Real World Analysis of Quality of Life and Toxicity in Cancer Patients Treated with Hyperthermia Combined with Radio(chemo)therapy

 , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Hyperthermia Treatment
2.2.1. Superficial Hyperthermia Treatment
2.2.2. Deep Regional Hyperthermia Treatment
2.3. Electronic Patient Records
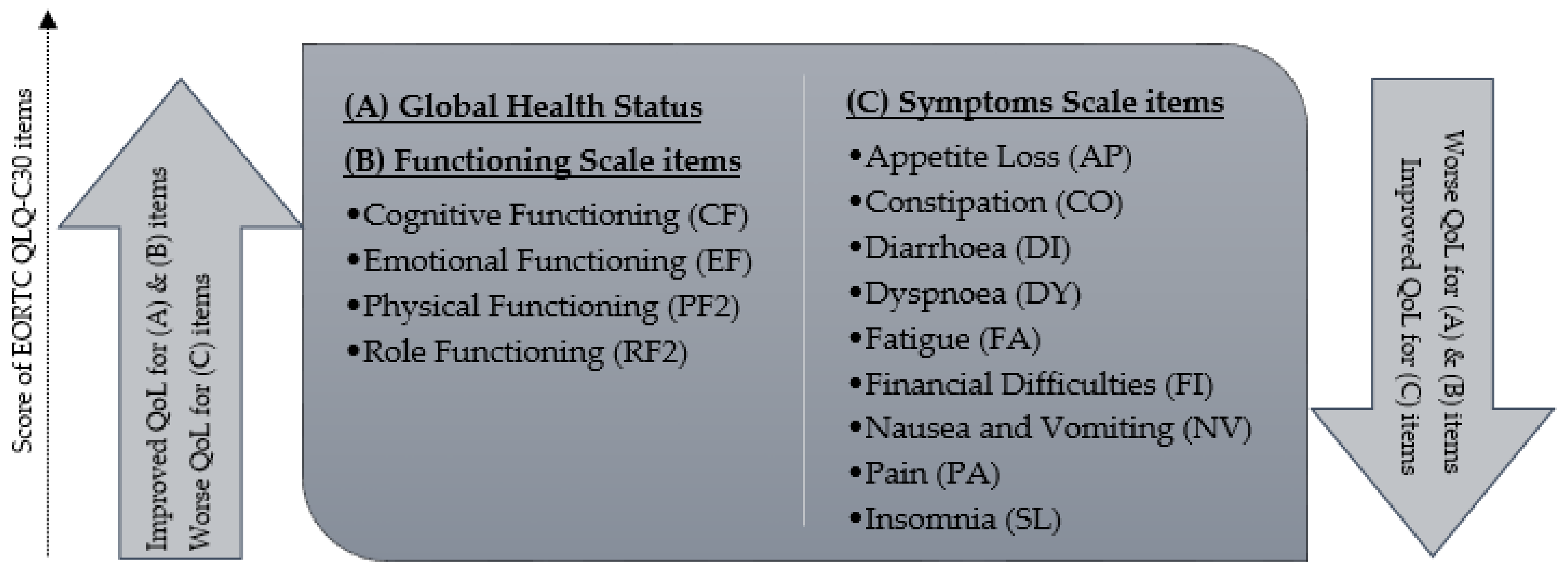
2.4. QoL Assessment and Secondary Outcomes
2.5. Statistical Analysis
3. Results
3.1. Patient and Treatment Characteristics
3.2. Subjective Assessment of EORTC QLQ-C30
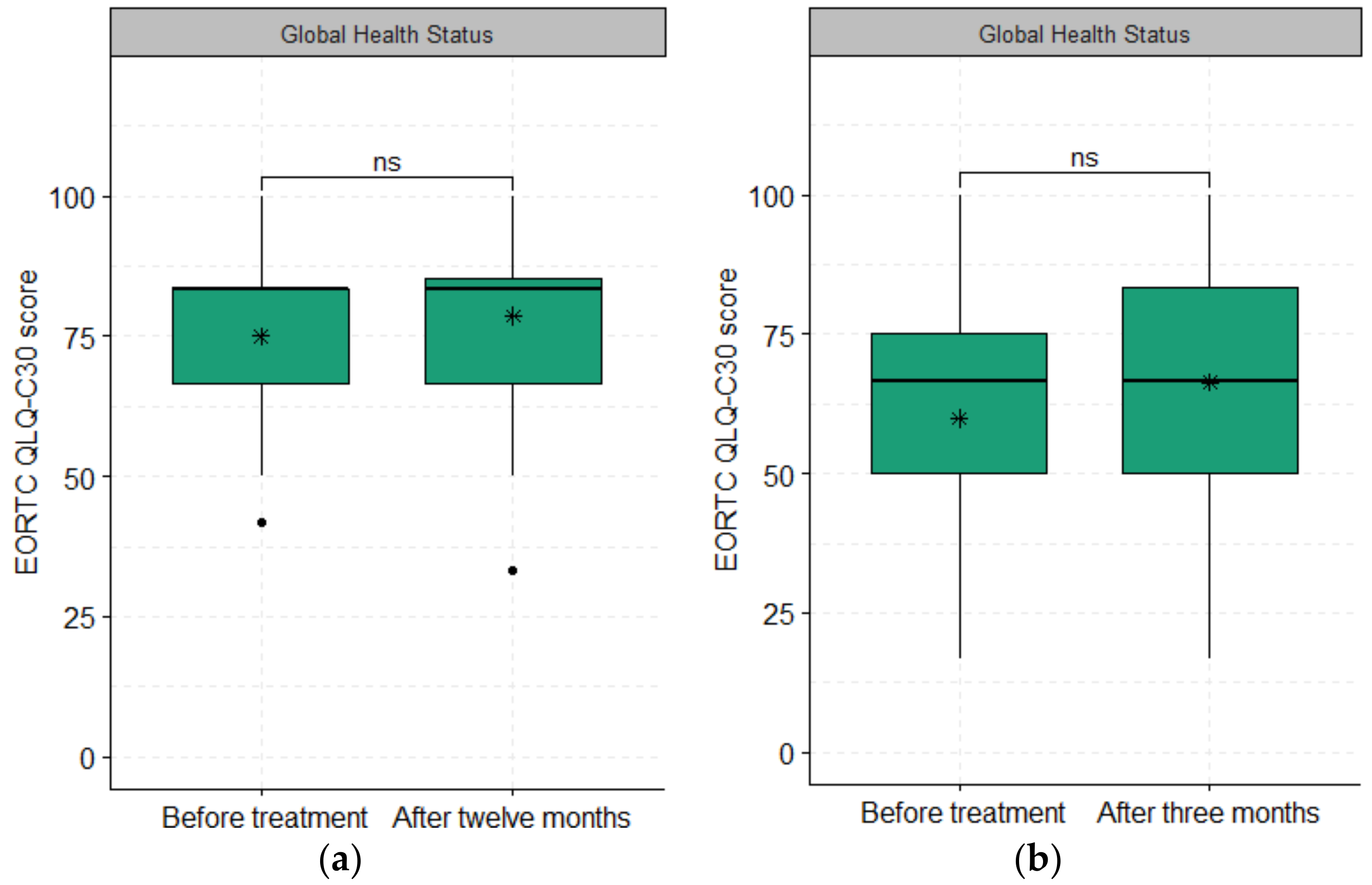
3.2.1. Global Health Status
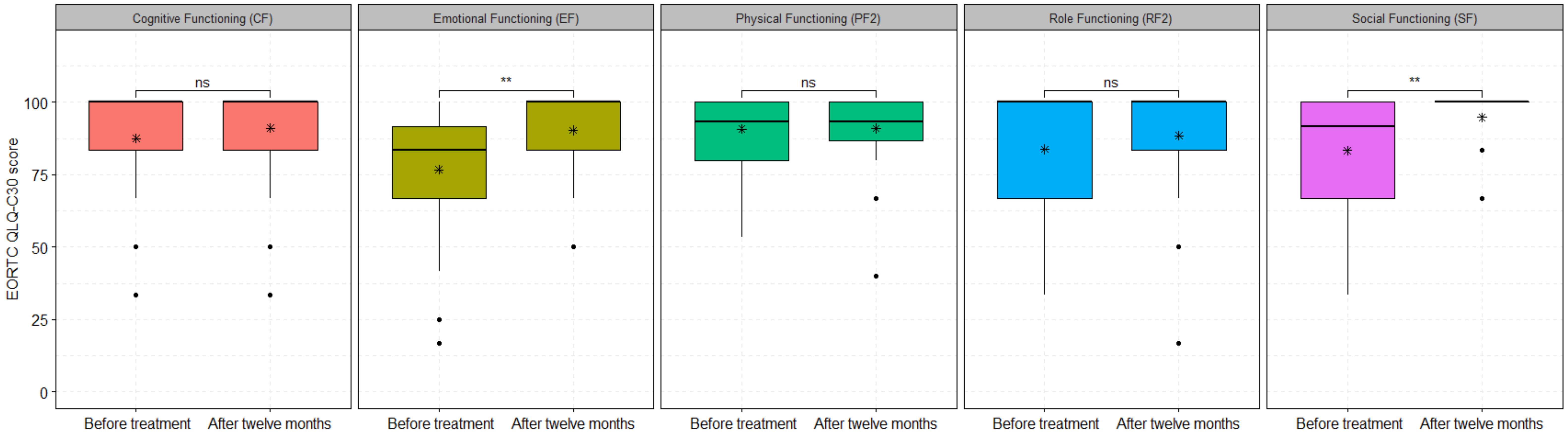
3.2.2. Functional Scales
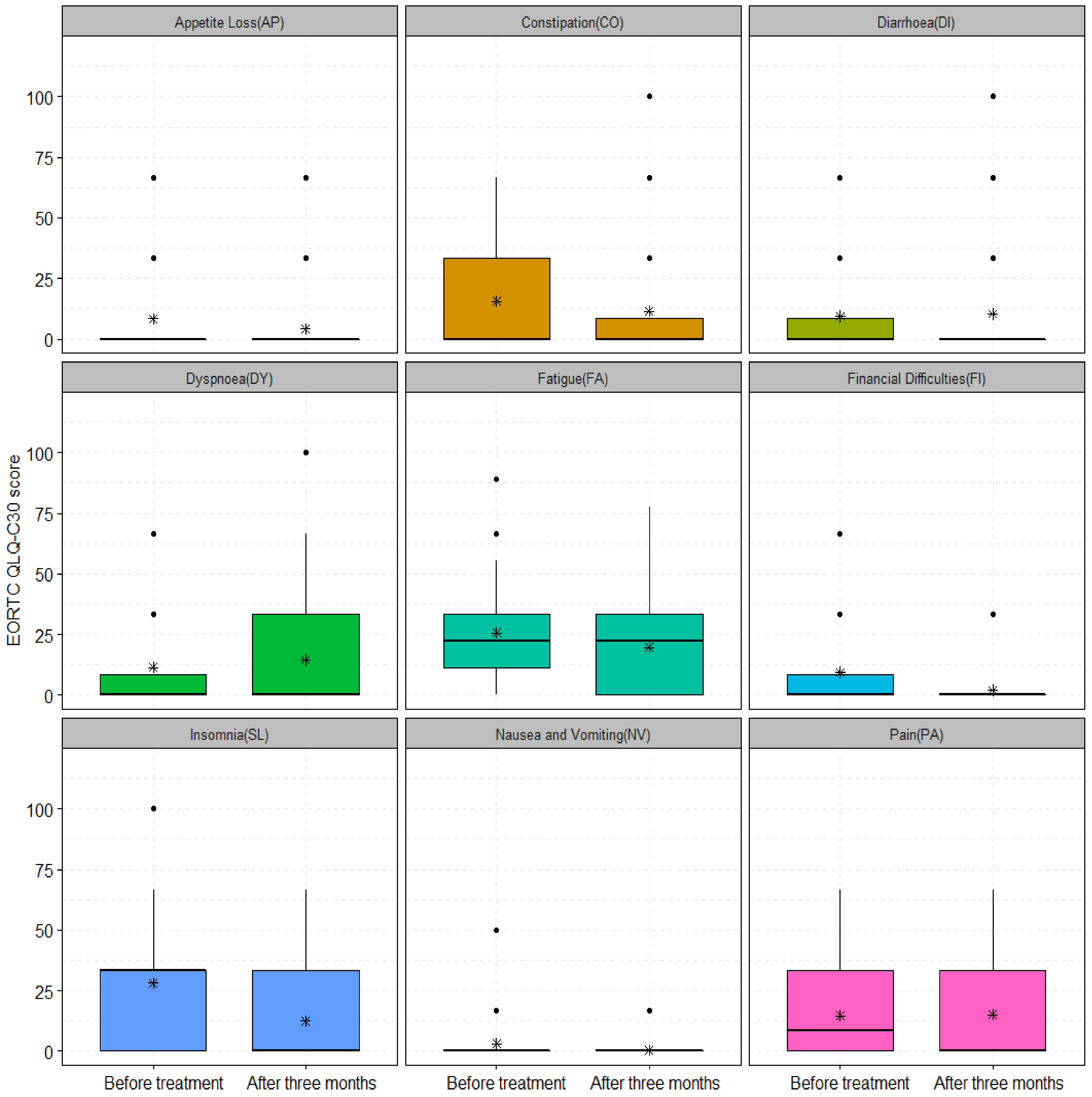
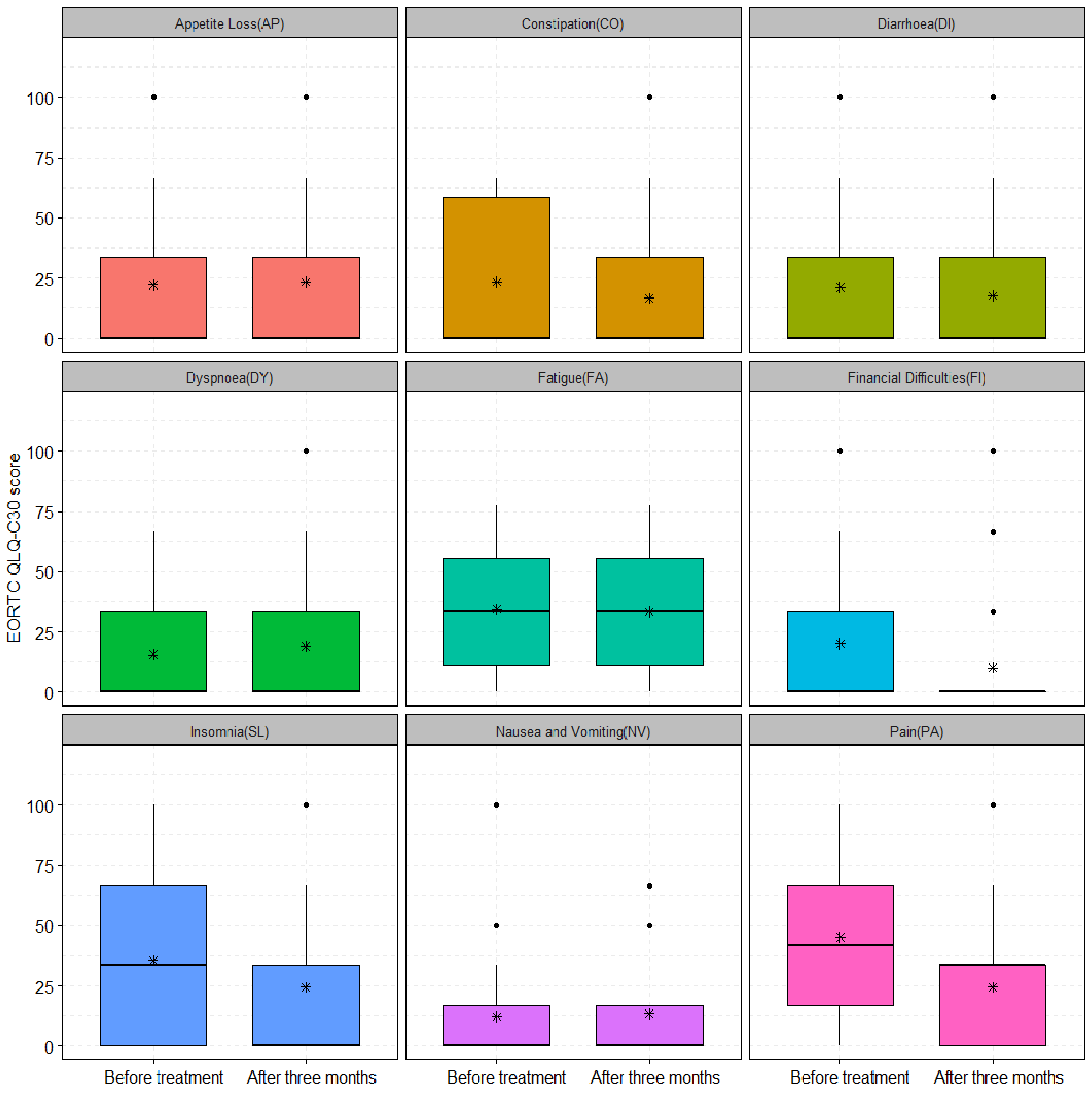
3.2.3. Symptoms Scales
3.3. Acute Toxicity Analysis
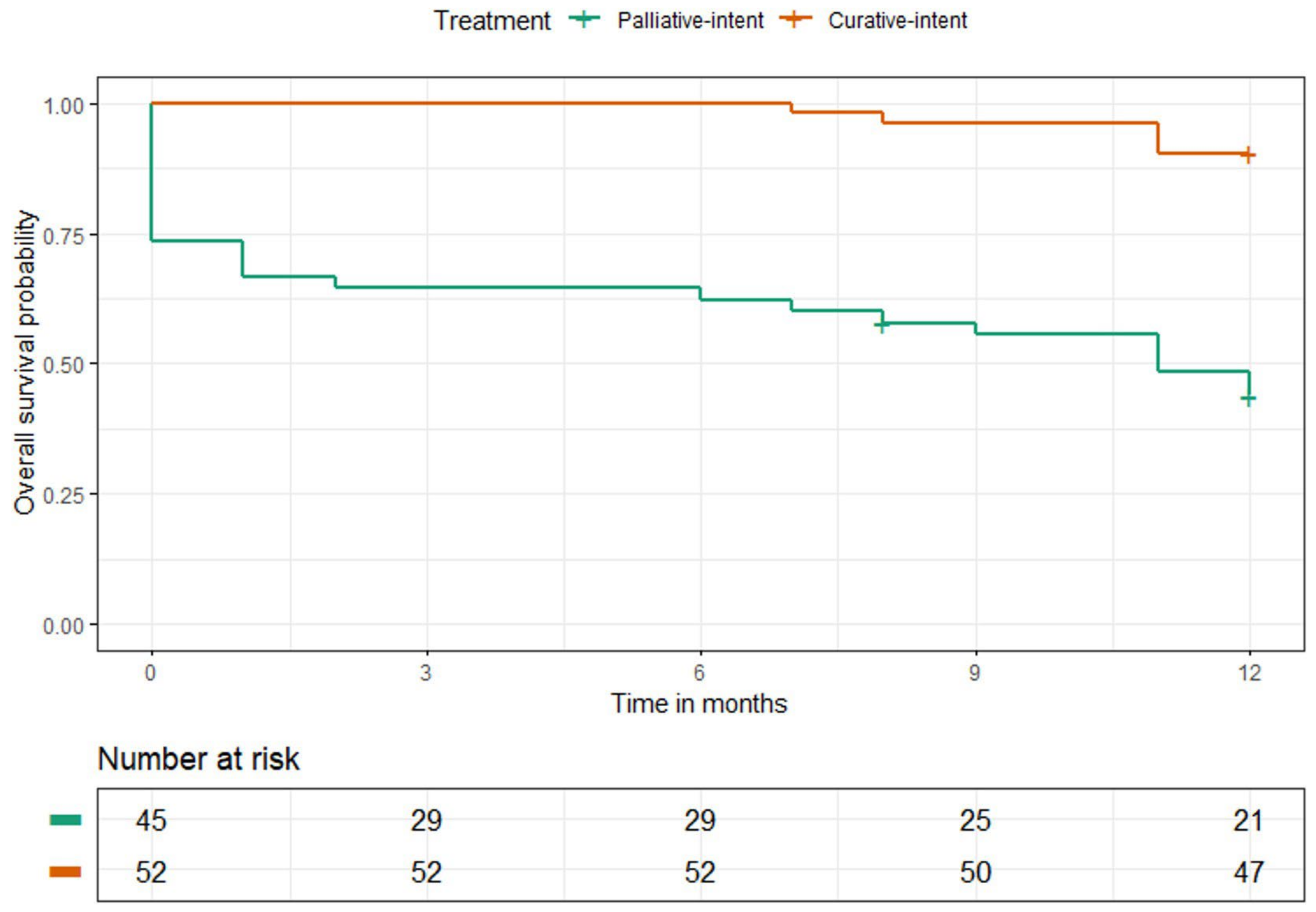
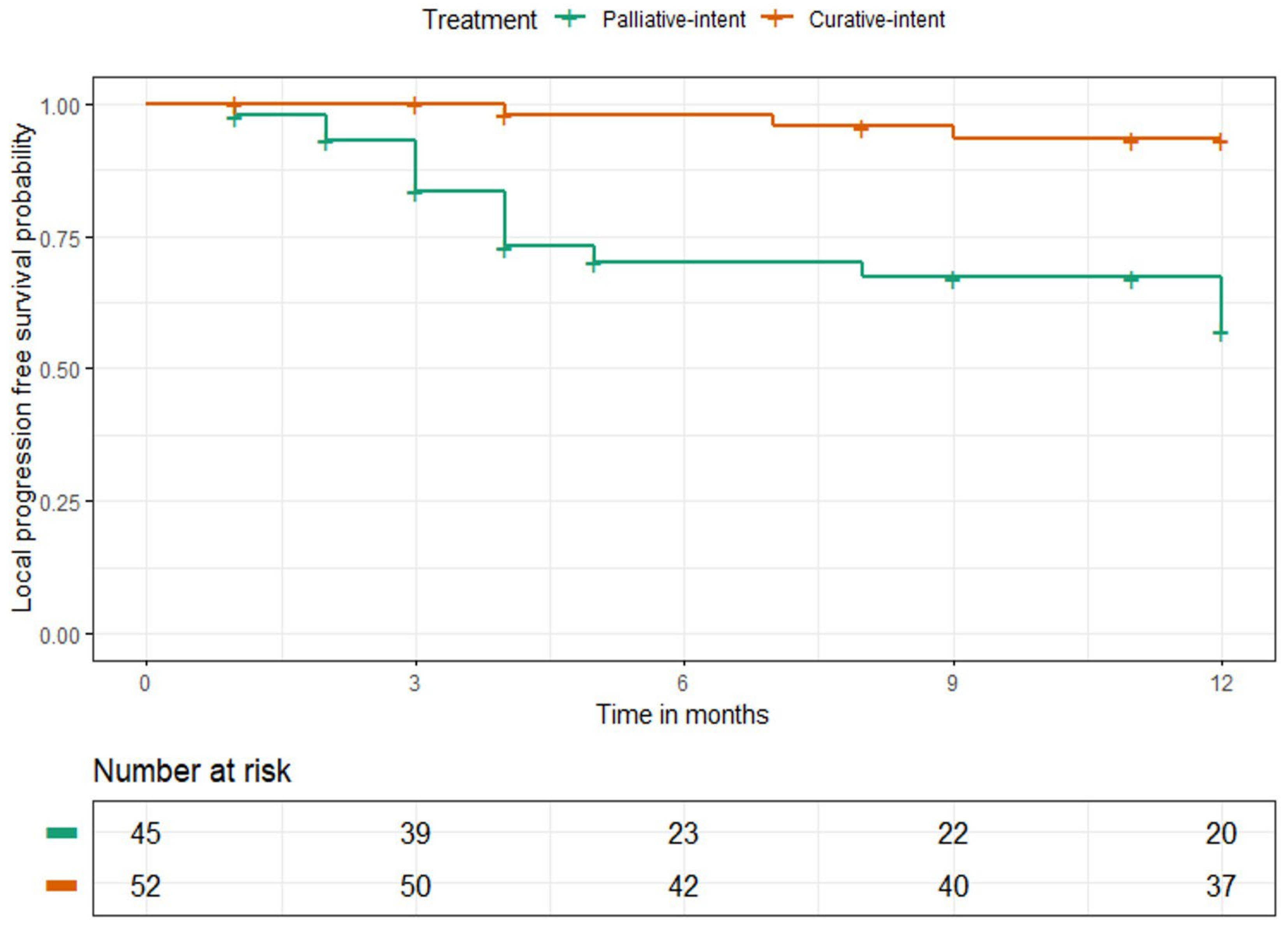
3.4. Survival Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wust, P.; Hildebrandt, B.; Sreenivasa, G.; Rau, B.; Gellermann, J.; Riess, H.; Felix, R.; Schlag, P.M. Hyperthermia in combined treatment of cancer. Lancet Oncol. 2002, 3, 487–497. [Google Scholar] [CrossRef] [PubMed]
- Oei, A.; Kok, H.; Oei, S.; Horsman, M.; Stalpers, L.; Franken, N.; Crezee, J. Molecular and biological rationale of hyperthermia as radio- and chemosensitizer. Adv. Drug Deliv. Rev. 2020, 163, 84–97. [Google Scholar] [CrossRef] [PubMed]
- Jones, E.L.; Oleson, J.R.; Prosnitz, L.R.; Samulski, T.V.; Vujaskovic, Z.; Yu, D.; Sanders, L.L.; Dewhirst, M.W. Randomized Trial of Hyperthermia and Radiation for Superficial Tumors. J. Clin. Oncol. 2005, 23, 3079–3085. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Overgaard, J.; Gonzalez, D.G.; Hulshof, M.C.C.H.; Arcangeli, G.; Dahl, O.; Mella, O.; Bentzen, S.M. Hyperthermia as an adjuvant to radiation therapy of recurrent or metastatic malignant melanoma. A multicentre randomized trial by the European Society for Hyperthermic Oncology. Int. J. Hyperth. 1996, 12, 3–20. [Google Scholar] [CrossRef]
- ICH Group; Vernon, C.C.; Hand, J.W.; Field, S.B.; Machin, D.; Whaley, J.B.; van der Zee, J.; van Putten, W.L.; van Rhoon, G.C.; van Dijk, J.D.; et al. Radiotherapy with or without hyperthermia in the treatment of superficial localized breast cancer: Results from five randomized controlled trials. International Collaborative Hyperthermia Group. Int. J. Radiat. Oncol. Biol. Phys. 1996, 35, 731–744. [Google Scholar] [CrossRef] [Green Version]
- Chi, M.-S.; Yang, K.-L.; Chang, Y.-C.; Ko, H.-L.; Lin, Y.-H.; Huang, S.-C.; Huang, Y.-Y.; Liao, K.-W.; Kondo, M.; Chi, K.-H. Comparing the Effectiveness of Combined External Beam Radiation and Hyperthermia Versus External Beam Radiation Alone in Treating Patients With Painful Bony Metastases: A Phase 3 Prospective, Randomized, Controlled Trial. Int. J. Radiat. Oncol. 2018, 100, 78–87. [Google Scholar] [CrossRef]
- Issels, R.D.; Lindner, L.H.; Verweij, J.; Wust, P.; Reichardt, P.; Schem, B.-C.; Abdel-Rahman, S.; Daugaard, S.; Salat, C.; Wendtner, C.-M.; et al. Neo-adjuvant chemotherapy alone or with regional hyperthermia for localised high-risk soft-tissue sarcoma: A randomised phase 3 multicentre study. Lancet Oncol. 2010, 11, 561–570. [Google Scholar] [CrossRef] [Green Version]
- Paulides, M.M.; Dobsicek Trefna, H.; Curto, S.; Rodrigues, D.B. Recent technological advancements in radiofrequency- and microwave-mediated hyperthermia for enhancing drug delivery. Adv. Drug Deliv. Rev. 2020, 163–164, 3–18. [Google Scholar] [CrossRef]
- Bruggmoser, G.; Bauchowitz, S.; Canters, R.; Crezee, H.; Ehmann, M.; Gellermann, J.; Lamprecht, U.; Lomax, N.; Messmer, M.B.; Ott, O.; et al. Guideline for the clinical application, documentation and analysis of clinical studies for regional deep hyperthermia: Quality management in regional deep hyperthermia. Strahlenther. Onkol. 2012, 188 (Suppl. 2), 198–211. [Google Scholar] [CrossRef] [Green Version]
- Kok, H.P.; Crezee, J. A comparison of the heating characteristics of capacitive and radiative superficial hyperthermia. Int. J. Hyperth. 2017, 33, 378–386. [Google Scholar] [CrossRef] [Green Version]
- Kamura, T.; Nielsen, O.S.; Overgaard, J.; Andersen, A.H. Development of thermotolerance during fractionated hyperthermia in a solid tumor in vivo. Cancer Res. 1982, 42, 1744–1748. [Google Scholar]
- Gabriele, P.; Orecchia, R.; Amichetti, M.; Valdagni, R. Hyperthermia and radiation therapy for inoperable or recurrent parotid carcinoma. A phase I/II study. Cancer 1995, 75, 908–913. [Google Scholar] [CrossRef]
- Masunaga, S.I.; Hiraoka, M.; Akuta, K.; Nishimura, Y.; Nagata, Y.; Jo, S.; Takahashi, M.; Abe, M.; Terachi, T.; Oishi, K.; et al. Phase I/II trial of preoperative thermoradiotherapy in the treatment of urinary bladder cancer. Int. J. Hyperth. 1994, 10, 31–40. [Google Scholar] [CrossRef]
- Bakker, A.; Valverde, C.P.T.; van Tienhoven, G.; Kolff, M.W.; Kok, H.P.; Slotman, B.J.; Konings, I.R.; Oei, A.L.; Oldenburg, H.S.; Rutgers, E.J.; et al. Post-operative re-irradiation with hyperthermia in locoregional breast cancer recurrence: Temperature matters. Radiother. Oncol. 2022, 167, 149–157. [Google Scholar] [CrossRef]
- Amichetti, M.; Graiff, C.; Fellin, G.; Pani, G.; Bolner, A.; Maluta, S.; Valdagni, R. Cisplatin, hyperthermia, and radiation (trimodal therapy) in patients with locally advanced head and neck tumors: A phase I-II study. Int. J. Radiat. Oncol. Biol. Phys. 1993, 26, 801–807. [Google Scholar] [CrossRef]
- Kroesen, M.; Mulder, H.T.; Van Holthe, J.M.L.; Aangeenbrug, A.A.; Mens, J.W.M.; Van Doorn, H.C.; Paulides, M.M.; Oomen-de Hoop, E.; Vernhout, R.M.; Lutgens, L.C.; et al. The Effect of the Time Interval Between Radiation and Hyperthermia on Clinical Outcome in 400 Locally Advanced Cervical Carcinoma Patients. Front. Oncol. 2019, 9, 134. [Google Scholar] [CrossRef]
- Tilly, W.; Gellermann, J.; Graf, R.; Hildebrandt, B.; Weissbach, L.; Budach, V.; Felix, R.; Wust, P. Regional Hyperthermia in Conjunction with Definitive Radiotherapy against Recurrent or Locally Advanced Prostate Cancer T3 pN0 M0. Strahlenther. Onkol. 2005, 181, 35–41. [Google Scholar] [CrossRef]
- Maluta, S.; Dall’Oglio, S.; Romano, M.; Marciai, N.; Pioli, F.; Giri, M.G.; Benecchi, P.L.; Comunale, L.; Porcaro, A.B. Conformal radiotherapy plus local hyperthermia in patients affected by locally advanced high risk prostate cancer: Preliminary results of a prospective phase II study. Int. J. Hyperth. 2007, 23, 451–456. [Google Scholar] [CrossRef]
- Dinges, S.; Harder, C.; Wurm, R.; Buchali, A.; Blohmer, J.; Gellermann, J.; Wust, P.; Randow, H.; Budach, V. Combined treatment of inoperable carcinomas of the uterine cervix with radiotherapy and regional hyperthermia. Strahlenther. Onkol. 1998, 174, 517–521. [Google Scholar] [CrossRef]
- Secord, A.A.; Jones, E.L.; Hahn, C.A.; Petros, W.P.; Yu, D.; Havrilesky, L.J.; Soper, J.T.; Berchuck, A.; Spasojevic, I.; Clarke-Pearson, D.L.; et al. Phase I/II trial of intravenous Doxil® and whole abdomen hyperthermia in patients with refractory ovarian cancer. Int. J. Hyperth. 2005, 21, 333–347. [Google Scholar] [CrossRef]
- Harima, Y.; Ohguri, T.; Imada, H.; Sakurai, H.; Ohno, T.; Hiraki, Y.; Tuji, K.; Tanaka, M.; Terashima, H. A multicentre randomised clinical trial of chemoradiotherapy plus hyperthermia versus chemoradiotherapy alone in patients with locally advanced cervical cancer. Int. J. Hyperth. 2016, 32, 801–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coates, A.; Porzsolt, F.; Osoba, D. Quality of life in oncology practice: Prognostic value of EORTC QLQ-C30 scores in patients with advanced malignancy. Eur. J. Cancer 1997, 33, 1025–1030. [Google Scholar] [CrossRef] [PubMed]
- Gotay, C.C.; Kawamoto, C.T.; Bottomley, A.; Efficace, F. The Prognostic Significance of Patient-Reported Outcomes in Cancer Clinical Trials. J. Clin. Oncol. 2008, 26, 1355–1363. [Google Scholar] [CrossRef] [PubMed]
- Gani, C.; Lamprecht, U.; Ziegler, A.; Moll, M.; Gellermann, J.; Heinrich, V.; Wenz, S.; Fend, F.; Königsrainer, A.; Bitzer, M.; et al. Deep regional hyperthermia with preoperative radiochemotherapy in locally advanced rectal cancer, a prospective phase II trial. Radiother. Oncol. 2021, 159, 155–160. [Google Scholar] [CrossRef]
- Beck, M.; Ghadjar, P.; Mehrhof, F.; Zips, D.; Paulsen, F.; Wegener, D.; Burock, S.; Kaul, D.; Stromberger, C.; Nadobny, J.; et al. Salvage-Radiation Therapy and Regional Hyperthermia for Biochemically Recurrent Prostate Cancer after Radical Prostatectomy (Results of the Planned Interim Analysis). Cancers 2021, 13, 1133. [Google Scholar] [CrossRef]
- Riesterer, O.; Ademaj, A.; Puric, E.; Eberle, B.; Beck, M.; Gomez, S.; Marder, D.; Oberacker, E.; Rogers, S.; Hälg, R.A.; et al. Tetramodal therapy with transurethral resection followed by chemoradiation in combination with hyperthermia for muscle-invasive bladder cancer: Early results of a multicenter phase IIB study. Int. J. Hyperth. 2022, 39, 1078–1087. [Google Scholar] [CrossRef]
- Maissenhaelter, B.E.; Woolmore, A.L.; Schlag, P.M. Real-world evidence research based on big data: Motivation-challenges-success factors. Onkologe 2018, 24, 91–98. [Google Scholar] [CrossRef] [Green Version]
- Dobšíček Trefná, H.; Schmidt, M.; van Rhoon, G.C.; Kok, H.P.; Gordeyev, S.S.; Lamprecht, U.; Marder, D.; Nadobny, J.; Ghadjar, P.; Abdel-Rahman, S.; et al. Quality assurance guidelines for interstitial hyperthermia. Int. J. Hyperth. 2019, 36, 276–293. [Google Scholar] [CrossRef] [Green Version]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; De Haes, J.C.J.M.; et al. The European Organization for Research and Treatment of Cancer QLQ-C30: A Quality-of-Life Instrument for Use in International Clinical Trials in Oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef]
- Fayers, P.; Aaronson, N.K.; Bjordal, K.; Grønvold, M.; Curran, D.; Bottomley, A. EORTC QLQ-C30 Scoring Manual; European Organisation for Research and Treatment of Cancer: Brussels, Belgium, 2001. [Google Scholar]
- Scott, N.W.; Fayers, P.; Aaronson, N.K.; Bottomley, A.; de Graeff, A.; Groenvold, M.; Gundy, C.; Koller, M.; Petersen, M.A.; Sprangers, M.A.; et al. EORTC QLQ-C30 Reference Values Manual, 2nd ed.; EORTC Quality of Life Group: Brussels, Belgium, 2008; p. 427. [Google Scholar]
- Jacobsen, P.B.; Davis, K.; Cella, D. Assessing quality of life in research and clinical practice. Oncology 2002, 16, 133–139. [Google Scholar]
- Eypasch, E.; Wood-Dauphinée, S.; Williams, J.I.; Ure, B.; Neugebauer, E.; Troidl, H. The Gastrointestinal Quality of Life Index. A clinical index for measuring patient status in gastroenterologic surgery. Der Chir. 1993, 64, 264–274. [Google Scholar]
- Schwenk, W.; Neudecker, J.; Haase, O.; Raue, W.; Strohm, T. Comparison of EORTC Quality of Life Core Questionnaire (EORTC-QLQ-C30) and Gastrointestinal Quality of Life Index (GIQLI) in patients undergoing elective colorectal cancer resection. Int. J. Color. Dis. 2004, 19, 554–560. [Google Scholar] [CrossRef]
- Schulze, T.; Wust, P.; Gellermann, J.; Hildebrandt, B.; Riess, H.; Felix, R.; Rau, B. Influence of neoadjuvant radiochemotherapy combined with hyperthermia on the quality of life in rectum cancer patients. Int. J. Hyperth. 2006, 22, 301–318. [Google Scholar] [CrossRef]
- Harima, Y.; Nagata, K.; Harima, K.; Ostapenko, V.V.; Tanaka, Y.; Sawada, S. A randomized clinical trial of radiation therapy versus thermoradiotherapy in stage IIIB cervical carcinoma. Int. J. Hyperth. 2009, 25, 338–343. [Google Scholar] [CrossRef]
- Ott, O.; Gani, C.; Lindner, L.; Schmidt, M.; Lamprecht, U.; Abdel-Rahman, S.; Hinke, A.; Weissmann, T.; Hartmann, A.; Issels, R.; et al. Neoadjuvant Chemoradiation Combined with Regional Hyperthermia in Locally Advanced or Recurrent Rectal Cancer. Cancers 2021, 13, 1279. [Google Scholar] [CrossRef]
- Seegenschmiedt, H.M.; Karlsson, U.L.; Sauer, R.; Brady, L.W.; Herbst, M.; Amendola, B.E.; Markoe, A.M.; Fisher, S.A.; Micaily, B. Superficial chest wall recurrences of breast cancer: Prognostic treatment factors for combined radiation therapy and hyperthermia. Radiology 1989, 173, 551–558. [Google Scholar] [CrossRef]
- Linthorst, M.; Baaijens, M.; Wiggenraad, R.; Creutzberg, C.; Ghidey, W.; van Rhoon, G.C.; van der Zee, J. Local control rate after the combination of re-irradiation and hyperthermia for irresectable recurrent breast cancer: Results in 248 patients. Radiother. Oncol. 2015, 117, 217–222. [Google Scholar] [CrossRef]
- Linthorst, M.; van Geel, A.N.; Baaijens, M.; Ameziane, A.; Ghidey, W.; van Rhoon, G.C.; van der Zee, J. Re-irradiation and hyperthermia after surgery for recurrent breast cancer. Radiother. Oncol. 2013, 109, 188–193. [Google Scholar] [CrossRef]
- Van der Zee, J.; González, D.; van Rhoon, G.C.; van Dijk, J.D.; van Putten, W.L.; Hart, A.A. Comparison of radiotherapy alone with radiotherapy plus hyperthermia in locally advanced pelvic tumours: A prospective, randomised, multicentre trial. Dutch Deep Hyperthermia Group. Lancet 2000, 355, 1119–1125. [Google Scholar] [CrossRef]
- Engin, K.; Tupchong, L.; Moylan, D.J.; Alexander, G.A.; Waterman, F.M.; Komarnicky, L.; Nerlinger, R.E.; Leeper, D.B. Randomized trial of one versus two adjuvant hyperthermia treatments per week in patients with superficial tumours. Int. J. Hyperth. 1993, 9, 327–340. [Google Scholar] [CrossRef]
- Yucel, B.; Akkaş, E.A.; Okur, Y.; Eren, A.A.; Eren, M.F.; Karapınar, H.; Babacan, N.A.; Kılıçkap, S. The impact of radiotherapy on quality of life for cancer patients: A longitudinal study. Support. Care Cancer 2014, 22, 2479–2487. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Palliative Intent Treatment, n (%) | Curative Intent Treatment, n (%) |
|---|---|---|
| Sex | ||
| Male | 25 (44) | 17 (33) |
| Female | 20 (56) | 35 (67) |
| Median age at treatment start ‡ | 66 (37–92) | 66 (28–84) |
| KPS prior to treatment | ||
| 100 | 14 (31) | 25 (48) |
| 90 | 7 (16) | 6 (12) |
| ≤80 | 14 (31) | 5 (10) |
| n.a. | 10 (22) | 16 (30) |
| Primary tumor histology | ||
| Breast cancer | 11 (25) | 22 (42) |
| Lung cancer | 5 (11) | 0 (0) |
| Bladder cancer | 2 (4) | 7 (13) |
| Anal cancer | 4 (9) | 2 (4) |
| Rectal cancer | 4 (9) | 6 (11) |
| Melanoma | 6 (13) | 0 (0) |
| Sarcoma | 1 (2) | 5 (10) |
| Pancreas cancer | 0 (0) | 5 (10) |
| Prostate cancer | 5 (11) | 2 (4) |
| Other | 7 (16) * | 3 (6) ** |
| Recurrent cancer | 25 (56) | 32 (62) |
| RT prescribed total dose (Gy) † | 38 (±10) | 50 (±6) |
| RT dose per fraction (Gy) † | 2.5 (±0.5) | 1.9 (±0.2) |
| Number of RT fractions† | 16 (±7) | 24 (±4) |
| Duration of RT + HT (days) † | 25 (±13) | 35 (±8) |
| HT techniques | ||
| Superficial HT | 22 (49) | 27 (52) |
| Deep regional HT | 23 (51) | 25 (48) |
| Time interval between RT and HT (minutes) ‡ | 15 (7–80) | 14 (6–83) |
| n.a. | 3 (7) | 7 (13) |
| Total HT sessions ‡ | 5 (3–11) | 5 (4–11) |
| Temperature metrics (°C) | ||
| Tavg † | 39.9 (±0.7) | 40.3 (±0.6) |
| Tmax † | 40.5 (±0.8) | 40.9 (±0.6) |
| n.a. | 11 (32) | 10 (19) |
| Thermal dose CEM43 † | 1.7 (±1.5) | 2.8 (±2.2) |
| n.a. | 11 (32) | 10 (19) |
| Chemotherapy | ||
| Superficial HT | 0 (0) | 0 (0) |
| Deep regional HT | 1 (4) | 14 (27) |
| Toxicity | Grade 1 | Grade 2 | Grade 3 | |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | ||
| During treatment, n = 51 | Dermatitis | 7 (14) | 7 (14) | 3 (6) |
| Mucositis | 0 | 0 | 1 (2) | |
| Skin reaction(s) | 7 (14) | 6 (12) | 4 (8) | |
| Diarrhoea | 8 (16) | 2 (4) | 2 (4) | |
| Urinary incontinence/ urinary retention/ Nocturia | 4 (8) | 0 | 0 | |
| Dysuria | 3 (6) | 1 (2) | 0 | |
| Pyelonephritis | 0 | 1 (2) | 0 | |
| Nausea | 1 (2) | 1 (2) | 0 | |
| Vomiting | 1 (2) | 0 | 0 | |
| Constipation | 0 | 2 (4) | 0 | |
| Pain | 1 (2) | 0 | 1 (2) | |
| Tiredness/fatigue | 11 (22) | 2 (4) | 0 | |
| Appetite loss | 1 (2) | 0 | 0 | |
| Three months after treatment, n = 45 | Skin reaction(s) | 4 (9) | 0 | 0 |
| Diarrhoea | 3 (6) | 0 | 0 | |
| Urinary incontinence/ urinary retention | 2 (4) | 0 | 0 | |
| Dysphagia | 1 (2) | 0 | 0 | |
| Nausea | 0 | 0 | 1 (2) | |
| Pain | 1 (2) | 1 (2) | 0 | |
| Vomiting | 0 | 0 | 1 (2) |
| Toxicity | Grade 1 | Grade 2 | Grade 3 | |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | ||
| During treatment n = 42 | Dermatitis | 4 (9) | 3 (7) | 0 |
| Skin reaction(s) | 4 (9) | 5 (11) | 0 | |
| Hepatitis | 0 | 1 (2) | 1 (2) | |
| Urinary incontinence/ urinary retention | 5 (11) | 0 | 0 | |
| Diarrhoea | 7 (16) | 0 | 1 (2) | |
| Dysphasia | 1 (2) | 0 | 0 | |
| Pain | 7 (17) | 0 | 0 | |
| Tiredness/fatigue | 9 (21) | 1 (2) | 0 | |
| Three months after treatment n = 29 | Dermatitis | 1 (3) | 0 | 0 |
| Skin reaction(s) | 3 (10) | 0 | 0 | |
| Diarrhoea | 2 (7) | 0 | 0 | |
| Urinary incontinence/ urinary retention | 4 (14) | 0 | 0 | |
| Pain | 3 (10) | 2 (7) | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ademaj, A.; Puric, E.; Timm, O.; Kurti, D.; Marder, D.; Kern, T.; Hälg, R.A.; Rogers, S.; Riesterer, O. Real World Analysis of Quality of Life and Toxicity in Cancer Patients Treated with Hyperthermia Combined with Radio(chemo)therapy. Cancers 2023, 15, 1241. https://doi.org/10.3390/cancers15041241
Ademaj A, Puric E, Timm O, Kurti D, Marder D, Kern T, Hälg RA, Rogers S, Riesterer O. Real World Analysis of Quality of Life and Toxicity in Cancer Patients Treated with Hyperthermia Combined with Radio(chemo)therapy. Cancers. 2023; 15(4):1241. https://doi.org/10.3390/cancers15041241
Chicago/Turabian StyleAdemaj, Adela, Emsad Puric, Olaf Timm, David Kurti, Dietmar Marder, Thomas Kern, Roger A. Hälg, Susanne Rogers, and Oliver Riesterer. 2023. "Real World Analysis of Quality of Life and Toxicity in Cancer Patients Treated with Hyperthermia Combined with Radio(chemo)therapy" Cancers 15, no. 4: 1241. https://doi.org/10.3390/cancers15041241
APA StyleAdemaj, A., Puric, E., Timm, O., Kurti, D., Marder, D., Kern, T., Hälg, R. A., Rogers, S., & Riesterer, O. (2023). Real World Analysis of Quality of Life and Toxicity in Cancer Patients Treated with Hyperthermia Combined with Radio(chemo)therapy. Cancers, 15(4), 1241. https://doi.org/10.3390/cancers15041241