



Subsequent Upper Urinary Tract Carcinoma Related to Worse Survival in Patients Treated with BCG

 ,
,  , , , , and
, , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection and Study Cohort
2.2. Intravesical BCG Treatment after Transurethral Resection of Bladder Tumor (TURBT)
2.3. Surveillance
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
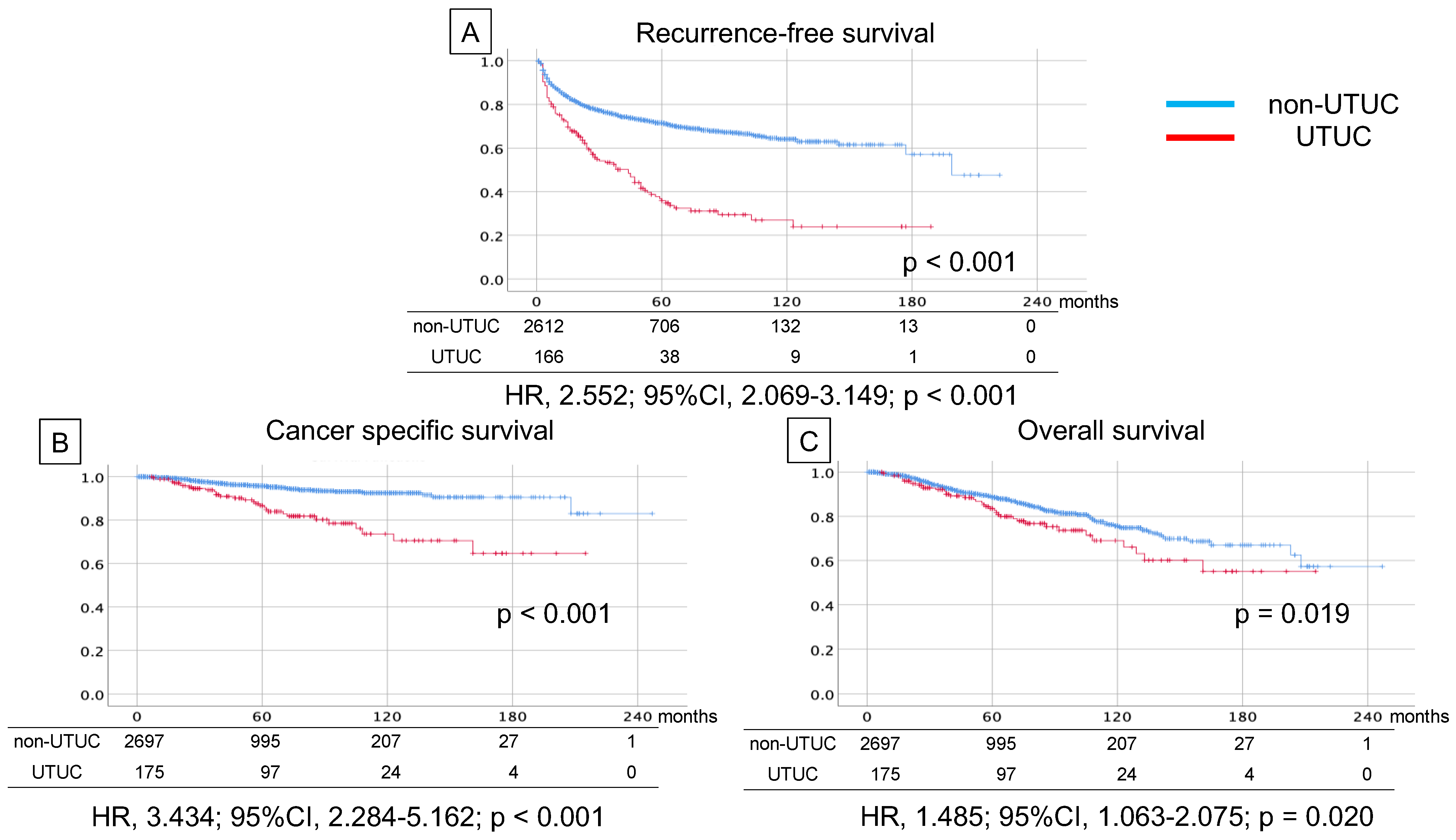
3.2. Survival Analyses
3.3. Analyses of Predictive Factors for Subsequent UTUC after BCG
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Inokuchi, J.; Kuroiwa, K.; Kakehi, Y.; Sugimoto, M.; Tanigawa, T.; Fujimoto, H.; Gotoh, M.; Masumori, N.; Ogawa, O.; Eto, M.; et al. Role of lymph node dissection during radical nephroureterectomy for upper urinary tract urothelial cancer: Multi-institutional large retrospective study JCOG1110A. World J. Urol. 2017, 35, 1737–1744. [Google Scholar] [CrossRef] [PubMed]
- Sfakianos, J.P.; Gul, Z.; Shariat, S.F.; Matin, S.F.; Daneshmand, S.; Plimack, E.; Lerner, S.; Roupret, M.; Pal, S. Genetic Differences between Bladder and Upper Urinary Tract Carcinoma: Implications for Therapy. Eur. Urol. Oncol. 2021, 4, 170–179. [Google Scholar] [CrossRef]
- Roupret, M.; Babjuk, M.; Comperat, E.; Zigeuner, R.; Sylvester, R.J.; Burger, M.; Cowan, N.C.; Gontero, P.; Van Rhijn, B.W.G.; Mostafid, A.H.; et al. European Association of Urology Guidelines on Upper Urinary Tract Urothelial Carcinoma: 2017 Update. Eur. Urol. 2018, 73, 111–122. [Google Scholar] [CrossRef]
- Adibi, M.; Youssef, R.; Shariat, S.F.; Lotan, Y.; Wood, C.G.; Sagalowsky, A.I.; Zigeuner, R.; Montorsi, F.; Bolenz, C.; Margulis, V. Oncological outcomes after radical nephroureterectomy for upper tract urothelial carcinoma: Comparison over the three decades. Int. J. Urol. 2012, 19, 1060–1066. [Google Scholar] [CrossRef] [Green Version]
- Hautmann, R.E.; de Petriconi, R.C.; Pfeiffer, C.; Volkmer, B.G. Radical cystectomy for urothelial carcinoma of the bladder without neoadjuvant or adjuvant therapy: Long-term results in 1100 patients. Eur. Urol. 2012, 61, 1039–1047. [Google Scholar] [CrossRef] [PubMed]
- Nishiyama, N.; Hotta, H.; Takahashi, A.; Yanase, M.; Itoh, N.; Tachiki, H.; Miyao, N.; Matsukawa, M.; Kunishima, Y.; Taguchi, K.; et al. Upper tract urothelial carcinoma following intravesical bacillus Calmette-Guerin therapy for nonmuscle-invasive bladder cancer: Results from a multi-institutional retrospective study. Urol. Oncol. 2018, 36, 306.e9–306.e15. [Google Scholar] [CrossRef] [PubMed]
- Millan-Rodriguez, F.; Chechile-Toniolo, G.; Salvador-Bayarri, J.; Huguet-Perez, J.; Vicente-Rodriguez, J. Upper urinary tract tumors after primary superficial bladder tumors: Prognostic factors and risk groups. J. Urol. 2000, 164, 1183–1187. [Google Scholar] [CrossRef]
- Picozzi, S.; Ricci, C.; Gaeta, M.; Ratti, D.; Macchi, A.; Casellato, S.; Bozzini, G.; Carmignani, L. Upper urinary tract recurrence following radical cystectomy for bladder cancer: A meta-analysis on 13,185 patients. J. Urol. 2012, 188, 2046–2054. [Google Scholar] [CrossRef] [PubMed]
- Gakis, G.; Black, P.C.; Bochner, B.H.; Boorjian, S.A.; Stenzl, A.; Thalmann, G.N.; Kassouf, W. Systematic Review on the Fate of the Remnant Urothelium after Radical Cystectomy. Eur. Urol. 2017, 71, 545–557. [Google Scholar] [CrossRef] [Green Version]
- Seisen, T.; Granger, B.; Colin, P.; Leon, P.; Utard, G.; Renard-Penna, R.; Comperat, E.; Mozer, P.; Cussenot, O.; Shariat, S.F.; et al. A Systematic Review and Meta-analysis of Clinicopathologic Factors Linked to Intravesical Recurrence after Radical Nephroureterectomy to Treat Upper Tract Urothelial Carcinoma. Eur. Urol. 2015, 67, 1122–1133. [Google Scholar] [CrossRef]
- Giannarini, G.; Birkhauser, F.D.; Recker, F.; Thalmann, G.N.; Studer, U.E. Bacillus Calmette-Guerin failure in patients with non-muscle-invasive urothelial carcinoma of the bladder may be due to the urologist’s failure to detect urothelial carcinoma of the upper urinary tract and urethra. Eur. Urol. 2014, 65, 825–831. [Google Scholar] [CrossRef]
- Babjuk, M.; Burger, M.; Comperat, E.M.; Gontero, P.; Mostafid, A.H.; Palou, J.; van Rhijn, B.W.G.; Roupret, M.; Shariat, S.F.; Sylvester, R.; et al. European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (TaT1 and Carcinoma In Situ)—2019 Update. Eur. Urol. 2019, 76, 639–657. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.S.; Bochner, B.H.; Chou, R.; Dreicer, R.; Kamat, A.M.; Lerner, S.P.; Lotan, Y.; Meeks, J.J.; Michalski, J.M.; Morgan, T.M.; et al. Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ASCO/ASTRO/SUO Guideline. J. Urol. 2017, 198, 552–559. [Google Scholar] [CrossRef]
- Matsumoto, H.; Shiraishi, K.; Azuma, H.; Inoue, K.; Uemura, H.; Eto, M.; Ohyama, C.; Ogawa, O.; Kikuchi, E.; Kitamura, H.; et al. Clinical Practice Guidelines for Bladder Cancer 2019 edition by the Japanese Urological Association: Revision working position paper. Int. J. Urol. 2020, 27, 362–368. [Google Scholar] [CrossRef] [PubMed]
- Habuchi, T.; Takahashi, R.; Yamada, H.; Kakehi, Y.; Sugiyama, T.; Yoshida, O. Metachronous multifocal development of urothelial cancers by intraluminal seeding. Lancet 1993, 342, 1087–1088. [Google Scholar] [CrossRef] [PubMed]
- Jones, T.D.; Wang, M.; Eble, J.N.; MacLennan, G.T.; Lopez-Beltran, A.; Zhang, S.; Cocco, A.; Cheng, L. Molecular evidence supporting field effect in urothelial carcinogenesis. Clin. Cancer Res. 2005, 11, 6512–6519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Audenet, F.; Isharwal, S.; Cha, E.K.; Donoghue, M.T.A.; Drill, E.N.; Ostrovnaya, I.; Pietzak, E.J.; Sfakianos, J.P.; Bagrodia, A.; Murugan, P.; et al. Clonal Relatedness and Mutational Differences between Upper Tract and Bladder Urothelial Carcinoma. Clin. Cancer Res. 2019, 25, 967–976. [Google Scholar] [CrossRef] [Green Version]
- Schwalb, M.D.; Herr, H.W.; Sogani, P.C.; Russo, P.; Sheinfeld, J.; Fair, W.R. Positive urinary cytology following a complete response to intravesical bacillus Calmette-Guerin therapy: Pattern of recurrence. J. Urol. 1994, 152, 382–387. [Google Scholar] [CrossRef]
- Merz, V.W.; Marth, D.; Kraft, R.; Ackermann, D.K.; Zingg, E.J.; Studer, U.E. Analysis of early failures after intravesical instillation therapy with bacille Calmette-Guerin for carcinoma in situ of the bladder. Br. J. Urol. 1995, 75, 180–184. [Google Scholar] [CrossRef]
- Herr, H.W. Extravesical tumor relapse in patients with superficial bladder tumors. J. Clin. Oncol. 1998, 16, 1099–1102. [Google Scholar] [CrossRef] [PubMed]
- Niwa, N.; Kikuchi, E.; Matsumoto, K.; Kosaka, T.; Mizuno, R.; Oya, M. Does switching the bacillus Calmette-Guerin strain affect clinical outcome in patients with recurrent non-muscle-invasive bladder cancer after initial bacillus Calmette-Guerin therapy? Urol. Oncol. 2018, 36, 306.e1–306.e8. [Google Scholar] [CrossRef]
- Sakiyama, M.; Kozaki, Y.; Komatsu, T.; Niwa, K.; Suzuki, H.; Ota, M.; Ono, Y.; Miyagawa, Y.; Kiyozumi, T.; Kawana, A. Specificity of tuberculin skin test improved by BCG immunization schedule change in Japan. J. Infect. Chemother. 2021, 27, 1306–1310. [Google Scholar] [CrossRef]
- Kamat, A.M.; Colombel, M.; Sundi, D.; Lamm, D.; Boehle, A.; Brausi, M.; Buckley, R.; Persad, R.; Palou, J.; Soloway, M.; et al. BCG-unresponsive non-muscle-invasive bladder cancer: Recommendations from the IBCG. Nat. Rev. Urol. 2017, 14, 244–255. [Google Scholar] [CrossRef] [PubMed]
- Aragon-Ching, J.B.; Nizam, A.; Henson, D.E. Carcinomas of the Renal Pelvis, Ureters, and Urinary Bladder Share a Carcinogenic Field as Revealed in Epidemiological Analysis of Tumor Registry Data. Clin. Genitourin. Cancer 2019, 17, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Naser-Tavakolian, A.; Ghodoussipour, S.; Djaladat, H. Upper urinary tract recurrence following bladder cancer therapy: A review of surveillance and management. Curr. Opin. Urol. 2019, 29, 189–197. [Google Scholar] [CrossRef]
- Villa, L.; Haddad, M.; Capitanio, U.; Somani, B.K.; Cloutier, J.; Doizi, S.; Salonia, A.; Briganti, A.; Montorsi, F.; Traxer, O. Which Patients with Upper Tract Urothelial Carcinoma Can be Safely Treated with Flexible Ureteroscopy with Holmium:YAG Laser Photoablation? Long-Term Results from a High Volume Institution. J. Urol. 2018, 199, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Volkmer, B.G.; Schnoeller, T.; Kuefer, R.; Gust, K.; Finter, F.; Hautmann, R.E. Upper urinary tract recurrence after radical cystectomy for bladder cancer—Who is at risk? J. Urol. 2009, 182, 2632–2637. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Subsequent Diagnosis with UTUC (N = 175, 5.4%) | ||
|---|---|---|
| Observation duration | Months (range) | 27.8 (0–182) |
| Gender | Male | 132 |
| Female | 43 | |
| Age | Median (range) | 71.0 (28.0–86) |
| Location of UTUC | Renal pelvis | 33 |
| Ureter | 105 | |
| Renal pelvis + ureter | 8 | |
| Not described | 27 | |
| Primary bladder T stage | a or 1 | 124 |
| CIS | 51 | |
| 95% CI | |||||||
|---|---|---|---|---|---|---|---|
| Subsequent UTUC | No UTUC | OR | Lower | Upper | p | ||
| Gender | Male:Female | 132:43 | 2236:462 | 1.577 | 1.102 | 2.256 | 0.018 |
| Age | Median (range) | 71.0 (28.0–86.0) | 72.0 (29.0–97.0) | - | - | - | 0.499 |
| PS | 0:1 or More | 151:15 | 2317:278 | 0.828 | 0.480 | 1.428 | 0.603 |
| Smoking | Previous and present:No | 77:76 | 1461:959 | 1.504 | 1.085 | 2.088 | 0.017 |
| Grade | High:Low | 159:8 | 2324:291 | 2.489 | 1.211 | 5.116 | 0.009 |
| T | 0 and 1:CIS | 124:51 | 2189:512 | 1.758 | 1.252 | 2.470 | 0.002 |
| Concurrent CIS | Yes:No | 81:37 | 1030:591 | 1.256 | 0.840 | 1.877 | 0.277 |
| Multiplicity | Multiple:Solitary | 130:29 | 1825:806 | 1.980 | 1.313 | 2.986 | 0.001 |
| Maximum diameter (cm) | 3 or more:Less than 3 | 33:68 | 438:1638 | 1.815 | 1.182 | 2.787 | 0.009 |
| Appearance | Papillary:Others | 46:114 | 648:1973 | 1.213 | - | - | 0.259 |
| Variant histology | UC:Others | 5:170 | 63:2619 | 1.206 | - | - | 0.607 |
| Lympho-vascular invasion | Yes:No | 10:164 | 117:2581 | 1.345 | 0.692 | 2.615 | 0.343 |
| BCG strain | Connaught:Tokyo | 59:114 | 603:2086 | 1.789 | 1.290 | 2.183 | 0.001 |
| Incomplete BCG induction therapy | Yes:No | 19:156 | 348:2353 | 0.824 | - | - | 0.485 |
| Maintenance Therapy | Yes:No | 24:151 | 493:2208 | 0.712 | 0.458 | 1.107 | 0.154 |
| Recurrence in bladder | Yes:No | 108:66 | 752:1930 | 4.200 | 3.057 | 5.770 | <0.001 |
| Factor | Risk Category | Multivariable | |||
|---|---|---|---|---|---|
| OR | 95% CI | p | |||
| Lower Limit | Upper Limit | ||||
| Gender | female | 1.644 | 0.938 | 2.881 | 0.082 |
| Smoking history | yes | 1.490 | 0.917 | 2.427 | 0.108 |
| Grade | high | 1.405 | 0.591 | 3.342 | 0.442 |
| T | CIS | 1.217 | 0.633 | 2.339 | 0.557 |
| Multiplicity | multiple | 1.681 | 1.005 | 2.812 | 0.048 |
| Tumor diameter | 3 cm≤ | 1.610 | 1.001 | 2.591 | 0.055 |
| Strain | Connaught | 2.211 | 1.380 | 3.543 | 0.001 |
| Intravesical recurrence | yes | 5.097 | 3.225 | 8.056 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Numakura, K.; Miyake, M.; Kobayashi, M.; Muto, Y.; Sekine, Y.; Nishimura, N.; Iida, K.; Shiga, M.; Morizane, S.; Yoneyama, T.; et al. Subsequent Upper Urinary Tract Carcinoma Related to Worse Survival in Patients Treated with BCG. Cancers 2023, 15, 2002. https://doi.org/10.3390/cancers15072002
Numakura K, Miyake M, Kobayashi M, Muto Y, Sekine Y, Nishimura N, Iida K, Shiga M, Morizane S, Yoneyama T, et al. Subsequent Upper Urinary Tract Carcinoma Related to Worse Survival in Patients Treated with BCG. Cancers. 2023; 15(7):2002. https://doi.org/10.3390/cancers15072002
Chicago/Turabian StyleNumakura, Kazuyuki, Makito Miyake, Mizuki Kobayashi, Yumina Muto, Yuya Sekine, Nobutaka Nishimura, Kota Iida, Masanori Shiga, Shuichi Morizane, Takahiro Yoneyama, and et al. 2023. "Subsequent Upper Urinary Tract Carcinoma Related to Worse Survival in Patients Treated with BCG" Cancers 15, no. 7: 2002. https://doi.org/10.3390/cancers15072002
APA StyleNumakura, K., Miyake, M., Kobayashi, M., Muto, Y., Sekine, Y., Nishimura, N., Iida, K., Shiga, M., Morizane, S., Yoneyama, T., Matsumura, Y., Abe, T., Yamada, T., Matsumoto, K., Inokuchi, J., Nishiyama, N., Taoka, R., Kobayashi, T., Kojima, T., ... Habuchi, T. (2023). Subsequent Upper Urinary Tract Carcinoma Related to Worse Survival in Patients Treated with BCG. Cancers, 15(7), 2002. https://doi.org/10.3390/cancers15072002