

Current Status of Management of Hepatocellular Carcinoma in The Gulf Region: Challenges and Recommendations


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
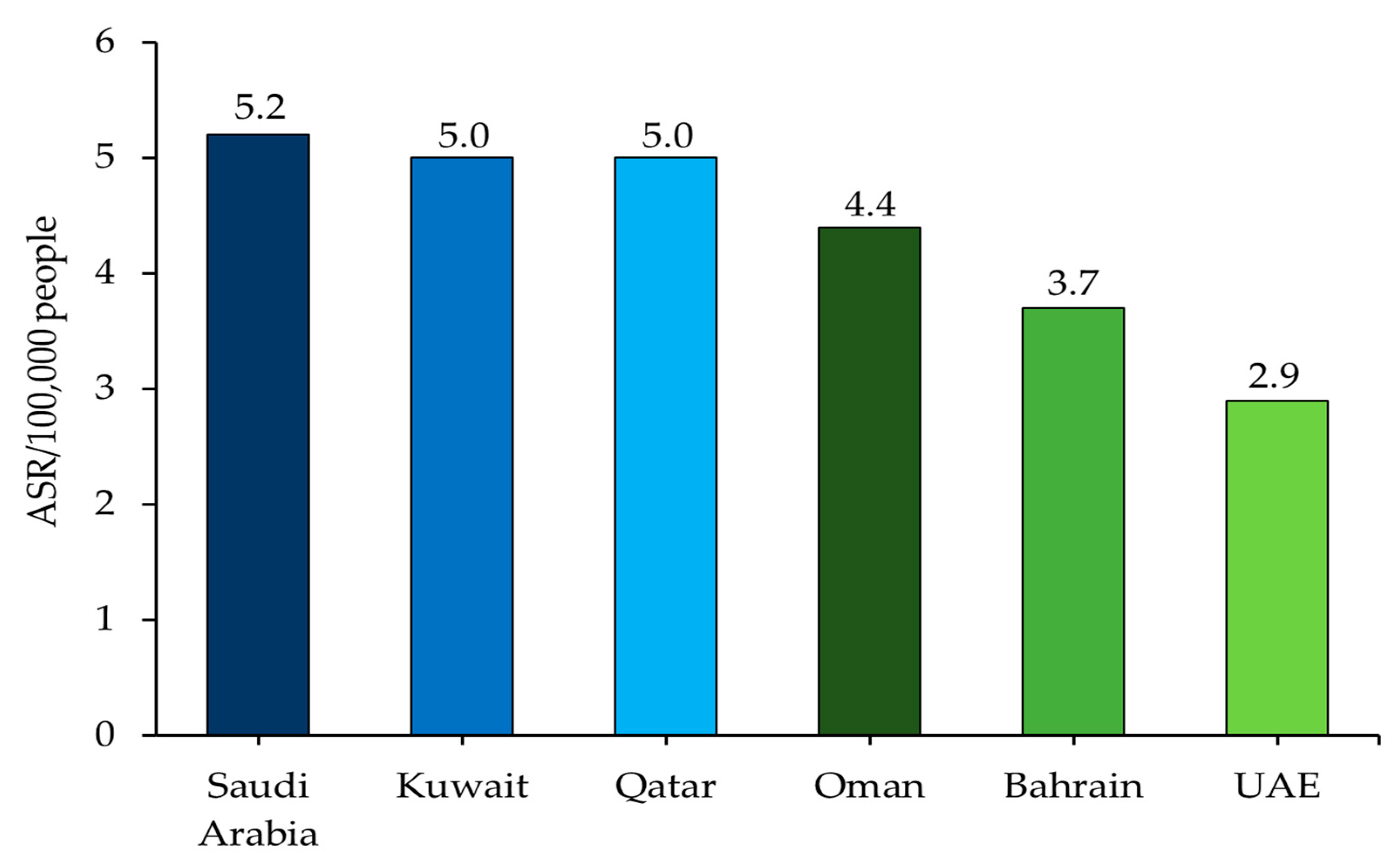
2. Epidemiology of HCC across the Gulf Region
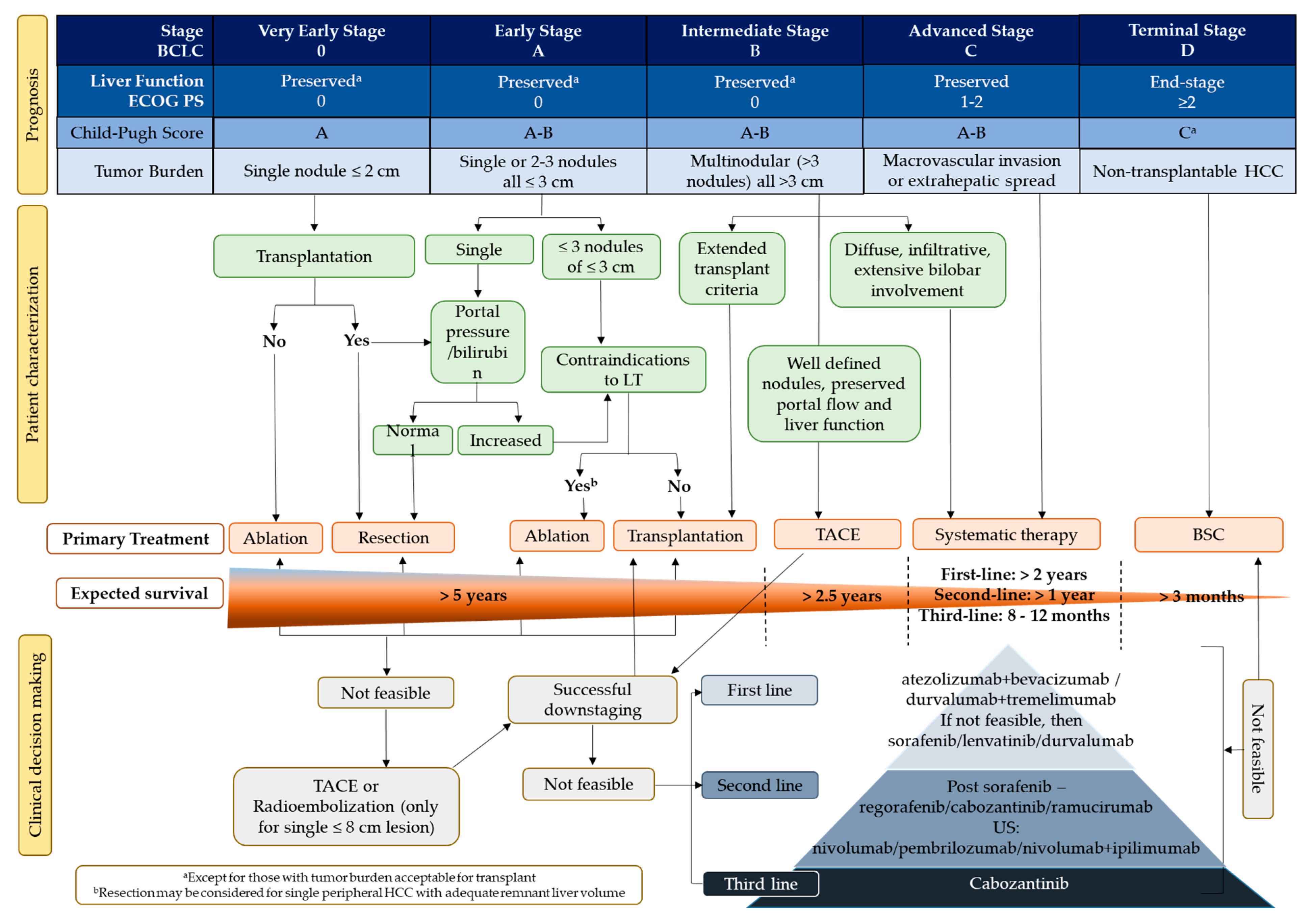
3. HCC Management in the Gulf: Staging and Treatment Modalities for Unresectable Intermediate and Advanced HCC
3.1. Surgery for Patients with HCC across the Gulf
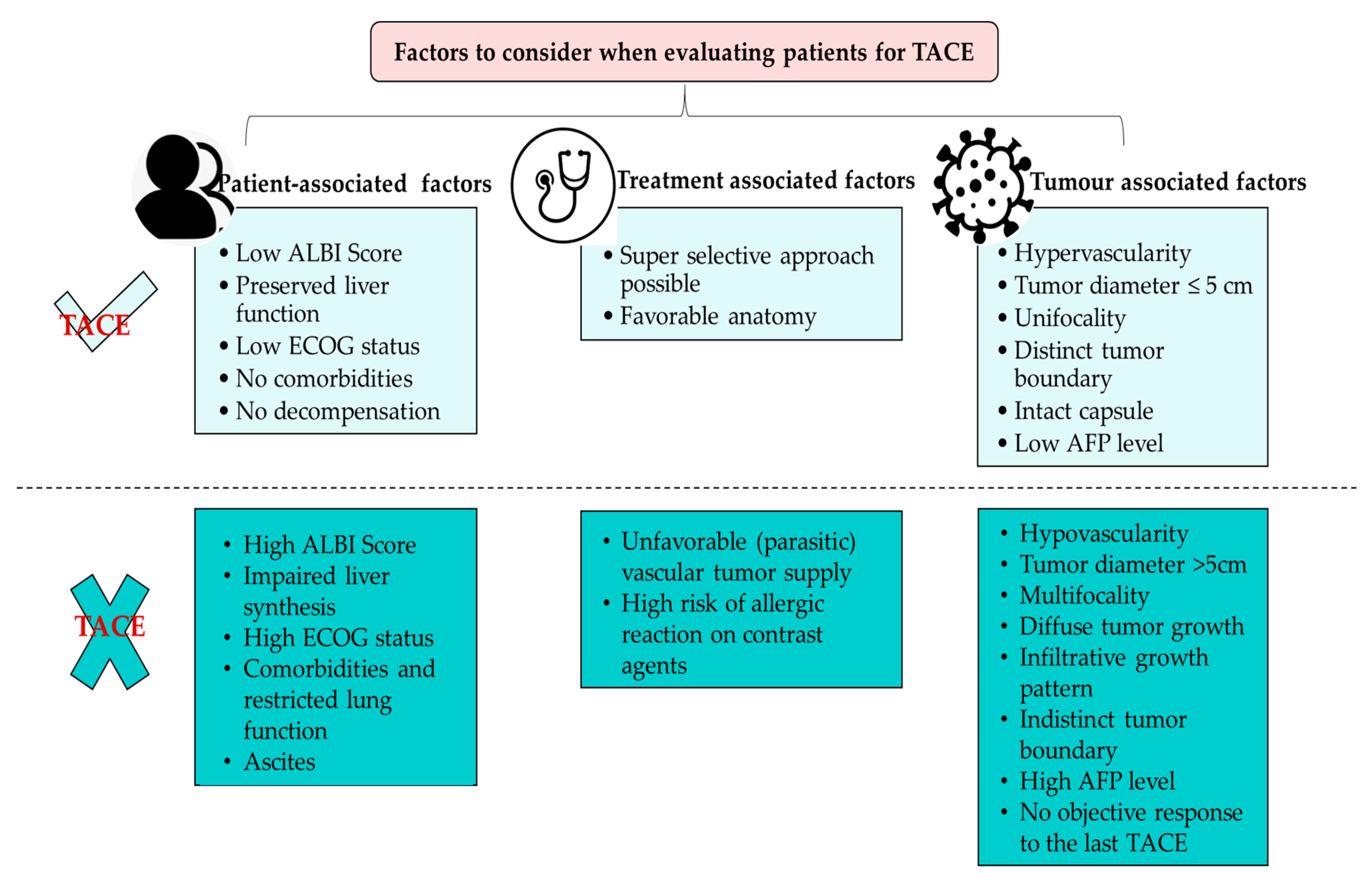
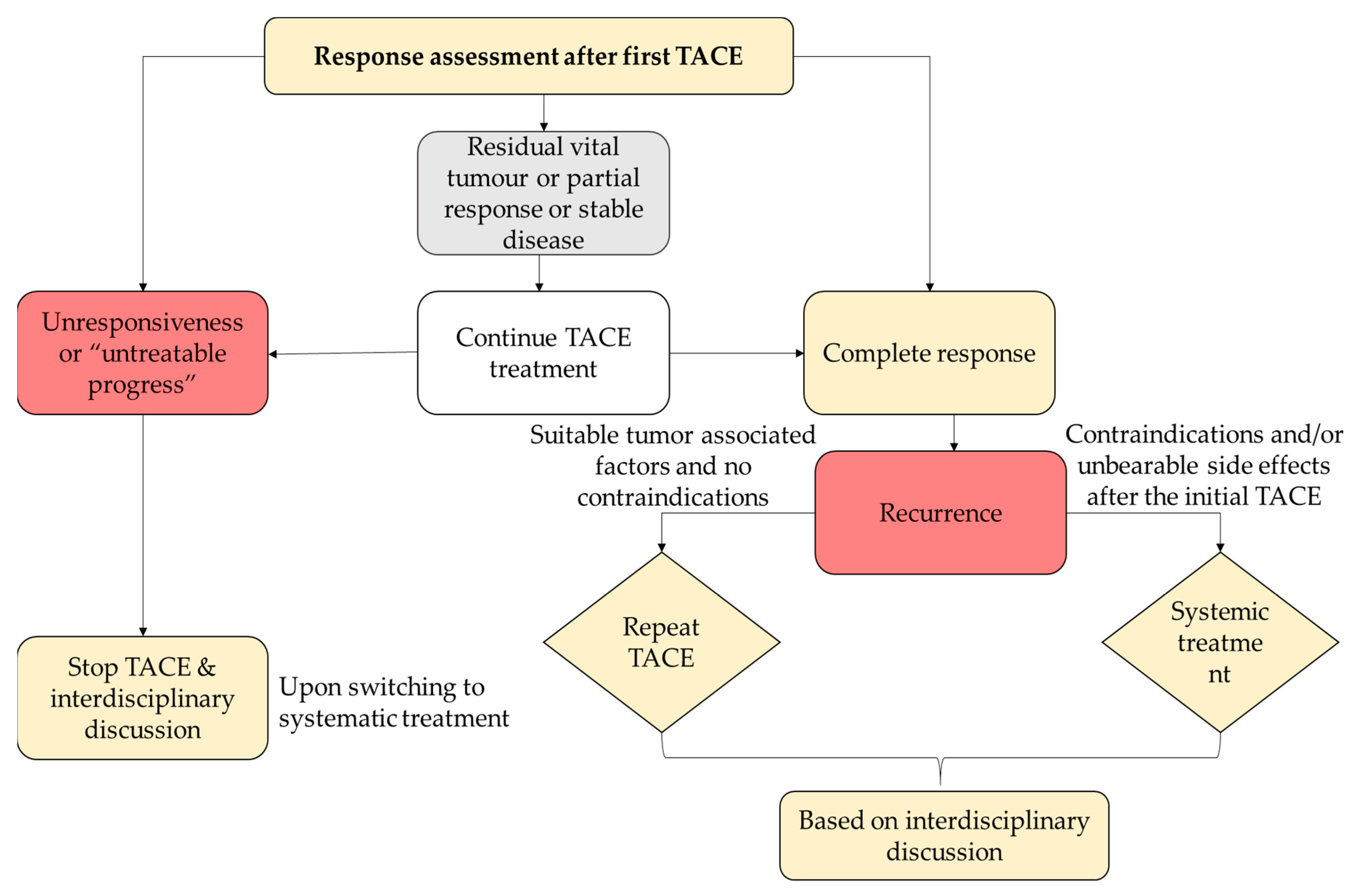
3.2. Role of Locoregional Therapy for Patients with HCC across the Gulf
3.3. Systemic Therapies Used for Patients with HCC across the Gulf
3.4. Challenges with Established Systemic Therapies in the Gulf and Emergence of Novel Combination Therapies
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; Singal, A.G.; Pikarsky, E.; Roayaie, S.; Lencioni, R.; Koike, K.; Zucman-Rossi, J.; Finn, R.S. Hepatocellular Carcinoma. Nat. Rev. Dis. Prim. 2021, 7, 6. [Google Scholar] [CrossRef]
- Llovet, J.M.; Zucman-Rossi, J.; Pikarsky, E.; Sangro, B.; Schwartz, M.; Sherman, M.; Gores, G. Hepatocellular Carcinoma. Nat. Rev. Dis. Prim. 2016, 2, 16018. [Google Scholar] [CrossRef] [PubMed]
- Cancer IARC. Globocan 2022. Available online: https://gco.iarc.fr/ (accessed on 25 March 2023).
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Colagrande, S.; Inghilesi, A.L.; Aburas, S.; Taliani, G.G.; Nardi, C.; Marra, F. Challenges of Advanced Hepatocellular Carcinoma. World J. Gastroenterol. 2016, 22, 7645–7659. [Google Scholar] [CrossRef]
- Vogel, A.; Cervantes, A.; Chau, I.; Daniele, B.; Llovet, J.M.; Meyer, T.; Nault, J.-C.; Neumann, U.; Ricke, J.; Sangro, B.; et al. Hepatocellular Carcinoma: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2018, 29, iv238–iv255. [Google Scholar] [CrossRef] [PubMed]
- Kanwal, F.; Kramer, J.; Asch, S.M.; Chayanupatkul, M.; Cao, Y.; El-Serag, H.B. Risk of Hepatocellular Cancer in HCV Patients Treated with Direct-Acting Antiviral Agents. Gastroenterology 2017, 153, 996–1005.e1. [Google Scholar] [CrossRef] [PubMed]
- Estes, C.; Razavi, H.; Loomba, R.; Younossi, Z.; Sanyal, A.J. Modeling the Epidemic of Nonalcoholic Fatty Liver Disease Demonstrates an Exponential Increase in Burden of Disease. Hepatology 2018, 67, 123–133. [Google Scholar] [CrossRef]
- Schulze, K.; Imbeaud, S.; Letouzé, E.; Alexandrov, L.B.; Calderaro, J.; Rebouissou, S.; Couchy, G.; Meiller, C.; Shinde, J.; Soysouvanh, F.; et al. Exome Sequencing of Hepatocellular Carcinomas Identifies New Mutational Signatures and Potential Therapeutic Targets. Nat. Genet. 2015, 47, 505–511. [Google Scholar] [CrossRef]
- Global Burden of Disease Liver Cancer Collaboration; Akinyemiju, T.; Abera, S.; Ahmed, M.; Alam, N.; Alemayohu, M.A.; Allen, C.; Al-Raddadi, R.; Alvis-Guzman, N.; Amoako, Y.; et al. The Burden of Primary Liver Cancer and Underlying Etiologies from 1990 to 2015 at the Global, Regional, and National Level: Results from the Global Burden of Disease Study 2015. JAMA Oncol. 2017, 3, 1683–1691. [Google Scholar] [CrossRef]
- Ogunwobi, O.O.; Harricharran, T.; Huaman, J.; Galuza, A.; Odumuwagun, O.; Tan, Y.; Ma, G.X.; Nguyen, M.T. Mechanisms of Hepatocellular Carcinoma Progression. WJG 2019, 25, 2279–2293. [Google Scholar] [CrossRef]
- Mohamoud, Y.A.; Riome, S.; Abu-Raddad, L.J. Epidemiology of Hepatitis C Virus in the Arabian Gulf Countries: Systematic Review and Meta-Analysis of Prevalence. Int. J. Infect. Dis. 2016, 46, 116–125. [Google Scholar] [CrossRef] [PubMed]
- Shaaban, A.; Salamah, R.; Abo Elseud, Y.; Mohanty, A.; Albarrak, J. Presentation and Outcomes of Hepatocellular Carcinoma in the Arabian Peninsula: A Review of a Single Institution Experience in the Sorafenib Era. J. Gastrointest. Canc. 2021, 52, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Shaaban, A.; Salamah, R.; Elseud, Y.A.; Mohanty, A.; Albarrak, J. Hepatocellular Carcinoma in Kuwait. In Liver Cancer in the Middle East; Carr, B.I., Ed.; Springer International Publishing: Cham, Switzerland, 2021; pp. 237–246. ISBN 978-3-030-78736-3. [Google Scholar]
- Rasul, K.I.; Al-Azawi, S.H.; Chandra, P. Hepatocellular Carcinoma in Qatar. Gulf J. Oncol. 2013, 1, 70–75. [Google Scholar]
- Alkhammash, M.; Bugis, B. A Comparison Review of the Clinical Healthcare Services Provided to Liver Disease Patients in the GCC. J. Basic Clin. Health Sci. 2021, 5, 22–35. [Google Scholar] [CrossRef]
- Rasul, K.I.; Al-Azawi, S.H.; Chandra, P.; Abou-Alfa, G.K.; Knuth, A. Status of Hepatocellular Carcinoma in Gulf Region. Chin. Clin. Oncol. 2013, 2, 42. [Google Scholar] [CrossRef]
- Mohd Hanafiah, K.; Groeger, J.; Flaxman, A.D.; Wiersma, S.T. Global Epidemiology of Hepatitis C Virus Infection: New Estimates of Age-Specific Antibody to HCV Seroprevalence. Hepatology 2013, 57, 1333–1342. [Google Scholar] [CrossRef]
- Member States of the GCC: Gulf Cooperation Council. Available online: https://www.worlddata.info/alliances/gcc-gulf-cooperation-council.php (accessed on 29 September 2022).
- Al-Othman, S.; Al-Madouj, A.; Al-Zahrani, A. Incidence and Trends of Liver Cancer in the Gulf Cooperation Council States, 1998-2012. Gulf J. Oncol. 2021, 1, 53–59. [Google Scholar]
- Estimated Age-Standardized Incidence Rates (Asia) in 2020, Both Sexes, All Ages. World Health Organization Globocan. 2020. Available online: https://gco.iarc.fr/today/home (accessed on 29 August 2022).
- Poustchi, H.; Sepanlou, S.; Esmaili, S.; Mehrabi, N.; Ansarymoghadam, A. Hepatocellular Carcinoma in the World and the Middle East. Middle East J. Dig. Dis. 2010, 2, 31–41. [Google Scholar]
- Sharafi, H.; Alavian, S.M. The Rising Threat of Hepatocellular Carcinoma in the Middle East and North Africa Region: Results From Global Burden of Disease Study 2017. Clin. Liver Dis. 2019, 14, 219–223. [Google Scholar] [CrossRef]
- Cancer in the Arab World; Al-Shamsi, H.O.; Abu-Gheida, I.H.; Iqbal, F.; Al-Awadhi, A. (Eds.) Springer Nature: Berlin/Heidelberg, Germany, 2022. [Google Scholar]
- Al-Hamdan, N.; Ravichandran, K.; Al-Sayyad, J.; Al-Lawati, J.; Khazal, Z.; Al-Khateeb, F.; Abdulwahab, A.; Al-Asfour, A. Incidence of Cancer in Gulf Cooperation Council Countries, 1998–2001. East Mediterr. Health J. 2009, 15, 600–611. [Google Scholar] [CrossRef]
- WHO. Liver fact sheet. In Globocan 2020; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Cancer Incidence Report Saudi Arabia 2014. Saudi Health Council Saudi Cancer. Available online: https://www.nhic.gov.sa/eServices/Documents/2014.pdf (accessed on 25 March 2023).
- Hussain, F.; Anjum, S.; Alrshoud, N.; Mehmood, A.; Bazarbashi, S.; Hussain, A.N.; Chaudhri, N. Trends and Patterns of Primary Hepatic Carcinoma in Saudi Arabia. Gulf J. Oncol. 2019, 1, 41–51. [Google Scholar]
- Elmoghazy, W.; Ahmed, K.; Vijay, A.; Kamel, Y.; Elaffandi, A.; El-Ansari, W.; Kakil, R.; Khalaf, H. Hepatocellular Carcinoma in a Rapidly Growing Community: Epidemiology, Clinico-Pathology and Predictors of Extrahepatic Metastasis. Arab. J. Gastroenterol. 2019, 20, 38–43. [Google Scholar] [CrossRef]
- Cancer Incidence in Oman 2019. Ministry of Health Sultanate of Oman. Available online: www.moh.gov.om (accessed on 25 March 2023).
- Al-Naamani, K.; Al-Hashami, Z.; Al-Siyabi, O.; Al-Moundri, M.; Al-Bahrani, B.; Al-Sinani, S.; Al-Zakwani, I.; Omar, H.; Al-Busafi, S.A.; Al-Zuhaibi, H.; et al. Hepatocellular Carcinoma in Oman: An Analysis of 284 Cases. Sultan Qaboos Univ. Med. J. 2020, 20, 316. [Google Scholar] [CrossRef]
- Cancer Incidence in United Arab Emirates Annual Report of the UAE—National Cancer Registry 2017; United Arab Emirates Ministry of Health & Prevention: Dubai, United Arab Emirates, 2017.
- Hashim, M.J.; Rizvi, S.S.; Khan, G. Hepatocellular Carcinoma in the United Arab Emirates. In Liver Cancer in the Middle East; Carr, B.I., Ed.; Springer International Publishing: Cham, Switzerland, 2021; pp. 101–108. ISBN 978-3-030-78736-3. [Google Scholar]
- Baffy, G. Editorial: Hepatocellular Carcinoma in Type 2 Diabetes: More than Meets the Eye. Am. J. Gastroenterol. 2012, 107, 53–55. [Google Scholar] [CrossRef]
- Salmon, D.; Bani-Sadr, F.; Loko, M.-A.; Stitou, H.; Gervais, A.; Durant, J.; Rosenthal, E.; Quertainmont, Y.; Barange, K.; Vittecoq, D.; et al. Insulin Resistance Is Associated with a Higher Risk of Hepatocellular Carcinoma in Cirrhotic HIV/HCV-Co-Infected Patients: Results from ANRS CO13 HEPAVIH. J. Hepatol. 2012, 56, 862–868. [Google Scholar] [CrossRef]
- Alswat, K.; Aljumah, A.; Sanai, F.; Abaalkhail, F.; Alghamdi, M.; Al Hamoudi, W.; Al Khathlan, A.; Al Quraishi, H.; Al Rifai, A.; Al Zaabi, M.; et al. Nonalcoholic Fatty Liver Disease Burden—Saudi Arabia and United Arab Emirates, 2017–2030. Saudi. J. Gastroenterol. 2018, 24, 211. [Google Scholar] [CrossRef]
- Al-Muhaimeed, A.A.; Dandash, K.; Ismail, M.S.; Saquib, N. Prevalence and Correlates of Overweight Status among Saudi School Children. Ann. Saudi. Med. 2015, 35, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, M.A.; Al Sharaf, F.; Shehzad, K.; Shoukat, F.; Naeem, Z.; Al Harbi, S.; Almutairi, A.S.; Al Ilaj, M.O.; Al Motairi, S. Prevalence and Trends of Overweight and Obesity amongst Saudi School Children, a Study Done by Using Three Noninvasive Methods. Int. J. Health Sci. 2016, 10, 381–387. [Google Scholar] [CrossRef]
- Ng, S.W.; Zaghloul, S.; Ali, H.; Harrison, G.; Yeatts, K.; El Sadig, M.; Popkin, B.M. Nutrition Transition in the United Arab Emirates. Eur. J. Clin. Nutr. 2011, 65, 1328–1337. [Google Scholar] [CrossRef] [PubMed]
- Musaiger, A.O.; Al-Mannai, M.; Al-Haifi, A.R.; Nabag, F.; Elati, J.; Abahussain, N.; Tayyem, R.; Jalambo, M.; Benhamad, M.; Al-Mufty, B. Prevalence of Overweight and Obesity among Adolescents in Eight Arab Countries: Comparison between Two International Standards (ARABEAT-2). Nutr. Hosp. 2016, 33, 567. [Google Scholar] [CrossRef]
- Al-Judaibi, B.; Dokus, M.K.; Al-Hamoudi, W.; Broering, D.; Mawardi, M.; AlMasri, N.; Aljawad, M.; Altraif, I.H.; Abaalkhail, F.; Alqahtani, S.A. Saudi Association for the Study of Liver Diseases and Transplantation Position Statement on the Hepatology Workforce in Saudi Arabia. Saudi. J. Gastroenterol. 2022, 28, 101–107. [Google Scholar] [CrossRef]
- Alkhouri, N.; Hanouneh, I.A.; Zein, N.N.; Lopez, R.; Kelly, D.; Eghtesad, B.; Fung, J.J. Liver Transplantation for Nonalcoholic Steatohepatitis in Young Patients. Transpl. Int. 2016, 29, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Lavanchy, D. Evolving Epidemiology of Hepatitis C Virus. Clin. Microbiol. Infect. 2011, 17, 107–115. [Google Scholar] [CrossRef]
- El-Zanaty, F.; Way, A. Egypt Demographic and Health Survey 2008; Ministry of Health, El-Zanaty and Associates, and Macro International: Cairo, Egypt, 2009; Volume 463. [Google Scholar]
- Zamor, P.J.; deLemos, A.S.; Russo, M.W. Viral Hepatitis and Hepatocellular Carcinoma: Etiology and Management. J. Gastrointest. Oncol. 2017, 8, 229–242. [Google Scholar] [CrossRef]
- Mohamoud, Y.A.; Mumtaz, G.R.; Riome, S.; Miller, D.; Abu-Raddad, L.J. The Epidemiology of Hepatitis C Virus in Egypt: A Systematic Review and Data Synthesis. BMC Infect. Dis. 2013, 13, 288. [Google Scholar] [CrossRef] [PubMed]
- Rashed, W.M.; Kandeil, M.A.M.; Mahmoud, M.O.; Ezzat, S. Hepatocellular Carcinoma (HCC) in Egypt: A Comprehensive Overview. J. Egypt. Natl. Cancer Inst. 2020, 32, 5. [Google Scholar] [CrossRef]
- Emara, M.H. Occult Hepatitis B: The Egyptian Situation. Trop Gastroenterol. 2012, 33, 242–250. [Google Scholar] [CrossRef]
- Ringelhan, M.; O’Connor, T.; Protzer, U.; Heikenwalder, M. The Direct and Indirect Roles of HBV in Liver Cancer: Prospective Markers for HCC Screening and Potential Therapeutic Targets. J. Pathol. 2015, 235, 355–367. [Google Scholar] [CrossRef] [PubMed]
- Habibzadeh, F. Viral Hepatitis in the Middle East. Lancet 2014, 384, 1–2. Available online: https://www.thelancet.com/pb/assets/raw/Lancet/global-health/middle-east/Oct14_MiddleEastEd.pdf?elsca1=220713&elsca2=MIDDLEEADTED&elsca3=segment (accessed on 3 November 2022).
- Awaidy, S.; Abuelyazeed, R.; Hosani, H.; Mulla, A.; Busaiedy, S.; Amiry, A.; Farah, Z.; Marrie, A.; Bock, H.; Alshaar, I. Sero-Epidemiology of Hepatitis B Infection in Pregnant Women in Oman, Qatar and the United Arab Emirates. J. Infect. 2006, 52, 202–206. [Google Scholar] [CrossRef]
- Qureshi, H.; Bile, K.M.; Jooma, R.; Alam, S.E.; Afridi, H.U.R. Prevalence of Hepatitis B and C Viral Infections in Pakistan: Findings of a National Survey Appealing for Effective Prevention and Control Measures. East Mediterr. Health J. 2010, 16, S15–S23. [Google Scholar] [CrossRef]
- Sayiner, M.; Golabi, P.; Younossi, Z.M. Disease Burden of Hepatocellular Carcinoma: A Global Perspective. Dig. Dis. Sci. 2019, 64, 910–917. [Google Scholar] [CrossRef] [PubMed]
- Ramakrishna, G.; Rastogi, A.; Trehanpati, N.; Sen, B.; Khosla, R.; Sarin, S.K. From Cirrhosis to Hepatocellular Carcinoma: New Molecular Insights on Inflammation and Cellular Senescence. Liver Cancer 2013, 2, 367–383. [Google Scholar] [CrossRef]
- Alali, A.A.; Abo-Shehada, M.N. Prevalence of Hepatitis B Virus Infection in the Gulf Cooperation Council: A Systematic Review and Meta-Analysis. BMC Infect. Dis. 2022, 22, 819. [Google Scholar] [CrossRef]
- Villanueva, A. Hepatocellular Carcinoma. N. Engl. J. Med. 2019, 380, 1450–1462. [Google Scholar] [CrossRef] [PubMed]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of Liver Function in Patients with Hepatocellular Carcinoma: A New Evidence-Based Approach-the ALBI Grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef]
- Pinato, D.J.; Sharma, R.; Allara, E.; Yen, C.; Arizumi, T.; Kubota, K.; Bettinger, D.; Jang, J.W.; Smirne, C.; Kim, Y.W.; et al. The ALBI Grade Provides Objective Hepatic Reserve Estimation across Each BCLC Stage of Hepatocellular Carcinoma. J. Hepatol. 2017, 66, 338–346. [Google Scholar] [CrossRef] [PubMed]
- Khan, G.; Hashim, M.J. Burden of Virus-Associated Liver Cancer in the Arab World, 1990–2010. Asian Pac. J. Cancer Prev. 2015, 16, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Scheiner, B.; Pomej, K.; Kirstein, M.M.; Hucke, F.; Finkelmeier, F.; Waidmann, O.; Himmelsbach, V.; Schulze, K.; von Felden, J.; Fründt, T.W.; et al. Prognosis of Patients with Hepatocellular Carcinoma Treated with Immunotherapy—Development and Validation of the CRAFITY Score. J. Hepatol. 2022, 76, 353–363. [Google Scholar] [CrossRef]
- Singal, A.G.; Hoshida, Y.; Pinato, D.J.; Marrero, J.; Nault, J.-C.; Paradis, V.; Tayob, N.; Sherman, M.; Lim, Y.S.; Feng, Z.; et al. International Liver Cancer Association (ILCA) White Paper on Biomarker Development for Hepatocellular Carcinoma. Gastroenterology 2021, 160, 2572–2584. [Google Scholar] [CrossRef]
- Cabibbo, G.; Maida, M.; Genco, C.; Parisi, P.; Peralta, M.; Antonucci, M.; Brancatelli, G.; Cammà, C.; Craxì, A.; Di Marco, V. Natural History of Untreatable Hepatocellular Carcinoma: A Retrospective Cohort Study. World J. Hepatol. 2012, 4, 256–261. [Google Scholar] [CrossRef] [PubMed]
- Draper, A. A Concise Review of the Changing Landscape of Hepatocellular Carcinoma. Am. J. Manag. Care 2020, 26, S211–S219. [Google Scholar] [CrossRef]
- Forner, A.; Llovet, J.M.; Bruix, J. Hepatocellular Carcinoma. Lancet 2012, 379, 1245–1255. [Google Scholar] [CrossRef]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and Response Criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef]
- Pugh, R.N.; Murray-Lyon, I.M.; Dawson, J.L.; Pietroni, M.C.; Williams, R. Transection of the Oesophagus for Bleeding Oesophageal Varices. Br. J. Surg. 1973, 60, 646–649. [Google Scholar] [CrossRef] [PubMed]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.-Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef] [PubMed]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC Strategy for Prognosis Prediction and Treatment Recommendation: The 2022 Update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; De Baere, T.; Kulik, L.; Haber, P.K.; Greten, T.F.; Meyer, T.; Lencioni, R. Locoregional Therapies in the Era of Molecular and Immune Treatments for Hepatocellular Carcinoma. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 293–313. [Google Scholar] [CrossRef]
- Mehta, N.; Bhangui, P.; Yao, F.Y.; Mazzaferro, V.; Toso, C.; Akamatsu, N.; Durand, F.; Ijzermans, J.; Polak, W.; Zheng, S.; et al. Liver Transplantation for Hepatocellular Carcinoma. Working Group Report from the ILTS Transplant Oncology Consensus Conference. Transplantation 2020, 104, 1136–1142. [Google Scholar] [CrossRef]
- Bruix, J.; Reig, M.; Sherman, M. Evidence-Based Diagnosis, Staging, and Treatment of Patients with Hepatocellular Carcinoma. Gastroenterology 2016, 150, 835–853. [Google Scholar] [CrossRef]
- Bruix, J.; Qin, S.; Merle, P.; Granito, A.; Huang, Y.-H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Breder, V.; et al. Regorafenib for Patients with Hepatocellular Carcinoma Who Progressed on Sorafenib Treatment (RESORCE): A Randomised, Double-Blind, Placebo-Controlled, Phase 3 Trial. Lancet 2017, 389, 56–66. [Google Scholar] [CrossRef]
- Wayne, J.D.; Lauwers, G.Y.; Ikai, I.; Doherty, D.A.; Belghiti, J.; Yamaoka, Y.; Regimbeau, J.-M.; Nagorney, D.M.; Do, K.-A.; Ellis, L.M.; et al. Preoperative Predictors of Survival after Resection of Small Hepatocellular Carcinomas. Ann. Surg. 2002, 235, 722–730; discussion 730–731. [Google Scholar] [CrossRef] [PubMed]
- Slotta, J.E.; Kollmar, O.; Ellenrieder, V.; Ghadimi, B.M.; Homayounfar, K. Hepatocellular Carcinoma: Surgeon’s View on Latest Findings and Future Perspectives. World J. Hepatol. 2015, 7, 1168–1183. [Google Scholar] [CrossRef] [PubMed]
- Lau, W.; Ho, S.K.W.; Yu, S.C.H.; Lai, E.C.H.; Liew, C.; Leung, T.W.T. Salvage Surgery Following Downstaging of Unresectable Hepatocellular Carcinoma. Ann. Surg. 2004, 240, 299–305. [Google Scholar] [CrossRef]
- Llovet, J.M.; Bustamante, J.; Castells, A.; Vilana, R.; del Carmen Ayuso, M.; Sala, M.; Brú, C.; Rodés, J.; Bruix, J. Natural History of Untreated Nonsurgical Hepatocellular Carcinoma: Rationale for the Design and Evaluation of Therapeutic Trials. Hepatology 1999, 29, 62–67. [Google Scholar] [CrossRef]
- Thomas, M.B.; Jaffe, D.; Choti, M.M.; Belghiti, J.; Curley, S.; Fong, Y.; Gores, G.; Kerlan, R.; Merle, P.; O’Neil, B.; et al. Hepatocellular Carcinoma: Consensus Recommendations of the National Cancer Institute Clinical Trials Planning Meeting. J. Clin. Oncol. 2010, 28, 3994–4005. [Google Scholar] [CrossRef] [PubMed]
- Galle, P.R.; Tovoli, F.; Foerster, F.; Wörns, M.A.; Cucchetti, A.; Bolondi, L. The Treatment of Intermediate Stage Tumours beyond TACE: From Surgery to Systemic Therapy. J. Hepatol. 2017, 67, 173–183. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver EASL Clinical Practice Guidelines for the Management of Patients with Decompensated Cirrhosis. J. Hepatol. 2018, 69, 406–460. [CrossRef] [PubMed]
- Granito, A.; Facciorusso, A.; Sacco, R.; Bartalena, L.; Mosconi, C.; Cea, U.V.; Cappelli, A.; Antonino, M.; Modestino, F.; Brandi, N.; et al. TRANS-TACE: Prognostic Role of the Transient Hypertransaminasemia after Conventional Chemoembolization for Hepatocellular Carcinoma. JPM 2021, 11, 1041. [Google Scholar] [CrossRef]
- Kudo, M.; Kawamura, Y.; Hasegawa, K.; Tateishi, R.; Kariyama, K.; Shiina, S.; Toyoda, H.; Imai, Y.; Hiraoka, A.; Ikeda, M.; et al. Management of Hepatocellular Carcinoma in Japan: JSH Consensus Statements and Recommendations 2021 Update. Liver Cancer 2021, 10, 181–223. [Google Scholar] [CrossRef]
- Finn, R.S.; Merle, P.; Granito, A.; Huang, Y.-H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Gerolami, R.; Caparello, C.; et al. Outcomes of Sequential Treatment with Sorafenib Followed by Regorafenib for HCC: Additional Analyses from the Phase III RESORCE Trial. J. Hepatol. 2018, 69, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Real, M.I.; Montaña, X.; Planas, R.; Coll, S.; Aponte, J.; Ayuso, C.; Sala, M.; Muchart, J.; Solà, R.; et al. Arterial Embolisation or Chemoembolisation versus Symptomatic Treatment in Patients with Unresectable Hepatocellular Carcinoma: A Randomised Controlled Trial. Lancet 2002, 359, 1734–1739. [Google Scholar] [CrossRef]
- Müller, L.; Stoehr, F.; Mähringer-Kunz, A.; Hahn, F.; Weinmann, A.; Kloeckner, R. Current Strategies to Identify Patients That Will Benefit from TACE Treatment and Future Directions a Practical Step-by-Step Guide. J. Hepatocell. Carcinoma 2021, 8, 403–419. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Han, K.-H.; Ye, S.-L.; Zhou, J.; Huang, Y.-H.; Lin, S.-M.; Wang, C.-K.; Ikeda, M.; Chan, S.L.; Choo, S.P.; et al. A Changing Paradigm for the Treatment of Intermediate-Stage Hepatocellular Carcinoma: Asia-Pacific Primary Liver Cancer Expert Consensus Statements. Liver Cancer 2020, 9, 245–260. [Google Scholar] [CrossRef] [PubMed]
- D’Avola, D.; Granito, A.; de la Torre-Aláez, M.; Piscaglia, F. The Importance of Liver Functional Reserve in the Non-Surgical Treatment of Hepatocellular Carcinoma. J. Hepatol. 2022, 76, 1185–1198. [Google Scholar] [CrossRef] [PubMed]
- Huang, A.; Yang, X.-R.; Chung, W.-Y.; Dennison, A.R.; Zhou, J. Targeted Therapy for Hepatocellular Carcinoma. Signal. Transduct. Target. Ther. 2020, 5, 146. [Google Scholar] [CrossRef]
- Sangro, B.; Chan, S.L.; Meyer, T.; Reig, M.; El-Khoueiry, A.; Galle, P.R. Diagnosis and Management of Toxicities of Immune Checkpoint Inhibitors in Hepatocellular Carcinoma. J. Hepatol. 2020, 72, 320–341. [Google Scholar] [CrossRef]
- Galle, P.R.; Finn, R.S.; Qin, S.; Ikeda, M.; Zhu, A.X.; Kim, T.-Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.; et al. Patient-Reported Outcomes with Atezolizumab plus Bevacizumab versus Sorafenib in Patients with Unresectable Hepatocellular Carcinoma (IMbrave150): An Open-Label, Randomised, Phase 3 Trial. Lancet Oncol. 2021, 22, 991–1001. [Google Scholar] [CrossRef]
- Hsu, C.; Rimassa, L.; Sun, H.-C.; Vogel, A.; Kaseb, A.O. Immunotherapy in Hepatocellular Carcinoma: Evaluation and Management of Adverse Events Associated with Atezolizumab plus Bevacizumab. Ther. Adv. Med. Oncol. 2021, 13, 17588359211031140. [Google Scholar] [CrossRef]
- Gordan, J.D.; Kennedy, E.B.; Abou-Alfa, G.K.; Beg, M.S.; Brower, S.T.; Gade, T.P.; Goff, L.; Gupta, S.; Guy, J.; Harris, W.P.; et al. Systemic Therapy for Advanced Hepatocellular Carcinoma: ASCO Guideline. J. Clin. Oncol. 2020, 38, 4317–4345. [Google Scholar] [CrossRef]
- Greten, T.F.; Sangro, B. Targets for Immunotherapy of Liver Cancer. J. Hepatol. 2017, 68, 157–166. [Google Scholar] [CrossRef]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.-H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.-W.; Han, G.; Jassem, J.; et al. Lenvatinib versus Sorafenib in First-Line Treatment of Patients with Unresectable Hepatocellular Carcinoma: A Randomised Phase 3 Non-Inferiority Trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef] [PubMed]
- Gallage, S.; García-Beccaria, M.; Szydlowska, M.; Rahbari, M.; Mohr, R.; Tacke, F.; Heikenwalder, M. The Therapeutic Landscape of Hepatocellular Carcinoma. Med 2021, 2, 505–552. [Google Scholar] [CrossRef] [PubMed]
- Kelley, R.K.; Yau, T.; Cheng, A.-L.; Kaseb, A.; Qin, S.; Zhu, A.X.; Chan, S.; Sukeepaisarnjaroen, W.; Breder, V.; Verset, G.; et al. VP10-2021: Cabozantinib (C) plus Atezolizumab (A) versus Sorafenib (S) as First-Line Systemic Treatment for Advanced Hepatocellular Carcinoma (AHCC): Results from the Randomized Phase III COSMIC-312 Trial. Ann. Oncol. 2022, 33, 114–116. [Google Scholar] [CrossRef]
- Qin, S.; Chen, Z.; Fang, W.; Ren, Z.; Xu, R.; Ryoo, B.-Y.; Meng, Z.; Bai, Y.; Chen, X.; Liu, X.; et al. Pembrolizumab plus Best Supportive Care versus Placebo plus Best Supportive Care as Second-Line Therapy in Patients in Asia with Advanced Hepatocellular Carcinoma (HCC): Phase 3 KEYNOTE-394 Study. JCO 2022, 40, 383. [Google Scholar] [CrossRef]
- Liu, W.; Quan, B.; Lu, S.; Tang, B.; Li, M.; Chen, R.; Ren, Z.; Yin, X. First-Line Systemic Treatment Strategies for Unresectable Hepatocellular, Carcinoma: A Systematic Review and Network Meta-Analysis of Randomized Clinical Trials. Front. Oncol. 2021, 11, 771045. [Google Scholar] [CrossRef]
- Rasul, K.; Issameldin, A.; Elazzazi, S.; Ghasoub, R.; Gulied, A. Can We Use Sorafenib for Advanced Hepatocellular Carcinoma (HCC) Child Pugh B? Gulf J. Oncol. 2015, 1, 82–84. [Google Scholar]
- Granito, A.; Forgione, A.; Marinelli, S.; Renzulli, M.; Ielasi, L.; Sansone, V.; Benevento, F.; Piscaglia, F.; Tovoli, F. Experience with Regorafenib in the Treatment of Hepatocellular Carcinoma. Therap. Adv. Gastroenterol. 2021, 14, 175628482110169. [Google Scholar] [CrossRef]
- Trevisani, F.; Brandi, G.; Garuti, F.; Barbera, M.A.; Tortora, R.; Casadei Gardini, A.; Granito, A.; Tovoli, F.; De Lorenzo, S.; Inghilesi, A.L.; et al. Metronomic Capecitabine as Second-Line Treatment for Hepatocellular Carcinoma after Sorafenib Discontinuation. J. Cancer Res. Clin. Oncol. 2018, 144, 403–414. [Google Scholar] [CrossRef]
- Cheng, A.-L.; Kang, Y.-K.; Chen, Z.; Tsao, C.-J.; Qin, S.; Kim, J.S.; Luo, R.; Feng, J.; Ye, S.; Yang, T.-S.; et al. Efficacy and Safety of Sorafenib in Patients in the Asia-Pacific Region with Advanced Hepatocellular Carcinoma: A Phase III Randomised, Double-Blind, Placebo-Controlled Trial. Lancet Oncol. 2009, 10, 25–34. [Google Scholar] [CrossRef]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.-F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.-L.; Forner, A.; et al. Sorafenib in Advanced Hepatocellular Carcinoma. N. Engl. J. Med 2008, 359, 378–390. [Google Scholar] [CrossRef] [PubMed]
- Ben Mousa, A. Sorafenib in the Treatment of Advanced Hepatocellular Carcinoma. Saudi. J. Gastroenterol. 2008, 14, 40–42. [Google Scholar] [CrossRef]
- Lopez, P.M.; Villanueva, A.; Llovet, J.M. Systematic Review: Evidence-Based Management of Hepatocellular Carcinoma—An Updated Analysis of Randomized Controlled Trials. Aliment. Pharmacol. Ther. 2006, 23, 1535–1547. [Google Scholar] [CrossRef]
- Tovoli, F.; Ielasi, L.; Casadei-Gardini, A.; Granito, A.; Foschi, F.G.; Rovesti, G.; Negrini, G.; Orsi, G.; Renzulli, M.; Piscaglia, F. Management of Adverse Events with Tailored Sorafenib Dosing Prolongs Survival of Hepatocellular Carcinoma Patients. J. Hepatol. 2019, 71, 1175–1183. [Google Scholar] [CrossRef] [PubMed]
- Kulik, L.; da Fonseca, L.G.; He, A.R.; Rimola, J.; Wilson Woods, A.; Zöllner, Y.F.; Galle, P.R. Potential Impact of IMbrave150 Results in the Evolving Treatment Landscape of Advanced Hepatocellular Carcinoma: A Multidisciplinary Expert Opinion. J. Hepatocell. Carcinoma 2020, 7, 423–433. [Google Scholar] [CrossRef]
- Finn, R.S.; Kudo, M.; Merle, P.; Meyer, T.; Qin, S.; Ikeda, M.; Xu, R.; Edeline, J.; Ryoo, B.; Ren, Z.; et al. LBA34—Primary Results from the Phase III LEAP-002 Study: Lenvatinib plus Pembrolizumab versus Lenvatinib as First-Line (1L) Therapy for Advanced Hepatocellular Carcinoma (AHCC). Ann. Oncol. 2022, 33, S808–S869. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Chan, S.L.; Kudo, M.; Lau, G.; Kelley, R.K.; Furuse, J.; Sukeepaisarnjaroen, W.; Kang, Y.-K.; Dao, T.V.; De Toni, E.N.; et al. Phase 3 Randomized, Open-Label, Multicenter Study of Tremelimumab (T) and Durvalumab (D) as First-Line Therapy in Patients (Pts) with Unresectable Hepatocellular Carcinoma (UHCC): HIMALAYA. JCO 2022, 40, 379. [Google Scholar] [CrossRef]
- Stefanini, B.; Ielasi, L.; Chen, R.; Abbati, C.; Tonnini, M.; Tovoli, F.; Granito, A. TKIs in Combination with Immunotherapy for Hepatocellular Carcinoma. Expert Rev. Anticancer. Ther. 2023, 23, 279–291. [Google Scholar] [CrossRef]
- Finn, R.S.; Ikeda, M.; Zhu, A.X.; Sung, M.W.; Baron, A.D.; Kudo, M.; Okusaka, T.; Kobayashi, M.; Kumada, H.; Kaneko, S.; et al. Phase Ib Study of Lenvatinib plus Pembrolizumab in Patients with Unresectable Hepatocellular Carcinoma. J. Clin. Oncol. 2020, 38, 2960–2970. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Meyer, T.; Cheng, A.-L.; El-Khoueiry, A.B.; Rimassa, L.; Ryoo, B.-Y.; Cicin, I.; Merle, P.; Chen, Y.; Park, J.-W.; et al. Cabozantinib in Patients with Advanced and Progressing Hepatocellular Carcinoma. N. Engl. J. Med. 2018, 379, 54–63. [Google Scholar] [CrossRef]
- AstraZeneca A Randomized, Open-Label, Multi-Center Phase III Study of Durvalumab and Tremelimumab as First-Line Treatment in Patients with Advanced Hepatocellular Carcinoma, 2022. Available online: clinicaltrials.gov (accessed on 25 March 2023).
- Kudo, M. Durvalumab plus Tremelimumab: A Novel Combination Immunotherapy for Unresectable Hepatocellular Carcinoma. Liver Cancer 2022, 11, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Siddique, O.; Yoo, E.R.; Perumpail, R.B.; Perumpail, B.J.; Liu, A.; Cholankeril, G.; Ahmed, A. The Importance of a Multidisciplinary Approach to Hepatocellular Carcinoma. J. Multidiscip. Healthc. 2017, 10, 95–100. [Google Scholar] [CrossRef] [PubMed]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albarrak, J.; Al-Shamsi, H. Current Status of Management of Hepatocellular Carcinoma in The Gulf Region: Challenges and Recommendations. Cancers 2023, 15, 2001. https://doi.org/10.3390/cancers15072001
Albarrak J, Al-Shamsi H. Current Status of Management of Hepatocellular Carcinoma in The Gulf Region: Challenges and Recommendations. Cancers. 2023; 15(7):2001. https://doi.org/10.3390/cancers15072001
Chicago/Turabian StyleAlbarrak, Jasem, and Humaid Al-Shamsi. 2023. "Current Status of Management of Hepatocellular Carcinoma in The Gulf Region: Challenges and Recommendations" Cancers 15, no. 7: 2001. https://doi.org/10.3390/cancers15072001
APA StyleAlbarrak, J., & Al-Shamsi, H. (2023). Current Status of Management of Hepatocellular Carcinoma in The Gulf Region: Challenges and Recommendations. Cancers, 15(7), 2001. https://doi.org/10.3390/cancers15072001