

Haploidentical versus Double-Cord Blood Stem Cells as a Second Transplantation for Relapsed Acute Myeloid Leukemia

 , , , , , , , ,
, , , , , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Patient Characteristics
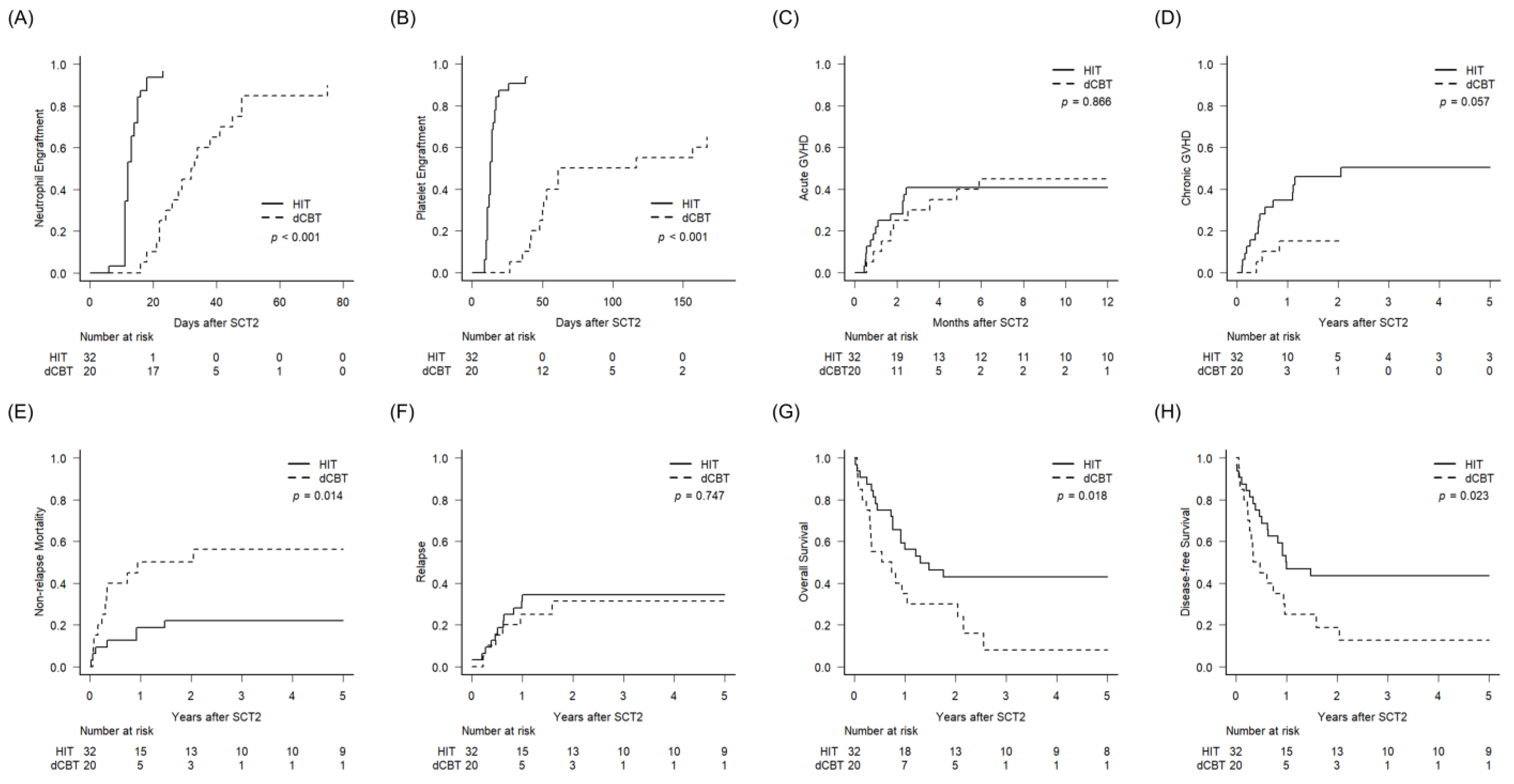
2.2. Engraftment, GVHD, and Other Complications
2.3. Survival Outcomes between HIT and dCBT
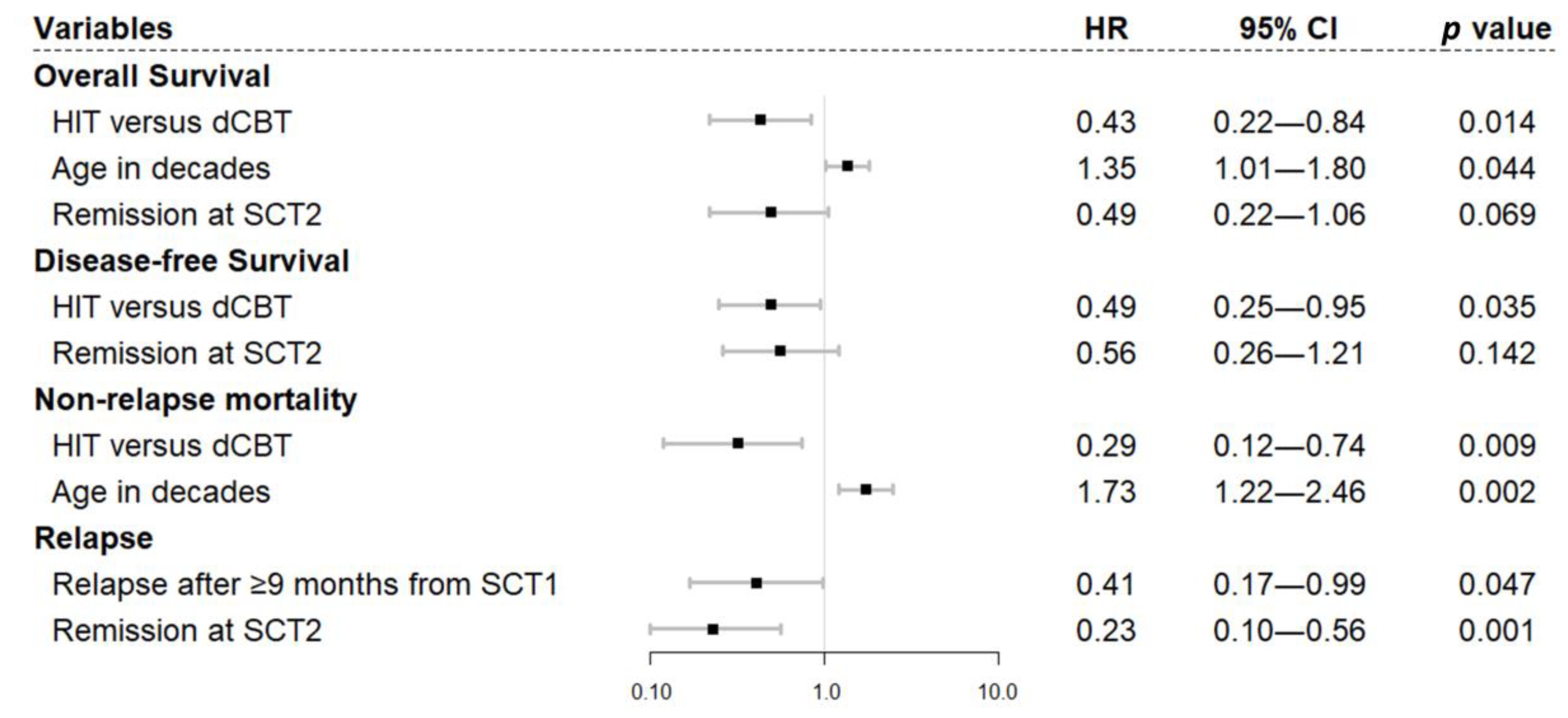
2.4. Factors Affecting Survival Outcomes
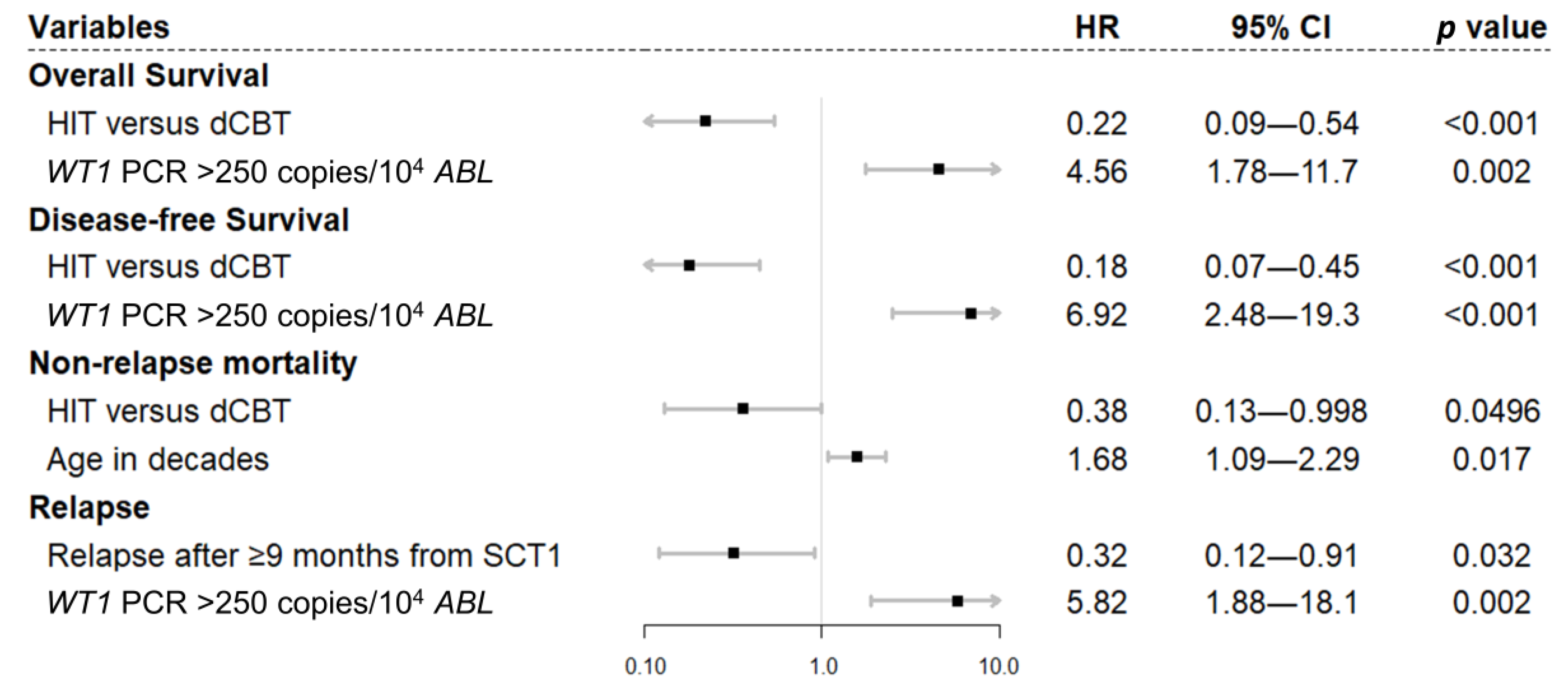
2.5. Subgroup Analysis with Patients Who Underwent Allogeneic SCT1
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Patients
5.2. Transplantation Procedures
5.3. Definitions
5.4. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sauer, T.; Silling, G.; Groth, C.; Rosenow, F.; Krug, U.; Gorlich, D.; Evers, G.; Albring, J.; Besoke, R.; Mesters, R.M.; et al. Treatment strategies in patients with AML or high-risk myelodysplastic syndrome relapsed after Allo-SCT. Bone Marrow Transplant. 2015, 50, 485–492. [Google Scholar] [CrossRef] [PubMed]
- Schmid, C.; Labopin, M.; Nagler, A.; Niederwieser, D.; Castagna, L.; Tabrizi, R.; Stadler, M.; Kuball, J.; Cornelissen, J.; Vorlicek, J.; et al. Treatment, risk factors, and outcome of adults with relapsed AML after reduced intensity conditioning for allogeneic stem cell transplantation. Blood 2012, 119, 1599–1606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kharfan-Dabaja, M.A.; Labopin, M.; Polge, E.; Nishihori, T.; Bazarbachi, A.; Finke, J.; Stadler, M.; Ehninger, G.; Lioure, B.; Schaap, N.; et al. Association of Second Allogeneic Hematopoietic Cell Transplant vs Donor Lymphocyte Infusion with Overall Survival in Patients with Acute Myeloid Leukemia Relapse. JAMA Oncol. 2018, 4, 1245–1253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Federico, V.; Dargenio, M.; Matera, R.; Canaris, A.; Bozzoli, V.; Caretto, V.; Carlino, D.; De Paolis, M.R.; Fina, M.P.; Loglisci, G.; et al. Venetoclax Combined with Hypomethylating Agent (HMA) is Safe and Effective May Be a Good Bridge to Transplant in High-risk Acute Myeloid Leukemia. Bone Marrow Transplant. 2021, 56, 28–29. [Google Scholar]
- Perl, A.E.; Larson, R.A.; Podoltsev, N.A.; Strickland, S.; Wang, E.S.; Atallah, E.; Schiller, G.J.; Martinelli, G.; Neubauer, A.; Sierra, J.; et al. Follow-up of patients with R/R FLT3-mutation-positive AML treated with gilteritinib in the phase 3 ADMIRAL trial. Blood 2022, 139, 3366–3375. [Google Scholar] [CrossRef] [PubMed]
- Hosing, C.; Saliba, R.M.; Shahjahan, M.; Estey, E.H.; Couriel, D.; Giralt, S.; Andersson, B.; Champlin, R.E.; De Lima, M. Disease burden may identify patients more likely to benefit from second allogeneic hematopoietic stem cell transplantation to treat relapsed acute myelogenous leukemia. Bone Marrow Transplant. 2005, 36, 157–162. [Google Scholar] [CrossRef]
- Christopeit, M.; Kuss, O.; Finke, J.; Bacher, U.; Beelen, D.W.; Bornhäuser, M.; Schwerdtfeger, R.; Bethge, W.A.; Basara, N.; Gramatzki, M.; et al. Second Allograft for Hematologic Relapse of Acute Leukemia after First Allogeneic Stem-Cell Transplantation from Related and Unrelated Donors: The Role of Donor Change. J. Clin. Oncol. 2013, 31, 3259–3271. [Google Scholar] [CrossRef]
- Andreola, G.; Labopin, M.; Beelen, D.; Chevallier, P.; Tabrizi, R.; Bosi, A.; Michallet, M.; Santarone, S.; Ehninger, G.; Polge, E.; et al. Long-term outcome and prognostic factors of second allogeneic hematopoietic stem cell transplant for acute leukemia in patients with a median follow-up of 10 years. Bone Marrow Transplant. 2015, 50, 1508–1512. [Google Scholar] [CrossRef]
- Ruutu, T.; de Wreede, L.C.; van Biezen, A.; Brand, R.; Mohty, M.; Dreger, P.; Duarte, R.; Peters, C.; Garderet, L.; Schonland, S.; et al. Second allogeneic transplantation for relapse of malignant disease: Retrospective analysis of outcome and predictive factors by the EBMT. Bone Marrow Transplant. 2015, 50, 1542–1550. [Google Scholar] [CrossRef] [Green Version]
- Orti, G.; Sanz, J.; Bermudez, A.; Caballero, D.; Martinez, C.; Sierra, J.; Cabrera Marin, J.R.; Espigado, I.; Solano, C.; Ferra, C.; et al. Outcome of Second Allogeneic Hematopoietic Cell Transplantation after Relapse of Myeloid Malignancies following Allogeneic Hematopoietic Cell Transplantation: A Retrospective Cohort on Behalf of the Grupo Espanol de Trasplante Hematopoyetico. Biol. Blood Marrow Transplant. 2016, 22, 584–588. [Google Scholar] [CrossRef] [Green Version]
- Park, S.S.; Kim, H.J.; Min, K.I.; Min, G.J.; Jeon, Y.W.; Yoon, J.H.; Yahng, S.A.; Shin, S.H.; Lee, S.E.; Cho, B.S.; et al. Prognostic Prediction Model for Second Allogeneic Stem-Cell Transplantation in Patients with Relapsed Acute Myeloid Leukemia: Single-Center Report. Clin. Lymphoma Myeloma Leuk. 2018, 18, e167–e182. [Google Scholar] [CrossRef]
- Schneidawind, C.; Hagmaier, V.; Faul, C.; Kanz, L.; Bethge, W.; Schneidawind, D. Second allogeneic hematopoietic cell transplantation enables long-term disease-free survival in relapsed acute leukemia. Ann. Hematol. 2018, 97, 2491–2500. [Google Scholar] [CrossRef]
- Gyurkocza, B.; Storb, R.; Chauncey, T.R.; Maloney, D.G.; Storer, B.E.; Sandmaier, B.M. Second allogeneic hematopoietic cell transplantation for relapse after first allografts. Leuk. Lymphoma 2019, 60, 1758–1766. [Google Scholar] [CrossRef]
- Kharfan-Dabaja, M.A.; Labopin, M.; Brissot, E.; Kroger, N.; Finke, J.; Ciceri, F.; Deconinck, E.; Blaise, D.; Chevallier, P.; Gramatzki, M.; et al. Second allogeneic haematopoietic cell transplantation using HLA-matched unrelated versus T-cell-replete haploidentical donor and survival in relapsed acute myeloid leukaemia. Br. J. Haematol. 2021, 193, 592–601. [Google Scholar] [CrossRef]
- Yalniz, F.F.; Saliba, R.M.; Greenbaum, U.; Ramdial, J.; Popat, U.; Oran, B.; Alousi, A.; Olson, A.; Alatrash, G.; Marin, D.; et al. Outcomes of Second Allogeneic Hematopoietic Cell Transplantation for Patients with Acute Myeloid Leukemia. Transplant. Cell Ther. 2021, 27, 689–695. [Google Scholar] [CrossRef]
- Tischer, J.; Engel, N.; Fritsch, S.; Prevalsek, D.; Hubmann, M.; Schulz, C.; Zoellner, A.K.; Bucklein, V.; Lippl, S.; Reibke, R.; et al. Second haematopoietic SCT using HLA-haploidentical donors in patients with relapse of acute leukaemia after a first allogeneic transplantation. Bone Marrow Transplant. 2014, 49, 895–901. [Google Scholar] [CrossRef] [Green Version]
- Shimoni, A.; Labopin, M.; Finke, J.; Ciceri, F.; Deconinck, E.; Kroger, N.; Gramatzki, M.; Stelljes, M.; Blaise, D.; Stoelzel, F.; et al. Donor selection for a second allogeneic stem cell transplantation in AML patients relapsing after a first transplant: A study of the Acute Leukemia Working Party of EBMT. Blood Cancer J. 2019, 9, 88. [Google Scholar] [CrossRef] [Green Version]
- Vrhovac, R.; Labopin, M.; Ciceri, F.; Finke, J.; Holler, E.; Tischer, J.; Lioure, B.; Gribben, J.; Kanz, L.; Blaise, D.; et al. Second reduced intensity conditioning allogeneic transplant as a rescue strategy for acute leukaemia patients who relapse after an initial RIC allogeneic transplantation: Analysis of risk factors and treatment outcomes. Bone Marrow Transplant. 2016, 51, 186–193. [Google Scholar] [CrossRef] [Green Version]
- Cho, B.S.; Min, G.J.; Park, S.; Park, S.S.; Shin, S.H.; Yahng, S.A.; Jeon, Y.W.; Yoon, J.H.; Lee, S.E.; Eom, K.S.; et al. Haploidentical vs matched unrelated donor transplantation for acute myeloid leukemia in remission: A prospective comparative study. Am. J. Hematol. 2021, 96, 98–109. [Google Scholar] [CrossRef]
- Chang, Y.J.; Zhao, X.Y.; Huang, X.J. Haploidentical Stem Cell Transplantation for Acute Myeloid Leukemia: Current Therapies, Challenges and Future Prospective. Front. Oncol. 2021, 11, 758512. [Google Scholar] [CrossRef]
- Barker, J.N.; Weisdorf, D.J.; Wagner, J.E. Creation of a double chimera after the transplantation of umbilical-cord blood from two partially matched unrelated donors. N. Engl. J. Med. 2001, 344, 1870–1871. [Google Scholar] [CrossRef] [PubMed]
- De Lima, M.; St John, L.S.; Wieder, E.D.; Lee, M.S.; McMannis, J.; Karandish, S.; Giralt, S.; Beran, M.; Couriel, D.; Korbling, M.; et al. Double-chimaerism after transplantation of two human leucocyte antigen mismatched, unrelated cord blood units. Br. J. Haematol. 2002, 119, 773–776. [Google Scholar] [CrossRef] [PubMed]
- Lister, J.; Gryn, J.F.; McQueen, K.L.; Harris, D.T.; Rossetti, J.M.; Shadduck, R.K. Multiple unit HLA-unmatched sex-mismatched umbilical cord blood transplantation for advanced hematological malignancy. Stem Cells Dev. 2007, 16, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Sideri, A.; Neokleous, N.; Brunet De La Grange, P.; Guerton, B.; Le Bousse Kerdilles, M.C.; Uzan, G.; Peste-Tsilimidos, C.; Gluckman, E. An overview of the progress on double umbilical cord blood transplantation. Haematologica 2011, 96, 1213–1220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoon, J.H.; Min, G.J.; Park, S.S.; Park, S.; Lee, S.E.; Cho, B.S.; Eom, K.S.; Kim, Y.J.; Kim, H.J.; Min, C.K.; et al. Durable outcomes of double-cord blood transplantation in adults with acute lymphoblastic leukemia: High-risk features for early and long-term mortality. Ther. Adv. Hematol. 2022, 13, 20406207221076762. [Google Scholar] [CrossRef]
- Srour, S.A.; Kongtim, P.; Rondon, G.; Chen, J.; Petropoulos, D.; Ramdial, J.; Popat, U.; Kebriaei, P.; Qazilbash, M.; Shpall, E.J.; et al. Haploidentical transplants for patients with relapse after the first allograft. Am. J. Hematol. 2020, 77, 45–49. [Google Scholar] [CrossRef]
- Cho, B.S.; Yoon, J.H.; Shin, S.H.; Yahng, S.A.; Lee, S.E.; Eom, K.S.; Kim, Y.J.; Lee, S.; Min, C.K.; Cho, S.G.; et al. Comparison of allogeneic stem cell transplantation from familial-mismatched/haploidentical donors and from unrelated donors in adults with high-risk acute myelogenous leukemia. Biol. Blood Marrow Transplant. 2012, 18, 1552–1563. [Google Scholar] [CrossRef] [Green Version]
- Yahng, S.A.; Kim, J.H.; Jeon, Y.W.; Yoon, J.H.; Shin, S.H.; Lee, S.E.; Cho, B.S.; Eom, K.S.; Kim, Y.J.; Lee, S.; et al. A well-tolerated regimen of 800 cGy TBI-fludarabine-busulfan-ATG for reliable engraftment after unmanipulated haploidentical peripheral blood stem cell transplantation in adult patients with acute myeloid leukemia. Biol. Blood Marrow Transplant. 2015, 21, 119–129. [Google Scholar] [CrossRef] [Green Version]
- Bacigalupo, A.; Ballen, K.; Rizzo, D.; Giralt, S.; Lazarus, H.; Ho, V.; Apperley, J.; Slavin, S.; Pasquini, M.; Sandmaier, B.M.; et al. Defining the intensity of conditioning regimens: Working definitions. Biol. Blood Marrow Transplant. 2009, 15, 1628–1633. [Google Scholar] [CrossRef] [Green Version]
- Giralt, S.; Ballen, K.; Rizzo, D.; Bacigalupo, A.; Horowitz, M.; Pasquini, M.; Sandmaier, B. Reduced-intensity conditioning regimen workshop: Defining the dose spectrum. Report of a workshop convened by the center for international blood and marrow transplant research. Biol. Blood Marrow Transplant. 2009, 15, 367–369. [Google Scholar] [CrossRef] [Green Version]
- Gyurkocza, B.; Sandmaier, B.M. Conditioning regimens for hematopoietic cell transplantation: One size does not fit all. Blood 2014, 124, 344–353. [Google Scholar] [CrossRef]
- Schmid, C.; Schleuning, M.; Ledderose, G.; Tischer, J.; Kolb, H.J. Sequential regimen of chemotherapy, reduced-intensity conditioning for allogeneic stem-cell transplantation, and prophylactic donor lymphocyte transfusion in high-risk acute myeloid leukemia and myelodysplastic syndrome. J. Clin. Oncol. 2005, 23, 5675–5687. [Google Scholar] [CrossRef]
- Marks, R.; Potthoff, K.; Hahn, J.; Ihorst, G.; Bertz, H.; Spyridonidis, A.; Holler, E.; Finke, J.M. Reduced-toxicity conditioning with fludarabine, BCNU, and melphalan in allogeneic hematopoietic cell transplantation: Particular activity against advanced hematologic malignancies. Blood 2008, 112, 415–425. [Google Scholar] [CrossRef]
- Wais, V.; Kundgen, L.; Bohl, S.R.; von Harsdorf, S.; Schlenk, R.F.; Dohner, K.; Teleanu, V.; Bullinger, L.; Nguyen, T.M.; Drognitz, K.; et al. Reduced-toxicity conditioning for allogeneic hematopoietic cell transplantation in elderly or comorbid patients with AML using fludarabine, BCNU and melphalan: Disease stage at transplant determines outcome. Bone Marrow Transplant. 2018, 53, 94–96. [Google Scholar] [CrossRef] [Green Version]
- Spyridonidis, A.; Labopin, M.; Savani, B.N.; Niittyvuopio, R.; Blaise, D.; Craddock, C.; Socie, G.; Platzbecker, U.; Beelen, D.; Milpied, N.; et al. Redefining and measuring transplant conditioning intensity in current era: A study in acute myeloid leukemia patients. Bone Marrow Transplant. 2020, 55, 1114–1125. [Google Scholar] [CrossRef]
- Grimwade, D.; Hills, R.K.; Moorman, A.V.; Walker, H.; Chatters, S.; Goldstone, A.H.; Wheatley, K.; Harrison, C.J.; Burnett, A.K.; National Cancer Research Institute Adult Leukaemia Working Group. Refinement of cytogenetic classification in acute myeloid leukemia: Determination of prognostic significance of rare recurring chromosomal abnormalities among 5876 younger adult patients treated in the United Kingdom Medical Research Council trials. Blood 2010, 116, 354–365. [Google Scholar] [CrossRef] [Green Version]
- Eom, K.S.; Min, W.S.; Kim, H.J.; Cho, B.S.; Choi, S.M.; Lee, D.G.; Lee, S.; Min, C.K.; Kim, Y.J.; Cho, S.G.; et al. FLANG salvage chemotherapy is an effective regimen that offers a safe bridge to transplantation for patients with relapsed or refractory acute myeloid leukemia. Med. Oncol. 2011, 28 (Suppl. S1), S462–S470. [Google Scholar] [CrossRef]
- Ruggeri, A.; Sun, Y.; Labopin, M.; Bacigalupo, A.; Lorentino, F.; Arcese, W.; Santarone, S.; Gulbas, Z.; Blaise, D.; Messina, G.; et al. Post-transplant cyclophosphamide versus anti-thymocyte globulin as graft- versus-host disease prophylaxis in haploidentical transplant. Haematologica 2017, 102, 401–410. [Google Scholar] [CrossRef] [Green Version]
- Yoon, J.H.; Min, G.J.; Park, S.S.; Park, S.; Lee, S.E.; Cho, B.S.; Eom, K.S.; Kim, Y.J.; Kim, H.J.; Min, C.K.; et al. Impact of donor type on long-term graft-versus-host disease-free/relapse-free survival for adult acute lymphoblastic leukemia in first remission. Bone Marrow Transplant. 2021, 56, 828–840. [Google Scholar] [CrossRef]
- Rocha, V.; Mohty, M.; Gluckman, E.; Rio, B.; Eurocord; Reduced-Intensity Conditioning Subcommittee of the Acute Leukaemia Working Party; French Society of Bone Marrow Transplantation and Cellular Therapy. Reduced-intensity conditioning regimens before unrelated cord blood transplantation in adults with acute leukaemia and other haematological malignancies. Curr. Opin. Oncol. 2009, 21 (Suppl. S1), S31–S34. [Google Scholar] [CrossRef]
- Sheth, V.; Volt, F.; Sanz, J.; Clement, L.; Cornelissen, J.; Blaise, D.; Sierra, J.; Michallet, M.; Saccardi, R.; Rocha, V.; et al. Reduced-Intensity versus Myeloablative Conditioning in Cord Blood Transplantation for Acute Myeloid Leukemia (40–60 years) across Highly Mismatched HLA Barriers-On Behalf of Eurocord and the Cellular Therapy & Immunobiology Working Party (CTIWP) of EBMT. Biol. Blood Marrow Transplant. 2020, 26, 2098–2104. [Google Scholar] [CrossRef] [PubMed]
- Baron, F.; Ruggeri, A.; Beohou, E.; Labopin, M.; Sanz, G.; Milpied, N.; Michallet, M.; Bacigalupo, A.; Blaise, D.; Sierra, J.; et al. RIC versus MAC UCBT in adults with AML: A report from Eurocord, the ALWP and the CTIWP of the EBMT. Oncotarget 2016, 7, 43027–43038. [Google Scholar] [CrossRef] [Green Version]
- Brunstein, C.G.; Fuchs, E.J.; Carter, S.L.; Karanes, C.; Costa, L.J.; Wu, J.; Devine, S.M.; Wingard, J.R.; Aljitawi, O.S.; Cutler, C.S.; et al. Alternative donor transplantation after reduced intensity conditioning: Results of parallel phase 2 trials using partially HLA-mismatched related bone marrow or unrelated double umbilical cord blood grafts. Blood 2011, 118, 282–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuchs, E.J.; O’Donnell, P.V.; Eapen, M.; Logan, B.; Antin, J.H.; Dawson, P.; Devine, S.; Horowitz, M.M.; Horwitz, M.E.; Karanes, C.; et al. Double unrelated umbilical cord blood vs HLA-haploidentical bone marrow transplantation: The BMT CTN 1101 trial. Blood 2021, 137, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Kekre, N.; Antin, J.H. Cord blood versus haploidentical stem cell transplantation for hematological malignancies. Semin. Hematol. 2016, 53, 98–102. [Google Scholar] [CrossRef]
- Konuma, T.; Kanda, J.; Yamasaki, S.; Harada, K.; Shimomura, Y.; Terakura, S.; Mizuno, S.; Uchida, N.; Tanaka, M.; Doki, N.; et al. Single Cord Blood Transplantation Versus Unmanipulated Haploidentical Transplantation for Adults with Acute Myeloid Leukemia in Complete Remission. Transplant. Cell Ther. 2021, 27, 334.e1–334.e11. [Google Scholar] [CrossRef]
- Wu, R.; Ma, L. Haploidentical Hematopoietic Stem Cell Transplantation Versus Umbilical Cord Blood Transplantation in Hematologic Malignancies: A Systematic Review and Meta-Analysis. Cell Transplant. 2020, 29, 963689720964771. [Google Scholar] [CrossRef]
- Ruggeri, A.; Labopin, M.; Sanz, G.; Piemontese, S.; Arcese, W.; Bacigalupo, A.; Blaise, D.; Bosi, A.; Huang, H.; Karakasis, D.; et al. Comparison of outcomes after unrelated cord blood and unmanipulated haploidentical stem cell transplantation in adults with acute leukemia. Leukemia 2015, 29, 1891–1900. [Google Scholar] [CrossRef]
- Ruggeri, A.; Galimard, J.E.; Labopin, M.; Rafii, H.; Blaise, D.; Ciceri, F.; Diez-Martin, J.L.; Cornelissen, J.; Chevallier, P.; Sanchez-Guijo, F.; et al. Comparison of Outcomes after Unrelated Double-Unit Cord Blood and Haploidentical Peripheral Blood Stem Cell Transplantation in Adults with Acute Myelogenous Leukemia: A Study on Behalf of Eurocord and the Acute Leukemia Working Party of the European Society for Blood and Marrow Transplantation. Transplant. Cell Ther. 2022, 28, 710.e1–710.e10. [Google Scholar] [CrossRef]
- Yan, C.H.; Liu, D.H.; Liu, K.Y.; Xu, L.P.; Liu, Y.R.; Chen, H.; Han, W.; Wang, Y.; Qin, Y.Z.; Huang, X.J. Risk stratification-directed donor lymphocyte infusion could reduce relapse of standard-risk acute leukemia patients after allogeneic hematopoietic stem cell transplantation. Blood 2012, 119, 3256–3262. [Google Scholar] [CrossRef]
- Choi, I.; Yoon, S.R.; Park, S.Y.; Kim, H.; Jung, S.J.; Jang, Y.J.; Kang, M.; Yeom, Y.I.; Lee, J.L.; Kim, D.Y.; et al. Donor-derived natural killer cells infused after human leukocyte antigen-haploidentical hematopoietic cell transplantation: A dose-escalation study. Biol. Blood Marrow Transplant. 2014, 20, 696–704. [Google Scholar] [CrossRef]
- Kinoshita, H.; Cooke, K.R.; Grant, M.; Stanojevic, M.; Cruz, C.R.; Keller, M.; Fortiz, M.F.; Hoq, F.; Lang, H.; Barrett, A.J.; et al. Outcome of donor-derived TAA-T cell therapy in patients with high-risk or relapsed acute leukemia post allogeneic BMT. Blood Adv. 2022, 6, 2520–2534. [Google Scholar] [CrossRef]
- Xuan, L.; Liu, Q. Maintenance therapy in acute myeloid leukemia after allogeneic hematopoietic stem cell transplantation. J. Hematol. Oncol. 2021, 14, 4. [Google Scholar] [CrossRef]
- Cho, B.S.; Min, G.J.; Park, S.S.; Shin, S.H.; Yahng, S.A.; Jeon, Y.W.; Yoon, J.H.; Lee, S.E.; Eom, K.S.; Kim, Y.J.; et al. WT1 Measurable Residual Disease Assay in Patients with Acute Myeloid Leukemia Who Underwent Allogeneic Hematopoietic Stem Cell Transplantation: Optimal Time Points, Thresholds, and Candidates. Biol. Blood Marrow Transplant. 2019, 25, 1925–1932. [Google Scholar] [CrossRef]
- Cho, B.S.; Yahng, S.A.; Min, G.J.; Park, S.; Park, S.S.; Shin, S.H.; Jeon, Y.W.; Yoon, J.H.; Lee, S.E.; Eom, K.S.; et al. Comparable Outcomes After Alternative and Matched Sibling Donor Hematopoietic Stem Cell Transplantation and the Role of Molecular Measurable Residual Disease for Acute Myeloid Leukemia in Elderly Patients. Transplant. Cell Ther. 2021, 27, 774.e–774.e12. [Google Scholar] [CrossRef]
- Kayser, S.; Levis, M.J. Updates on targeted therapies for acute myeloid leukaemia. Br. J. Haematol. 2022, 196, 316–328. [Google Scholar] [CrossRef]
- Cheson, B.D.; Bennett, J.M.; Kopecky, K.J.; Buchner, T.; Willman, C.L.; Estey, E.H.; Schiffer, C.A.; Doehner, H.; Tallman, M.S.; Lister, T.A.; et al. Revised recommendations of the International Working Group for Diagnosis, Standardization of Response Criteria, Treatment Outcomes, and Reporting Standards for Therapeutic Trials in Acute Myeloid Leukemia. J. Clin. Oncol. 2003, 21, 4642–4649. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | HIT (N = 32), N (%) | dCBT (N = 20), N (%) | p Value | |
|---|---|---|---|---|
| AML MRC/treatment-related | 5 (16)/1 (3) | 5 (25)/0 (0) | 0.480 | |
| Age at SCT2, median (range) | 46.5 (23–67) | 49 (25–63) | 0.785 | |
| Male | 15 (47) | 13 (65) | 0.258 | |
| Hyperleukocytosis (≥50 × 109/L) at diagnosis Unavailable CBC at diagnosis | 4 (16) a 7 | 3 (17) a 5 | 1.000 | |
| Cytogenetics b | Favorable Intermediate Adverse | 4 (13) 25 (78) 3 (9) | 3 (15) 10 (50) 7 (35) | 0.053 |
| FLT3-ITD | Positive Negative Not available | 4 (13) 20 (63) 8 (25) | 3 (15) 14 (70) 3 (15) | 0.697 |
| Donor at SCT1 | Autologous Matched-related Matched-unrelated Haploidentical Cord blood | 13 (41) 11 (34) 7 (22) 0 (0) 1 (3) | 1 (5) 4 (20) 2 (10) 13 (65) 0 (0) | <0.001 |
| SCT1 Intensity | MAC RTC c RIC | 25 (78) 3 (9) 4 (13) | 5 (25) 12 (60) 3 (15) | <0.001 |
| Remission duration after SCT1 ≥9 months | 24 (75) | 14 (70) | 0.754 | |
| Salvage therapy | Intensive FLANG d FLAG-Ida e MEC f IA g Non-intensive Venetoclax-based Sorafenib-based With DLI | 30 (94) 22 (69) 1 (3) 4 (13) 3 (9) 2 (6) 1 (3) 1 (3) 2 (6) | 18 (90) 14 (70) 0 (0) 2 (10) 1 (5) 2 (10) 2 (10) 0 (0) 0 (0) | 0.6340.517 |
| Complete remission before SCT2 | 25 (78) | 17 (85) | 0.722 | |
| WT1 PCR (/104 ABL) before SCT2 CR, ≥250 (MRD-positive) CR, <250 (MRD-negative) CR, but data unavailable Non-CR | 5 (16) 18 (56) 2 (6) 7 (22) | 3 (15) 13 (65) 1 (5) 3 (15) | 0.960 | |
| HCT-CI | 0 1–2 ≥3 | 5 (16) 12 (38) 15 (47) | 5 (25) 3 (15) 12 (60) | 0.207 |
| Donor sex | Match Partial mismatch Full mismatch | 16 (50) - 16 (50) | 3 (15) 12 (60) 5 (25) | |
| Donor HLA match (of eight loci, the lower value in dCBT) | 4 5 6 ≥7 | 11 (34) 16 (50) 5 (16) 0 (0) | 3 (15) 7 (35) 6 (30) 4 (20) | <0.001 |
| Total nucleated cells, median (range), 108/kg | 20.5 (8.7–40.3) | 0.39 (0.18–0.71) | <0.001 | |
| CD34, median (range), 106/kg | 7.44 (1.77–28.96) | 0.07 (0.03–0.32) | <0.001 | |
| Time between SCT1 and SCT2, median months (range) | 17.2 (6.6–142.0) | 15.7 (6.6–82.0) | 0.333 | |
| Time between relapse and SCT2, median months (range) | 3.7 (2.8–7.9) | 3.7 (2.8–7.1) | 0.631 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.-H.; Cho, B.-S.; Kwag, D.; Min, G.-J.; Park, S.-S.; Park, S.; Yoon, J.-H.; Lee, S.-E.; Eom, K.-S.; Kim, Y.-J.; et al. Haploidentical versus Double-Cord Blood Stem Cells as a Second Transplantation for Relapsed Acute Myeloid Leukemia. Cancers 2023, 15, 454. https://doi.org/10.3390/cancers15020454
Lee J-H, Cho B-S, Kwag D, Min G-J, Park S-S, Park S, Yoon J-H, Lee S-E, Eom K-S, Kim Y-J, et al. Haploidentical versus Double-Cord Blood Stem Cells as a Second Transplantation for Relapsed Acute Myeloid Leukemia. Cancers. 2023; 15(2):454. https://doi.org/10.3390/cancers15020454
Chicago/Turabian StyleLee, Jong-Hyuk, Byung-Sik Cho, Daehun Kwag, Gi-June Min, Sung-Soo Park, Silvia Park, Jae-Ho Yoon, Sung-Eun Lee, Ki-Seong Eom, Yoo-Jin Kim, and et al. 2023. "Haploidentical versus Double-Cord Blood Stem Cells as a Second Transplantation for Relapsed Acute Myeloid Leukemia" Cancers 15, no. 2: 454. https://doi.org/10.3390/cancers15020454
APA StyleLee, J. -H., Cho, B. -S., Kwag, D., Min, G. -J., Park, S. -S., Park, S., Yoon, J. -H., Lee, S. -E., Eom, K. -S., Kim, Y. -J., Lee, S., Min, C. -K., Cho, S. -G., Lee, J. -W., & Kim, H. -J. (2023). Haploidentical versus Double-Cord Blood Stem Cells as a Second Transplantation for Relapsed Acute Myeloid Leukemia. Cancers, 15(2), 454. https://doi.org/10.3390/cancers15020454