
Survival Trends in Patients with Small Intestinal Neuroendocrine Tumours—A Cohort Study in Central Norway


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Radiological Imaging
2.3. Surgical and Non-Surgical Treatment
2.4. Disease Stage and Severity
2.5. Survival and Disease Recurrence
2.6. Statistical Analyses
3. Results
3.1. Patient Demographics
3.2. Surgical Procedures
3.3. Disease Stage and Severity at Time of Diagnosis
3.4. Surgery with Curative Intention and Disease Recurrence
3.5. Non-Surgical Treatment during Follow-Up
3.6. Patients Not Resected for SI-NETs
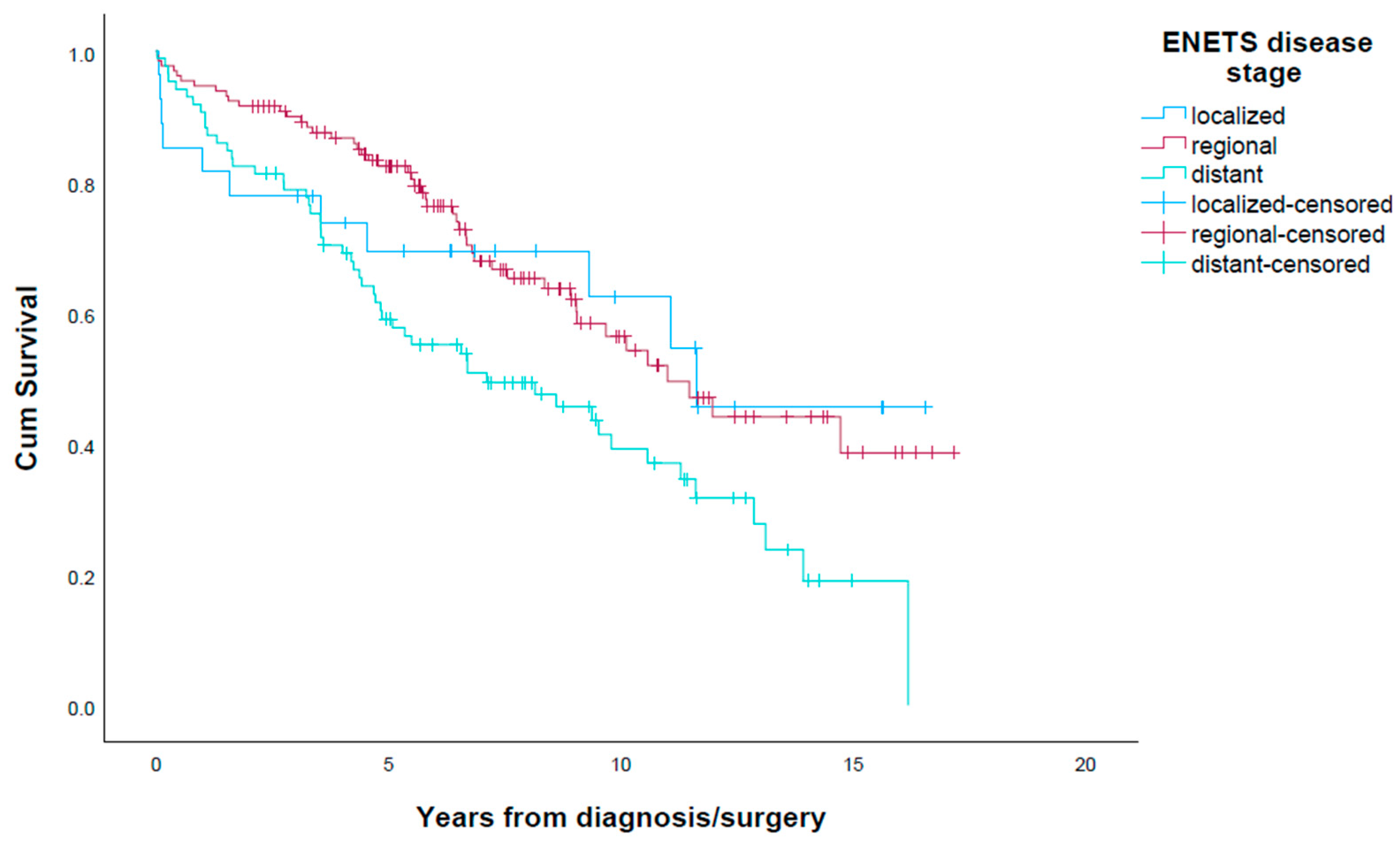
3.7. Overall Survival and Cause of Death
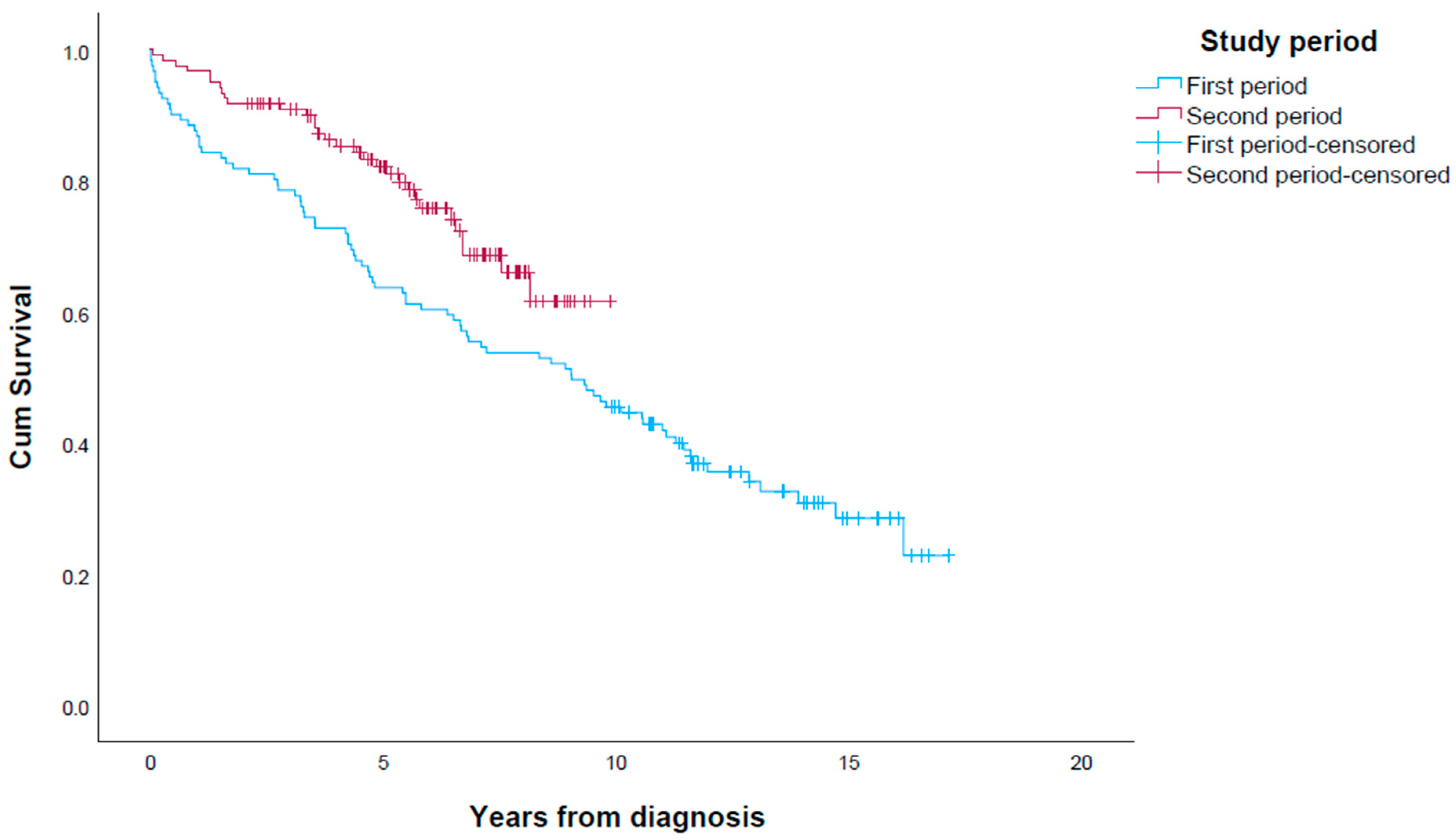
3.8. Survival in First Period vs. Second Period
4. Discussion
4.1. Identifying SI-NET Patients
4.2. Survival
4.3. Survival Trend
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients With Neuroendocrine Tumors in the United States. JAMA Oncol. 2017, 3, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Landerholm, K. Time trends in incidence and survival of small intestinal cancer in Sweden. BJS Open 2021, 5, zraa044. [Google Scholar] [CrossRef] [PubMed]
- Landerholm, K.; Falkmer, S.; Jarhult, J. Epidemiology of small bowel carcinoids in a defined population. World J. Surg. 2010, 34, 1500–1505. [Google Scholar] [CrossRef]
- Hauso, O.; Gustafsson, B.I.; Kidd, M.; Waldum, H.L.; Drozdov, I.; Chan, A.K.; Modlin, I.M. Neuroendocrine tumor epidemiology: Contrasting Norway and North America. Cancer 2008, 113, 2655–2664. [Google Scholar] [CrossRef] [PubMed]
- Stensbøl, A.B.; Krogh, J.; Holmager, P.; Klose, M.; Oturai, P.; Kjaer, A.; Hansen, C.P.; Federspiel, B.; Langer, S.W.; Knigge, U.; et al. Incidence, Clinical Presentation and Trends in Indication for Diagnostic Work-Up of Small Intestinal and Pancreatic Neuroendocrine Tumors. Diagnostics 2021, 11, 2030. [Google Scholar] [CrossRef] [PubMed]
- Thiis-Evensen, E.; Boyar Cetinkaya, R. Incidence and prevalence of neuroendocrine neoplasms in Norway 1993–2021. J. Neuroendocrinol. 2023, 35, e13264. [Google Scholar] [CrossRef]
- Eriksson, J.; Norlen, O.; Ogren, M.; Garmo, H.; Ihre-Lundgren, C.; Hellman, P. Primary small intestinal neuroendocrine tumors are highly prevalent and often multiple before metastatic disease develops. Scand. J. Surg. 2021, 110, 44–50. [Google Scholar] [CrossRef] [Green Version]
- Berge, T.; Linell, F. Carcinoid tumours. Frequency in a defined population during a 12-year period. Acta Pathol. Microbiol. Scand. A 1976, 84, 322–330. [Google Scholar]
- Snorradottir, S.; Asgeirsdottir, A.; Rögnvaldsson, S.; Jonasson, J.G.; Björnsson, E.S. Incidence and prognosis of patients with small intestinal neuroendocrine tumors in a population based nationwide study. Cancer Epidemiol. 2022, 79, 102197. [Google Scholar] [CrossRef]
- Modlin, I.M.; Lye, K.D.; Kidd, M. A 5-decade analysis of 13,715 carcinoid tumors. Cancer 2003, 97, 934–959. [Google Scholar] [CrossRef]
- Jann, H.; Roll, S.; Couvelard, A.; Hentic, O.; Pavel, M.; Muller-Nordhorn, J.; Koch, M.; Rocken, C.; Rindi, G.; Ruszniewski, P.; et al. Neuroendocrine tumors of midgut and hindgut origin: Tumor-node-metastasis classification determines clinical outcome. Cancer 2011, 117, 3332–3341. [Google Scholar] [CrossRef]
- Norlen, O.; Stalberg, P.; Oberg, K.; Eriksson, J.; Hedberg, J.; Hessman, O.; Janson, E.T.; Hellman, P.; Akerstrom, G. Long-term results of surgery for small intestinal neuroendocrine tumors at a tertiary referral center. World J. Surg. 2012, 36, 1419–1431. [Google Scholar] [CrossRef]
- Garcia-Carbonero, R.; Capdevila, J.; Crespo-Herrero, G.; Diaz-Perez, J.A.; Martinez Del Prado, M.P.; Alonso Orduna, V.; Sevilla-Garcia, I.; Villabona-Artero, C.; Beguiristain-Gomez, A.; Llanos-Munoz, M.; et al. Incidence, patterns of care and prognostic factors for outcome of gastroenteropancreatic neuroendocrine tumors (GEP-NETs): Results from the National Cancer Registry of Spain (RGETNE). Ann. Oncol. 2010, 21, 1794–1803. [Google Scholar] [CrossRef]
- Quaedvlieg, P.F.; Visser, O.; Lamers, C.B.; Janssen-Heijen, M.L.; Taal, B.G. Epidemiology and survival in patients with carcinoid disease in The Netherlands. An epidemiological study with 2391 patients. Ann. Oncol. 2001, 12, 1295–1300. [Google Scholar] [CrossRef]
- Keller, H.R.; Senapathi, S.H.; Morada, A.; Bertsch, D.; Cagir, B. Survival in patients with neuroendocrine tumors of the colon, rectum and small intestine. Am. J. Surg. 2023, 225, 58–65. [Google Scholar] [CrossRef]
- Bergestuen, D.S.; Aabakken, L.; Holm, K.; Vatn, M.; Thiis-Evensen, E. Small intestinal neuroendocrine tumors: Prognostic factors and survival. Scand. J. Gastroenterol. 2009, 44, 1084–1091. [Google Scholar] [CrossRef] [PubMed]
- Boyar Cetinkaya, R.; Aagnes, B.; Myklebust, T.; Thiis-Evensen, E. Survival in neuroendocrine neoplasms; A report from a large Norwegian population-based study. Int. J. Cancer 2018, 142, 1139–1147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niederle, B.; Pape, U.F.; Costa, F.; Gross, D.; Kelestimur, F.; Knigge, U.; Oberg, K.; Pavel, M.; Perren, A.; Toumpanakis, C.; et al. ENETS Consensus Guidelines Update for Neuroendocrine Neoplasms of the Jejunum and Ileum. Neuroendocrinology 2016, 103, 125–138. [Google Scholar] [CrossRef] [Green Version]
- Rinke, A.; Muller, H.H.; Schade-Brittinger, C.; Klose, K.J.; Barth, P.; Wied, M.; Mayer, C.; Aminossadati, B.; Pape, U.F.; Blaker, M.; et al. Placebo-controlled, double-blind, prospective, randomized study on the effect of octreotide LAR in the control of tumor growth in patients with metastatic neuroendocrine midgut tumors: A report from the PROMID Study Group. J. Clin. Oncol. 2009, 27, 4656–4663. [Google Scholar] [CrossRef] [PubMed]
- Caplin, M.E.; Pavel, M.; Cwikla, J.B.; Phan, A.T.; Raderer, M.; Sedlackova, E.; Cadiot, G.; Wolin, E.M.; Capdevila, J.; Wall, L.; et al. Lanreotide in metastatic enteropancreatic neuroendocrine tumors. N. Engl. J. Med. 2014, 371, 224–233. [Google Scholar] [CrossRef] [PubMed]
- Strosberg, J.; El-Haddad, G.; Wolin, E.; Hendifar, A.; Yao, J.; Chasen, B.; Mittra, E.; Kunz, P.L.; Kulke, M.H.; Jacene, H.; et al. Phase 3 Trial of (177)Lu-Dotatate for Midgut Neuroendocrine Tumors. N. Engl. J. Med. 2017, 376, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Pape, U.F.; Perren, A.; Niederle, B.; Gross, D.; Gress, T.; Costa, F.; Arnold, R.; Denecke, T.; Plockinger, U.; Salazar, R.; et al. ENETS Consensus Guidelines for the management of patients with neuroendocrine neoplasms from the jejuno-ileum and the appendix including goblet cell carcinomas. Neuroendocrinology 2012, 95, 135–156. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.C.; Hassan, M.; Phan, A.; Dagohoy, C.; Leary, C.; Mares, J.E.; Abdalla, E.K.; Fleming, J.B.; Vauthey, J.N.; Rashid, A.; et al. One hundred years after “carcinoid”: Epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J. Clin. Oncol. 2008, 26, 3063–3072. [Google Scholar] [CrossRef] [Green Version]
- Daskalakis, K.; Karakatsanis, A.; Hessman, O.; Stuart, H.C.; Welin, S.; Tiensuu Janson, E.; Oberg, K.; Hellman, P.; Norlen, O.; Stalberg, P. Association of a Prophylactic Surgical Approach to Stage IV Small Intestinal Neuroendocrine Tumors with Survival. JAMA Oncol. 2018, 4, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Levy, S.; Arthur, J.D.; Banks, M.; Kok, N.F.M.; Fenwick, S.W.; Diaz-Nieto, R.; van Leerdam, M.E.; Cuthbertson, D.J.; Valk, G.D.; Kuhlmann, K.F.D.; et al. Primary Tumor Resection is Associated with Improved Disease-Specific Mortality in Patients with Stage IV Small Intestinal Neuroendocrine Tumors (NETs): A Comparison of Upfront Surgical Resection Versus a Watch and Wait Strategy in Two Specialist NET Centers. Ann. Surg. Oncol. 2022, 29, 7822–7832. [Google Scholar] [CrossRef]
- Fossmark, R.; Balto, T.M.; Martinsen, T.C.; Gronbech, J.E.; Munkvold, B.; Mjones, P.G.; Waldum, H.L. Hepatic micrometastases outside macrometastases are present in all patients with ileal neuroendocrine primary tumour at the time of liver resection. Scand. J. Gastroenterol. 2019, 54, 1003–1007. [Google Scholar] [CrossRef] [PubMed]
- Selberherr, A.; Freermann, S.; Koperek, O.; Niederle, M.B.; Riss, P.; Scheuba, C.; Niederle, B. Neuroendocrine liver metastasis from the small intestine: Is surgery beneficial for survival? Orphanet J. Rare Dis. 2021, 16, 30. [Google Scholar] [CrossRef]
- Folkestad, O.; Wasmuth, H.H.; Mjønes, P.; Fougner, R.; Hauso, Ø.; Fossmark, R. Survival and disease recurrence in patients operated for small intestinal neuroendocrine tumors at a referral hospital. Surg. Oncol. 2020, 35, 336–343. [Google Scholar] [CrossRef]
- Daskalakis, K.; Wedin, M.; Tsoli, M.; Kogut, A.; Srirajaskanthan, R.; Sarras, K.; Kattiparambil, S.; Giovos, G.; Weickert, M.O.; Kos-Kudla, B.; et al. Association of lymph node metastases, grade and extent of mesenteric lymph node dissection in locoregional small intestinal neuroendocrine tumors with recurrence-free survival. J. Neuroendocrinol. 2022, 34, e13205. [Google Scholar] [CrossRef]
- Evers, M.; Rinke, A.; Rütz, J.; Ramaswamy, A.; Maurer, E.; Bartsch, D.K. Prognostic Factors in Curative Resected Locoregional Small Intestine Neuroendocrine Neoplasms. World J. Surg. 2021, 45, 1109–1117. [Google Scholar] [CrossRef]
- Zaidi, M.Y.; Lopez-Aguiar, A.G.; Dillhoff, M.; Beal, E.; Poultsides, G.; Makris, E.; Rocha, F.; Crown, A.; Idrees, K.; Marincola Smith, P.; et al. Prognostic Role of Lymph Node Positivity and Number of Lymph Nodes Needed for Accurately Staging Small-Bowel Neuroendocrine Tumors. JAMA Surg. 2019, 154, 134–140. [Google Scholar] [CrossRef]
- Li, M.X.; Lopez-Aguiar, A.G.; Poultsides, G.; Rocha, F.; Weber, S.; Fields, R.; Idrees, K.; Cho, C.; Maithel, S.K.; Zhang, X.F.; et al. Surgical Treatment of Neuroendocrine Tumors of the Terminal Ileum or Cecum: Ileocecectomy Versus Right Hemicolectomy. J. Gastrointest. Surg. 2022, 26, 1266–1274. [Google Scholar] [CrossRef]
- Zhou, Z.; Ge, H.; Li, Y.; Wang, D.; Güngör, C. Survival effects of primary and metastatic surgical treatment in metastatic small intestinal tumors: A propensity score-matching study. PLoS ONE 2022, 17, e0270608. [Google Scholar] [CrossRef] [PubMed]
- Landry, C.S.; Lin, H.Y.; Phan, A.; Charnsangavej, C.; Abdalla, E.K.; Aloia, T.; Nicolas Vauthey, J.; Katz, M.H.; Yao, J.C.; Fleming, J.B. Resection of at-risk mesenteric lymph nodes is associated with improved survival in patients with small bowel neuroendocrine tumors. World J. Surg. 2013, 37, 1695–1700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Motz, B.M.; Lorimer, P.D.; Boselli, D.; Hill, J.S.; Salo, J.C. Optimal Lymphadenectomy in Small Bowel Neuroendocrine Tumors: Analysis of the NCDB. J. Gastrointest. Surg. 2018, 22, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Almond, L.M.; Hodson, J.; Ford, S.J.; Gourevitch, D.; Roberts, K.J.; Shah, T.; Isaac, J.; Desai, A. Role of palliative resection of the primary tumour in advanced pancreatic and small intestinal neuroendocrine tumours: A systematic review and meta-analysis. Eur. J. Surg. Oncol. 2017, 43, 1808–1815. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Surgical Resection of Primary SI-NET (n = 205) | Patients with SI-NETs Not Resected (n = 37) | p-Value | |
|---|---|---|---|
| Age, median (range) | 68.0 (17–91) | 76.0 (52–87) | 0.01 |
| Male, n (%) | 117 (57.1%) | 18 (48.6%) | 0.25 |
| Preoperative SI-NET diagnoses, n (%) | |||
| Known | 154 (75.1%) | ||
| Unknown, n (%) | 51 (24.9%) | ||
| Reason for no resection, n (%) | |||
| Age/comorbidity | 7 (18.9%) | ||
| Patient declined surgery | 4 (10.8%) | ||
| Tumour assessed inoperable | 21 (56.8%) | ||
| Surgery not considered | 3 (8.1%) | ||
| Other cause | 1 (2.7%) | ||
| ENETS stage, n (%) | 0.003 | ||
| Localized | 24 (11.7%) | 3 (8.1%) | |
| Regional | 118 (57.6%) | 12 (32.4%) | |
| Distant | 63 (30.7%) | 22 (59.5%) | |
| Multifocal primary tumours, n (%) | 63 (30.7%) | ||
| WHO grade *, n (%) | 0.168 0.20 | ||
| G1 | 116 (56.6%) | 15 (40.5%) | |
| G2 | 79 (38.5%) | 10 (27%) | |
| Unknown | 10 (4.9%) | 12 (32.4%) | |
| Carcinoid heart disease, n (%) | 8 (3.9%) | 3 (8.1%) | |
| Synchronous cancer, n (%) | 23 (11.2%) | 3 (8.1%) | |
| Curative surgery, n (%) | 137 (66.8%) | - | |
| Recurrence, n (%) | 42 (20.5%) | - | |
| Deaths, n (%) | 87 (42.4%) | 25 (67.6%) | |
| Due to surg. complication | 5 (2.4%) | - | |
| 30-day mortality postop. | 5 (2.4%) | - | |
| 90-day mortality postop. | 9 (4.3%) | - | |
| Due to SI-NET disease | 36 (17.6%) | 14 (37.8%) | |
| Other cancer | 17 (8.3%) | 3 (8.1%) | |
| Other disease | 10 (4.9%) | 3 (8.1%) | |
| Unknown | 19 (9.3%) | 5 (13.5%) | |
| Non-surgical treatment, n (%) | |||
| SSA | 96 (46.8%) | 30 (81.1%) | |
| Interferon | 13 (6.3%) | 1 (2.7%) | |
| mTOR inhibitor | 8 (3.9%) | 4 (10.8%) | |
| TAE | 10 (4.9%) | 0 | |
| Cytostatic treatment | 7 (3.4%) | 2 (5.4%) | |
| PRRT | 22 (10.7%) | 5 (13.5%) | |
| Liver surgery | 12 (5.9%) | 0 |
| Total (n = 242) | First Period (n = 121) | Second Period (n = 121) | p-Value | |
|---|---|---|---|---|
| Age (median, range) | 69.0 | 71.0 | 0.506 | |
| Sex (male) | 70 (57.9%) | 65 (53.7%) | 0.605 | |
| WHO grade *, n (%) | 0.039 | |||
| G1 | 131 (54.1) | 69 (57.0) | 62 (51.2) | |
| G2 | 89 (36.8) | 34 (28.1) | 55 (45.5) | |
| Unknown | 22 (9.1) | 18 (14.9) | 4 (3.3) | |
| ENETS stage, n (%) | 0.171 | |||
| Localized | 27 (11.2) | 14 (11.6) | 13 (10.7) | |
| Regional | 130 (53.7) | 58 (47.9) | 72 (59.5) | |
| Distant | 85 (35.1) | 49 (40.5) | 36 (29.8) | |
| Carcinoid heart disease, n (%) | 11 (4.5) | 9 (7.4) | 2 (1.7) | 0.031 |
| Any surgery, n (%) | 211 (87.2) | 110 (90.0) | 101 (83.5) | 0.123 |
| Primary tumour resected **, n (%) | 205 (84.7) | 104 (86.0) | 101 (83.5) | 0.721 |
| Preop. known SI-NET, n (%) | 154 (75.1) | 73 (70.2) | 81 (80.2) | 0.108 |
| Curative surgery, n (%) | 137 (66.8) | 62 (59.6) | 75 (74.3) | 0.027 |
| Lymph nodes in specimen, median (range) | 8 (0–62) | 5 (0–30) | 10 (0–62) | 0.037 |
| Synchronous cancer in specimen | 23 (11.2) | 12 (11.5) | 11 (10.9) | 1.0 |
| Relapse/death in radically resected patient | 72 (52.6%) | 42 (40.4%) | 30 (29.7%) | 0.09 |
| Liver surgery, n (%) | 12 (5.0) | 4 (3.3%) | 8 (6.6%) | 0.247 |
| Non-surgical treatment | ||||
| SSA | 64 (52.9) | 62 (51.2) | 0.898 | |
| Everolimus | 4 (3.3) | 8 (6.6) | 0.375 | |
| PRRT | 14 (11.6) | 13 (10.7) | 1.0 | |
| Interferon | 11 (9.1) | 3 (2.5) | 0.050 | |
| Chemotherapy | 5 (4.1) | 4 (3.3) | 1.0 | |
| TAE | 7 (5.8) | 3 (2.5) | 0.33 | |
| One-year mortality, n (%) | 21 (8.7) | 17 (14) | 4 (3.3) | 0.005 |
| Surg. complication | 5 (2.1) | 4 (3.3) | 1 (0.8) | 0.37 |
| SI-NET | 5 (2.1) | 4 (3.3) | 1 (0.8) | 0.37 |
| Other cancer | 4 (1.7) | 3 (2.5) | 1 (0.8) | 0.62 |
| Other disease | 3 (1.2) | 2 (1.7) | 1 (0.8) | 1.0 |
| Unknown cause | 4 (1.7) | 4 (3.3) | 0 | 0.12 |
| Total (n = 205) | First Period (n = 104) | Second Period (n = 101) | p-Value * | |||
|---|---|---|---|---|---|---|
| Elective (n = 76) | Emergency (n = 28) | Elective (n = 77) | Emergency (n = 24) | |||
| T stage, n (%) | 0.277 | |||||
| 0 | 2 (1.0) | 1 (1.3) | 0 | 1 (1.3) | 0 | |
| 1 | 12 (5.9) | 5 (6.6) | 3 (10.7) | 2 (2.6) | 2 (8.3) | |
| 2 | 38 (18.5) | 14 (18.4) | 4 (14.3) | 16 (20.8) | 4 (16.7) | |
| 3 | 94 (45.9) | 31 (40.8) | 12 (42.9) | 43 (55.8%) | 8 (33.3) | |
| 4 | 53 (25.9) | 21 (27.6) | 7 (25) | 15 (19.5) | 10 (41.7) | |
| Unknown | 6 (2.9) | 4 (5.3) | 2 (7.1) | 0 | 0 | |
| N stage, n (%) | 0.218 | |||||
| 0 | 16 (7.8) | 9 (11.8) | 0 | 5 (6.5) | 2 (8.3) | |
| 1 | 91 (44.4) | 27 (35.5) | 13 (46.4) | 41 (53.2) | 10 (41.7) | |
| 2 | 79 (38.5) | 32 (42.1) | 10 (35.7) | 30 (39.0) | 7 (29.2) | |
| Nx | 19 (9.3) | 8 (10.5) | 5 (17.9) | 1 (1.3) | 5 (20.8) | |
| Unknown | ||||||
| M stage, n (%) | 0.317 | |||||
| M0 | 142 (69.3) | 45 (59.2) | 21 (75.0) | 58 (75.3) | 18 (75.0) | |
| M1a | 39 (19.0) | 20 (26.3) | 3 (10.7) | 12 (15.6) | 4 (16.7) | |
| M1b | 7 (3.4) | 3 (3.9) | 1 (3.6) | 3 (3.9) | 0 | |
| M1c | 17 (8.3) | 8 (10.5) | 3 (10.7) | 4 (5.2) | 2 (8.3) | |
| Unknown | 0 | 0 | ||||
| Multifocal primary tumours, n (%) | 63 (30.7) | 16 (21.1) | 9 (32.1) | 33 (42.9) | 5 (20.8) | 0.049 |
| Lymph node resections | ||||||
| Median, n (range) | 8.0 (0–62) | 5 (0–30) | 6 (0–24) | 11 (0–42) | 5.5 (0–62) | 0.014 |
| Pts. with ≥8 LN, n (%) | 108 (52.9) | 34 (45.3) | 13 (46.4) | 51 (66.2) | 10 (41.7) | 0.037 |
| LN+/patient, median (range) | 2.0 (0–15) | 2.0 (0–15) | 2 (0–10) | 2 (0–13) | 2.5 (0–9) | 0.523 |
| Resection margins, n (%) | 0.716 | |||||
| R0 | 157 (76.6) | 57 (75.0) | 20 (71.4) | 64 (83.1) | 16 (66.7) | |
| R1 | 20 (9.8) | 8 (10.5) | 2 (7.1) | 9 (11.7) | 1 (4.2) | |
| R2 | 26 (12.7) | 9 (11.8) | 6 (21.4) | 4 (5.2) | 7 (29.2) | |
| Unknown | 2 (1.0) | 2 (2.6) | 0 | 0 | 0 | |
| Curative surgery, n (%) | 137 (66.8) | 42 (55.3) | 20 (71.4) | 60 (77.9) | 15 (62.5) | 0.027 |
| Variable | Univariate | Multivariate | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Tumour resected | 0.40 (0.25–0.62) | <0.001 | 0.52 (0.29–0.91) | 0.022 |
| WHO grade 2 | 1.51 (1.00–2.27) | 0.047 | 1.28 (0.83–1.97) | 0.265 |
| ENETS stage | 1.53 (1.13–2.07) | 0.006 | 1.81 (1.26–2.61) | 0.001 |
| Female sex | 1.40 (0.98–2.06) | 0.068 | 1.32 (0.88–1.99) | 0.18 |
| Age at diagnosis | 1.06 (1.04–1.09) | <0.001 | 1.07 (1.05–1.10) | 0.001 |
| Diagnosis in second period | 0.58 (0.37–0.90) | 0.015 | 0.56 (0.35–0.89) | 0.014 |
| Variable | Multivariate | |
|---|---|---|
| HR (95% CI) | p-Value | |
| R1 or R2 resection * | 0.64 (0.30–0.1.37) | 0.25 |
| WHO grade 2 | 1.28 (0.60–2.72) | 0.53 |
| ENETS stage | 2.29 (1.14–4.57) | 0.019 |
| Female sex | 1.27 (0.61–2.65) | 0.52 |
| Age at diagnosis | 1.07 (1.03–1.12) | 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Folkestad, O.; Hauso, Ø.; Mjønes, P.; Fougner, R.; Wasmuth, H.H.; Fossmark, R. Survival Trends in Patients with Small Intestinal Neuroendocrine Tumours—A Cohort Study in Central Norway. Cancers 2023, 15, 3272. https://doi.org/10.3390/cancers15133272
Folkestad O, Hauso Ø, Mjønes P, Fougner R, Wasmuth HH, Fossmark R. Survival Trends in Patients with Small Intestinal Neuroendocrine Tumours—A Cohort Study in Central Norway. Cancers. 2023; 15(13):3272. https://doi.org/10.3390/cancers15133272
Chicago/Turabian StyleFolkestad, Oddry, Øyvind Hauso, Patricia Mjønes, Reidun Fougner, Hans H. Wasmuth, and Reidar Fossmark. 2023. "Survival Trends in Patients with Small Intestinal Neuroendocrine Tumours—A Cohort Study in Central Norway" Cancers 15, no. 13: 3272. https://doi.org/10.3390/cancers15133272
APA StyleFolkestad, O., Hauso, Ø., Mjønes, P., Fougner, R., Wasmuth, H. H., & Fossmark, R. (2023). Survival Trends in Patients with Small Intestinal Neuroendocrine Tumours—A Cohort Study in Central Norway. Cancers, 15(13), 3272. https://doi.org/10.3390/cancers15133272