

Effectiveness of Treatments That Alter Metabolomics in Cancer Patients—A Systematic Review




Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Documentary Sources Consulted
2.3. Search Strategy
2.4. Inclusion Criteria
- −
- Human randomized controlled clinical trials published between 2016 and 2023.
- −
- The use of English or Spanish language.
- −
- Breast cancer, colon cancer and prostate cancer.
2.5. Exclusion Criteria
2.6. Study Selection Process
2.7. Data Extraction
2.8. Risk of Bias Measurement Tool
2.9. Quality of the Evidence
3. Results
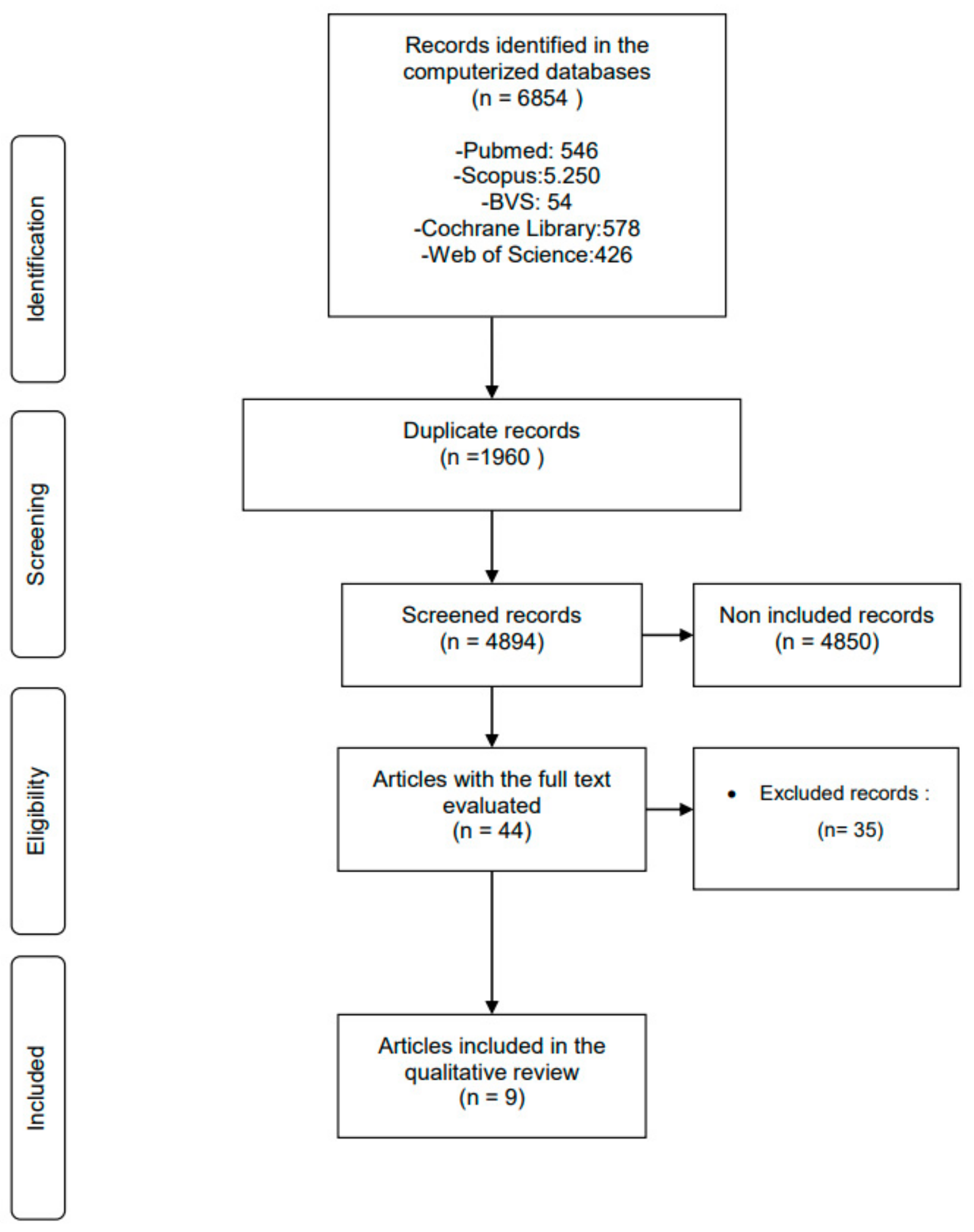
3.1. Study Identification and Selection Process
3.2. General Characteristics of the Selected Studies
3.3. Risk of Bias in the Included Studies
3.4. Intervention Characteristics
- (1)
- Pietri et al. [44] studied the effects of DHEA intake, 100 mg/day orally on post-menopausal patients with breast cancer with the main outcome safety. The duration of treatment was 8 weeks and an intervention and a control group were included.
- (2)
- Ávila-Gálvez A et al. [45] studied the impact of a multi-nutrient supplement on women with breast cancer after biopsy-confirmed diagnosis for surgery. Nineteen breast cancer patients consumed three capsules daily whereas the control group (n = 8) did not receive any additional treatment. The multi-nutrient capsules contained pomegranate, orange, lemon, olive extracts, cocoa and grape seed.
- (3)
- Chi et al. [46] studied the metabolomic changes in a low-carbohydrate diet in conjunction with androgen deprivation therapy. Fasting blood samples were taken for the control of glucose, insulin, protein C, lipids, etc., and these samples were used for metabolomic analysis. Eleven participants in the intervention group finalized the study (11/20), whereas 18 in the control group also finalized the study (18/20).
- (4)
- Qu et al. [47] studied the effects of the combined application of neoadjuvant docetaxel and androgen deprivation therapy in people with prostate cancer. The purpose of this study was to investigate, with the use of metabolomics, the difference in endogenous tumor metabolism in prostate cancer patients who received or did not receive neoadjuvant therapy. The cohort consisted of 42 patients receiving the combined neoadjuvant therapy before radical prostatectomy whereas 54 patients in the control group were operated on without additional intervention next to the radical prostatectomy.
- (5)
- Lee et al. [48] studied the metabolic effects of intravenous selenium injections in breast cancer patients. A placebo (n = 14) and an experimental group (n = 15) were included in the study design.
- (6)
- Febvey-Combes et al. [49] studied the effects on metabolomics of an aerobic exercise program in breast cancer patients. A six-month long combined program including aerobic exercise and nutritional changes were added to the current chemotherapy treatment in women (n = 40) with breast cancer, whereas the control group (n = 18) only received chemotherapy.
- (7)
- Hanada et al. [50] studied the effects of a Chinese herbal medicine, Daikenchuto, on the metabolites of patients with colon cancer after a left-sided laparoscopic colectomy. Nine patients received the herbal medicine for 6 months whereas the control group did not receive any additional treatment to the colectomy.
- (8)
- Zarei et al. [51] studied the effects of bean intake on metabolomics measured in plasma and urine of obese and overweight colorectal cancer survivors. Plasma and urine samples were collected at baseline, 2 weeks and 4 weeks after consumption. The study included an intervention group and a placebo meal-receiving group of in total 20 participants.
- (9)
- Ávila-Gálvez B et al. [52] studied the presence of isoflavones, curcuminoids and lignans (polyphenols) in the tissue of people with breast cancer after the intake of three capsules daily, containing the aforementioned substances daily. The metabolic profiles of these polyphenols in normal and malignant breast tissue in newly diagnosed breast cancer patients and the anticancer activity of metabolites produced in tissues were evaluated. The patients were randomized into two groups; the patients of the experimental group consumed three capsules daily until the day of surgery. The control group did not receive any type of supplementation before they were operated on.
3.5. Results of Oncometabolite Targeting Interventions
- Breast cancer: five studies researched metabolomic changes in breast cancer (Table 4).
- (a)
- Pietri et al. [44]: no clear changes were observed in metabolites during the 8 weeks of treatment; the authors indicate that this may be due to the small sample size.
- (b)
- Ávila-Gálvez A et al. [45]: some changes were detected in the following oncometabolites after the intervention were urolithin A-3-O-glucuronide, 2,5-dihydroxybenzoic acid and resveratrol-3-O-sulfate.
- (c)
- Lee et al. [48]: in this study, the levels of corticosterone, LTB4-DMA and PGE3, which are anti-inflammatory compounds, were found to be significantly higher in the experimental group compared with the control group.
- (d)
- Febvey-Combes et al. [49]: after 6 months of intervention, no metabolomic changes were observed between the subjects who engaged in the experimental group and those in the control group. Inflammatory biomarkers increased slightly in both groups but no significant differences were observed between groups.
- (e)
- Ávila-Gálvez B et al. [52]: in the experimental group, high concentrations of curcumin were present in mammary tissues. The use of curcumin could offer long-term anticancer effects.
- Prostate cancer (Table 5):
- (a)
- The study by Chi et al. [46] in the experimental group comprised a combination of a dietary intervention along with androgen deprivation therapy. Several changes were found in the experimental group such as a decrease in steroid synthesis, and a reduction in androgen levels, which were associated with higher serum glucose levels. In addition, 3-hydroxybutyric acid and ketogenesis decreased, and acyl-carnitines and 3-formyl-indole were reduced with these changes being associated with androgen deprivation therapy.
- (b)
- The study by Qu et al. [47] investigated a combined neoadjuvant therapy with androgen deprivation therapy (experimental group) versus androgen deprivation therapy only (control group). Nucleotide synthesis, lipids, citric acid, and glutathione metabolism were all beneficially changed after the combined treatment in prostate cancer patients compared with the control group.
- Colon cancer—colorectal (Table 6):
- (a)
- Hanada et al. [50]: metabolome and gut microbiome analyses showed that the levels of plasma lipid mediators associated with the pro-inflammatory arachidonic acid cascade were lower in the experimental group than in the control group, which suspects a reduction in inflammatory activity in those patients using Daikenchuto as a complementary intervention.
- (b)
- Zarei et al. [51]: the following metabolites which all have protective actions against cancer showed an increase in the experimental group only: (i) 2,3-dihydroxy-2-methylbutyrate, (ii) S-methylcysteine and pipecolate in plasma and (iii) S-adenosylhomocysteine and (iv) cysteine in urine. These promising results justify further studies of the effects nutritional interventions in people suffering from colon cancer and a primary intervention study could also be conducted.
3.6. Grade System
4. Discussion
4.1. Practical Application
Study Limitations
4.2. Prospective
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Salaverry, O. La etimología del cáncer y su curioso curso histórico. Rev. Peru Med. Exp. Salud Publica 2013, 30, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Halperin, E.C. Paleo-oncology: The role of ancient remains in the study of cancer. Perspect. Biol. Med. 2004, 47, 1–14. [Google Scholar] [CrossRef]
- Salas, D.; Peiró, R. Evidencias sobre la prevención del cáncer [Evidence on the prevention of cancer]. Rev. Esp. Sanid Penit. 2013, 15, 66–75. [Google Scholar] [CrossRef]
- Muhamad, N.; Na-Bangchang, K. Metabolite Profiling in Anticancer Drug Development: A Systematic Review. Drug Des. Dev. Ther. 2020, 14, 1401–1444. [Google Scholar] [CrossRef]
- Conceptos, Teorías y Factores Psicosociales en la Adaptación al Cáncer [Actas Esp. Psiquiatr. 2005]—Medes. Available online: https://medes.com/publication/19455 (accessed on 11 July 2023).
- Gallo Cantafio, M.E.; Grillone, K.; Caracciolo, D.; Scionti, F.; Arbitrio, M.; Barbieri, V.; Pensabene, L.; Guzzi, P.H.; Di Martino, M.T. From Single Level Analysis to Multi-Omics Integrative Approaches: A Powerful Strategy towards the Precision Oncology. High Throughput 2018, 7, 33. [Google Scholar] [CrossRef] [PubMed]
- Hobbins, L.; Gaoua, N.; Hunter, S.; Girard, O. Psycho-physiological responses to perceptually-regulated interval runs in hypoxia and normoxia. Physiol. Behav. 2019, 209, 112611. [Google Scholar] [CrossRef] [PubMed]
- McTiernan, A.; Friedenreich, C.M.; Katzmarzyk, P.T.; Powell, K.E.; Macko, R.; Buchner, D.; Pescatello, L.S.; Bloodgood, B.; Tennant, B.; Vaux-Bjerke, A.; et al. Physical Activity in Cancer Prevention and Survival: A Systematic Review. Med. Sci. Sports Exerc. 2019, 51, 1252–1261. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Wishart, D. Metabolomics and the Multi-Omics View of Cancer. Metabolites 2022, 12, 154. [Google Scholar] [CrossRef]
- Griffin, J.L.; Shockcor, J.P. Metabolic profiles of cancer cells. Nat. Rev. Cancer 2004, 4, 551–561. [Google Scholar] [CrossRef]
- Schmidt, D.R.; Patel, R.; Kirsch, D.G.; Lewis, C.A.; Vander Heiden, M.G.; Locasale, J.W. Metabolomics in cancer research and emerging applications in clinical oncology. CA Cancer J. Clin. 2021, 71, 333–358. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, O.; Rocklöv, J.; Lehoux, A.P.; Bergquist, J.; Rutgersson, A.; Blunt, M.J.; Birnbaum, L.S. The human exposome and health in the Anthropocene. Int. J. Epidemiol. 2021, 50, 378–389. [Google Scholar] [CrossRef]
- Aprile, F.; Bruno, G.; Palma, R.; Mascellino, M.T.; Panetta, C.; Scalese, G.; Oliva, A.; Severi, C.; Pontone, S. Microbiota Alterations in Precancerous Colon Lesions: A Systematic Review. Cancers 2021, 13, 3061. [Google Scholar] [CrossRef] [PubMed]
- Reglero, C.; Reglero, G. Precision Nutrition and Cancer Relapse Prevention: A Systematic Literature Review. Nutrients 2019, 11, 2799. [Google Scholar] [CrossRef]
- Koopaie, M.; Kolahdooz, S.; Fatahzadeh, M.; Manifar, S. Salivary biomarkers in breast cancer diagnosis: A systematic review and diagnostic meta-analysis. Cancer Med. 2022, 11, 2644–2661. [Google Scholar] [CrossRef]
- Leysen, L.; Lahousse, A.; Nijs, J.; Adriaenssens, N.; Mairesse, O.; Ivakhnov, S.; Bilterys, T.; Van Looveren, E.; Pas, R.; Beckwée, D. Prevalence and risk factors of sleep disturbances in breast cancersurvivors: Systematic review and meta-analyses. Support Care Cancer 2019, 27, 4401–4433. [Google Scholar] [CrossRef]
- Takayama, T.; Tsutsui, H.; Shimizu, I.; Toyama, T.; Yoshimoto, N.; Endo, Y.; Inoue, K.; Todoroki, K.; Min, J.Z.; Mizuno, H.; et al. Diagnostic approach to breast cancer patients based on target metabolomics in saliva by liquid chromatography with tandem mass spectrometry. Clin. Chim. Acta 2016, 452, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Paz, E.A.; LaFleur, B.; Gerner, E.W. Polyamines are oncometabolites that regulate the LIN28/let-7 pathway in colorectal cancer cells. Mol. Carcinog. 2014, 53 (Suppl. 1), E96–E106. [Google Scholar] [CrossRef] [PubMed]
- Kdadra, M.; Höckner, S.; Leung, H.; Kremer, W.; Schiffer, E. Metabolomics Biomarkers of Prostate Cancer: A Systematic Review. Diagnostics 2019, 9, 21. [Google Scholar] [CrossRef] [PubMed]
- Feng, L.R.; Wolff, B.S.; Lukkahatai, N.; Espina, A.; Saligan, L.N. Exploratory Investigation of Early Biomarkers for Chronic Fatigue in Prostate Cancer Patients Following Radiation Therapy. Cancer Nurs. 2017, 40, 184–193. [Google Scholar] [CrossRef]
- Czerwińska, M.; Bilewicz, A.; Kruszewski, M.; Wegierek-Ciuk, A.; Lankoff, A. Targeted Radionuclide Therapy of Prostate Cancer-From Basic Research to Clinical Perspectives. Molecules 2020, 25, 1743. [Google Scholar] [CrossRef]
- Wang, L.; Lu, B.; He, M.; Wang, Y.; Wang, Z.; Du, L. Prostate Cancer Incidence and Mortality: Global Status and Temporal Trends in 89 Countries From 2000 to 2019. Front. Public Health 2022, 10, 811044. [Google Scholar] [CrossRef]
- Wang, G.; Zhao, D.; Spring, D.J.; DePinho, R.A. Genetics and biology of prostate cancer. Genes Dev. 2018, 32, 1105–1140. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Zhang, K. Quantifying the Contributions of Environmental Factors to Prostate Cancer and Detecting Risk-Related Diet Metrics and Racial Disparities. Cancer Inform. 2023, 22, 11769351231168006. [Google Scholar] [CrossRef]
- Glunde, K.; Bhujwalla, Z.M.; Ronen, S.M. Choline metabolism in malignant transformation. Nat. Rev. Cancer 2011, 11, 835–848. [Google Scholar] [CrossRef]
- Lala, P.K.; Chakraborty, C. Role of nitric oxide in carcinogenesis and tumour progression. Lancet Oncol. 2001, 2, 149–156. [Google Scholar] [CrossRef]
- Mi, S.; Gong, L.; Sui, Z. Friend or Foe? An Unrecognized Role of Uric Acid in Cancer Development and the Potential Anticancer Effects of Uric Acid-lowering Drugs. J. Cancer 2020, 11, 5236–5244. [Google Scholar] [CrossRef]
- Kukko, V.; Kaipia, A.; Talala, K.; Taari, K.; Tammela, T.L.J.; Auvinen, A.; Murtola, T.J. Allopurinol and prostate cancer survival in a Finnish population-based cohort. Prostate Cancer Prostatic Dis. 2022. [Google Scholar] [CrossRef] [PubMed]
- Ni, Y.; Xie, G.; Jia, W. Metabonomics of human colorectal cancer: New approaches for early diagnosis and biomarker discovery. J. Proteome Res. 2014, 13, 3857–3870. [Google Scholar] [CrossRef] [PubMed]
- Zwezerijnen-Jiwa, F.H.; Sivov, H.; Paizs, P.; Zafeiropoulou, K.; Kinross, J. A systematic review of microbiome-derived biomarkers for early colorectal cancer detection. Neoplasia 2023, 36, 100868. [Google Scholar] [CrossRef]
- Mallafré-Muro, C.; Llambrich, M.; Cumeras, R.; Pardo, A.; Brezmes, J.; Marco, S.; Gumà, J. Comprehensive Volatilome and Metabolome Signatures of Colorectal Cancer in Urine: A Systematic Review and Meta-Analysis. Cancers 2021, 13, 2534. [Google Scholar] [CrossRef]
- Wanders, D.; Hobson, K.; Ji, X. Methionine Restriction and Cancer Biology. Nutrients 2020, 12, 684. [Google Scholar] [CrossRef]
- Zhang, H.-L.; Zhang, A.-H.; Miao, J.-H.; Sun, H.; Yan, G.-L.; Wu, F.-F.; Wang, X.-J. Targeting regulation of tryptophan metabolism for colorectal cancer therapy: A systematic review. RSC Adv. 2019, 9, 3072–3080. [Google Scholar] [CrossRef]
- Junn, E.; Mouradian, M.M. MicroRNAs in neurodegenerative diseases and their therapeutic potential. Pharmacol. Ther. 2012, 133, 142–150. [Google Scholar] [CrossRef]
- Luszczynska, A.; Benight, C.C.; Cieslak, R. Self-Efficacy and Health-Related Outcomes of Collective Trauma. Eur. Psychologist. 2009, 14, 51–62. [Google Scholar] [CrossRef]
- Tian, J.; Xue, W.; Yin, H.; Zhang, N.; Zhou, J.; Long, Z.; Wu, C.; Liang, Z.; Xie, K.; Li, S.; et al. Differential Metabolic Alterations and Biomarkers Between Gastric Cancer and Colorectal Cancer: A Systematic Review and Meta-Analysis. Onco. Targets Ther. 2020, 13, 6093–6108. [Google Scholar] [CrossRef]
- Yang, L.; Wang, Y.; Cai, H.; Wang, S.; Shen, Y.; Ke, C. Application of metabolomics in the diagnosis of breast cancer: A systematic review. J. Cancer 2020, 11, 2540–2551. [Google Scholar] [CrossRef]
- Lima, A.R.; Pinto, J.; Amaro, F.; Bastos, M.L.; Carvalho, M.; Guedes de Pinho, P. Advances and Perspectives in Prostate Cancer Biomarker Discovery in the Last 5 Years through Tissue and Urine Metabolomics. Metabolites 2021, 11, 181. [Google Scholar] [CrossRef]
- Welch, V.; Petticrew, M.; Tugwell, P.; Moher, D.; O’Neill, J.; Waters, E.; White, H. PRISMA-Equity 2012 extension: Reporting guidelines for systematic reviews with a focus on health equity. PLoS Med. 2012, 9, e1001333. [Google Scholar] [CrossRef]
- Rayyan—A Web and Mobile App for Systematic Reviews|Systematic Reviews|Full Text. Available online: https://systematicreviewsjournal.biomedcentral.com/articles/10.1186/s13643-016-0384-4 (accessed on 11 July 2023).
- Cochrane Handbook for Systematic Reviews of Interventions. Available online: https://handbook-5-1.cochrane.org/ (accessed on 11 July 2023).
- Aguayo-Albasini, J.L.; Flores-Pastor, B.; Soria-Aledo, V. Sistema GRADE: Clasificación de la calidad de la evidencia y graduación de la fuerza de la recomendación [GRADE system: Classification of quality of evidence and strength of recommendation]. Cir. Esp. 2014, 92, 82–88. [Google Scholar] [CrossRef]
- Pietri, E.; Massa, I.; Bravaccini, S.; Ravaioli, S.; Tumedei, M.M.; Petracci, E.; Donati, C.; Schirone, A.; Piacentini, F.; Gianni, L.; et al. Phase II Study of Dehydroepiandrosterone in Androgen Receptor-Positive Metastatic Breast Cancer. Oncologist 2019, 24, 743-e205. [Google Scholar] [CrossRef]
- Ávila-Gálvez, M.Á.; García-Villalba, R.; Martínez-Díaz, F.; Ocaña-Castillo, B.; Monedero-Saiz, T.; Torrecillas-Sánchez, A.; Abellán, B.; González-Sarrías, A.; Espín, J.C. Metabolic Profiling of Dietary Polyphenols and Methylxanthines in Normal and Malignant Mammary Tissues from Breast Cancer Patients. Mol. Nutr. Food Res. 2019, 63, e1801239. [Google Scholar] [CrossRef]
- Chi, J.; Lin, P.; Tolstikov, V.; Oyekunle, T.; Chen, E.Y.; Bussberg, V.; Greenwood, B.; Sarangarajan, R.; Narain, N.R.; Kiebish, M.A.; et al. Metabolomic effects of androgen deprivation therapy treatment for prostate cancer. Cancer Med. 2020, 9, 3691–3702. [Google Scholar] [CrossRef]
- Qu, F.; Gu, Y.; Xue, M.; He, M.; Zhou, F.; Wang, G.; Peng, Y. Impact of therapy on cancer metabolism in high-risk localized prostate cancer treated with neoadjuvant docetaxel and androgen deprivation therapy. Prostate 2021, 81, 560–571. [Google Scholar] [CrossRef]
- Lee, H.; Lee, B.; Kim, Y.; Min, S.; Yang, E.; Lee, S. Effects of Sodium Selenite Injection on Serum Metabolic Profiles in Women Diagnosed with Breast Cancer-Related Lymphedema-Secondary Analysis of a Randomized Placebo-Controlled Trial Using Global Metabolomics. Nutrients 2021, 13, 3253. [Google Scholar] [CrossRef]
- Febvey-Combes, O.; Jobard, E.; Rossary, A.; Pialoux, V.; Foucaut, A.-M.; Morelle, M.; Delrieu, L.; Martin, A.; Caldefie-Chézet, F.; Touillaud, M.; et al. Effects of an Exercise and Nutritional Intervention on Circulating Biomarkers and Metabolomic Profiling During Adjuvant Treatment for Localized Breast Cancer: Results from the PASAPAS Feasibility Randomized Controlled Trial. Integr. Cancer Ther. 2021, 20, 1534735420977666. [Google Scholar] [CrossRef] [PubMed]
- Hanada, K.; Wada, T.; Kawada, K.; Hoshino, N.; Okamoto, M.; Hirata, W.; Mizuno, R.; Itatani, Y.; Inamoto, S.; Takahashi, R.; et al. Effect of herbal medicine daikenchuto on gastrointestinal symptoms following laparoscopic colectomy in patients with colon cancer: A prospective randomized study. Biomed Pharmacother. 2021, 141, 111887. [Google Scholar] [CrossRef]
- Zarei, I.; Baxter, B.A.; Oppel, R.C.; Borresen, E.C.; Brown, R.J.; Ryan, E.P. Plasma and Urine Metabolite Profiles Impacted by Increased Dietary Navy Bean Intake in Colorectal Cancer Survivors: A Randomized-Controlled Trial. Cancer Prev. Res. 2021, 14, 497–508. [Google Scholar] [CrossRef]
- Ávila-Gálvez, M.; González-Sarrías, A.; Martínez-Díaz, F.; Abellán, B.; Martínez-Torrano, A.J.; Fernández-López, A.J.; Giménez-Bastida, J.A.; Espín, J.C. Disposition of Dietary Polyphenols in Breast Cancer Patients’ Tumors, and Their Associated Anticancer Activity: The Particular Case of Curcumin. Mol. Nutr. Food Res. 2021, 65, e2100163. [Google Scholar] [CrossRef] [PubMed]
- Barcenas, C.; Hurvitz, S.; Di Palma, J.; Bose, R.; Chien, A.; Iannotti, N.; Marx, G.; Brufsky, A.; Litvak, A.; Ibrahim, E.; et al. Improved tolerability of neratinib in patients with HER2-positive early-stage breast cancer: The CONTROL trial. Ann. Oncol. 2020, 31, 1223–1230. [Google Scholar] [CrossRef] [PubMed]
- Tutt, A.N.; Garber, J.E.; Kaufman, B.; Viale, G.; Fumagalli, D.; Rastogi, P.; Gelber, R.D.; de Azambuja, E.; Fielding, A.; Balmaña, J.; et al. Adjuvant Olaparib for Patients with BRCA1- or BRCA2-Mutated Breast Cancer. N. Engl. J. Med. 2021, 384, 2394–2405. [Google Scholar] [CrossRef] [PubMed]
- Akinyele, O.; Wallace, H.M. Understanding the Polyamine and mTOR Pathway Interaction in Breast Cancer Cell Growth. Med. Sci. 2022, 10, 51. [Google Scholar] [CrossRef] [PubMed]
- Razavi, M.; Jamilian, M.; Kashan, Z.F.; Heidar, Z.; Mohseni, M.; Ghandi, Y.; Bagherian, T.; Asemi, Z. Selenium Supplementation and the Effects on Reproductive Outcomes, Biomarkers of Inflammation, and Oxidative Stress in Women with Polycystic Ovary Syndrome. Horm. Metab. Res. 2016, 48, 185–190. [Google Scholar] [CrossRef]
- Kunihiro, A.G.; Brickey, J.A.; Frye, J.B.; Cheng, J.N.; Luis, P.B.; Schneider, C.; Funk, J.L. Curcumin Inhibition of TGFβ signaling in bone metastatic breast cancer cells and the possible role of oxidative metabolites. J. Nutr. Biochem. 2022, 99, 108842. [Google Scholar] [CrossRef]
- Bahrami, A.; Atkin, S.L.; Majeed, M.; Sahebkar, A. Effects of curcumin on hypoxia-inducible factor as a new therapeutic target. Pharmacol. Res. 2018, 137, 159–169. [Google Scholar] [CrossRef]
- James, M.I.; Iwuji, C.; Irving, G.; Karmokar, A.; Higgins, J.A.; Griffin-Teal, N.; Thomas, A.; Greaves, P.; Cai, H.; Patel, S.R.; et al. Curcumin inhibits cancer stem cell phenotypes in ex vivo models of colorectal liver metastases, and is clinically safe and tolerable in combination with FOLFOX chemotherapy. Cancer Lett. 2015, 364, 135–141. [Google Scholar] [CrossRef]
- Keenan, M.M.; Chi, J.T. Alternative fuels for cancer cells. Cancer J. 2015, 21, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.E.; Meynköhn, A.; Habermann, N.; Wiskemann, J.; Oelmann, J.; Hof, H.; Wessels, S.; Klassen, O.; Debus, J.; Potthoff, K.; et al. Resistance Exercise and Inflammation in Breast Cancer Patients Undergoing Adjuvant Radiation Therapy: Mediation Analysis from a Randomized, Controlled Intervention Trial. Int. J. Radiat. Oncol. Biol. Phys. 2016, 94, 329–337. [Google Scholar] [CrossRef]
- Bye, A.; Sandmael, J.A.; Stene, G.B.; Thorsen, L.; Balstad, T.R.; Solheim, T.S.; Pripp, A.H.; Oldervoll, L.M. Exercise and Nutrition Interventions in Patients with Head and Neck Cancer during Curative Treatment: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 3233. [Google Scholar] [CrossRef]
- Wang, L.; Wu, L.; Qian, C.; Ju, Y.; Liu, T.; Chen, Y.; Wang, X. The Beneficial Effect of a Healthy Dietary Pattern on Androgen Deprivation Therapy-Related Metabolic Abnormalities in Patients with Prostate Cancer: A Meta-Analysis Based on Randomized Controlled Trials and Systematic Review. Metabolites 2022, 12, 969. [Google Scholar] [CrossRef]
- Ben Zichri, S.; Kolusheva, S.; Shames, A.I.; Schneiderman, E.A.; Poggio, J.L.; Stein, D.E.; Doubijensky, E.; Levy, D.; Orynbayeva, Z.; Jelinek, R. Mitochondria membrane transformations in colon and prostate cancer and their biological implications. Biochim. Biophys. Acta Biomembr. 2021, 1863, 183471. [Google Scholar] [CrossRef] [PubMed]
- Hoshino, N.; Kawada, K.; Hida, K.; Wada, T.; Takahashi, R.; Yoshitomi, M.; Sakai, Y. Effect of Daikenchuto (TJ-100) on gastrointestinal symptoms following laparoscopic colectomy in patients with colon cancer: Study protocol for a randomized controlled trial. Trials 2017, 18, 553. [Google Scholar] [CrossRef] [PubMed]
- Han, S.; Gao, J.; Zhou, Q.; Liu, S.; Wen, C.; Yang, X. Role of intestinal flora in colorectal cancer from the metabolite perspective: A systematic review. Cancer Manag. Res. 2018, 10, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Bischoff-Ferrari, H.A.; Willett, W.C.; Manson, J.E.; Dawson-Hughes, B.; Manz, M.G.; Theiler, R.; Braendle, K.; Vellas, B.; Rizzoli, R.; Kressig, R.W.; et al. Combined Vitamin D, Omega-3 Fatty Acids, and a Simple Home Exercise Program May Reduce Cancer Risk Among Active Adults Aged 70 and Older: A Randomized Clinical Trial. Front. Aging 2022, 3, 852643. [Google Scholar] [CrossRef]


{kind=link}
| Author | Year | Country | Cancer | Sample | Gender | Age (Years) |
|---|---|---|---|---|---|---|
| Pietri et al. [44] | 2019 | Italy | Breast Cancer | N = 18 | Female | 74 |
| Ávila-Galvez et al. [45] | 2019 | Spain | Breast Cancer | N = 27 | Female 19 Female 8 (CG) | 56 ± 10 |
| Chi et al. [46] | 2020 | USA | Prostate Cancer | N = 40 | Male | - |
| Qu et al. [47] | 2021 | China | Prostate Cancer | N = 32 | Male | 64 (57–75) |
| Lee et al. [48] | 2021 | Switzerland | Breast Cancer | N = 29 | Female | - |
| Febvey-Combes et al. [49] | 2021 | France | Breast Cancer | N = 58 | Female | 53.8 |
| Hanada et al. [50]. | 2021 | Japan | Colon Cancer | N = 8 | Male/female 4/4 | 64.0 |
| N = 9 | Male/Female 6/3 | |||||
| Zarei et al. [51] | 2021 | USA | Colorectal Cancer | N = 20 | Male Female | - |
| Ávila-Galvez B et al. [52] | 2021 | Spain | Breast Cancer | N = 39 | Female | 55 ± 14 |
| Pietri et al. [44] | Ávila-Gálvez A et al. [45] | Chi et al. [46] | Qu et al. [47] | Lee et al. [48] | Combes et al. [49] | Hanada et al. [50] | Zarei et al. [51] | Ávila-Gálvez et al. [52] | |
|---|---|---|---|---|---|---|---|---|---|
| Proper sequence generation (selection risk) | + | + | + | + | + | + | + | + | + |
| Selection hiding (selection bias) | + | + | + | + | + | + | + | + | + |
| Blinding of participants and staff (implementation bias) | + | + | + | + | + | + | + | + | + |
| Blinding of outcome evaluators (detection bias) | − | + | + | + | − | + | + | + | + |
| Incomplete results data (wear bias) | − | + | + | + | − | + | + | + | ? |
| Selective reporting of results (notification bias) | + | + | + | + | + | + | + | + | + |
| Other sources of bias | ? | ? | ? | ? | ? | ? | ? | ? | ? |
| Author | Year | Type of Intervention | Dosage | Intervention | Duration of the Intervention (Weeks) | Changes (Weeks) | Metabolomics | Metabolite Changes | |
|---|---|---|---|---|---|---|---|---|---|
| Pietri et al. [44] | 2019 | Androgen deprivation therapy | DHEA 100 mg/day | GE = 12 | GC = 6 | 8 | 8 | Plasma | No changes observed |
| Ávila galvez A et al. [45] | 2019 | Capsules pomegranate, orange, lemon, olive, cocoa and grape seed extracts. | Three capsules daily | GE N = 19 | GC N = 8 | 9 | 1–2 | Urine, plasma, normal and malignant tissue | 2,5-dihydroxybenzoic acid, 2,6-dihydroxybenzoic acid. urolithin-a 3-o-glucuronide |
| Chi et al. [46] | 2020 | Extreme low-carbohydrate diet (LCD) + Androgen deprivation therapy | Not specified | GE N = 19 | GC N = 21 | 24 | 12–24 | Plasma | Dihydroxycholestanoyl taurine, dodecanedioic acid, eicosatetraenoic acid, palmitoylcarnitine, oleoylcarnitine, 2-Aminoadipic acid, malonylcarnitine, octanoylarnitine, hexanoylcarnitine, myristoylcarnitine, decanoylcarnitine, heptanoycarnitine, dodecanoylcarnitine, androsterone sulfate, hydroxymyristoylcarnitine, palmitelaidic acid, 3-hydroxybutryc acid |
| Qu et al. [47] | 2021 | Neoadjuvant docetaxel + Androgen deprivation therapy | docetaxel (75 mg/m2) every 3 weeks | GE N = 12 | GC N = 10 | 24 | 12–24 | tumoral tissue | Citrate, succinic acid, glutamine, GSSG, adenine, glycerol 3-phosphate, PC, PE, LPE, GSH, PS, uridine |
| Lee et al. [48] | 2021 | Sodium Selenite Injection | 500 µg sodium selenite, five times over 2 weeks. | GE N = 15 | GC N = 14 | 2 | 2 | Plasma | Cortisone, LTB4-DMA y PGE3, elevated in the experimental group |
| Febvey-Combes et al. [49] | 2021 | Aerobic exercise and dietary advice | exercise sessions 2–3 times a week supervised by a trainer. | GE N = 40 | GC N = 18 | 24 | No changes observed | Plasma | No changes observed |
| Hanada et al. [50] | 2021 | Herbal medicine Daikenchuto | DKT (5 g) orally three times daily | GE N = 8 | GC N = 9 | 4 | 4 | Plasma and faeces | Decrease in arachidonic acid, serratia and bilophila. |
| Zarei et al. [51] | 2021 | Dietary Navy Bean Intake | 35 g of bean powder/day | GE:10 | GC = 10 | 4 | 4 | Plasma and urine | 2,3-dihidroxi-2-metilbutirato S-methylcysteine, plasma pipecolate, urinary S-adenosylhomocysteine |
| Ávila-Galvez B et al. [52] | 2021 | Curcumin capsules | Three capsules/day (extracts of turmeric, red clover and flaxseed plus resveratrol; 296.4 mg phenolics/capsule; 296.4 mg phenolics/capsule) | GE N = 26 | GC N = 13 | From diagnosis to surgery | 1–2 | Plasma, urine, malignant tissue, normal tissue | 4′-O-glucuronide, demethoxycurcumin curcumin, resveratrol 3-O-glucuronide, dihydroresveratrol 3-O-glucuronide, resveratrol 3-O-sulfate, and resveratrol 3-O-sulfate. |
| Author | Year | Cancer | Results of Oncometabolite |
|---|---|---|---|
| Pietri et al. [44] | 2019 | Breast Cancer | No significant changes in oncometabolites were observed. |
| Ávila Galvez et al. [45] | 2019 | Breast Cancer | Changes in: urolithin A-3-O-glucuronide, 2,5-dihydroxybenzoic acid and resvera-trol-3-O-sulfate (after surgery). |
| Lee et al. [48] | 2021 | Breast Cancer | Corticosterone, LTB4-DMA and PGE levels increased in the experimental group. |
| Febveys-Combes et al. [49] | 2021 | Breast Cancer | No significant differences were observed |
| Ávila Galvez et al. [52] | 2021 | Breast Cancer | Curcumin may offer long-term anticancer effects |
| Author | Year | Cancer | Results of Oncometabolite |
|---|---|---|---|
| Chi et al. [46] | 2020 | Prostate Cancer | Decreased steroid synthesis, androgen levels, 3-hydroxybutyric acid, ketogenesis, acylcarnitines, and 3-formylindole |
| Qu et al. [47] | 2021 | Prostate Cancer | Beneficial changes in nucleotide synthesis, lipid, citric acid, and glutathione metabolism. |
| Author | Year | Cancer | Results of Oncometabolite |
|---|---|---|---|
| Hanada et al. [50] | 2021 | Colon Cancer | Decreased levels of plasma lipid mediators associated with the pro-inflammatory arachidonic acid cascade in the Daikenchuto group. |
| Zarei et al. [51] | 2021 | Colorectal Cancer | The following were increased in the experimental group: (i) 2,3-dihydroxy-2-methylbutyrate, (ii) S-methylcysteine and pipecolate in plasma and (iii) S-adenosylhomocysteine and cysteine in urine. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Navarro Ledesma, S.; Hamed-Hamed, D.; González-Muñoz, A.; Pruimboom, L. Effectiveness of Treatments That Alter Metabolomics in Cancer Patients—A Systematic Review. Cancers 2023, 15, 4297. https://doi.org/10.3390/cancers15174297
Navarro Ledesma S, Hamed-Hamed D, González-Muñoz A, Pruimboom L. Effectiveness of Treatments That Alter Metabolomics in Cancer Patients—A Systematic Review. Cancers. 2023; 15(17):4297. https://doi.org/10.3390/cancers15174297
Chicago/Turabian StyleNavarro Ledesma, Santiago, Dina Hamed-Hamed, Ana González-Muñoz, and Leo Pruimboom. 2023. "Effectiveness of Treatments That Alter Metabolomics in Cancer Patients—A Systematic Review" Cancers 15, no. 17: 4297. https://doi.org/10.3390/cancers15174297
APA StyleNavarro Ledesma, S., Hamed-Hamed, D., González-Muñoz, A., & Pruimboom, L. (2023). Effectiveness of Treatments That Alter Metabolomics in Cancer Patients—A Systematic Review. Cancers, 15(17), 4297. https://doi.org/10.3390/cancers15174297