
Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy with Intra-Operative Radiotherapy for Patients with Locally Advanced or Locally Recurrent Rectal Cancer and Peritoneal Metastases
 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Treatment
3.2. Safety
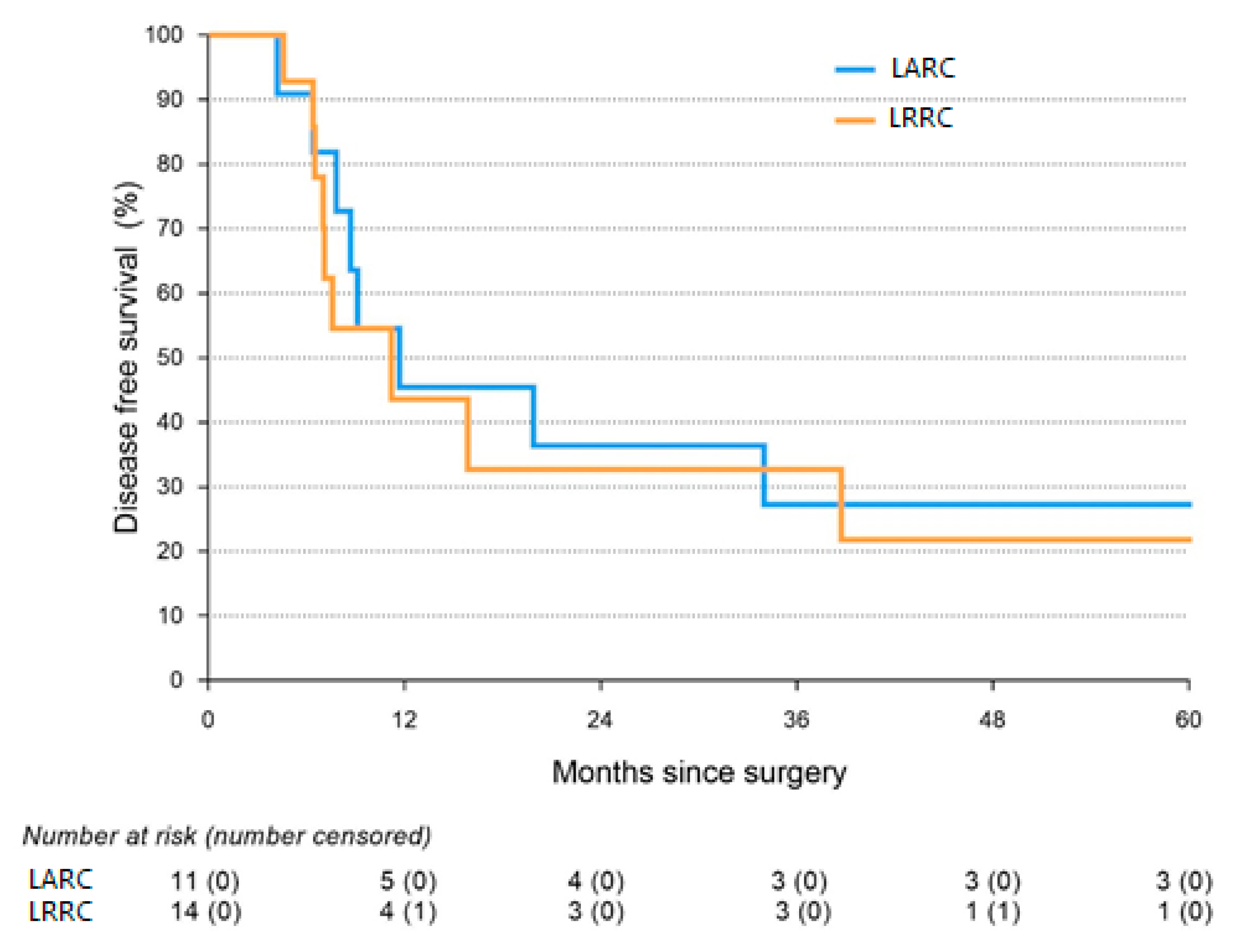
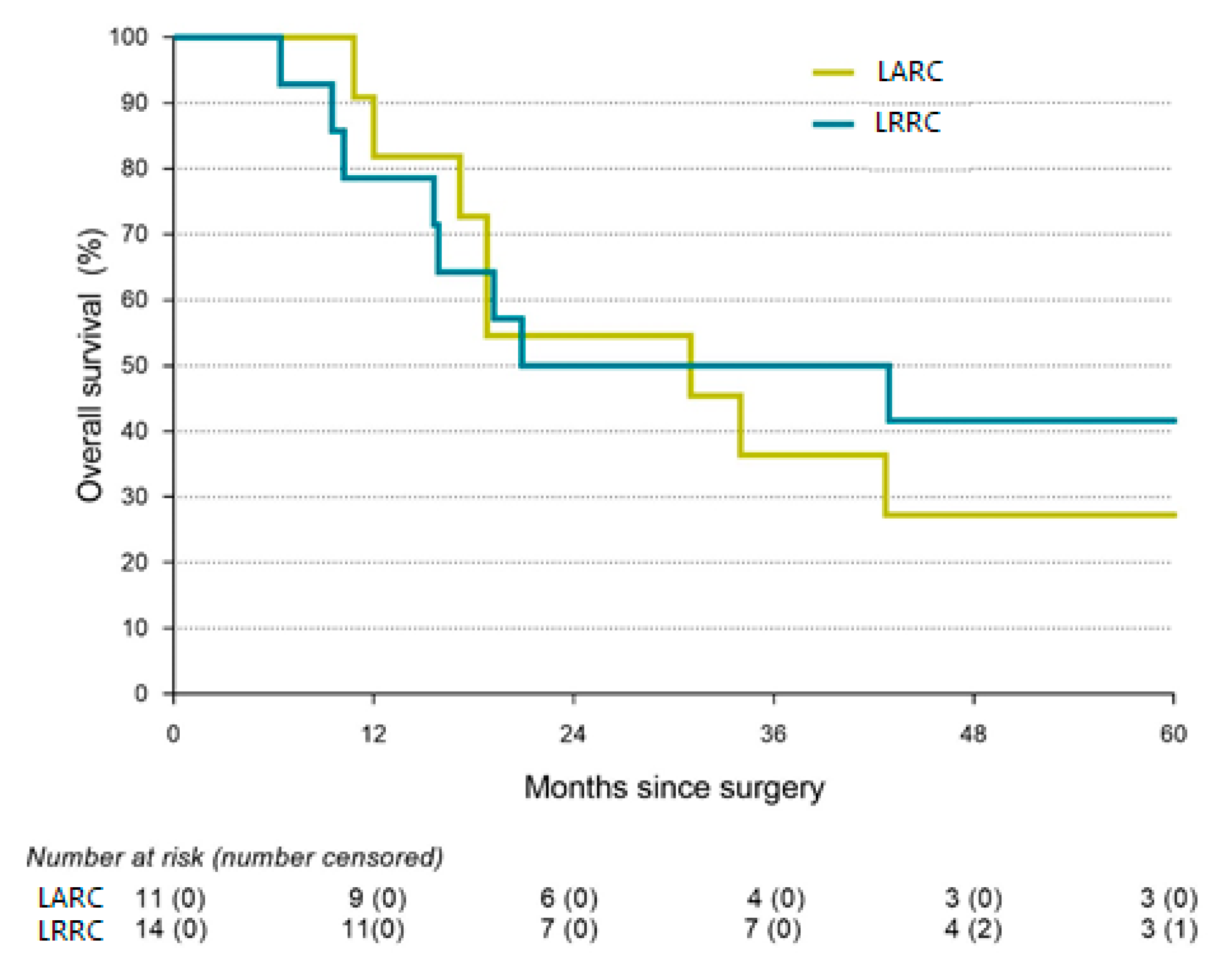
3.3. Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Araghi, M.; Soerjomataram, I.; Jenkins, M.; Brierley, J.; Morris, E.; Bray, F.; Arnold, M. Global trends in colorectal cancer mortality: Projections to the year 2035. Int. J. Cancer 2019, 144, 2992–3000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegel, R.L.; Miller, K.D.; Goding Sauer, A.; Fedewa, S.A.; Butterly, L.F.; Anderson, J.C.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 145–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Wilt, J.H.; Vermaas, M.; Ferenschild, F.T.; Verhoef, C. Management of locally advanced primary and recurrent rectal cancer. Clin. Colon Rectal Surg. 2007, 20, 255–263. [Google Scholar] [CrossRef] [Green Version]
- Kokelaar, R.F.; Evans, M.D.; Davies, M.; Harris, D.A.; Beynon, J. Locally advanced rectal cancer: Management challenges. Onco Targets Ther. 2016, 9, 6265–6272. [Google Scholar] [CrossRef] [Green Version]
- Beyond TME Collaborative. Consensus statement on the multidisciplinary management of patients with recurrent and primary rectal cancer beyond total mesorectal excision planes. J. Br. Surg. 2013, 100, E1–E33. [Google Scholar] [CrossRef]
- Collaborative, T.P. Factors affecting outcomes following pelvic exenteration for locally recurrent rectal cancer. J. Br. Surg. 2018, 105, 650–657. [Google Scholar] [CrossRef] [PubMed]
- Lurvink, R.J.; Bakkers, C.; Rijken, A.; van Erning, F.N.; Nienhuijs, S.W.; Burger, J.W.; Creemers, G.J.; Verhoef, C.; Lemmens, V.E.; De Hingh, I.H. Increase in the incidence of synchronous and metachronous peritoneal metastases in patients with colorectal cancer: A nationwide study. Eur. J. Surg. Oncol. 2021, 47, 1026–1033. [Google Scholar] [CrossRef] [PubMed]
- IKNL, Integraal kankercentrum Nederland; Darmkanker. Cijfers Darmkanker. Available online: https://iknl.nl (accessed on 31 October 2022).
- Dresen, R.C.; Gosens, M.J.; Martijn, H.; Nieuwenhuijzen, G.A.; Creemers, G.J.; Daniels-Gooszen, A.W.; van den Brule, A.J.; van den Berg, H.A.; Rutten, H.J. Radical resection after IORT-containing multimodality treatment is the most important determinant for outcome in patients treated for locally recurrent rectal cancer. Ann. Surg. Oncol. 2008, 15, 1937–1947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferenschild, F.T.; Vermaas, M.; Nuyttens, J.J.; Graveland, W.J.; Marinelli, A.W.; van der Sijp, J.R.; Wiggers, T.; Verhoef, C.; Eggermont, A.M.; de Wilt, J.H. Value of intraoperative radiotherapy in locally advanced rectal cancer. Dis. Colon Rectum 2006, 49, 1257–1265. [Google Scholar] [CrossRef]
- Glynne-Jones, R.; Kronfli, M. Locally advanced rectal cancer: A comparison of management strategies. Drugs 2011, 71, 1153–1177. [Google Scholar] [CrossRef]
- Goéré, D.; Souadka, A.; Faron, M.; Cloutier, A.S.; Viana, B.; Honoré, C.; Dumont, F.; Elias, D. Extent of colorectal peritoneal carcinomatosis: Attempt to define a threshold above which HIPEC does not offer survival benefit: A comparative study. Ann. Surg. Oncol. 2015, 22, 2958–2964. [Google Scholar] [CrossRef] [PubMed]
- Simkens, G.A.; van Oudheusden, T.R.; Nieboer, D.; Steyerberg, E.W.; Rutten, H.J.; Luyer, M.D.; Nienhuijs, S.W.; de Hingh, I.H. Development of a Prognostic Nomogram for Patients with Peritoneally Metastasized Colorectal Cancer Treated with Cytoreductive Surgery and HIPEC. Ann. Surg. Oncol. 2016, 23, 4214–4221. [Google Scholar] [CrossRef] [PubMed]
- Steffen, T.; Eden, J.; Bijelic, L.; Glatzer, M.; Glehen, O.; Goéré, D.; de Hingh, I.; Li, Y.; Moran, B.; Morris, D.; et al. Patient Selection for Hyperthermic Intraperitoneal Chemotherapy in Patients With Colorectal Cancer: Consensus on Decision Making Among International Experts. Clin. Colorectal. Cancer 2020, 19, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Van Oudheusden, T.; Braam, H.; Luyer, M.; Wiezer, M.; van Ramshorst, B.; Nienhuijs, S.; de Hingh, I. Peritoneal cancer patients not suitable for cytoreductive surgery and HIPEC during explorative surgery: Risk factors, treatment options, and prognosis. Ann. Surg. Oncol. 2015, 22, 1236–1242. [Google Scholar] [CrossRef] [PubMed]
- Ihemelandu, C.U.; McQuellon, R.; Shen, P.; Stewart, J.H.; Votanopoulos, K.; Levine, E.A. Predicting postoperative morbidity following cytoreductive surgery with hyperthermic intraperitoneal chemotherapy (CS+HIPEC) with preoperative FACT-C (Functional Assessment of Cancer Therapy) and patient-rated performance status. Ann. Surg. Oncol. 2013, 20, 3519–3526. [Google Scholar] [CrossRef]
- Jacquet, P.; Sugarbaker, P. Current methodologies for clinical assessment of patients with peritoneal carcinomatosis. J. Exp. Clin. Cancer Res. 1996, 15, 49–58. [Google Scholar]
- Kranenburg, O.; Speeten, K.V.D.; Hingh, I.D. Peritoneal metastases from colorectal cancer: Defining and addressing the challenges. Front. Oncol. 2021, 11, 650098. [Google Scholar] [CrossRef]
- Klaver, Y.L.; Lemmens, V.E.; Nienhuijs, S.W.; Nieuwenhuijzen, G.A.; Rutten, H.J.; de Hingh, I.H. Intraoperative radiotherapy and cytoreductive surgery with hyperthermic intraperitoneal chemotherapy. Five consecutive case reports of locally advanced rectal cancer with synchronous peritoneal carcinomatosis. Strahlenther. Onkol. 2013, 189, 256–260. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Guren, M.G.; Undseth, C.; Rekstad, B.L.; Brændengen, M.; Dueland, S.; Spindler, K.L.; Glynne-Jones, R.; Tveit, K.M. Reirradiation of locally recurrent rectal cancer: A systematic review. Radiother. Oncol. 2014, 113, 151–157. [Google Scholar] [CrossRef] [Green Version]
- Voogt, E.L.K.; van Rees, J.M.; Hagemans, J.A.W.; Rothbarth, J.; Nieuwenhuijzen, G.A.P.; Cnossen, J.S.; Peulen, H.M.U.; Dries, W.J.F.; Nuyttens, J.; Kolkman-Deurloo, I.K.; et al. Intraoperative Electron Beam Radiation Therapy (IOERT) versus High-Dose-Rate Intraoperative Brachytherapy (HDR-IORT) in Patients with an R1 Resection for Locally Advanced or Locally Recurrent Rectal Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 1032–1043. [Google Scholar] [CrossRef] [PubMed]
- Quénet, F.; Elias, D.; Roca, L.; Goéré, D.; Ghouti, L.; Pocard, M.; Facy, O.; Arvieux, C.; Lorimier, G.; Pezet, D.; et al. Cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy versus cytoreductive surgery alone for colorectal peritoneal metastases (PRODIGE 7): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 256–266. [Google Scholar] [CrossRef] [PubMed]
- van de Vlasakker, V.C.J.; Lurvink, R.J.; Cashin, P.H.; Ceelen, W.; Deraco, M.; Goéré, D.; González-Moreno, S.; Lehmann, K.; Li, Y.; Moran, B.; et al. The impact of PRODIGE 7 on the current worldwide practice of CRS-HIPEC for colorectal peritoneal metastases: A web-based survey and 2021 statement by Peritoneal Surface Oncology Group International (PSOGI). Eur. J. Surg. Oncol. 2021, 47, 2888–2892. [Google Scholar] [CrossRef] [PubMed]
- Verwaal, V.J.; Bruin, S.; Boot, H.; Van Slooten, G.; Van Tinteren, H. 8-year follow-up of randomized trial: Cytoreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy in patients with peritoneal carcinomatosis of colorectal cancer. Ann. Surg. Oncol. 2008, 15, 2426–2432. [Google Scholar] [CrossRef]
- Verwaal, V.J.; van Ruth, S.; de Bree, E.; van Slooten, G.W.; van Tinteren, H.; Boot, H.; Zoetmulder, F.A. Randomized trial of cytoreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy and palliative surgery in patients with peritoneal carcinomatosis of colorectal cancer. J. Clin. Oncol. 2003, 21, 3737–3743. [Google Scholar] [CrossRef]
- Bakkers, C.; van Erning, F.N.; Rovers, K.P.; Nienhuijs, S.W.; Burger, J.W.; Lemmens, V.E.; Aalbers, A.G.; Kok, N.F.; Boerma, D.; Brandt, A.R.; et al. Long-term survival after hyperthermic intraperitoneal chemotherapy using mitomycin C or oxaliplatin in colorectal cancer patients with synchronous peritoneal metastases: A nationwide comparative study. Eur. J. Surg. Oncol. 2020, 46, 1902–1907. [Google Scholar] [CrossRef]
- Simkens, G.A.; van Oudheusden, T.R.; Braam, H.J.; Wiezer, M.J.; Nienhuijs, S.W.; Rutten, H.J.; van Ramshorst, B.; de Hingh, I.H. Cytoreductive surgery and HIPEC offers similar outcomes in patients with rectal peritoneal metastases compared to colon cancer patients: A matched case control study. J. Surg. Oncol. 2016, 113, 548–553. [Google Scholar] [CrossRef]
- Azzam, A.Z.; Amin, T.M. Combined Intraoperative Radiotherapy (IORT) and Hyperthermic Intraperitoneal Chemotherapy (HIPEC) with Cytoreduction Surgery (CRS) as a Novel Approach in the Management of Resectable Pancreatic Cancer. Gulf J. Oncol. 2020, 1, 19–26. [Google Scholar]
- Dubois, J.B.; Bussieres, E.; Richaud, P.; Rouanet, P.; Becouarn, Y.; Mathoulin-Pélissier, S.; Saint-Aubert, B.; Ychou, M. Intra-operative radiotherapy of rectal cancer: Results of the French multi-institutional randomized study. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2011, 98, 298–303. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total Group (n = 30) | LARC (n = 14) | LRRC (n = 16) | p-Value | |
|---|---|---|---|---|
| Sex | ||||
| Male | 19 (63) | 9 (64) | 10 (62.5) | 0.919 |
| Female | 11 (37) | 5 (36) | 6 (37.5) | |
| Age | ||||
| (in years) | 57.9 ± 11 | 56.8 ± 10.8 | 58.8 ± 11.5 | 0.547 |
| ASA-score | ||||
| 1 | 2 (7) | 2 (14) | 0 (0) | 0.291 |
| 2 | 23 (77) | 10 (71) | 13 (81) | |
| 3 | 5 (17) | 2 (14) | 3 (19) | |
| Smoking | ||||
| No | 22 (73) | 9 (64) | 13 (81) | 0.295 |
| Yes | 8 (27) | 5 (36) | 3 (19) | |
| T-stage | ||||
| 2 | 1 (3) | 0 (0) | 1 (6) | 0.158 |
| 3 | 15 (50) | 5 (36) | 10 (63) | |
| 4 | 14 (47) | 9 (64) | 5 (31) | |
| N-stage | ||||
| 0 | 9 (30) | 3 (21) | 6 (38) | 0.141 |
| 1 | 13 (43) | 5 (36) | 8 (50) | |
| 2 | 8 (27) | 6 (43) | 2 (13) | |
| PCI-score | 7.4 ± 5.0 | 5.4 ± 5.0 | 9.1 ± 4.5 | 0.016 |
| Total Group (n = 30) | LARC (n = 14) | LRCC (n = 16) | p-Value | |
|---|---|---|---|---|
| Neoadjuvant treatment | ||||
| Radiotherapy | 2 (7) | 0 (0) | 2 (13) | 0.218 |
| Chemotherapy | 4 (13) | 1 (7) | 3 (19) | |
| Chemoradiotherapy | 24 (80) | 13 (93) | 11 (69) | |
| Duration of the operative procedure | ||||
| (in minutes) | 438 ± 75 | 427 ± 83 | 447 ± 68 | 1.000 |
| Blood loss | ||||
| (in mL) | 2062 ± 1328 | 1501 ± 937 | 2552 ± 1449 | 0.057 |
| IORT-dose | ||||
| 10 Gray | 27 (90) | 13 (93) | 14 (87.5) | 0.626 |
| 12.5 Gray | 3 (10) | 1 (7) | 2 (12.5) | |
| HIPEC-regime | ||||
| Mitomycin C | 28 (93) | 14 (100) | 14 (87.5) | 0.171 |
| Oxaliplatin | 2 (7) | 0 (0) | 2 (12.5) |
| Total Group (n = 30) | LARC (n = 14) | LRRC (n = 16) | p-Value | |
|---|---|---|---|---|
| Postoperative ICU stay (in days) | 1 (1–3) | 1 (1–2) | 1 (1–3) | 0.423 |
| Highest Severity of complications, according to the Clavien-Dindo classification | ||||
| CD 0–2 | 13 (43) | 9 (64) | 4 (25) | 0.010 |
| CD 3 | 12 (40) | 5 (36) | 7 (44) | |
| CD 4 | 5 (17) | 0 (0) | 5 (31) | |
| CD 5 | 0 (0) | 0 (0) | 0 (0) | |
| Readmission within 90 days | ||||
| No | 22 (73) | 10 (71) | 12 (75) | 0.825 |
| Yes | 8 (27) | 4 (29) | 4 (25) |
| Total Group (n = 25) | LARC (n = 11) | LRRC (n = 14) | p-Value | |
|---|---|---|---|---|
| Disease-free survival | ||||
| in months | 10.0 (6.4–38.7) | 11.7 (7.8– *) | 10.0 (6.4–38.7) | 0.123 |
| Site of recurrence ** | 0.723 | |||
| No recurrence | 8 | 4 | 4 | |
| Local | 1 | 0 | 1 | |
| Locoregional | 10 | 5 | 5 | |
| Systemic | 6 | 2 | 4 | |
| Overall survival | ||||
| in months | 31.0 (15.9–144.3) | 31.0 (17.2–144.3) | 20.9 (15.6–81.3) | 0.123 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van de Vlasakker, V.C.J.; van den Heuvel, T.B.M.; Rijken, A.; Nienhuijs, S.W.; Ketelaers, S.H.J.; Verrijssen, A.-S.E.; Rutten, H.J.; Nieuwenhuijzen, G.A.P.; Burger, J.W.A.; de Hingh, I.H.J.T. Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy with Intra-Operative Radiotherapy for Patients with Locally Advanced or Locally Recurrent Rectal Cancer and Peritoneal Metastases. Cancers 2023, 15, 858. https://doi.org/10.3390/cancers15030858
van de Vlasakker VCJ, van den Heuvel TBM, Rijken A, Nienhuijs SW, Ketelaers SHJ, Verrijssen A-SE, Rutten HJ, Nieuwenhuijzen GAP, Burger JWA, de Hingh IHJT. Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy with Intra-Operative Radiotherapy for Patients with Locally Advanced or Locally Recurrent Rectal Cancer and Peritoneal Metastases. Cancers. 2023; 15(3):858. https://doi.org/10.3390/cancers15030858
Chicago/Turabian Stylevan de Vlasakker, Vincent C. J., Teun B. M. van den Heuvel, Anouk Rijken, Simon W. Nienhuijs, Stijn H. J. Ketelaers, An-Sofie E. Verrijssen, Harm J. Rutten, Grard A. P. Nieuwenhuijzen, Jacobus W. A. Burger, and Ignace H. J. T. de Hingh. 2023. "Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy with Intra-Operative Radiotherapy for Patients with Locally Advanced or Locally Recurrent Rectal Cancer and Peritoneal Metastases" Cancers 15, no. 3: 858. https://doi.org/10.3390/cancers15030858
APA Stylevan de Vlasakker, V. C. J., van den Heuvel, T. B. M., Rijken, A., Nienhuijs, S. W., Ketelaers, S. H. J., Verrijssen, A. -S. E., Rutten, H. J., Nieuwenhuijzen, G. A. P., Burger, J. W. A., & de Hingh, I. H. J. T. (2023). Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy with Intra-Operative Radiotherapy for Patients with Locally Advanced or Locally Recurrent Rectal Cancer and Peritoneal Metastases. Cancers, 15(3), 858. https://doi.org/10.3390/cancers15030858