
Dosimetric Impact of Lesion Number, Size, and Volume on Mean Brain Dose with Stereotactic Radiosurgery for Multiple Brain Metastases
 , ,
, ,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
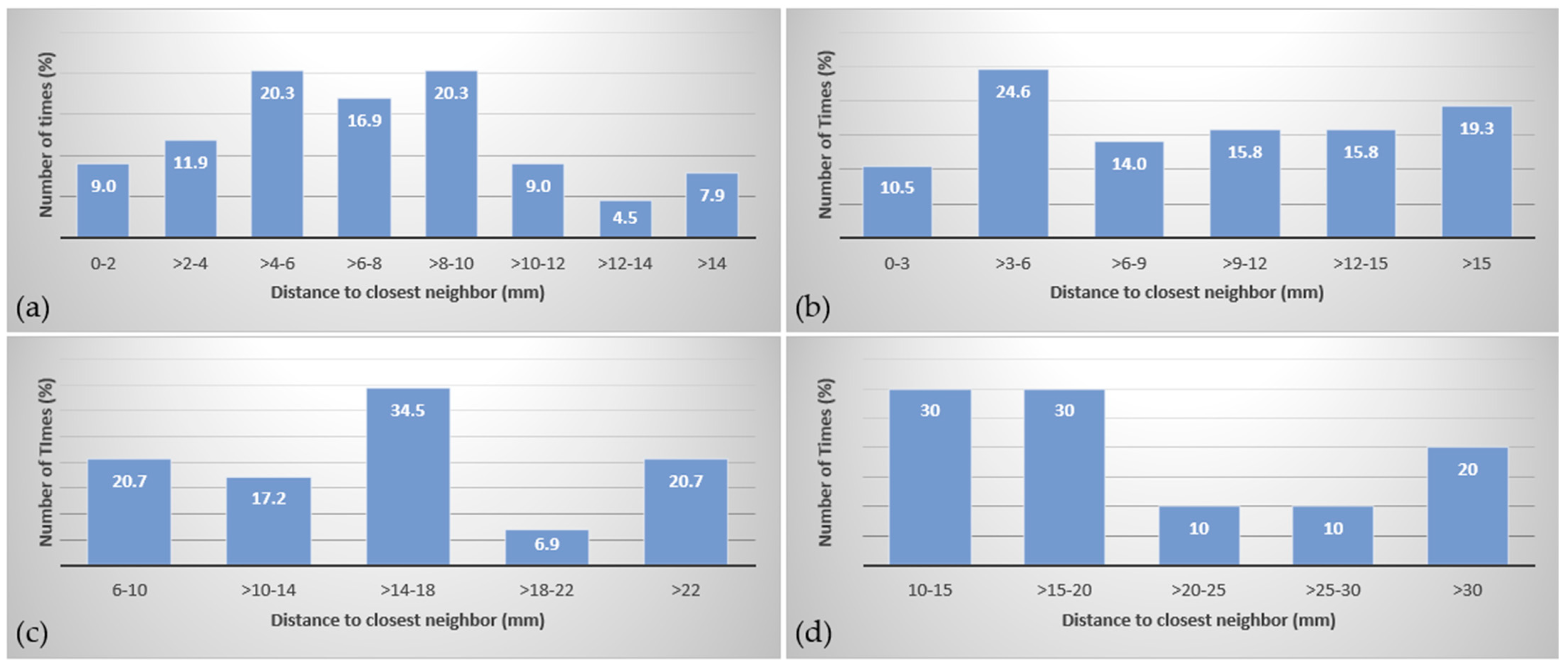
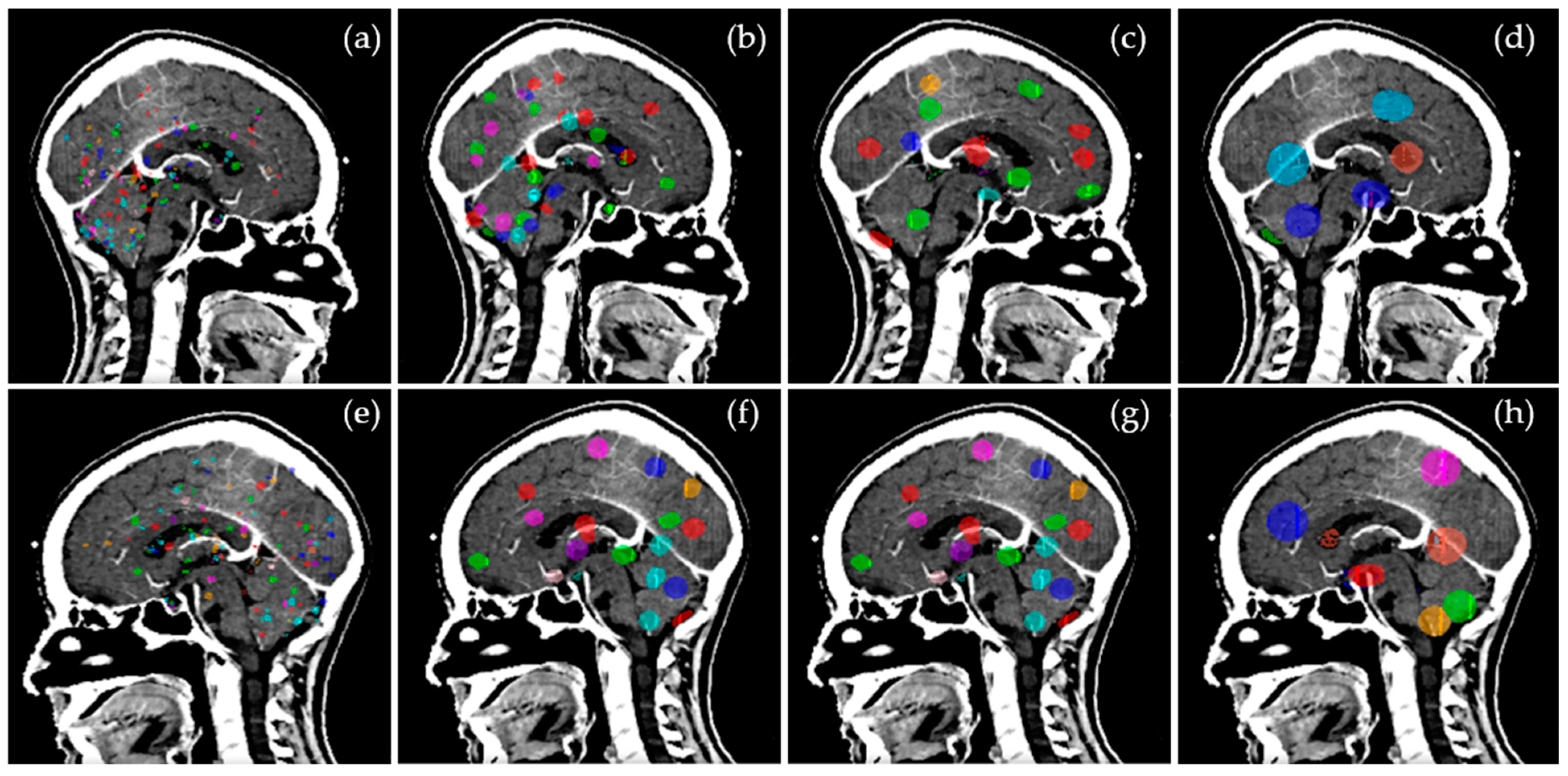
3.1. Target Distribution
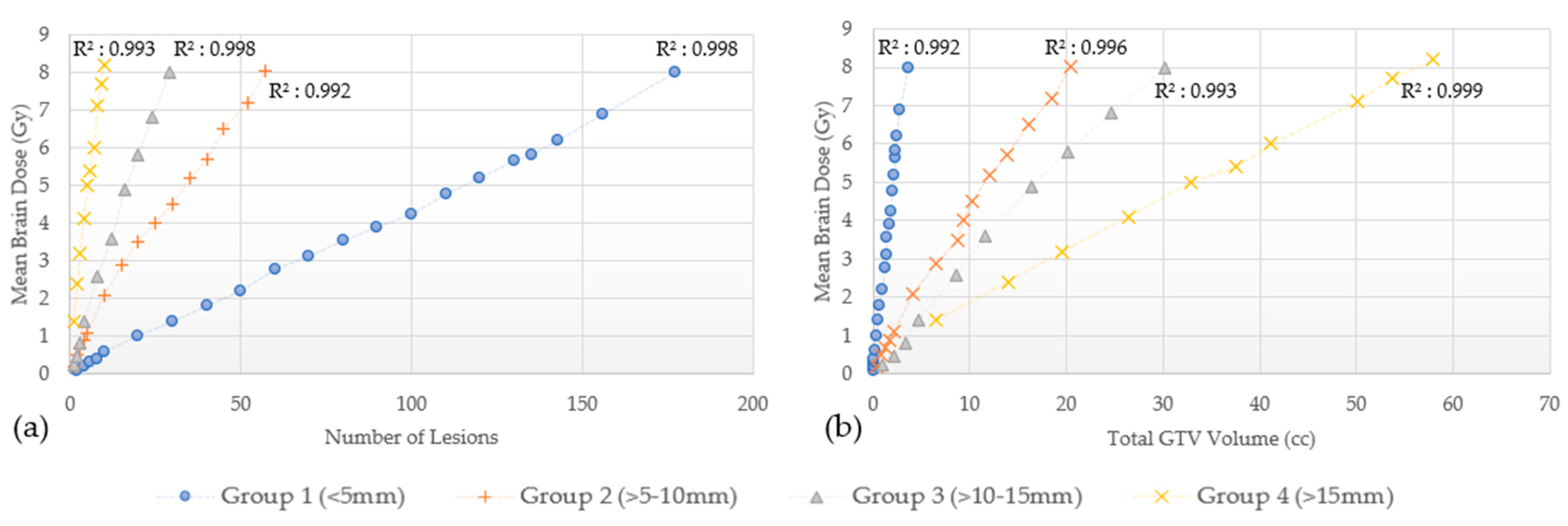
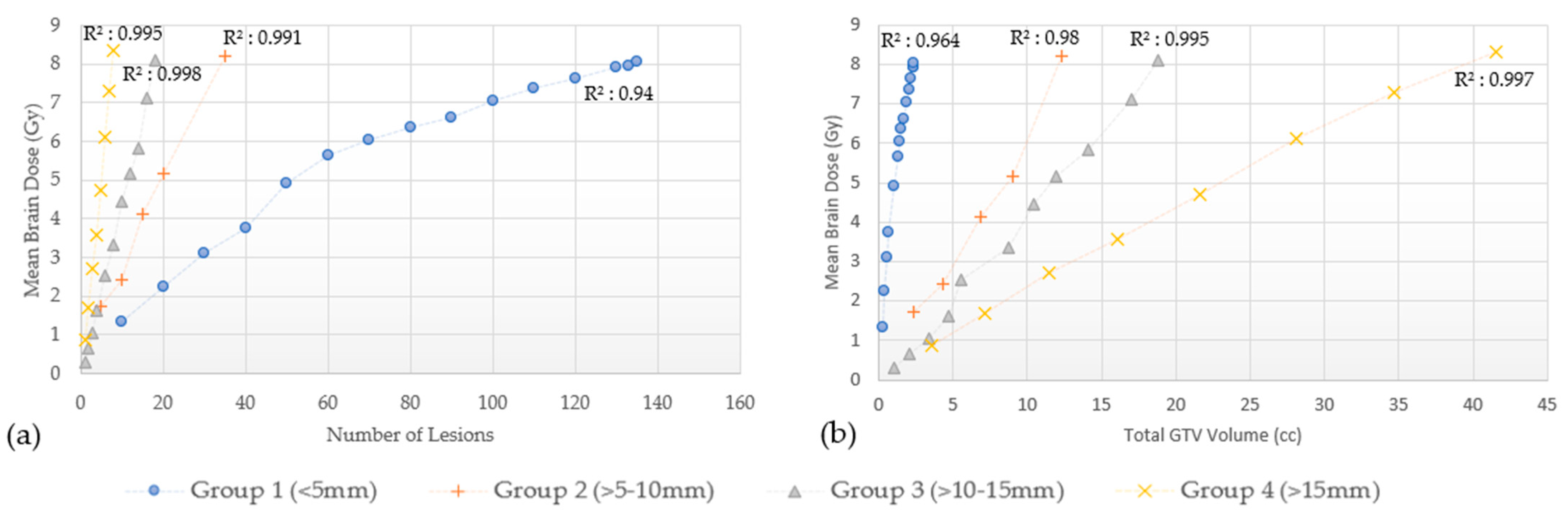
3.2. Effect of the Number of Lesions and Total Volume
3.2.1. Brain Mean Dose
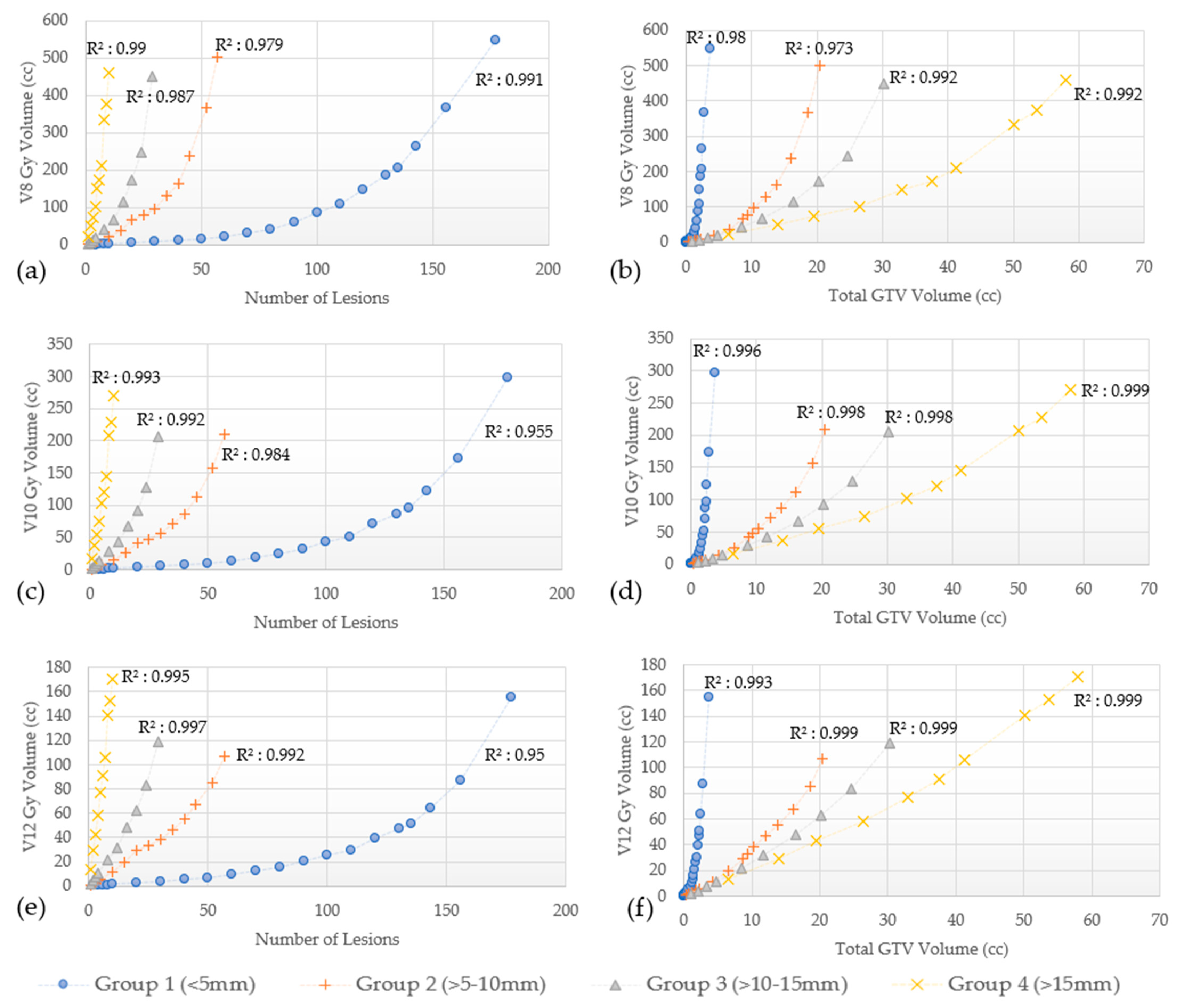
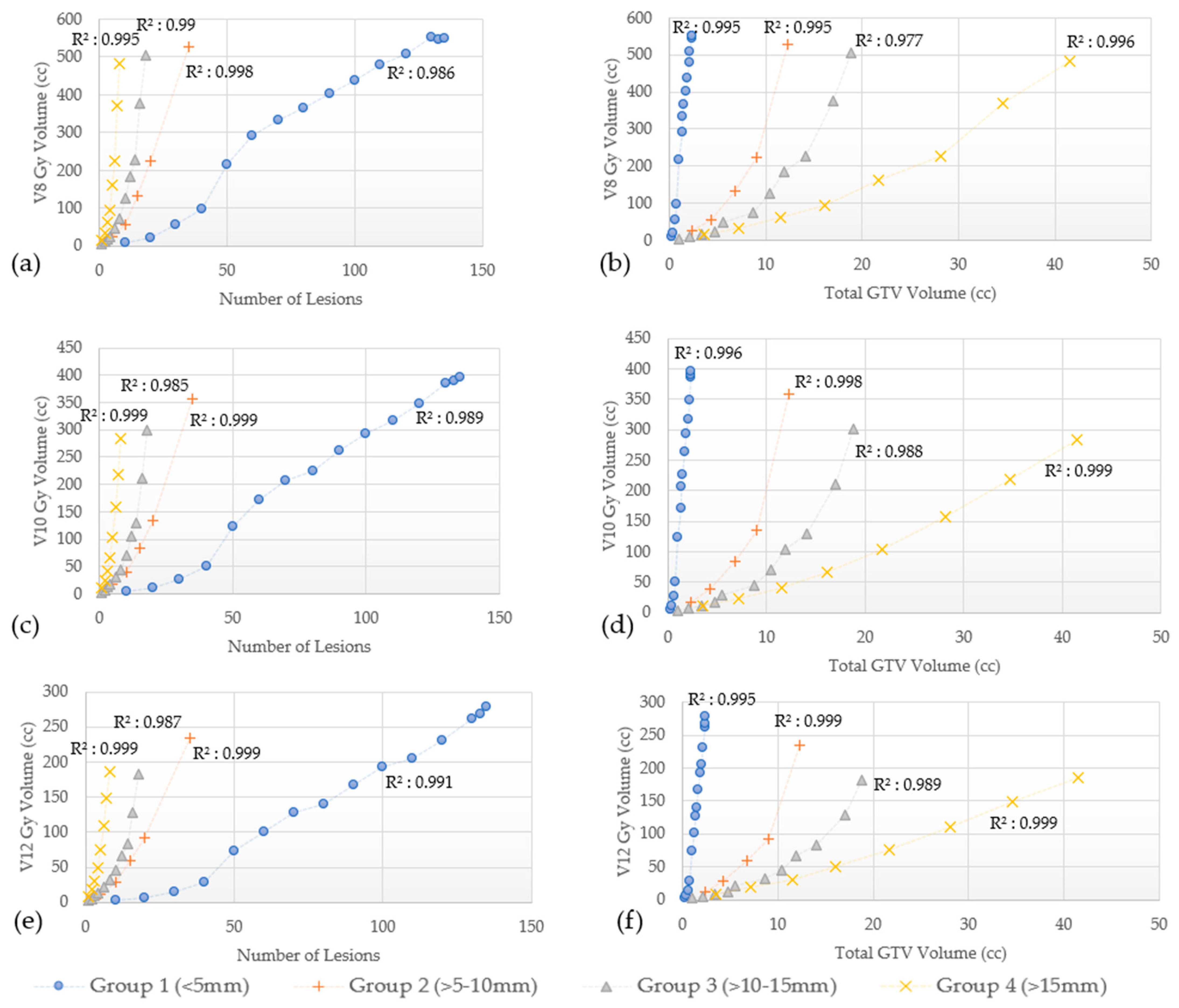
3.2.2. Other Dosimetric Parameters (V8 Gy, V10 Gy and V12 Gy)
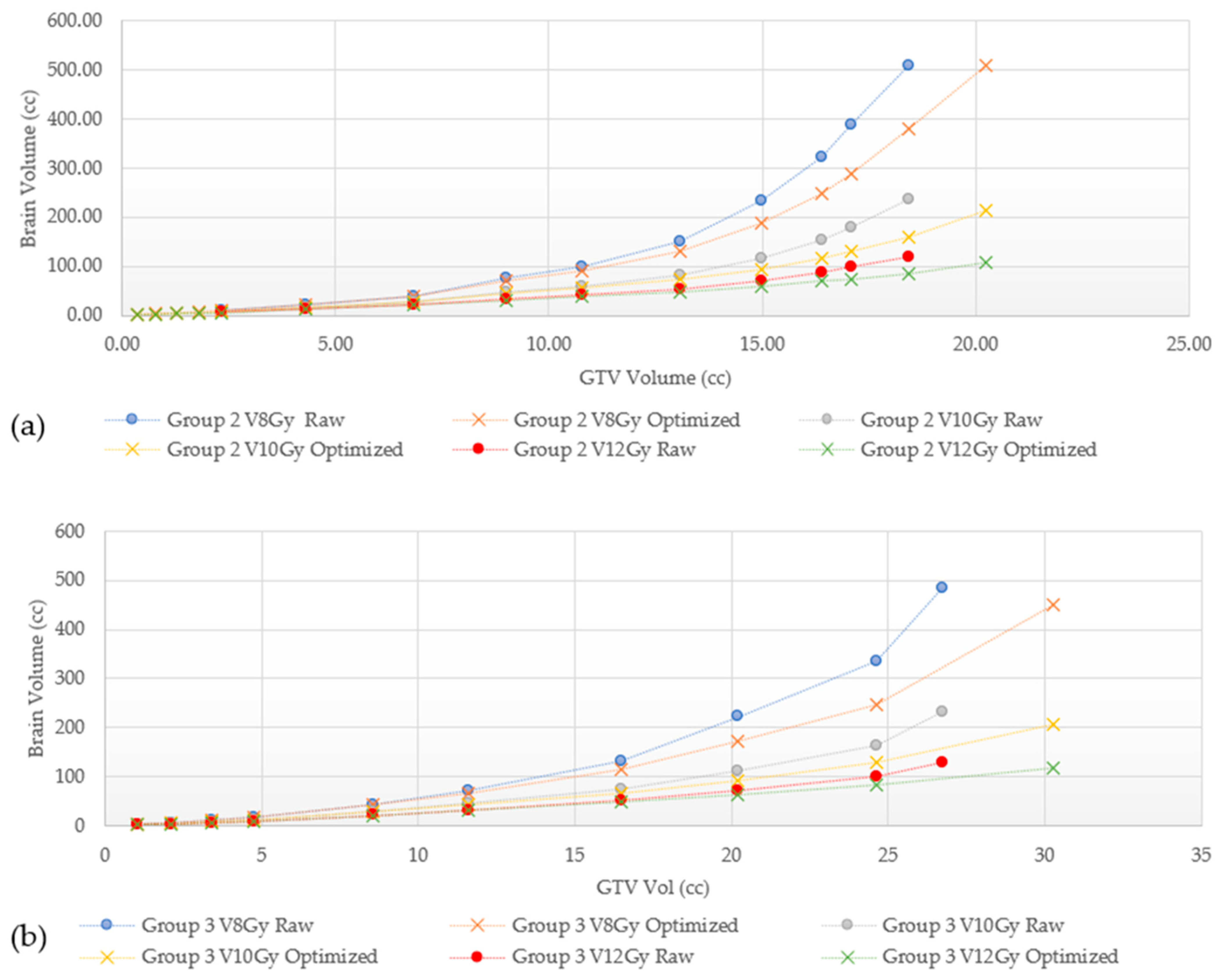
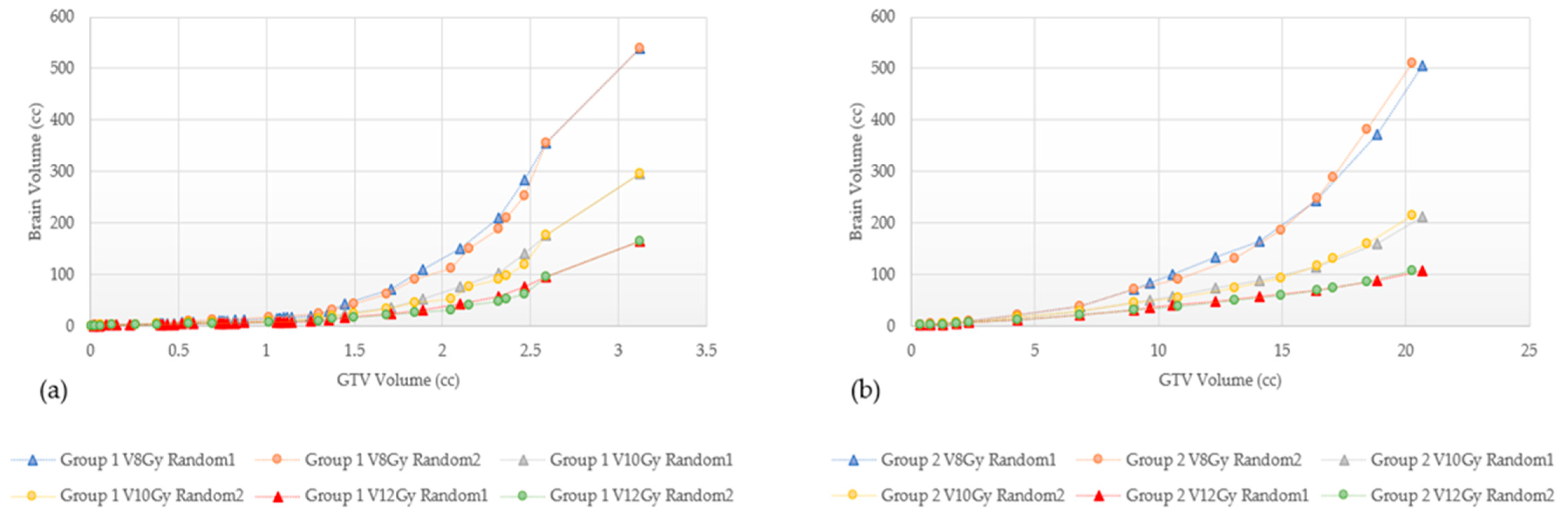
3.3. Effect of Treatment Planning Technique
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Campbell, S.T.; Ward, M.C.; Suh, J.H. Brain Metastasis. In Essentials of Clinical Radiation Oncology, 2nd ed.; Ward, M.C., Tendulkar, R., Videtic, G., Eds.; Demos Medical: New York, NY, USA, 2021. [Google Scholar]
- Kutuk, T.; Abrams, K.J.; Tom, M.C.; Rubens, M.; Appel, H.; Sidani, C.; Hall, M.D.; Tolakanahalli, R.; Wieczorek, D.J.J.; Gutierrez, A.N.; et al. Dedicated isotropic 3-D T1 SPACE sequence imaging for radiosurgery planning improves brain metastases detection and reduces the risk of intracranial relapse. Radiother. Oncol. 2022, 173, 84–92. [Google Scholar] [CrossRef]
- Gondi, V.; Pugh, S.; Brown, P.D.; Wefel, J.; Gilbert, M.; Bovi, J.; Robinson, C.; Tammie, B.; Tome, W.; Armstrong, T.; et al. NCOG-01. Preservation of Neurocognitive Function (NCF) with Hippocampal Avoidance During Whole-Brain Radiotherapy (WBRT) for Brain Metastases: Preliminary Results of Phase III Trial NRG Oncology CC001. Neuro-Oncol. 2018, 20, vi172. [Google Scholar] [CrossRef] [Green Version]
- Brown, P.D.; Gondi, V.; Pugh, S.; Tome, W.A.; Wefel, J.S.; Armstrong, T.S.; Bovi, J.A.; Robinson, C.; Konski, A.; Khuntia, D.; et al. Hippocampal Avoidance During Whole-Brain Radiotherapy Plus Memantine for Patients with Brain Metastases: Phase III Trial NRG Oncology CC001. J. Clin. Oncol. 2020, 38, 1019–1029. [Google Scholar] [CrossRef] [PubMed]
- Andrews, D.W.; Scott, C.B.; Sperduto, P.W.; Flanders, A.E.; Gaspar, L.E.; Schell, M.C.; Werner-Wasik, M.; Demas, W.; Ryu, J.; Bahary, J.P.; et al. Whole brain radiation therapy with or without stereotactic radiosurgery boost for patients with one to three brain metastases: Phase III results of the RTOG 9508 randomised trial. Lancet 2004, 363, 1665–1672. [Google Scholar] [CrossRef]
- Yamamoto, M.; Serizawa, T.; Shuto, T.; Akabane, A.; Higuchi, Y.; Kawagishi, J.; Yamanaka, K.; Sato, Y.; Jokura, H.; Yomo, S.; et al. Stereotactic radiosurgery for patients with multiple brain metastases (JLGK0901): A multi-institutional prospective observational study. Lancet Oncol. 2014, 15, 387–395. [Google Scholar] [CrossRef] [PubMed]
- Kocher, M.; Soffietti, R.; Abacioglu, U.; Villà, S.; Fauchon, F.; Baumert, B.G.; Fariselli, L.; Tzuk-Shina, T.; Kortmann, R.D.; Carrie, C.; et al. Adjuvant whole-brain radiotherapy versus observation after radiosurgery or surgical resection of one to three cerebral metastases: Results of the EORTC 22952-26001 study. J. Clin. Oncol. 2011, 29, 134–141. [Google Scholar] [CrossRef] [Green Version]
- Brown, P.D.; Jaeckle, K.; Ballman, K.V.; Farace, E.; Cerhan, J.H.; Anderson, S.K.; Carrero, X.W.; Barker, F.G., 2nd; Deming, R.; Burri, S.H.; et al. Effect of Radiosurgery Alone vs Radiosurgery with Whole Brain Radiation Therapy on Cognitive Function in Patients With 1 to 3 Brain Metastases: A Randomized Clinical Trial. JAMA 2016, 316, 401–409. [Google Scholar] [CrossRef]
- Vogelbaum, M.A.; Brown, P.D.; Messersmith, H.; Brastianos, P.K.; Burri, S.; Cahill, D.; Dunn, I.F.; Gaspar, L.E.; Gatson, N.T.N.; Gondi, V.; et al. Treatment for Brain Metastases: ASCO-SNO-ASTRO Guideline. J. Clin. Oncol. 2022, 40, 492–516. [Google Scholar] [CrossRef]
- Li, J.; Ludmir, E.B.; Wang, Y.; Guha-Thakurta, N.; McAleer, M.F.; Settle, S.H., Jr.; Yeboa, D.N.; Ghia, A.J.; McGovern, S.L.; Chung, C.; et al. Stereotactic Radiosurgery versus Whole-brain Radiation Therapy for Patients with 4–15 Brain Metastases: A Phase III Randomized Controlled Trial. Int. J. Radiat. Oncol. Biol. Phys. 2020, 108, S21–S22. [Google Scholar] [CrossRef]
- Bashir, A.; Hodge, C.; Dababneh, H.; Hussain, M.; Hahn, S.; Canute, G. Impact of the number of metastatic brain lesions on survival after Gamma Knife radiosurgery—ClinicalKey. J. Clin. Neurosci. 2014, 21, 1928–1933. [Google Scholar] [CrossRef]
- Ojerholm, E.; Lee, J.Y.; Kolker, J.; Lustig, R.; Dorsey, J.; Alonso-Basanta, M. Gamma Knife radiosurgery to four or more brain metastases in patients without prior intracranial radiation or surgery. Cancer Med. 2014, 3, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, A.M.; Schroeder, J.L.; Angelov, L.; Chao, S.T.; Murphy, E.S.; Yu, J.S.; Neyman, G.; Jia, X.; Suh, J.H.; Barnett, G.H.; et al. Impact of the radiosurgery prescription dose on the local control of small (2 cm or smaller) brain metastases. J. Neurosurg. 2017, 126, 735–743. [Google Scholar] [CrossRef]
- Nguyen, T.K.; Sahgal, A.; Detsky, J.; Soliman, H.; Myrehaug, S.; Tseng, C.L.; Husain, Z.A.; Carty, A.; Das, S.; Yang, V.; et al. Single-Fraction Stereotactic Radiosurgery Versus Hippocampal-Avoidance Whole Brain Radiation Therapy for Patients With 10 to 30 Brain Metastases: A Dosimetric Analysis. Int. J. Radiat. Oncol. Biol. Phys. 2019, 105, 394–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Francel, P.; Bhattacharjee, S.; Tompkins, P. Skull base approaches and gamma knife radiosurgery for multimodality treatment of skull base tumors. J. Neurosurg. 2002, 97, 674–676. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.; Main, W.; Martin, D.; Gibbs, I.; Heilbrun, M. An analysis of the accuracy of the CyberKnife: A robotic frameless stereotactic radiosurgical system. Neurosurgery 2003, 52, 140–147. [Google Scholar] [CrossRef]
- Miller, J.; Bennett, E.; Xiao, R.; Kotecha, R.; Chao, S.; Vogelbaum, M.A.; Barnett, G.H.; Angelov., L.; Murphy, E.S.; Jennifer, S.Y.; et al. Association Between Radiation Necrosis and Tumor Biology After Stereotactic Radiosurgery for Brain Metastasis. Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 1060–1069. [Google Scholar] [CrossRef]
- Wieczorek, D.J.; Kotecha, R.; Hall, M.D.; Tom, M.C.; Davis, S.; Ahluwalia, M.S.; McDermott, M.W.; Mehta, M.P.; Gutierrez, A.N.; Tolakanahalli, R. Systematic evaluation and plan quality assessment of the Leksell® gamma knife® lightning dose optimizer. Med. Dosim. 2022, 47, 70–78. [Google Scholar] [CrossRef]
- Harwood, A.R.; Simson, W.J. Radiation therapy of cerebral metastases: A randomized prospective clinical trial. Int. J. Radiat. Oncol. Biol. Phys. 1977, 2, 1091–1094. [Google Scholar] [CrossRef]
- Hanna, G.; Murray, L.; Patel, R.; Jain, S.; Aitken, K.; Franks, K.; Tree, A.; Hatfield, P.; Harrow, S.; McDonald, F.; et al. UK Consensus on Normal Tissue Dose Constraints for Stereotactic Radiotherapy. Clin. Oncol. (R Coll. Radiol.) 2018, 30, 5–14. [Google Scholar] [CrossRef] [Green Version]
- Hindo, W.; DeTrana, F.; Lee, M.; Hendrickson, F. Large dose increment irradiation in treatment of cerebral metastases. Cancer 1970, 26, 2–5. [Google Scholar] [CrossRef]
- Gondi, V.; Bauman, G.; Bradfield, L.; Burri, S.H.; Cabrera, A.R.; Cunningham, D.A.; Eaton, B.R.; Hattangadi-Gluth, J.A.; Kim, M.M.; Kotecha, R.; et al. Radiation Therapy for Brain Metastases: An ASTRO Clinical Practice Guideline. Pract. Radiat. Oncol. 2022, 12, 265–282. [Google Scholar] [CrossRef]
- Mohammadi, A.M.; Recinos, P.F.; Barnett, G.H.; Weil, R.J.; Vogelbaum, M.A.; Chao, S.T.; Suh, J.H.; Marko, N.F.; Elson, P.; Neyman, G.; et al. Role of Gamma Knife surgery in patients with 5 or more brain metastases. J. Neurosurg. 2012, 117, 5–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamamoto, M.; Kawabe, T.; Sato, Y.; Higuchi, Y.; Nariai, T.; Watanabe, S.; Kasuya, H. Stereotactic radiosurgery for patients with multiple brain metastases: A case-matched study comparing treatment results for patients with 2–9 versus 10 or more tumors. J. Neurosurg. 2014, 121, 16–25. [Google Scholar] [CrossRef] [Green Version]
- Ali, M.A.; Hirshman, B.R.; Wilson, B.; Carroll, K.T.; Proudfoot, J.A.; Goetsch, S.J.; Alksne, J.F.; Ott, K.; Aiyama, H.; Nagano, O.; et al. Survival Patterns of 5750 Stereotactic Radiosurgery-Treated Patients with Brain Metastasis as a Function of the Number of Lesions. World Neurosurg. 2017, 107, 944–951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baschnagel, A.M.; Meyer, K.D.; Chen, P.Y.; Krauss, D.J.; Olson, R.E.; Pieper, D.R.; Maitz, A.H.; Ye, H.; Grills, I.S. Tumor volume as a predictor of survival and local control in patients with brain metastases treated with Gamma Knife surgery. J. Neurosurg. 2013, 119, 1139–1144. [Google Scholar] [CrossRef] [Green Version]
- Rava, P.; Leonard, K.; Sioshansi, S.; Curran, B.; Wazer, D.E.; Cosgrove, G.R.; Norén, G.; Hepel, J.T. Survival among patients with 10 or more brain metastases treated with stereotactic radiosurgery. J. Neurosurg. 2013, 119, 457–462. [Google Scholar] [CrossRef] [Green Version]
- Palmer, J.D.; Sebastian, N.T.; Chu, J.; DiCostanzo, D.; Bell, E.H.; Grecula, J.; Arnett, A.; Blakaj, D.M.; McGregor, J.; Elder, J.B.; et al. Single-Isocenter Multitarget Stereotactic Radiosurgery Is Safe and Effective in the Treatment of Multiple Brain Metastases. Adv. Radiat. Oncol. 2020, 5, 70–76. [Google Scholar] [CrossRef] [Green Version]
- Hughes, R.T.; Masters, A.H.; McTyre, E.R.; Farris, M.K.; Chung, C.; Page, B.R.; Kleinberg, L.R.; Hepel, J.; Contessa, J.N.; Chiang, V.; et al. Initial SRS for Patients With 5 to 15 Brain Metastases: Results of a Multi-Institutional Experience. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 1091–1098. [Google Scholar] [CrossRef] [PubMed]
- Serizawa, T.; Higuchi, Y.; Nagano, O.; Matsuda, S.; Aoyagi, K.; Ono, J.; Saeki, N.; Iwadate, Y.; Hirai, T.; Takemoto, S.; et al. Robustness of the neurological prognostic score in brain metastasis patients treated with Gamma Knife radiosurgery. J. Neurosurg. 2017, 127, 1000–1006. [Google Scholar] [CrossRef]
- Milano, M.T.; Grimm, J.; Niemierko, A.; Soltys, S.G.; Moiseenko, V.; Redmond, K.J.; Yorke, E.; Sahgal, A.; Xue, J.; Mahadevan, A.; et al. Single- and Multifraction Stereotactic Radiosurgery Dose/Volume Tolerances of the Brain. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 68–86. [Google Scholar] [CrossRef] [PubMed]
- Sita, T.L.; Gopalakrishnan, M.; Rooney, M.K.; Ho, A.; Savoor, R.; Sonabend, A.M.; Tate, M.C.; Chandler, J.P.; Lesniak, M.S.; Kruser, T.J.; et al. Mean Brain Dose Remains Uninfluenced by the Lesion Number for Gamma Knife Stereotactic Radiosurgery for 10+ Metastases. World Neurosurg. 2022, 165, e380–e385. [Google Scholar] [CrossRef] [PubMed]
- Miyawaki, L.; Dowd, C.; Wara, W.; Goldsmith, B.; Albright, N.; Gutin, P.; Halbach, V.; Hieshima, G.; Higashida, R.; Lulu, B.; et al. Five year results of LINAC radiosurgery for arteriovenous malformations: Outcome for large AVMS. Int. J. Radiat. Oncol. Biol. Phys. 1999, 44, 1089–1106. [Google Scholar] [CrossRef]
- Ohtakara, K.; Hayashi, S.; Nakayama, N.; Ohe, N.; Yano, H.; Iwama, T.; Hoshi, H. Significance of target location relative to the depth from the brain surface and high-dose irradiated volume in the development of brain radionecrosis after micromultileaf collimator-based stereotactic radiosurgery for brain metastases. J. Neurooncol. 2012, 108, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Peng, L.; Grimm, J.; Gui, C.; Shen, C.J.; Redmond, K.J.; Sloan, L.; Hazell, S.; Moore, J.; Huang, E.; Spoleti, N.; et al. Updated risk models demonstrate low risk of symptomatic radionecrosis following stereotactic radiosurgery for brain metastases. Surg. Neurol. Int. 2019, 10, 32. [Google Scholar] [CrossRef] [PubMed]
- Korytko, T.; Radivoyevitch, T.; Colussi, V.; Wessels, B.W.; Pillai, K.; Maciunas, R.J.; Einstein, D.B. 12 Gy gamma knife radiosurgical volume is a predictor for radiation necrosis in non-AVM intracranial tumors. Int. J. Radiat. Oncol. Biol. Phys. 2006, 64, 419–424. [Google Scholar] [CrossRef] [PubMed]
- Minniti, G.; Clarke, E.; Lanzetta, G.; Osti, M.F.; Trasimeni, G.; Bozzao, A.; Romano, A.; Enrici, R.M. Stereotactic radiosurgery for brain metastases: Analysis of outcome and risk of brain radionecrosis. Radiat. Oncol. 2011, 6, 48. [Google Scholar] [CrossRef] [Green Version]
- Blonigen, B.J.; Steinmetz, R.D.; Levin, L.; Lamba, M.A.; Warnick, R.E.; Breneman, J.C. Irradiated Volume as a Predictor of Brain Radionecrosis After Linear Accelerator Stereotactic Radiosurgery. Int. J. Radiat. Oncol. Biol. Phys. 2010, 77, 996–1001. [Google Scholar] [CrossRef]
- Shaw, E.; Scott, C.; Souhami, L.; Dinapoli, R.; Kline, R.; Loeffler, J.; Farnan, N. Single dose radiosurgical treatment of recurrent previously irradiated primary brain tumors and brain metastases: Final report of RTOG protocol 90-05. Int. J. Radiat. Oncol. Biol. Phys. 2000, 47, 291–298. [Google Scholar] [CrossRef]
- Kohutek, Z.A.; Yamada, Y.; Chan, T.A.; Brennan, C.W.; Tabar, V.; Gutin, P.H.; Yang, T.J.; Rosenblum, M.K.; Ballangrud, Å.; Young, R.J.; et al. Long-term risk of radionecrosis and imaging changes after stereotactic radiosurgery for brain metastases. J. Neurooncol. 2015, 125, 149–156. [Google Scholar] [CrossRef] [Green Version]
- Han, J.H.; Kim, D.G.; Kim, C.Y.; Chung, H.T.; Jung, H.W. Stereotactic radiosurgery for large brain metastases. Prog. Neurol. Surg. 2012, 25, 248–260. [Google Scholar] [CrossRef]
- Remick, J.S.; Kowalski, E.; Khairnar, R.; Sun, K.; Morse, E.; Cherng, H.R.; Poirier, Y.; Lamichhane, N.; Becker, S.J.; Chen, S.; et al. A multi-center analysis of single-fraction versus hypofractionated stereotactic radiosurgery for the treatment of brain metastasis. Radiat. Oncol. 2020, 15, 128. [Google Scholar] [CrossRef]
- Prabhu, R.S.; Press, R.H.; Patel, K.R.; Boselli, D.M.; Symanowski, J.T.; Lankford, S.P.; McCammon, R.J.; Moeller, B.J.; Heinzerling, J.H.; Fasola, C.E.; et al. Single-Fraction Stereotactic Radiosurgery (SRS) Alone Versus Surgical Resection and SRS for Large Brain Metastases: A Multi-institutional Analysis. Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Loo, M.; Pin, Y.; Thierry, A.; Clavier, J.B. Single-fraction radiosurgery versus fractionated stereotactic radiotherapy in patients with brain metastases: A comparative study. Clin. Exp. Metastasis 2020, 37, 425–434. [Google Scholar] [CrossRef] [PubMed]
- Chin, L.S.; Ma, L.; DiBiase, S. Radiation necrosis following gamma knife surgery: A case-controlled comparison of treatment parameters and long-term clinical follow up. J. Neurosurg. 2001, 94, 899–904. [Google Scholar] [CrossRef]
- Inoue, H.K.; Sato, H.; Seto, K.; Torikai, K.; Suzuki, Y.; Saitoh, J.; Noda, S.E.; Nakano, T. Five-fraction CyberKnife radiotherapy for large brain metastases in critical areas: Impact on the surrounding brain volumes circumscribed with a single dose equivalent of 14 Gy (V14) to avoid radiation necrosis. J. Radiat. Res. 2014, 55, 334–342. [Google Scholar] [CrossRef] [Green Version]
- Inoue, H.K.; Seto, K.; Nozaki, A.; Torikai, K.; Suzuki, Y.; Saitoh, J.; Noda, S.E.; Nakano, T. Three-fraction CyberKnife radiotherapy for brain metastases in critical areas: Referring to the risk evaluating radiation necrosis and the surrounding brain volumes circumscribed with a single dose equivalence of 14 Gy (V14). J. Radiat. Res. 2013, 54, 727–735. [Google Scholar] [CrossRef] [Green Version]
- Voges, J.; Treuer, H.; Sturm, V.; Büchner, C.; Lehrke, R.; Kocher, M.; Staar, S.; Kuchta, J.; Müller, R.P. Risk analysis of linear accelerator radiosurgery. Int. J. Radiat. Oncol. Biol. Phys. 1996, 36, 1055–1063. [Google Scholar] [CrossRef] [PubMed]
- Flickinger, J.C.; Kondziolka, D.; Pollock, B.E.; Maitz, A.H.; Lunsford, L.D. Complications from arteriovenous malformation radiosurgery: Multivariate analysis and risk modeling. Int. J. Radiat. Oncol. Biol. Phys. 1997, 38, 485–490. [Google Scholar] [CrossRef]
- Nakamura, J.L.; Verhey, L.J.; Smith, V.; Petti, P.L.; Lamborn, K.R.; Larson, D.A.; Wara, W.M.; McDermott, M.W.; Sneed, P.K. Dose conformity of gamma knife radiosurgery and risk factors for complications. Int. J. Radiat. Oncol. Biol. Phys. 2001, 51, 1313–1319. [Google Scholar] [CrossRef]
- Minniti, G.; Capone, L.; Nardiello, B.; El Gawhary, R.; Raza, G.; Scaringi, C.; Bianciardi, F.; Gentile, P.; Paolini, S. Neurological outcome and memory performance in patients with 10 or more brain metastases treated with frameless linear accelerator (LINAC)-based stereotactic radiosurgery. J. Neurooncol. 2020, 148, 47–55. [Google Scholar] [CrossRef]
- Wowra, B.; Muacevic, A.; Tonn, J. Quality of radiosurgery for single brain metastases with respect to treatment technology: A matched-pair analysis. J. Neuro-Oncol. 2009, 94, 69–77. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group 1 (<5 mm) | Group 2 (5–10 mm) | Group 3 (>10–15 mm) | Group 4 (>15 mm) | |
|---|---|---|---|---|
| Mean Distance to Closest Neighbor (mm) | 7.5 | 10.2 | 15.9 | 22.2 |
| Median Distance to Closest Neighbor (mm) | 7.1 | 9.5 | 15.1 | 19.6 |
| Range Distance to Closest Neighbor (mm) | (0.5–22.7) | (1–32.8) | (6–28.3) | (13.5–43.9) |
| Group 1 (<5 mm) | Group 2 (5–10 mm) | Group 3 (>10–15 mm) | Group 4 (>15 mm) | |||||
|---|---|---|---|---|---|---|---|---|
| GK | CK | GK | CK | GK | CK | GK | CK | |
| Number of lesions | 177 | 135 | 57 | 35 | 29 | 18 | 10 | 8 |
| Total GTV Volume (cc) | 3.62 | 2.322 | 20.366 | 12.088 | 30.252 | 18.244 | 57.955 | 41.524 |
| Mean GTV Volume (cc) | 0.02 ± 0.017 | 0.017 ± 0.016 | 0.357 ± 0.141 | 0.352 ± 0.16 | 1.043 ± 0.259 | 1.014 ± 0.261 | 5.974 ± 1.776 | 5.188 ± 1.348 |
| GTV Volume Range (cc) | (0.004, 0.081) | (0.001, 0.064) | (0.116, 0.619) | (0.116, 0.619) | (0.53, 1.567) | (0.53, 1.763) | (3.535, 8.922) | (3.535, 6.881) |
| Mean GTV Dimension (mm) | 3.6 ± 1.0 | 3.4 ± 1.0 | 9.0 ± 1.1 | 8.9 ± 1.3 | 13.8 ± 1.1 | 13.8 ± 1.2 | 23.4 ± 2.1 | 23.0 ± 2.2 |
| GTV Dimension Range (mm) | (1.8, 5) | (1.8, 5) | (6.1, 9.9) | (6.1, 9.9) | (10.8, 14.9) | (10.8, 14.9) | (19.8, 26.1) | (19.8, 26.1) |
| Median GTV Dimension (mm) | 3.8 | 3.2 | 9.8 | 9.8 | 13.8 | 14.3 | 24.0 | 23.4 |
| Study | System Used | Parameter | Volume Constraint | RN Risk/Comments | |
|---|---|---|---|---|---|
| Brain–normal tissue dose received | Miyawaki et al., 1999 (AVMs) [33] | LINAC non-CK | V16 Gy | >14 cc | 72% MR changes; 22% RN resected |
| Voges et al., 1996 (Mixed) [48] | LINAC non-CK | V10 Gy | >10 cc | 23.7% | |
| Flickinger et al., 1997 (AVMs) [49] | GK | V12 Gy | - | 10.7% | |
| Chin et al., 2001 (Mixed) [45] | GK | V10 Gy | - | - | |
| Koryto et al., 2006 (BM) [36] | GK | V12 Gy | >10 cc | >50% | |
| Blonigen et al., 2010 (BM) [38] | LINAC non-CK | V10 Gy | >10.5 cc | 35% | |
| V12 Gy | 7.85 cc | ||||
| V8 Gy and V16 Gy | - | Showed most predictive for SRN (p < 0.0001) | |||
| Minniti et al., 2011 (BM) [37] | LINAC non-CK | V10 Gy | >12.3 cc | 47% | |
| V12 Gy | >10.9 cc | 47% | |||
| V12 Gy | 6–10.9 cc | 24% | |||
| Ohtakara et al. 2012 (BM) [34] | LINAC non-CK | V15 Gy | 5.20 cc | Presented as cut-off in patients with no prior WBRT | |
| V22 Gy | 2.14 cc | ||||
| Inoue et al., 2013 (BM) [47] | CK | V14 Gy | ≥7 cc | 12.8%—SFED (from 5 fractions) | |
| Inoue et al., 2014 (BM) [46] | CK | V14 Gy | ≥7 cc | 6.2%—SFED (from 3 fractions) | |
| Peng et al., 2019 (BM) [35] | - | V14 Gy | 5 cc | 0.4% | |
| 10 cc | 0.8% | ||||
| 20 cc | 3.4% | ||||
| Milano et al., 2021 (AVMs and BM) [31] | GK, LINAC | V12 Gy | 5 cc | 10% | |
| V12 Gy | 10 cc | 15% | |||
| V12 Gy | >15 cc | 20% | |||
| Diameter of BMs | Shaw et al., 2000 (BM, PBT) [39] | GK, LINAC | >2.1-4 cm | x7.3–16 | |
| Kohutek et al., 2015 (BM) [40] | LINAC non-CK | >1.5 cm | 37.5% | ||
| Minniti et al., 2016 (BM) [51] | LINAC non-CK | >2 cm | 20% | ||
| >3 cm | 33% | ||||
| Mohammadi et al., 2017 (BM) [13] | GK | 1–2 cm vs. <1 cm | x2.1 (RRN); x4.8 (SRN) | ||
| Remick et al., 2020 (BM) [42] | LINAC non-CK | >2 cm | 10% | ||
| Volume of BMs | Nakamura et al., 2001 (Mixed) [50] | GK | 0.67–3 cc; 3.2–8.6 cc; and 8.7–95.1 cc | 3%; 7%; and 9% | |
| Han et al., 2012 [41] | - | 22.4 cc (median) | 38.8% for large BM, low doses (13.8 Gy) | ||
| Prabhu et al., 2017 (BM) [43] | - | 5.9 cc | 17.2% | ||
| Mohammadi et al., 2017 (BM) [13] | GK | >0.1 cc | x2.1 (RRN); x4 (SRN) | ||
| Loo et al., 2020 (BM) [44] | - | - | HR 1.09, 95% CI (1.01–1.18); p = 0.02 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
La Rosa, A.; Wieczorek, D.J.J.; Tolakanahalli, R.; Lee, Y.C.; Kutuk, T.; Tom, M.C.; Hall, M.D.; McDermott, M.W.; Mehta, M.P.; Gutierrez, A.N.; et al. Dosimetric Impact of Lesion Number, Size, and Volume on Mean Brain Dose with Stereotactic Radiosurgery for Multiple Brain Metastases. Cancers 2023, 15, 780. https://doi.org/10.3390/cancers15030780
La Rosa A, Wieczorek DJJ, Tolakanahalli R, Lee YC, Kutuk T, Tom MC, Hall MD, McDermott MW, Mehta MP, Gutierrez AN, et al. Dosimetric Impact of Lesion Number, Size, and Volume on Mean Brain Dose with Stereotactic Radiosurgery for Multiple Brain Metastases. Cancers. 2023; 15(3):780. https://doi.org/10.3390/cancers15030780
Chicago/Turabian StyleLa Rosa, Alonso, D Jay J. Wieczorek, Ranjini Tolakanahalli, Yongsook C. Lee, Tugce Kutuk, Martin C. Tom, Matthew D. Hall, Michael W. McDermott, Minesh P. Mehta, Alonso N. Gutierrez, and et al. 2023. "Dosimetric Impact of Lesion Number, Size, and Volume on Mean Brain Dose with Stereotactic Radiosurgery for Multiple Brain Metastases" Cancers 15, no. 3: 780. https://doi.org/10.3390/cancers15030780
APA StyleLa Rosa, A., Wieczorek, D. J. J., Tolakanahalli, R., Lee, Y. C., Kutuk, T., Tom, M. C., Hall, M. D., McDermott, M. W., Mehta, M. P., Gutierrez, A. N., & Kotecha, R. (2023). Dosimetric Impact of Lesion Number, Size, and Volume on Mean Brain Dose with Stereotactic Radiosurgery for Multiple Brain Metastases. Cancers, 15(3), 780. https://doi.org/10.3390/cancers15030780