
Prognosis and Treatment Outcomes of Bone Metastasis in Gallbladder Adenocarcinoma: A SEER-Based Study
 , , , , , and
, , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Data Source
2.2. Patient Selection
2.3. Study Variables
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Factors Impacting Survival
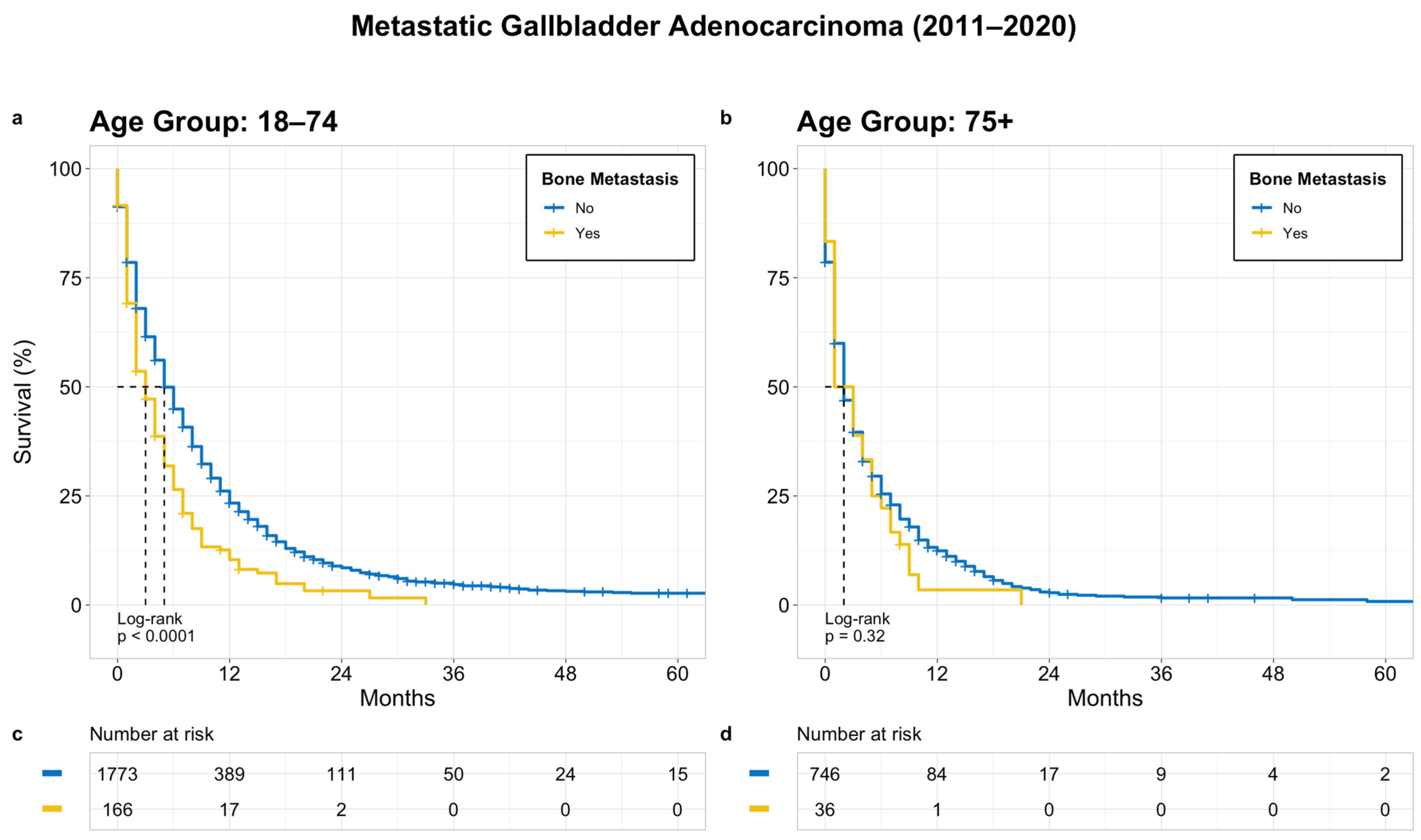
3.3. Prognostic Significance and Survival
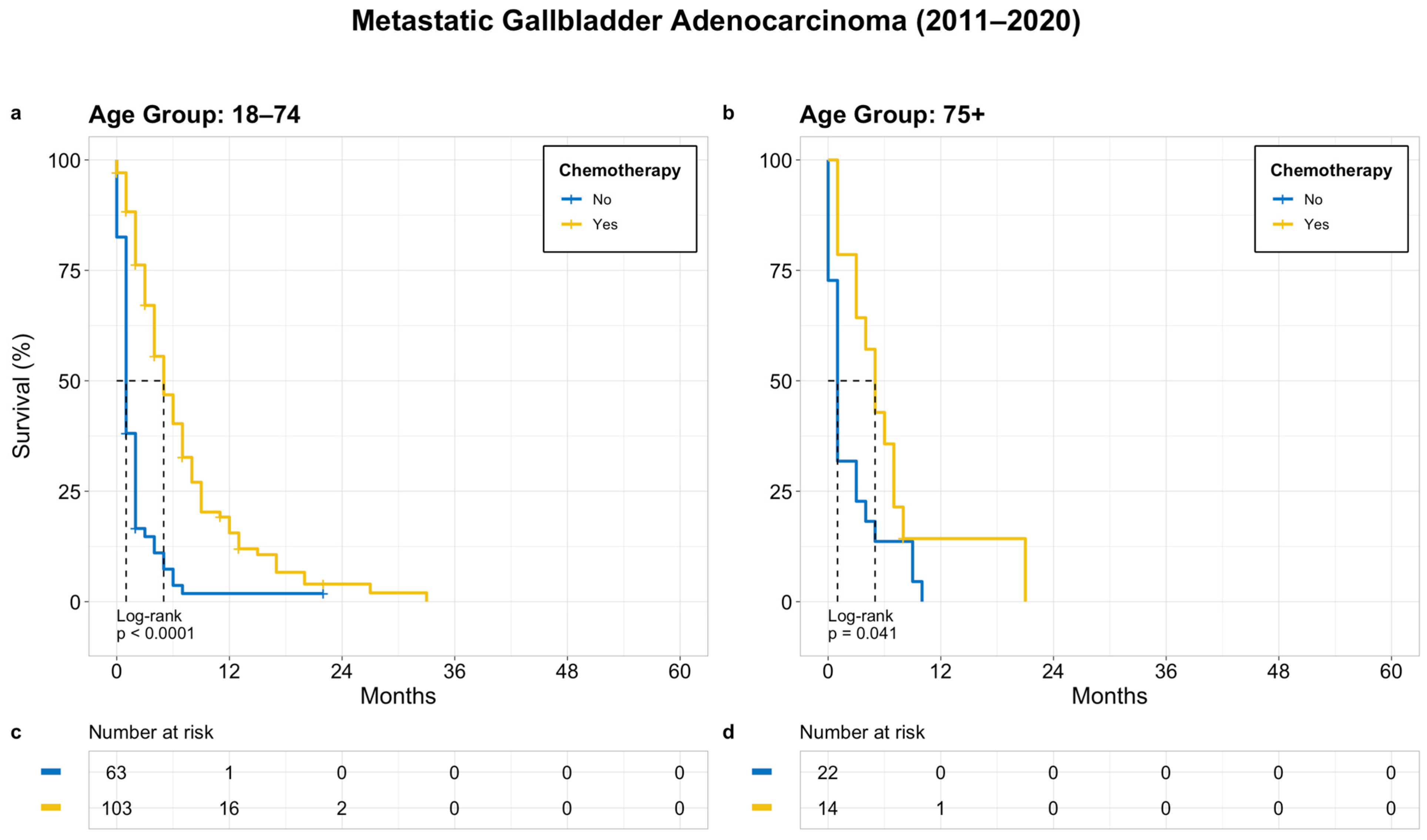
3.4. Treatment Outcomes
3.4.1. Metastatic GBC
3.4.2. Metastatic GBC with Bone Metastasis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| GBC | Gall bladder cancer |
| OS | Overall survival |
| BTC | Biliary tract cancer |
| SEER | Surveillance, Epidemiology, and End Results |
References
- Key Statistics for Gallbladder Cancer. Available online: https://www.cancer.org/cancer/types/gallbladder-cancer/about/key-statistics.html (accessed on 27 June 2023).
- Sharma, A.; Sharma, K.L.; Gupta, A.; Yadav, A.; Kumar, A. Gallbladder cancer epidemiology, pathogenesis and molecular genetics: Recent update. World J. Gastroenterol. 2017, 23, 3978. [Google Scholar] [CrossRef] [PubMed]
- Van Dyke, A.L.; Shiels, M.S.; Jones, G.S.; Pfeiffer, R.M.; Petrick, J.L.; Beebe-Dimmer, J.L.; Koshiol, J. Biliary tract cancer incidence and trends in the United States by demographic group, 1999–2013. Cancer 2019, 125, 1489–1498. [Google Scholar] [CrossRef]
- Roa, J.C.; García, P.; Kapoor, V.K.; Maithel, S.K.; Javle, M.; Koshiol, J. Gallbladder cancer. Nat. Rev. Dis. Primer 2022, 8, 69. [Google Scholar] [CrossRef]
- Dwivedi, A.N.D. Gall bladder carcinoma: Aggressive malignancy with protean loco-regional and distant spread. World J. Clin. Cases 2015, 3, 231. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Bhojwani, R.; Singh, S.; Bhatnagar, A.; Saran, R.K.; Agarwal, A.K. Skeletal metastasis in gall bladder cancer. HPB 2007, 9, 71–72. [Google Scholar] [CrossRef] [PubMed]
- Kanthan, R.; Senger, J.-L.; Ahmed, S.; Kanthan, S.C. Gallbladder Cancer in the 21st Century. J. Oncol. 2015, 2015, 967472. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, A.; Brandi, G. First-line Chemotherapy in Advanced Biliary Tract Cancer Ten Years After the ABC-02 Trial: “And Yet It Moves!”. Cancer Treat. Res. Commun. 2021, 27, 100335. [Google Scholar] [CrossRef]
- Javle, M.; Borad, M.J.; Azad, N.S.; Kurzrock, R.; Abou-Alfa, G.K.; George, B.; Hainsworth, J.; Meric-Bernstam, F.; Swanton, C.; Sweeney, C.J.; et al. Pertuzumab and trastuzumab for HER2-positive, metastatic biliary tract cancer (MyPathway): A multicentre, open-label, phase 2a, multiple basket study. Lancet Oncol. 2021, 22, 1290–1300. [Google Scholar] [CrossRef]
- Aswani, Y.; Hira, P. Skeletal Metastasis from Carcinoma of the Gall Bladder: Need for Bone Scintigraphy Justified? Pol. J. Radiol. 2016, 81, 206–208. [Google Scholar] [CrossRef]
- Santini, D.; Brandi, G.; Aprile, G.; Russano, M.; Cereda, S.; Leone, F.; Lonardi, S.; Fornaro, L.; Scartozzi, M.; Silvestris, N.; et al. Bone metastases in biliary cancers: A multicenter retrospective survey. J. Bone Oncol. 2018, 12, 33–37. [Google Scholar] [CrossRef]
- Witjes, C.D.M.; Van Den Akker, S.A.W.; Visser, O.; Karim-Kos, H.E.; De Vries, E.; IJzermans, J.N.M.; De Man, R.A.; Coebergh, J.W.W.; Verhoef, C. Gallbladder Cancer in the Netherlands: Incidence, Treatment and Survival Patterns since 1989. Dig. Surg. 2012, 29, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Ertel, A.E.; Bentrem, D.; Abbott, D.E. Gall Bladder Cancer. In Gastrointestinal Malignancies; Cancer Treatment and Research; Bentrem, D., Benson, A.B., Eds.; Springer International Publishing: Cham, Switzerland, 2016; pp. 101–120. ISBN 978-3-319-34242-9. [Google Scholar]
- Shindoh, J.; De Aretxabala, X.; Aloia, T.A.; Roa, J.C.; Roa, I.; Zimmitti, G.; Javle, M.; Conrad, C.; Maru, D.M.; Aoki, T.; et al. Tumor Location Is a Strong Predictor of Tumor Progression and Survival in T2 Gallbladder Cancer: An International Multicenter Study. Ann. Surg. 2015, 261, 733–739. [Google Scholar] [CrossRef]
- Müller, B.G.; De Aretxabala, X.; González Domingo, M. A Review of Recent Data in the Treatment of Gallbladder Cancer: What We Know, What We Do, and What Should Be Done. Am. Soc. Clin. Oncol. Educ. Book 2014, 34, e165–e170. [Google Scholar] [CrossRef] [PubMed]
- Castro, F.A.; Koshiol, J.; Hsing, A.W.; Devesa, S.S. Biliary tract cancer incidence in the United States-Demographic and temporal variations by anatomic site: Biliary tract cancer incidence in the US by anatomic site. Int. J. Cancer 2013, 133, 1664–1671. [Google Scholar] [CrossRef] [PubMed]
- Registry Groupings in SEER Data and Statistics—SEER Registries. Available online: https://seer.cancer.gov/registries/terms.html (accessed on 28 June 2023).
- Valle, J.; Wasan, H.; Palmer, D.H.; Cunningham, D.; Anthoney, A.; Maraveyas, A.; Madhusudan, S.; Iveson, T.; Hughes, S.; Pereira, S.P.; et al. Cisplatin plus Gemcitabine versus Gemcitabine for Biliary Tract Cancer. N. Engl. J. Med. 2010, 362, 1273–1281. [Google Scholar] [CrossRef]
- Wernberg, J.A.; Lucarelli, D.D. Gallbladder Cancer. Surg. Clin. N. Am. 2014, 94, 343–360. [Google Scholar] [CrossRef] [PubMed]
- Jaruvongvanich, V.; Yang, J.D.; Peeraphatdit, T.; Roberts, L.R. The incidence rates and survival of gallbladder cancer in the USA. Eur. J. Cancer Prev. 2019, 28, 1–9. [Google Scholar] [CrossRef]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012: Globocan 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef]
- Ries, L.G.; Young, J.L.; Keel, G.E.; Eisner, M.P.; Lin, Y.D.; Horner, M.J. (Eds.) SEER Survival Monograph: Cancer Survival among Adults: U.S. SEER Program, 1988–2001, Patient and Tumor Characteristics; National Cancer Institute, SEER Program: Bethesda, MD, USA, 2007.
- Randi, G.; Malvezzi, M.; Levi, F.; Ferlay, J.; Negri, E.; Franceschi, S.; La Vecchia, C. Epidemiology of biliary tract cancers: An update. Ann. Oncol. 2009, 20, 146–159. [Google Scholar] [CrossRef]
- Carriaga, M.T.; Henson, D.E. Liver, gallbladder, extrahepatic bile ducts, and pancreas. Cancer 1995, 75, 171–190. [Google Scholar] [CrossRef]
- Novacek, G. Gender and Gallstone Disease. Wien. Med. Wochenschr. 2006, 156, 527–533. [Google Scholar] [CrossRef]
- Jiang, Y.; Jiang, L.; Li, H.; Yuan, S.; Huang, S.; Fu, Y.; Li, S.; Li, F.; Li, Q.; Yan, X.; et al. Adjuvant chemoradiotherapy in resected gallbladder cancer: A SEER-based study. Heliyon 2023, 9, e14574. [Google Scholar] [CrossRef]
- Han, D.; Yang, J.; Xu, F.; Huang, Q.; Bai, L.; Wei, Y.; Kaaya, R.E.; Wang, S.; Lyu, J. Prognostic factors in patients with gallbladder adenocarcinoma identified using competing-risks analysis: A study of cases in the SEER database. Medicine 2020, 99, e21322. [Google Scholar] [CrossRef]
- Jaruvongvanich, V.; Assavapongpaiboon, B.; Wong, L. Racial/ethnic disparities in gallbladder cancer receipt of treatments. J. Gastrointest. Oncol. 2018, 9, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.; Chao, K.S.C.; Østbye, T.; Castleberry, A.W.; Pietrobon, R.; Gloor, B.; Clary, B.M.; White, R.R.; Worni, M. Trends in Racial Disparities in Pancreatic Cancer Surgery. J. Gastrointest. Surg. 2013, 17, 1897–1906. [Google Scholar] [CrossRef] [PubMed]
- Ha, J.; Yan, M.; Aguilar, M.; Tana, M.; Liu, B.; Frenette, C.T.; Bhuket, T.; Wong, R.J. Race/Ethnicity-specific Disparities in Hepatocellular Carcinoma Stage at Diagnosis and its Impact on Receipt of Curative Therapies. J. Clin. Gastroenterol. 2016, 50, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Landi, L.; D’Incà, F.; Gelibter, A.; Chiari, R.; Grossi, F.; Delmonte, A.; Passaro, A.; Signorelli, D.; Gelsomino, F.; Galetta, D.; et al. Bone metastases and immunotherapy in patients with advanced non-small-cell lung cancer. J. Immunother. Cancer 2019, 7, 316. [Google Scholar] [CrossRef]
- DePuy, V.; Anstrom, K.J.; Castel, L.D.; Schulman, K.A.; Weinfurt, K.P.; Saad, F. Effects of skeletal morbidities on longitudinal patient-reported outcomes and survival in patients with metastatic prostate cancer. Support. Care Cancer 2007, 15, 869–876. [Google Scholar] [CrossRef] [PubMed]
- Gandaglia, G.; Karakiewicz, P.I.; Briganti, A.; Passoni, N.M.; Schiffmann, J.; Trudeau, V.; Graefen, M.; Montorsi, F.; Sun, M. Impact of the Site of Metastases on Survival in Patients with Metastatic Prostate Cancer. Eur. Urol. 2015, 68, 325–334. [Google Scholar] [CrossRef]
- Yang, Y.; Tu, Z.; Ye, C.; Cai, H.; Yang, S.; Chen, X.; Tu, J. Site-specific metastases of gallbladder adenocarcinoma and their prognostic value for survival: A SEER-based study. BMC Surg. 2021, 21, 59. [Google Scholar] [CrossRef]
- Halabi, S.; Kelly, W.K.; Ma, H.; Zhou, H.; Solomon, N.C.; Fizazi, K.; Tangen, C.M.; Rosenthal, M.; Petrylak, D.P.; Hussain, M.; et al. Meta-Analysis Evaluating the Impact of Site of Metastasis on Overall Survival in Men with Castration-Resistant Prostate Cancer. J. Clin. Oncol. 2016, 34, 1652–1659. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Zhu, Y.; Liu, X.; Liao, X.; He, J.; Niu, L. The Clinicopathological features and survival outcomes of patients with different metastatic sites in stage IV breast cancer. BMC Cancer 2019, 19, 1091. [Google Scholar] [CrossRef] [PubMed]
- Tufano, A.; Cordua, N.; Nardone, V.; Ranavolo, R.; Flammia, R.S.; D’Antonio, F.; Borea, F.; Anceschi, U.; Leonardo, C.; Morrione, A.; et al. Prognostic Significance of Organ-Specific Metastases in Patients with Metastatic Upper Tract Urothelial Carcinoma. J. Clin. Med. 2022, 11, 5310. [Google Scholar] [CrossRef] [PubMed]
- Youssef, F.; Khan, A.W.; Davidson, B.R. Disseminated bony metastases following incidental gallbladder cancer detected after laparoscopic cholecystectomy. HPB 2003, 5, 258–260. [Google Scholar] [CrossRef]
- Zhu, A.X.; Hong, T.S.; Hezel, A.F.; Kooby, D.A. Current Management of Gallbladder Carcinoma. Oncologist 2010, 15, 168–181. [Google Scholar] [CrossRef]
- Oh, D.-Y.; He, A.; Qin, S.; Chen, L.-T.; Okusaka, T.; Kim, J.W.; Suksombooncharoen, T.; Lee, M.; Kitano, M.; Burris, H.; et al. Durvalumab plus Gemcitabine and Cisplatin in Advanced Biliary Tract Cancer. NEJM Evid. 2022, 1. [Google Scholar] [CrossRef]
- Kelley, R.K.; Ueno, M.; Yoo, C.; Finn, R.S.; Furuse, J.; Ren, Z.; Yau, T.; Klümpen, H.-J.; Chan, S.L.; Ozaka, M.; et al. Pembrolizumab in combination with gemcitabine and cisplatin compared with gemcitabine and cisplatin alone for patients with advanced biliary tract cancer (KEYNOTE-966): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2023, 401, 1853–1865. [Google Scholar] [CrossRef]
- Azizi, A.A.; Lamarca, A.; McNamara, M.G.; Valle, J.W. Chemotherapy for advanced gallbladder cancer (GBC): A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2021, 163, 103328. [Google Scholar] [CrossRef]
- Kang, M.J.; Song, Y.; Jang, J.; Han, I.W.; Kim, S. Role of radical surgery in patients with stage IV gallbladder cancer. HPB 2012, 14, 805–811. [Google Scholar] [CrossRef]
- D’Angelica, M.; Dalal, K.M.; DeMatteo, R.P.; Fong, Y.; Blumgart, L.H.; Jarnagin, W.R. Analysis of the Extent of Resection for Adenocarcinoma of the Gallbladder. Ann. Surg. Oncol. 2009, 16, 806–816. [Google Scholar] [CrossRef]
- Kayahara, M.; Nagakawa, T. Recent trends of gallbladder cancer in Japan: An analysis of 4770 patients. Cancer 2007, 110, 572–580. [Google Scholar] [CrossRef] [PubMed]
- Ercan, M.; Bostanci, E.B.; Cakir, T.; Karaman, K.; Ozer, I.; Ulas, M.; Dalgic, T.; Ozogul, Y.; Aksoy, E.; Akoglu, M. The rationality of resectional surgery and palliative interventions in the management of patients with gallbladder cancer. Am. Surg. 2015, 81, 591–599. [Google Scholar] [CrossRef] [PubMed]
- De Bitter, T.J.J.; de Reuver, P.R.; de Savornin Lohman, E.A.J.; Kroeze, L.I.; Vink-Börger, M.E.; van Vliet, S.; Simmer, F.; von Rhein, D.; Jansen, E.A.M.; Verheij, J.; et al. Comprehensive clinicopathological and genomic profiling of gallbladder cancer reveals actionable targets in half of patients. NPJ Precis. Oncol. 2022, 6, 83. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Chemotherapy Treatment | |||
|---|---|---|---|
| Variable | Overall, n = 2724 1 | No, n = 1206 1 | Yes, n = 1518 1 |
| Age at Diagnosis | |||
| Median (IQR) | 68.0 (60.0, 76.0) | 72.0 (64.0, 80.0) | 65.0 (57.0, 72.0) |
| Range | 24.0, 90.0 | 31.0, 90.0 | 24.0, 89.0 |
| Sex | |||
| Female | 1874 (69%) | 845 (70%) | 1029 (68%) |
| Male | 850 (31%) | 361 (30%) | 489 (32%) |
| Race/Ethnicity | |||
| Hispanic (All Races) | 685 (25%) | 339 (28%) | 346 (23%) |
| Non-Hispanic American Indian/Alaska Native | 31 (1.1%) | 18 (1.5%) | 13 (0.9%) |
| Non-Hispanic Asian or Pacific Islander | 279 (10%) | 121 (10%) | 158 (10%) |
| Non-Hispanic Black | 369 (14%) | 152 (13%) | 217 (14%) |
| Non-Hispanic Unknown Race | 3 (0.1%) | 0 (0%) | 3 (0.2%) |
| Non-Hispanic White | 1357 (50%) | 576 (48%) | 781 (51%) |
| Bone Metastasis | 202 (7.4%) | 85 (7.0%) | 117 (7.7%) |
| Year of diagnosis | |||
| 2011 | 226 (8.3%) | 106 (8.8%) | 120 (7.9%) |
| 2012 | 230 (8.4%) | 100 (8.3%) | 130 (8.6%) |
| 2013 | 242 (8.9%) | 107 (8.9%) | 135 (8.9%) |
| 2014 | 251 (9.2%) | 116 (9.6%) | 135 (8.9%) |
| 2015 | 256 (9.4%) | 109 (9.0%) | 147 (9.7%) |
| 2016 | 301 (11%) | 141 (12%) | 160 (11%) |
| 2017 | 306 (11%) | 131 (11%) | 175 (12%) |
| 2018 | 284 (10%) | 119 (9.9%) | 165 (11%) |
| 2019 | 325 (12%) | 153 (13%) | 172 (11%) |
| 2020 | 303 (11%) | 124 (10%) | 179 (12%) |
| Survival months | |||
| Median (IQR) | 4 (1, 9) | 1 (0, 3) | 7 (3, 12) |
| Range | 0, 107 | 0, 79 | 0, 107 |
| Histology | |||
| 8140/3: Adenocarcinoma, NOS | 2347 (86%) | 1040 (86%) | 1307 (86%) |
| 8144/3: Adenocarcinoma, intestinal type | 12 (0.4%) | 4 (0.3%) | 8 (0.5%) |
| 8160/3: Cholangiocarcinoma | 331 (12%) | 146 (12%) | 185 (12%) |
| 8211/3: Tubular adenocarcinoma | 1 (<0.1%) | 1 (<0.1%) | 0 (0%) |
| 8255/3: Adenocarcinoma with mixed subtypes | 14 (0.5%) | 7 (0.6%) | 7 (0.5%) |
| 8260/3: Papillary adenocarcinoma, NOS | 12 (0.4%) | 6 (0.5%) | 6 (0.4%) |
| 8263/3: Adenocarcinoma in tubulovillous adenoma | 1 (<0.1%) | 0 (0%) | 1 (<0.1%) |
| 8310/3: Clear cell adenocarcinoma, NOS | 6 (0.2%) | 2 (0.2%) | 4 (0.3%) |
| Bone Metastasis | |||
|---|---|---|---|
| Variable | Overall, n = 2724 1 | No, n = 2522 1 | Yes, n = 202 1 |
| Age at Diagnosis | |||
| Median (IQR) | 68.0 (60.0, 76.0) | 68.0 (60.0, 76.0) | 65.0 (57.0, 72.0) |
| Range | 24.0, 90.0 | 24.0, 90.0 | 25.0, 90.0 |
| Sex | |||
| Female | 1874 (69%) | 1749 (69%) | 125 (62%) |
| Male | 850 (31%) | 773 (31%) | 77 (38%) |
| Race/Ethnicity | |||
| Hispanic (All Races) | 685 (25%) | 640 (25%) | 45 (22%) |
| Non-Hispanic American Indian/Alaska Native | 31 (1.1%) | 30 (1.2%) | 1 (0.5%) |
| Non-Hispanic Asian or Pacific Islander | 279 (10%) | 262 (10%) | 17 (8.4%) |
| Non-Hispanic Black | 369 (14%) | 338 (13%) | 31 (15%) |
| Non-Hispanic Unknown Race | 3 (0.1%) | 3 (0.1%) | 0 (0%) |
| Non-Hispanic White | 1357 (50%) | 1249 (50%) | 108 (53%) |
| Chemotherapy | 1518 (56%) | 1401 (56%) | 117 (58%) |
| Year of diagnosis | |||
| 2011 | 226 (8.3%) | 217 (8.6%) | 9 (4.5%) |
| 2012 | 230 (8.4%) | 213 (8.4%) | 17 (8.4%) |
| 2013 | 242 (8.9%) | 222 (8.8%) | 20 (9.9%) |
| 2014 | 251 (9.2%) | 233 (9.2%) | 18 (8.9%) |
| 2015 | 256 (9.4%) | 239 (9.5%) | 17 (8.4%) |
| 2016 | 301 (11%) | 271 (11%) | 30 (15%) |
| 2017 | 306 (11%) | 280 (11%) | 26 (13%) |
| 2018 | 284 (10%) | 267 (11%) | 17 (8.4%) |
| 2019 | 325 (12%) | 304 (12%) | 21 (10%) |
| 2020 | 303 (11%) | 276 (11%) | 27 (13%) |
| Survival months | |||
| Median (IQR) | 4 (1, 9) | 4 (1, 9) | 3 (1, 6) |
| Range | 0, 107 | 0, 107 | 0, 33 |
| Histology | |||
| 8140/3: Adenocarcinoma, NOS | 2347 (86%) | 2179 (86%) | 168 (83%) |
| 8144/3: Adenocarcinoma, intestinal type | 12 (0.4%) | 12 (0.5%) | 0 (0%) |
| 8160/3: Cholangiocarcinoma | 331 (12%) | 301 (12%) | 30 (15%) |
| 8211/3: Tubular adenocarcinoma | 1 (<0.1%) | 1 (<0.1%) | 0 (0%) |
| 8255/3: Adenocarcinoma with mixed subtypes | 14 (0.5%) | 12 (0.5%) | 2 (1.0%) |
| 8260/3: Papillary adenocarcinoma, NOS | 12 (0.4%) | 11 (0.4%) | 1 (0.5%) |
| 8263/3: Adenocarcinoma in tubulovillous adenoma | 1 (<0.1%) | 1 (<0.1%) | 0 (0%) |
| 8310/3: Clear cell adenocarcinoma, NOS | 6 (0.2%) | 5 (0.2%) | 1 (0.5%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gera, K.; Kahramangil, D.; Fenton, G.A.; Martir, D.; Rodriguez, D.N.; Ijaz, Z.; Lin, R.Y.; Rogers, S.C.; Ramnaraign, B.H.; George, T.J.; et al. Prognosis and Treatment Outcomes of Bone Metastasis in Gallbladder Adenocarcinoma: A SEER-Based Study. Cancers 2023, 15, 5055. https://doi.org/10.3390/cancers15205055
Gera K, Kahramangil D, Fenton GA, Martir D, Rodriguez DN, Ijaz Z, Lin RY, Rogers SC, Ramnaraign BH, George TJ, et al. Prognosis and Treatment Outcomes of Bone Metastasis in Gallbladder Adenocarcinoma: A SEER-Based Study. Cancers. 2023; 15(20):5055. https://doi.org/10.3390/cancers15205055
Chicago/Turabian StyleGera, Kriti, Doga Kahramangil, Graeme A. Fenton, Daniela Martir, Diana N. Rodriguez, Zohaib Ijaz, Rick Y. Lin, Sherise C. Rogers, Brian H. Ramnaraign, Thomas J. George, and et al. 2023. "Prognosis and Treatment Outcomes of Bone Metastasis in Gallbladder Adenocarcinoma: A SEER-Based Study" Cancers 15, no. 20: 5055. https://doi.org/10.3390/cancers15205055
APA StyleGera, K., Kahramangil, D., Fenton, G. A., Martir, D., Rodriguez, D. N., Ijaz, Z., Lin, R. Y., Rogers, S. C., Ramnaraign, B. H., George, T. J., Hong, Y. -R., Hughes, S. J., Nassour, I., & Sahin, I. (2023). Prognosis and Treatment Outcomes of Bone Metastasis in Gallbladder Adenocarcinoma: A SEER-Based Study. Cancers, 15(20), 5055. https://doi.org/10.3390/cancers15205055