
Relative Risk of Bladder and Kidney Cancer in Lynch Syndrome: Systematic Review and Meta-Analysis

 , , and
, , and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction
2.4. Quality Assessment of Included Studies
2.5. Meta Analysis
2.6. Assessment of Quality of Evidence
3. Results
3.1. Study Selection
3.2. Study Characteristics
4. Risk of Bias
5. Evidence Synthesis
5.1. Bladder Cancer
5.2. Kidney Cancer
6. Discussion
6.1. Bladder Cancer
6.2. Kidney Cancer
6.3. Upper Tract Urothelial Carcinoma
6.4. Screening Tools in Clinical Practice for Patients with Lynch Syndrome
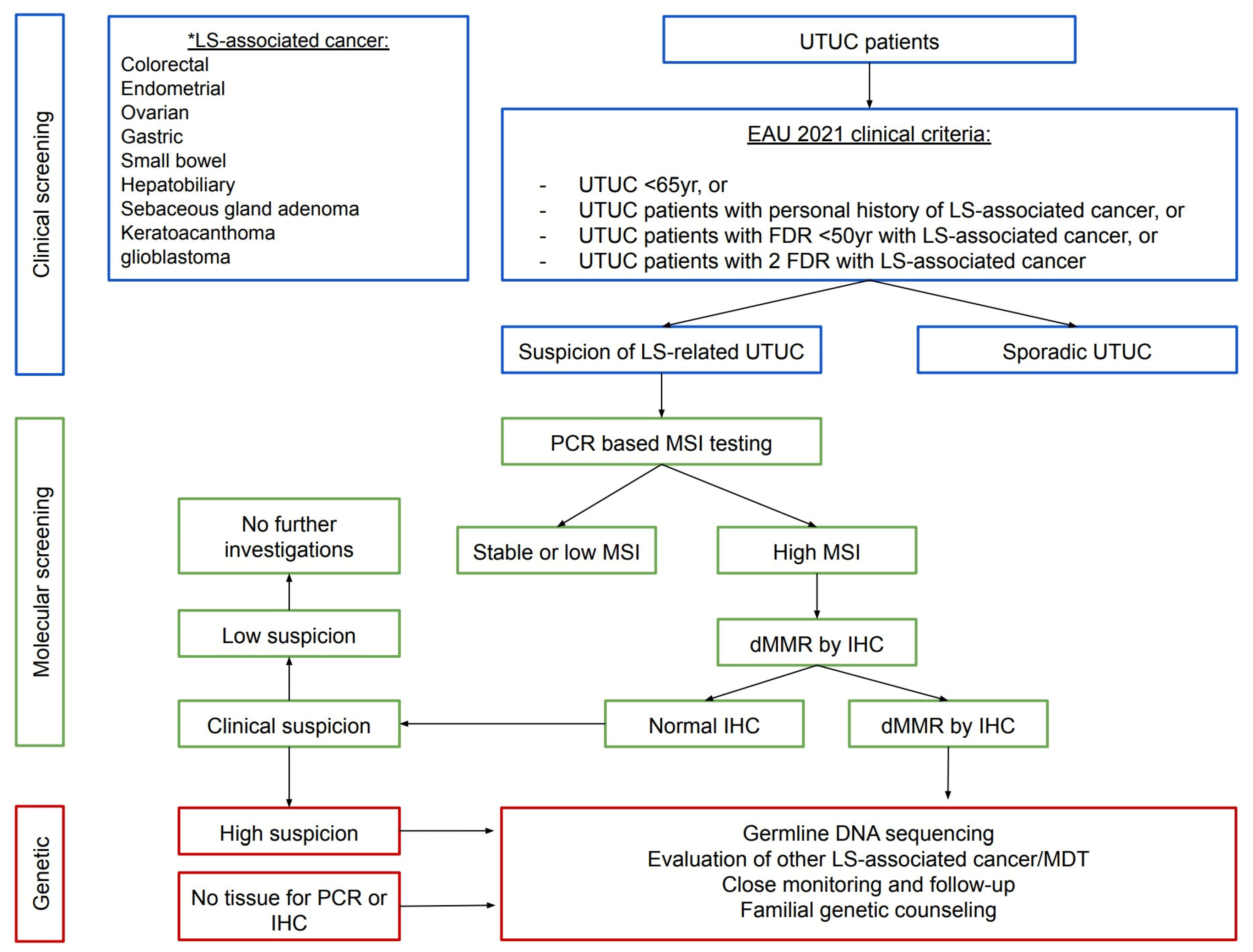
6.5. Screening Protocols in Clinical Practice for LS-Associated UTUC
- Before age 60 years;
- Possess a family history of UTUC, CRC, or endometrial cancer before age 60 years;
- Possess a personal history of colorectal or endometrial cancer.
- Under 65 years of age;
- UTUC individuals with a personal history of cases on the LS tumour spectrum;
- UTUC individuals with one FDR, under 50 years of age, with LS-related cancer;
- UTUC individuals with two FDRs with LS-related cancer, regardless of age.



6.6. Limitations
7. Implications for Practice and Future Research
8. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Lonati, C.; Simeone, C.; Suardi, N.; Spiess, P.E.; Necchi, A.; Moschini, M. Genitourinary manifestations of Lynch syndrome in the urological practice. Asian J. Urol. 2022, 9, 443–450. [Google Scholar] [CrossRef]
- Modrich, P. Mechanisms in eukaryotic mismatch repair. J. Biol. Chem. 2006, 281, 30305–30309. [Google Scholar] [CrossRef] [Green Version]
- Li, K.; Luo, H.; Huang, L.; Luo, H.; Zhu, X. Microsatellite instability: A review of what the oncologist should know. Cancer Cell Int. 2020, 20, 16. [Google Scholar] [CrossRef] [Green Version]
- Wischhusen, J.W.; Ukaegbu, C.; Dhingra, T.G.; Uno, H.; Kastrinos, F.; Syngal, S.; Yurgelun, M.B. Clinical Factors Associated with Urinary Tract Cancer in Individuals with Lynch Syndrome. Cancer Epidemiol. Biomark. Prev. 2020, 29, 193–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vasen, H.F.; Watson, P.; Mecklin, J.P.; Lynch, H.T. New clinical criteria for hereditary nonpolyposis colorectal cancer (HNPCC, Lynch syndrome) proposed by the International Collaborative group on HNPCC. Gastroenterology 1999, 116, 1453–1456. [Google Scholar] [CrossRef]
- Hubosky, S.G.; Boman, B.M.; Charles, S.; Bibbo, M.; Bagley, D.H. Ureteroscopic management of upper tract urothelial carcinoma (UTUC) in patients with Lynch Syndrome (hereditary nonpolyposis colorectal cancer syndrome). BJU Int. 2013, 112, 813–819. [Google Scholar] [CrossRef]
- Mork, M.; Hubosky, S.G.; Rouprêt, M.; Margulis, V.; Raman, J.; Lotan, Y.; O’Brien, T.; You, N.; Shariat, S.F.; Matin, S.F. Lynch Syndrome: A Primer for Urologists and Panel Recommendations. J. Urol. 2015, 194, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Joost, P.; Therkildsen, C.; Dominguez-Valentin, M.; Jönsson, M.; Nilbert, M. Urinary Tract Cancer in Lynch Syndrome; Increased Risk in Carriers of MSH2 Mutations. Urology 2015, 86, 1212–1217. [Google Scholar] [CrossRef] [PubMed]
- Geary, J.; Sasieni, P.; Houlston, R.; Izatt, L.; Eeles, R.; Payne, S.J.; Fisher, S.; Hodgson, S.V. Gene-related cancer spectrum in families with hereditary non-polyposis colorectal cancer (HNPCC). Fam. Cancer 2008, 7, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Barrow, P.J.; Ingham, S.; O’Hara, C.; Green, K.; McIntyre, I.; Lalloo, F.; Hill, J.; Evans, D.G. The spectrum of urological malignancy in Lynch syndrome. Fam. Cancer 2013, 12, 57–63. [Google Scholar] [CrossRef]
- Skeldon, S.C.; Semotiuk, K.; Aronson, M.; Holter, S.; Gallinger, S.; Pollett, A.; Kuk, C.; van Rhijn, B.; Bostrom, P.; Cohen, Z.; et al. Patients with Lynch syndrome mismatch repair gene mutations are at higher risk for not only upper tract urothelial cancer but also bladder cancer. Eur. Urol. 2013, 63, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Ryan, S.; Jenkins, M.A.; Win, A.K. Risk of prostate cancer in Lynch syndrome: A systematic review and meta-analysis. Cancer Epidemiol. Biomark. Prev. 2014, 23, 437–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (Updated February 2022). Cochrane (Chichester, UK). 2022. Available online: www.training.cochrane.org/handbook (accessed on 8 December 2022).
- Cochran, W.G. Tool to Assess Risk of Bias in Cohort Studies. Available online: http://methods.cochrane.org/sites/methods.cochrane.org.bias/files/uploads/Tool%20to%20Assess%20Risk%20of%20Bias%20in%20Cohort%20Studies.pdf (accessed on 8 December 2022).
- Cochran, W.G. The Comparison of Percentages in Matched Samples. Biometrika 1950, 37, 256–266. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H.; et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Glasziou, P.; Jaeschke, R.; Akl, E.A.; et al. GRADE guidelines: 7. Rating the quality of evidence-inconsistency. J. Clin. Epidemiol. 2011, 64, 1294–1302. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Rind, D.; Devereaux, P.J.; Montori, V.M.; Freyschuss, B.; Vist, G.; et al. GRADE guidelines 6. Rating the quality of evidence-imprecision. J. Clin. Epidemiol. 2011, 64, 1283–1293. [Google Scholar] [CrossRef]
- Balshem, H.; Helfand, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S.; et al. GRADE guidelines: 3. Rating the quality of evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef]
- Aarnio, M.; Sankila, R.; Pukkala, E.; Salovaara, R.; Aaltonen, L.A.; de la Chapelle, A.; Peltomäki, P.; Mecklin, J.P.; Järvinen, H.J. Cancer risk in mutation carriers of DNA-mismatch-repair genes. Int. J. Cancer 1999, 81, 214–218. [Google Scholar] [CrossRef]
- Pande, M.; Wei, C.; Chen, J.; Amos, C.I.; Lynch, P.M.; Lu, K.H.; Lucio, L.A.; Boyd-Rogers, S.G.; Bannon, S.A.; Mork, M.E.; et al. Cancer spectrum in DNA mismatch repair gene mutation carriers: Results from a hospital based Lynch syndrome registry. Fam. Cancer 2012, 11, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Engel, C.; Loeffler, M.; Steinke, V.; Rahner, N.; Holinski-Feder, E.; Dietmaier, W.; Schackert, H.K.; Goergens, H.; von Knebel Doeberitz, M.; Goecke, T.O.; et al. Risks of less common cancers in proven mutation carriers with lynch syndrome. J. Clin. Oncol. 2012, 30, 4409–4415. [Google Scholar] [CrossRef] [PubMed]
- Win, A.K.; Young, J.P.; Lindor, N.M.; Tucker, K.M.; Ahnen, D.J.; Young, G.P.; Buchanan, D.D.; Clendenning, M.; Giles, G.G.; Winship, I.; et al. Colorectal and other cancer risks for carriers and noncarriers from families with a DNA mismatch repair gene mutation: A prospective cohort study. J. Clin. Oncol. 2012, 30, 958–964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Metcalfe, M.J.; Petros, F.G.; Rao, P.; Mork, M.E.; Xiao, L.; Broaddus, R.R.; Matin, S.F. Universal Point of Care Testing for Lynch Syndrome in Patients with Upper Tract Urothelial Carcinoma. J. Urol. 2018, 199, 60–65. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef]
- Lonati, C.; Necchi, A.; Gómez Rivas, J.; Afferi, L.; Laukhtina, E.; Martini, A.; Ventimiglia, E.; Colombo, R.; Gandaglia, G.; Salonia, A.; et al. Upper Tract Urothelial Carcinoma in the Lynch Syndrome Tumour Spectrum: A Comprehensive Overview from the European Association of Urology—Young Academic Urologists and the Global Society of Rare Genitourinary Tumors. Eur. Urol. Oncol. 2022, 5, 30–41. [Google Scholar] [CrossRef]
- Weiss, J.M.; Gupta, S.; Burke, C.A.; Axell, L.; Chen, L.M.; Chung, D.C.; Clayback, K.M.; Dallas, S.; Felder, S.; Gbolahan, O.; et al. NCCN Guidelines® Insights: Genetic/Familial High-Risk Assessment: Colorectal, Version 1.2021. J. Natl. Compr. Cancer Netw. 2021, 19, 1122–1132. [Google Scholar] [CrossRef]
- Møller, P.; Seppälä, T.T.; Bernstein, I.; Holinski-Feder, E.; Sala, P.; Gareth Evans, D.; Lindblom, A.; Macrae, F.; Blanco, I.; Sijmons, R.H.; et al. Cancer risk and survival in path_MMR carriers by gene and gender up to 75 years of age: A report from the Prospective Lynch Syndrome Database. Gut 2018, 67, 1306–1316. [Google Scholar] [CrossRef] [Green Version]
- Samadder, N.J.; Smith, K.R.; Wong, J.; Thomas, A.; Hanson, H.; Boucher, K.; Kopituch, C.; Cannon-Albright, L.A.; Burt, R.W.; Curtin, K. Cancer Risk in Families Fulfilling the Amsterdam Criteria for Lynch Syndrome. JAMA Oncol. 2017, 3, 1697–1701. [Google Scholar] [CrossRef]
- Aarnio, M.; Säily, M.; Juhola, M.; Gylling, A.; Peltomäki, P.; Järvinen, H.J.; Mecklin, J.P. Uroepithelial and kidney carcinoma in Lynch syndrome. Fam. Cancer 2012, 11, 395–401. [Google Scholar] [CrossRef]
- Latham, A.; Srinivasan, P.; Kemel, Y.; Shia, J.; Bandlamudi, C.; Mandelker, D.; Middha, S.; Hechtman, J.; Zehir, A.; Dubard-Gault, M.; et al. Microsatellite Instability Is Associated With the Presence of Lynch Syndrome Pan-Cancer. J. Clin. Oncol. 2019, 37, 286–295. [Google Scholar] [CrossRef]
- Donahu, T.F.; Bagrodia, A.; Audenet, F.; Donoghue, M.T.A.; Cha, E.K.; Sfakianos, J.P.; Sperling, D.; Al-Ahmadie, H.; Clendenning, M.; Rosty, C.; et al. Genomic Characterization of Upper-Tract Urothelial Carcinoma in Patients With Lynch Syndrome. JCO Precis. Oncol. 2018, 2018, 17. [Google Scholar] [CrossRef]
- Watson, P.; Vasen, H.F.A.; Mecklin, J.P.; Bernstein, I.; Aarnio, M.; Järvinen, H.J.; Myrhøj, T.; Sunde, L.; Wijnen, J.T.; Lynch, H.T. The risk of extra-colonic, extra-endometrial cancer in the Lynch syndrome. Int. J. Cancer 2008, 123, 444–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sijmons, R.H.; Kiemeney, L.A.; Witjes, J.A.; Vasen, H.F. Urinary tract cancer and hereditary nonpolyposis colorectal cancer: Risks and screening options. J. Urol. 1998, 160, 466–470. [Google Scholar] [CrossRef] [PubMed]
- Rouprêt, M.; Babjuk, M.; Burger, M.; Capoun, O.; Cohen, D.; Compérat, E.M.; Cowan, N.C.; Dominguez-Escrig, J.L.; Gontero, P.; Hugh Mostafid, A.; et al. European Association of Urology Guidelines on Upper Urinary Tract Urothelial Carcinoma: 2020 Update. Eur. Urol. 2021, 79, 62–79. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, A.; Zanardo, L.; Bocker-Edmonston, T.; Blaszyk, H.; Dietmaier, W.; Stoehr, R.; Cheville, J.C.; Junker, K.; Wieland, W.; Knuechel, R.; et al. Frequent microsatellite instability in sporadic tumors of the upper urinary tract. Cancer Res. 2002, 62, 6796–6802. [Google Scholar] [PubMed]
- Urakami, S.; Inoshita, N.; Oka, S.; Miyama, Y.; Nomura, S.; Arai, M.; Sakaguchi, K.; Kurosawa, K.; Okaneya, T. Clinicopathological characteristics of patients with upper urinary tract urothelial cancer with loss of immunohistochemical expression of the DNA mismatch repair proteins in universal screening. Int. J. Urol. 2018, 25, 151–156. [Google Scholar] [CrossRef] [Green Version]
- Crockett, D.G.; Wagner, D.G.; Holmäng, S.; Johansson, S.L.; Lynch, H.T. Upper urinary tract carcinoma in Lynch syndrome cases. J. Urol. 2011, 185, 1627–1630. [Google Scholar] [CrossRef]
- Bai, S.; Nunez, A.L.; Wei, S.; Ziober, A.; Yao, Y.; Tomaszewski, J.E.; Bing, Z. Microsatellite instability and TARBP2 mutation study in upper urinary tract urothelial carcinoma. Am. J. Clin. Pathol. 2013, 139, 765–770. [Google Scholar] [CrossRef] [Green Version]
- Therkildsen, C.; Eriksson, P.; Höglund, M.; Jönsson, M.; Sjödahl, G.; Nilbert, M.; Liedberg, F. Molecular subtype classification of urothelial carcinoma in Lynch syndrome. Mol. Oncol. 2018, 12, 1286–1295. [Google Scholar] [CrossRef]
- Chen, S.; Wang, W.; Lee, S.; Nafa, K.; Lee, J.; Romans, K.; Watson, P.; Gruber, S.B.; Euhus, D.; Kinzler, K.W.; et al. Prediction of germline mutations and cancer risk in the Lynch syndrome. JAMA 2006, 296, 1479–1487. [Google Scholar] [CrossRef] [Green Version]
- Lynch, H.T.; Boland, C.R.; Rodriguez-Bigas, M.A.; Amos, C.; Lynch, J.F.; Lynch, P.M. Who should be sent for genetic testing in hereditary colorectal cancer syndromes? J. Clin. Oncol. 2007, 25, 3534–3542. [Google Scholar] [CrossRef]
- Goldberg, H.; Wallis, C.J.D.; Klaassen, Z.; Chandrasekar, T.; Fleshner, N.; Zlotta, A.R. Lynch Syndrome in Urologic Malignancies—What Does the Urologist Need to Know? Urology 2019, 134, 24–31. [Google Scholar] [CrossRef]
- Boland, C.R.; Lynch, H.T. The history of Lynch syndrome. Fam. Cancer 2013, 12, 145–157. [Google Scholar] [CrossRef] [Green Version]
- Yurgelun, M.B.; Hampel, H. Recent Advances in Lynch Syndrome: Diagnosis, Treatment, and Cancer Prevention. Am. Soc. Clin. Oncol. Educ. Book 2018, 38, 101–109. [Google Scholar] [CrossRef]
- Palomaki, G.E.; McClain, M.R.; Melillo, S.; Hampel, H.L.; Thibodeau, S.N. EGAPP supplementary evidence review: DNA testing strategies aimed at reducing morbidity and mortality from Lynch syndrome. Genet. Med. 2009, 11, 42–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasmussen, M.; Madsen, M.G.; Therkildsen, C. Immunohistochemical Screening of Upper Tract Urothelial Carcinomas for Lynch Syndrome Diagnostics: A Systematic Review. Urology 2022, 165, 44–53. [Google Scholar] [CrossRef]
- Järvinen, H.J.; Aarnio, M.; Mustonen, H.; Aktan–Collan, K.; Aaltonen, L.A.; Peltomäki, P.; Chapelle, A.D.L.; Mecklin, J.P. Controlled 15-year trial on screening for colorectal cancer in families with hereditary nonpolyposis colorectal cancer. Gastroenterology 2000, 118, 829–834. [Google Scholar] [CrossRef] [PubMed]
- De Jong, A.E.; Hendriks, Y.M.C.; Kleibeuker, J.H.; de Boer, S.Y.; Cats, A.; Griffioen, G.; Nagengast, F.M.; Nelis, F.G.; Rookus, M.A.; Vasen, H.F.A. Decrease in Mortality in Lynch Syndrome Families Because of Surveillance. Gastroenterology 2006, 130, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Shia, J.; Ellis, N.A.; Klimstra, D.S. The utility of immunohistochemical detection of DNA mismatch repair gene proteins. Virchows Arch. 2004, 445, 431–441. [Google Scholar] [CrossRef] [PubMed]
- Shia, J.; Klimstra, D.S.; Nafa, K.; Offit, K.; Guillem, J.G.; Markowitz, A.J.; Gerald, W.L.; Ellis, N.A. Value of immunohistochemical detection of DNA mismatch repair proteins in predicting germline mutation in hereditary colorectal neoplasms. Am. J. Surg. Pathol. 2005, 29, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Cicek, M.S.; Lindor, N.M.; Gallinger, S.; Bapat, B.; Hopper, J.L.; Jenkins, M.A.; Young, J.; Buchanan, D.; Walsh, M.D.; Le Marchand, L. Quality assessment and correlation of microsatellite instability and immunohistochemical markers among population-And clinic-based colorectal tumors: Results from the colon cancer family registry. J. Mol. Diagn. 2011, 13, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Yu, F.; Makrigiorgos, A.; Leong, K.W.; Makrigiorgos, G.M. Sensitive detection of microsatellite instability in tissues and liquid biopsies: Recent developments and updates. Comput. Struct. Biotechnol. J. 2021, 19, 4931–4940. [Google Scholar] [CrossRef] [PubMed]
- Rouprêt, M.; Yates, D.R.; Comperat, E.; Cussenot, O. Upper urinary tract urothelial cell carcinomas and other urological malignancies involved in the hereditary nonpolyposis colorectal cancer (lynch syndrome) tumor spectrum. Eur. Urol. 2008, 54, 1226–1236. [Google Scholar] [CrossRef]
- Therkildsen, C.; Jensen, L.H.; Rasmussen, M.; Bernstein, I. An Update on Immune Checkpoint Therapy for the Treatment of Lynch Syndrome. Clin. Exp. Gastroenterol. 2021, 14, 181–197. [Google Scholar] [CrossRef]
- Stelloo, E.; Jansen, A.M.L.; Osse, E.M.; Nout, R.A.; Creutzberg, C.L.; Ruano, D.; Church, D.N.; Morreau, H.; Smit, V.; van Wezel, T.; et al. Practical guidance for mismatch repair-deficiency testing in endometrial cancer. Ann. Oncol. 2017, 28, 96–102. [Google Scholar] [CrossRef]
- Loughrey, M.B.; McGrath, J.; Coleman, H.G.; Bankhead, P.; Maxwell, P.; McGready, C.; Bingham, V.; Humphries, M.P.; Craig, S.G.; McQuaid, S.; et al. Identifying mismatch repair-deficient colon cancer: Near-perfect concordance between immunohistochemistry and microsatellite instability testing in a large, population-based series. Histopathology 2021, 78, 401–413. [Google Scholar] [CrossRef]
- Roupret, M.; Catto, J.; Coulet, F.; Azzouzi, A.-R.; Amira, N.; Karmouni, T.; Fromont, G.; Sibony, M.; Vallancien, G.; Gattegno, B.; et al. Microsatellite instability as indicator of MSH2 gene mutation in patients with upper urinary tract transitional cell carcinoma. J. Med. Genet. 2004, 41, e91. [Google Scholar] [CrossRef] [Green Version]
- Rouprêt, M.; Azzouzi, A.R.; Cussenot, O. Microsatellite instability and transitional cell carcinoma of the upper urinary tract. BJU Int. 2005, 96, 489–492. [Google Scholar] [CrossRef]
- Vasen, H.F.; Blanco, I.; Aktan-Collan, K.; Gopie, J.P.; Alonso, A.; Aretz, S.; Bernstein, I.; Bertario, L.; Burn, J.; Capella, G.; et al. Revised guidelines for the clinical management of Lynch syndrome (HNPCC): Recommendations by a group of European experts. Gut 2013, 62, 812–823. [Google Scholar] [CrossRef]
- Snowsill, T.; Coelho, H.; Huxley, N.; Jones-Hughes, T.; Briscoe, S.; Frayling, I.M.; Hyde, C. Molecular testing for Lynch syndrome in people with colorectal cancer: Systematic reviews and economic evaluation. Health Technol. Assess. 2017, 21, 1–238. [Google Scholar] [CrossRef] [Green Version]
- Pradere, B.; Lotan, Y.; Roupret, M. Lynch syndrome in upper tract urothelial carcinoma: Significance, screening, and surveillance. Curr. Opin. Urol. 2017, 27, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Ladabaum, U.; Wang, G.; Terdiman, J.; Blanco, A.; Kuppermann, M.; Boland, C.R.; Ford, J.; Elkin, E.; Phillips, K.A. Strategies to identify the Lynch syndrome among patients with colorectal cancer: A cost-effectiveness analysis. Ann. Intern. Med. 2011, 155, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Bacher, J.W.; Flanagan, L.A.; Smalley, R.L.; Nassif, N.A.; Burgart, L.J.; Halberg, R.B.; Megid, W.M.A.; Thibodeau, S.N. Development of a fluorescent multiplex assay for detection of MSI-High tumors. Dis. Markers 2004, 20, 237–250. [Google Scholar] [CrossRef] [Green Version]
- Berg, K.D.; Glaser, C.L.; Thompson, R.E.; Hamilton, S.R.; Griffin, C.A.; Eshleman, J.R. Detection of microsatellite instability by fluorescence multiplex polymerase chain reaction. J. Mol. Diagn. 2000, 2, 20–28. [Google Scholar] [CrossRef] [Green Version]
- Wang, F.; Wang, L.; Briggs, C.; Sicinska, E.; Gaston, S.M.; Mamon, H.; Kulke, M.H.; Zamponi, R.; Loda, M.; Maher, E. DNA degradation test predicts success in whole-genome amplification from diverse clinical samples. J. Mol. Diagn. 2007, 9, 441–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baudrin, L.G.; Duval, A.; Daunay, A.; Buhard, O.; Bui, H.; Deleuze, J.-F.; How-Kit, A. Improved microsatellite instability detection and identification by nuclease-assisted microsatellite instability enrichment using HSP110 T17. Clin. Chem. 2018, 64, 1252–1253. [Google Scholar] [CrossRef] [Green Version]
- Silveira, A.B.; Bidard, F.-C.; Kasperek, A.; Melaabi, S.; Tanguy, M.-L.; Rodrigues, M.; Bataillon, G.; Cabel, L.; Buecher, B.; Pierga, J.-Y. High-accuracy determination of microsatellite instability compatible with liquid biopsies. Clin. Chem. 2020, 66, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Gilson, P.; Levy, J.; Rouyer, M.; Demange, J.; Husson, M.; Bonnet, C.; Salleron, J.; Leroux, A.; Merlin, J.-L.; Harlé, A. Evaluation of 3 molecular-based assays for microsatellite instability detection in formalin-fixed tissues of patients with endometrial and colorectal cancers. Sci. Rep. 2020, 10, 16386. [Google Scholar] [CrossRef] [PubMed]
- Trabucco, S.E.; Gowen, K.; Maund, S.L.; Sanford, E.; Fabrizio, D.A.; Hall, M.J.; Yakirevich, E.; Gregg, J.P.; Stephens, P.J.; Frampton, G.M. A novel next-generation sequencing approach to detecting microsatellite instability and pan-tumor characterization of 1000 microsatellite instability–high cases in 67,000 patient samples. J. Mol. Diagn. 2019, 21, 1053–1066. [Google Scholar] [CrossRef]
- Yu, F.; Leong, K.W.; Makrigiorgos, A.; Adalsteinsson, V.A.; Ladas, I.; Ng, K.; Mamon, H.; Makrigiorgos, G.M. NGS-based identification and tracing of microsatellite instability from minute amounts DNA using inter-Alu-PCR. Nucleic Acids Res. 2021, 49, e24. [Google Scholar] [CrossRef] [PubMed]
- Willis, J.; Lefterova, M.I.; Artyomenko, A.; Kasi, P.M.; Nakamura, Y.; Mody, K.; Catenacci, D.V.; Fakih, M.; Barbacioru, C.; Zhao, J. Validation of Microsatellite Instability Detection Using a Comprehensive Plasma-Based Genotyping PanelValidation of Plasma-Based MSI Detection. Clin. Cancer Res. 2019, 25, 7035–7045. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Zhang, S.; Zhou, D.C.; Wang, D.; He, X.; Yuan, D.; Li, R.; He, J.; Duan, X.; Wendl, M.C. MSIsensor-ct: Microsatellite instability detection using cfDNA sequencing data. Brief. Bioinform. 2021, 22, bbaa402. [Google Scholar] [CrossRef]
- Schrock, A.; Ouyang, C.; Sandhu, J.; Sokol, E.; Jin, D.; Ross, J.; Miller, V.; Lim, D.; Amanam, I.; Chao, J. Tumor mutational burden is predictive of response to immune checkpoint inhibitors in MSI-high metastatic colorectal cancer. Ann. Oncol. 2019, 30, 1096–1103. [Google Scholar] [CrossRef]
- Goodman, A.M.; Sokol, E.S.; Frampton, G.M.; Lippman, S.M.; Kurzrock, R. Microsatellite-Stable Tumors with High Mutational Burden Benefit from ImmunotherapyMicrosatellite-Stable Tumors with High TMB. Cancer Immunol. Res. 2019, 7, 1570–1573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Audenet, F.; Isharwal, S.; Cha, E.K.; Donoghue, M.T.A.; Drill, E.N.; Ostrovnaya, I.; Pietzak, E.J.; Sfakianos, J.P.; Bagrodia, A.; Murugan, P.; et al. Clonal Relatedness and Mutational Differences between Upper Tract and Bladder Urothelial Carcinoma. Clin. Cancer Res. 2019, 25, 967–976. [Google Scholar] [CrossRef] [Green Version]
- Robinson, B.D.; Vlachostergios, P.J.; Bhinder, B.; Liu, W.; Li, K.; Moss, T.J.; Bareja, R.; Park, K.; Tavassoli, P.; Cyrta, J.; et al. Upper tract urothelial carcinoma has a luminal-papillary T-cell depleted contexture and activated FGFR3 signaling. Nat. Commun. 2019, 10, 2977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niu, B.; Ye, K.; Zhang, Q.; Lu, C.; Xie, M.; McLellan, M.D.; Wendl, M.C.; Ding, L. MSIsensor: Microsatellite instability detection using paired tumor-normal sequence data. Bioinformatics 2014, 30, 1015–1016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindor, N.M.; Petersen, G.M.; Hadley, D.W.; Kinney, A.Y.; Miesfeldt, S.; Lu, K.H.; Lynch, P.; Burke, W.; Press, N. Recommendations for the care of individuals with an inherited predisposition to Lynch syndrome: A systematic review. JAMA 2006, 296, 1507–1517. [Google Scholar] [CrossRef]
- Acher, P.; Kiela, G.; Thomas, K.; O’Brien, T. Towards a rational strategy for the surveillance of patients with Lynch syndrome (hereditary non-polyposis colon cancer) for upper tract transitional cell carcinoma. BJU Int. 2010, 106, 300–302. [Google Scholar] [CrossRef]
- Zachhau, P.; Walter, S. Urinary tract cancer in patients with hereditary non-polyposis colorectal cancer. Scand. J. Urol. Nephrol. 2012, 46, 5–7. [Google Scholar] [CrossRef] [PubMed]
- Koornstra, J.J.; Mourits, M.J.; Sijmons, R.H.; Leliveld, A.M.; Hollema, H.; Kleibeuker, J.H. Management of extracolonic tumours in patients with Lynch syndrome. Lancet Oncol. 2009, 10, 400–408. [Google Scholar] [CrossRef]
- Myrhøj, T.; Andersen, M.B.; Bernstein, I. Screening for urinary tract cancer with urine cytology in Lynch syndrome and familial colorectal cancer. Fam. Cancer 2008, 7, 303–307. [Google Scholar] [CrossRef]
- Loo, R.K.; Lieberman, S.F.; Slezak, J.M.; Landa, H.M.; Mariani, A.J.; Nicolaisen, G.; Aspera, A.M.; Jacobsen, S.J. Stratifying risk of urinary tract malignant tumors in patients with asymptomatic microscopic hematuria. Mayo Clin. Proc. 2013, 88, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Grégoire, G.; Derderian, F.; Le Lorier, J. Selecting the language of the publications included in a meta-analysis: Is there a Tower of Babel bias? J. Clin. Epidemiol. 1995, 48, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, H.; Imai, K. Microsatellite instability: An update. Arch. Toxicol. 2015, 89, 899–921. [Google Scholar] [CrossRef]
- Valo, S.; Kaur, S.; Ristimäki, A.; Renkonen-Sinisalo, L.; Järvinen, H.; Mecklin, J.-P.; Nyström, M.; Peltomäki, P. DNA hypermethylation appears early and shows increased frequency with dysplasia in Lynch syndrome-associated colorectal adenomas and carcinomas. Clin. Epigenet. 2015, 7, 71. [Google Scholar] [CrossRef]
- Nieminen, T.T.; Niskakoski, A.; Peltomäki, P. Epigenetic Mechanisms in Lynch Syndrome. In Encyclopedia of Life Sciences; eLS: London, UK; pp. 1–9.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria |
|---|
|
|
|
|
| Exclusion criteria |
|
|
|
|
|
| Author (Year) | Study Design | Country | Registry/Database | Sample Size (Confirmed MMR Carriers Only) | Male | Mean Age at Diagnosis (Any Cancer) | Ethnicity | Results (SIR (95% CI), p-Value) |
|---|---|---|---|---|---|---|---|---|
| Aarnio et al. (1999) [22] | Retrospective—Cohort | Finland | Finnish cancer registry | 360 | Not reported | Not reported | Caucasian (100%) | Increased risk of RCC cancer (4.7 (1.0, 14.0), p < 0.005) |
| Pande et al. (2012) [23] | Retrospective—Cohort | USA | MD Anderson cancer centre database | 368 | 151 | 41.2 (SD 10.6) | Caucasian 84% | Increased risk of bladder cancer (10.6 (2.9, 27.2), p < 0.05) |
| African American 7% | ||||||||
| Hispanic 7% | ||||||||
| Other 2% | ||||||||
| Engel et al. (2012) [24] | Retrospective—Cohort | Germany and the Netherlands | German HNPCC consortium and the Netherlands foundation for the detection of hereditary tumours | 2118 | 1011 | M:53 (IQR 25–73) F:55 (IQR 23–71) | Caucasian 100% | Increased risk of bladder cancer in men (8.5 (5, 13.5), p < 0.005) and women (16.2 (8.6, 27.8), p < 0.005) |
| Win et al. (2012) [25] | Prospective—Cohort | Australasia (primary)/USA and Canada secondary | The Colon Cancer Family Registry | 446 | 205 | 62 (IQR 55–68) | Caucasian 95% | Increased risk of kidney cancer (11.22 (2.31, 32.79), p < 0.001) Increased risk of bladder cancer (9.51 (1.15, 34.37), p < 0.09) |
| Asian 2% | ||||||||
| Hispanic 1% | ||||||||
| Middle east 0.5% | ||||||||
| Other 1.5% | ||||||||
| Wischhusen et al. (2020) [4] | Retrospective—Cohort | USA | Myriad Genetic Laboratories database | 3828 | 1397 | 56 (IQR 48–64) | Caucasian 59.3% | Increased risk of any UTC (RR 4.1 vs. 1.2%, p < 0.0001; OR 3.22 (2.66, 3.99), p < 0.0001) Increased risk of bladder cancer (RR 1.8 vs. 0.4, p < 0.0001) and kidney cancer (RR 1.3 vs. 0.7%, p < 0.0003) |
| African American 4.8% | ||||||||
| Asian 2.9% | ||||||||
| Other 13.8% | ||||||||
| Missing/no response 19.1% |
| D1 | D2 | D3 | D4 | D5 | D6 | D7 | D8 | |
|---|---|---|---|---|---|---|---|---|
| Aarnio et al. (1999) [22] | A | A | B | C | B | B | B | N/A |
| Pande et al. (2012) [23] | B | B | B | C | B | B | B | N/A |
| Engel et al. (2012) [24] | A | A | B | C | B | B | B | N/A |
| Win et al. (2012) [25] | D | B | B | C | B | C | B | N/A |
| Wischhusen et al. (2020) [4] | A | A | B | C | B | B | B | N/A |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nassour, A.-J.; Jain, A.; Hui, N.; Siopis, G.; Symons, J.; Woo, H. Relative Risk of Bladder and Kidney Cancer in Lynch Syndrome: Systematic Review and Meta-Analysis. Cancers 2023, 15, 506. https://doi.org/10.3390/cancers15020506
Nassour A-J, Jain A, Hui N, Siopis G, Symons J, Woo H. Relative Risk of Bladder and Kidney Cancer in Lynch Syndrome: Systematic Review and Meta-Analysis. Cancers. 2023; 15(2):506. https://doi.org/10.3390/cancers15020506
Chicago/Turabian StyleNassour, Anthony-Joe, Anika Jain, Nicholas Hui, George Siopis, James Symons, and Henry Woo. 2023. "Relative Risk of Bladder and Kidney Cancer in Lynch Syndrome: Systematic Review and Meta-Analysis" Cancers 15, no. 2: 506. https://doi.org/10.3390/cancers15020506
APA StyleNassour, A. -J., Jain, A., Hui, N., Siopis, G., Symons, J., & Woo, H. (2023). Relative Risk of Bladder and Kidney Cancer in Lynch Syndrome: Systematic Review and Meta-Analysis. Cancers, 15(2), 506. https://doi.org/10.3390/cancers15020506