Total N (%) | Median OS in Months (95% CI) | HR (95% CI) | ||
| 0 | −1.0–0.0 | 77 (13) | 39 (24–54) | 1 | 45 (10) | 33 (19–47) | 1 |
| 1 | >0.0–1.0 | 337 (57) | 11 (10–12) | 1.92 (1.41–2.62) | 275 (63) | 12 (9–14) | 1.60 (1.12–2.29) |
| 2 | >1.0–2.9 | 176 (30) | 6 (5–7) | 3.46 (2.50–4.80) | 118 (27) | 6 (5–7) | 2.81 (1.91–4.14) |
| Overall | 590 (100) | 10 (9–11) | 438 (100) | 10 (8–12) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Winther, R.R.; Skovlund, E.; Andreassen, J.S.; Arvidsson, L.; Halvardson, J.; Solheim, O.; Bartek, J.; Kaasa, S.; Hjermstad, M.J.; Vik-Mo, E.O. Preoperative Prognostic Index for Patients with Brain Metastases—A Population-Based Multi-Centre Study. Cancers 2023, 15, 3174. https://doi.org/10.3390/cancers15123174
Winther RR, Skovlund E, Andreassen JS, Arvidsson L, Halvardson J, Solheim O, Bartek J, Kaasa S, Hjermstad MJ, Vik-Mo EO. Preoperative Prognostic Index for Patients with Brain Metastases—A Population-Based Multi-Centre Study. Cancers. 2023; 15(12):3174. https://doi.org/10.3390/cancers15123174
Chicago/Turabian StyleWinther, Rebecca Rootwelt, Eva Skovlund, Joakim Stray Andreassen, Lisa Arvidsson, Jonathan Halvardson, Ole Solheim, Jiri Bartek, Stein Kaasa, Marianne Jensen Hjermstad, and Einar Osland Vik-Mo. 2023. "Preoperative Prognostic Index for Patients with Brain Metastases—A Population-Based Multi-Centre Study" Cancers 15, no. 12: 3174. https://doi.org/10.3390/cancers15123174
APA StyleWinther, R. R., Skovlund, E., Andreassen, J. S., Arvidsson, L., Halvardson, J., Solheim, O., Bartek, J., Kaasa, S., Hjermstad, M. J., & Vik-Mo, E. O. (2023). Preoperative Prognostic Index for Patients with Brain Metastases—A Population-Based Multi-Centre Study. Cancers, 15(12), 3174. https://doi.org/10.3390/cancers15123174