
Multimodal Data Integration to Predict Severe Acute Oral Mucositis of Nasopharyngeal Carcinoma Patients Following Radiation Therapy
 , ,
, ,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
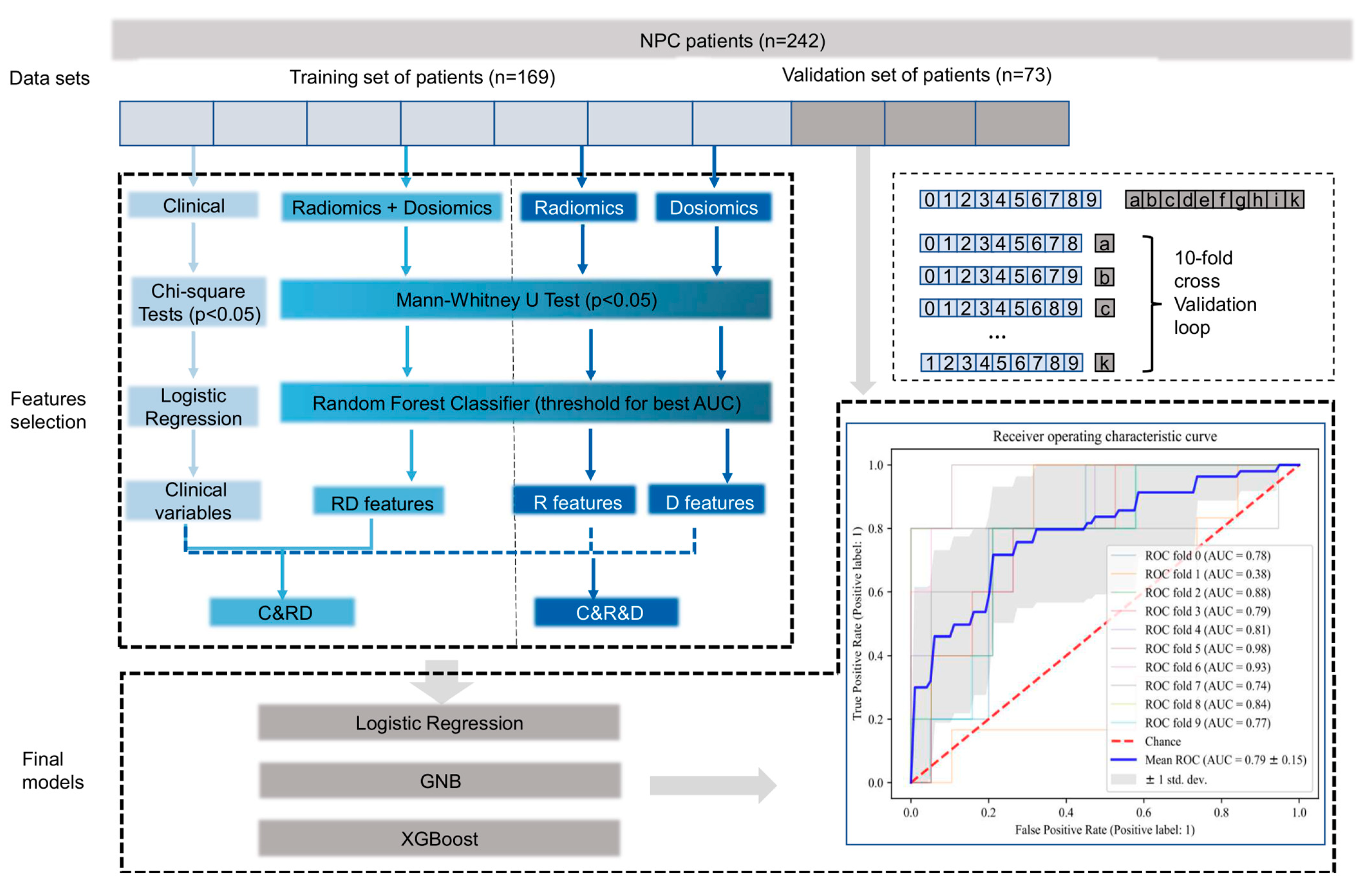
2. Materials and Methods
3. Results
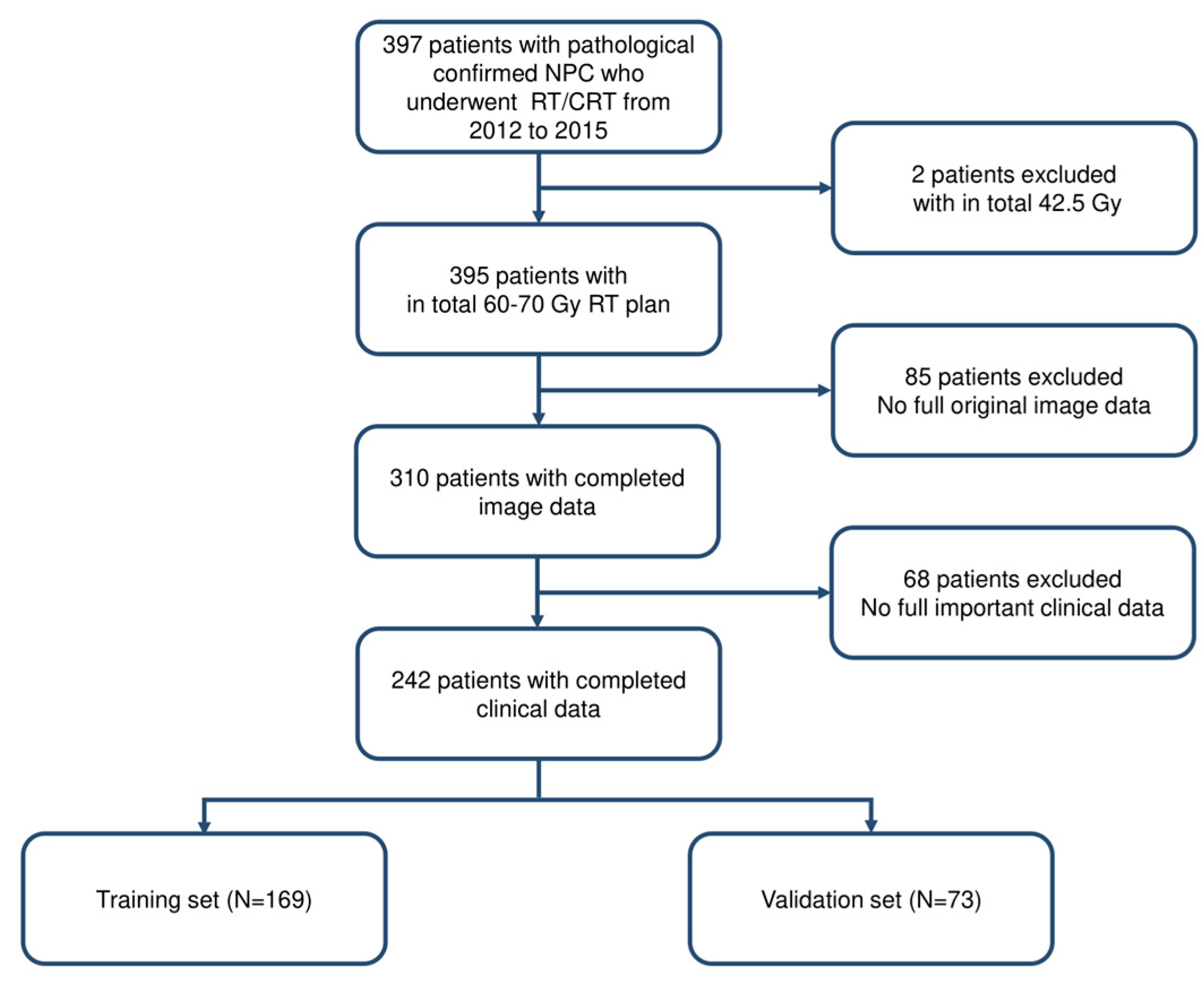
3.1. Patient Characteristics
3.2. Feature Extraction and Model Development
3.2.1. Feature Extraction
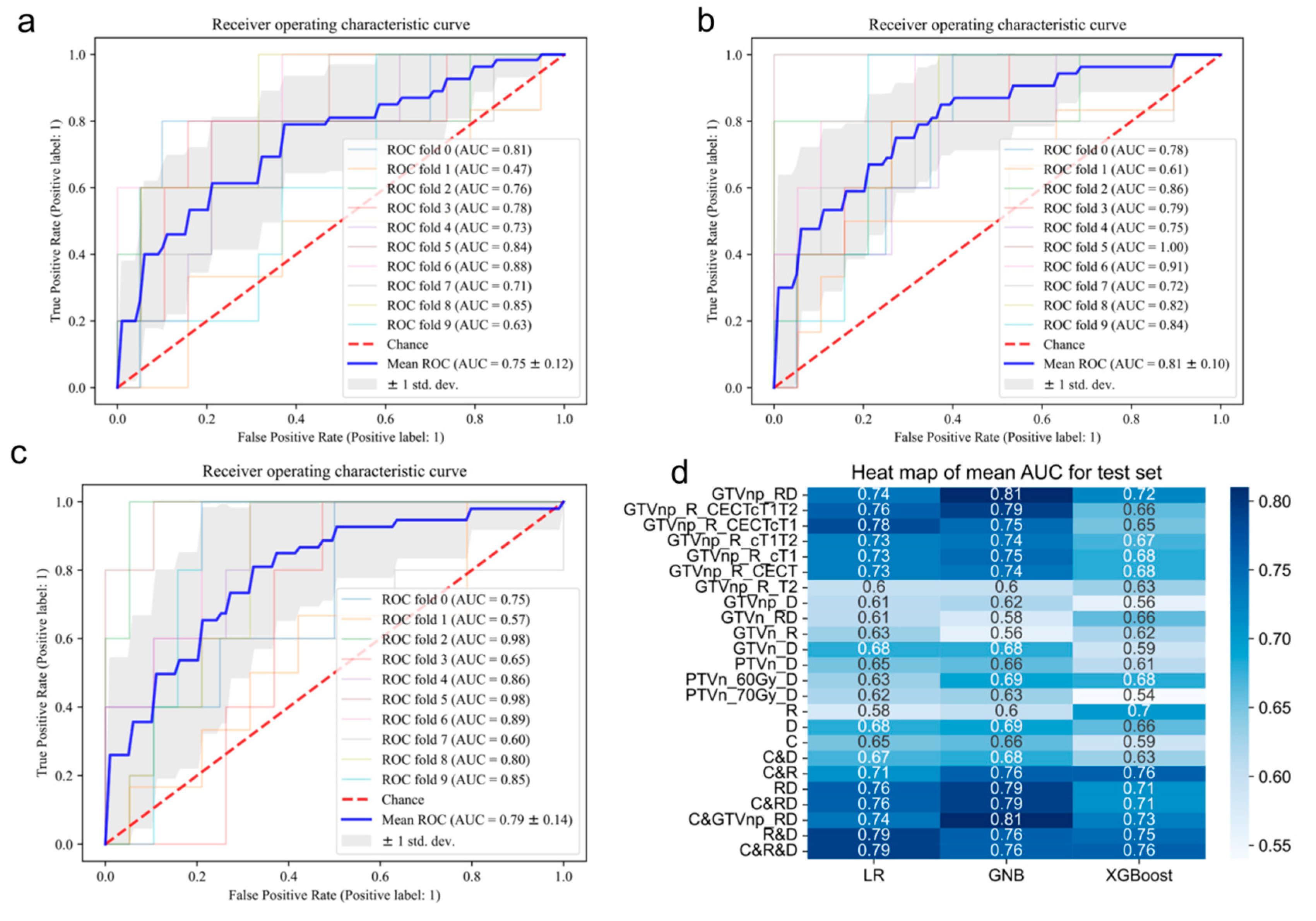
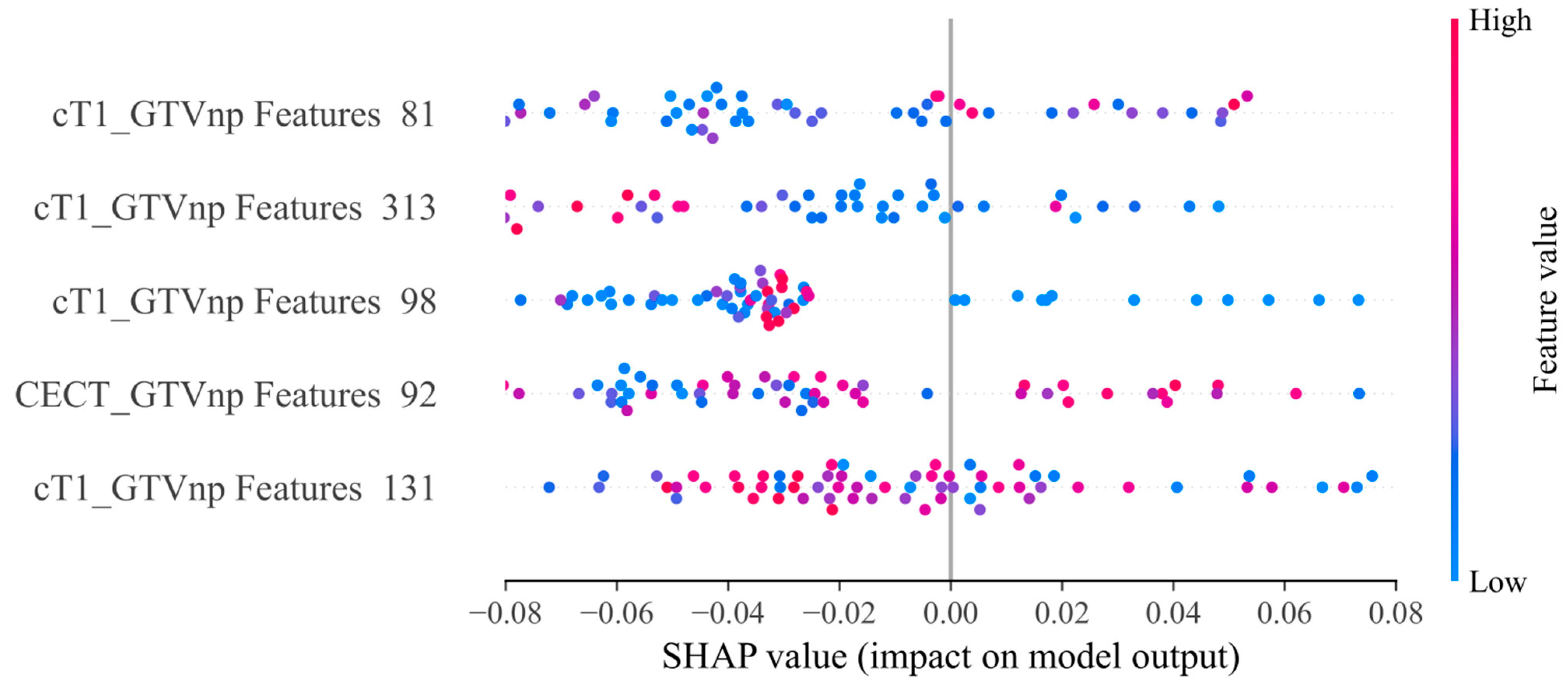
3.2.2. Models
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | CECT |
|---|---|
| Pitch | 1 |
| Kilovoltage (kV) | 120 |
| Current (mAs) | 250–350 |
| Slice thickness (mm) | 3 |
| Matrix | 512 × 512 |
| Scan time (s) | 15 |
| Parameters | T2-STIR | cT1WI |
|---|---|---|
| [TR]/[TE] (ms) | 7640/97 | 739/17 |
| FOV (cm2) | 24 × 24 | 24 × 24 |
| Number of acquisitions | 1 | 1 |
| Slice thickness (mm×slices) | 4 × 25 | 3 × 28 |
| Spacing (cm3) | 0.75 × 0.75 × 4.4 | 0.938 × 0.938 × 3.3 |
| Matrix | 320 × 320 | 256 × 256 |
Appendix C
| Modal of Data | Threshold | Number of Features |
|---|---|---|
| GTVnp_RD | 0.014 | 5 |
| GTVnp_R_CECTcT1T2 | 0.01 | 8 |
| GTVnp_R_CECTcT1 | 0.0125 | 5 |
| GTVnp_R_cT1T2 | 0.125 | 5 |
| GTVnp_R_cT1 | 0.015 | 4 |
| GTVnp_R_CECT | 0.01 | 19 |
| GTVnp_R_T2 | 0.03 | 2 |
| GTVnp_D | 0.024 | 6 |
| GTVn_RD | 0.02 | 7 |
| GTVn_R | 0.03 | 7 |
| GTVn_D | 0.06 | 7 |
| PTVn_D | 0.03 | 3 |
| PTVn_60Gy_D | 0.03 | 12 |
| PTVn_70Gy_D | 0.042 | 1 |
| R | 0.012 | 2 |
| D | 0.016 | 13 |
| RD | 0.005 | 13 |
Appendix D

References
- Chen, Y.-P.; Chan, A.T.C.; Le, Q.-T.; Blanchard, P.; Sun, Y.; Ma, J. Nasopharyngeal carcinoma. Lancet 2019, 394, 64–80. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.T.; Ye, W.; Zeng, Y.-X.; Adami, H.-O. The Evolving Epidemiology of Nasopharyngeal Carcinoma. Cancer Epidemiol. Biomarkers Prev. 2021, 30, 1035–1047. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-P.; Ismaila, N.; Chua, M.L.K.; Colevas, A.D.; Haddad, R.; Huang, S.H.; Wee, J.T.S.; Whitley, A.C.; Yi, J.-L.; Yom, S.S.; et al. Chemotherapy in Combination with Radiotherapy for Definitive-Intent Treatment of Stage II-IVA Nasopharyngeal Carcinoma: CSCO and ASCO Guideline. J. Clin. Oncol. 2021, 39, 840–859. [Google Scholar] [CrossRef]
- Bossi, P.; Chan, A.; Licitra, L.; Trama, A.; Orlandi, E.; Hui, E.; Halámková, J.; Mattheis, S.; Baujat, B.; Hardillo, J.; et al. Nasopharyngeal carcinoma: ESMO-EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 32, 452–465. [Google Scholar] [CrossRef]
- You, R.; Liu, Y.-P.; Huang, P.-Y.; Zou, X.; Sun, R.; He, Y.-X.; Wu, Y.-S.; Shen, G.-P.; Zhang, H.-D.; Duan, C.-Y.; et al. Efficacy and Safety of Locoregional Radiotherapy with Chemotherapy vs Chemotherapy Alone in De Novo Metastatic Nasopharyngeal Carcinoma: A Multicenter Phase 3 Randomized Clinical Trial. JAMA Oncol. 2020, 6, 1345. [Google Scholar] [CrossRef]
- Tang, L.-L.; Guo, R.; Zhang, N.; Deng, B.; Chen, L.; Cheng, Z.-B.; Huang, J.; Hu, W.-H.; Huang, S.H.; Luo, W.-J.; et al. Effect of Radiotherapy Alone vs Radiotherapy with Concurrent Chemoradiotherapy on Survival Without Disease Relapse in Patients with Low-risk Nasopharyngeal Carcinoma: A Randomized Clinical Trial. JAMA 2022, 328, 728–736. [Google Scholar] [CrossRef]
- Wang, K.; Tepper, J.E. Radiation therapy-associated toxicity: Etiology, management, and prevention. CA A Cancer J. Clin. 2021, 71, 437–454. [Google Scholar] [CrossRef]
- Elad, S.; Yarom, N.; Zadik, Y.; Kuten-Shorrer, M.; Sonis, S.T. The broadening scope of oral mucositis and oral ulcerative mucosal toxicities of anticancer therapies. CA A Cancer J. Clin. 2021, 72, 57–77. [Google Scholar] [CrossRef]
- Raber-Durlacher, J.E.; Elad, S.; Barasch, A. Oral mucositis. Oral Oncol. 2010, 46, 452–456. [Google Scholar] [CrossRef] [PubMed]
- McDowell, L.; Corry, J.; Ringash, J.; Rischin, D. Quality of Life, Toxicity and Unmet Needs in Nasopharyngeal Cancer Survivors. Front. Oncol. 2020, 10, 930. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; You, Y.; Lin, C.; Zheng, M.; Hong, C.; Chen, J.; Li, D.; Au, W.W.; Chen, Z. XRCC1 codon 399Gln polymorphism is associated with radiotherapy-induced acute dermatitis and mucositis in nasopharyngeal carcinoma patients. Radiat. Oncol. 2013, 8, 31. [Google Scholar] [CrossRef] [Green Version]
- Yang, D.-W.; Wang, T.-M.; Zhang, J.-B.; Li, X.-Z.; He, Y.-Q.; Xiao, R.; Xue, W.-Q.; Zheng, X.-H.; Zhang, P.-F.; Zhang, S.-D.; et al. Genome-wide association study identifies genetic susceptibility loci and pathways of radiation-induced acute oral mucositis. J. Transl. Med. 2020, 18, 1–12. [Google Scholar] [CrossRef]
- Orlandi, E.; Iacovelli, N.A.; Rancati, T.; Cicchetti, A.; Bossi, P.; Pignoli, E.; Bergamini, C.; Licitra, L.; Fallai, C.; Valdagni, R.; et al. Multivariable model for predicting acute oral mucositis during combined IMRT and chemotherapy for locally advanced nasopharyngeal cancer patients. Oral Oncol. 2018, 86, 266–272. [Google Scholar] [CrossRef]
- Inada, M.; Nishimura, Y.; Ishikura, S.; Ishikawa, K.; Murakami, N.; Kodaira, T.; Ito, Y.; Tsuchiya, K.; Murakami, Y.; Saito, J.; et al. Organs-at-risk dose constraints in head and neck intensity-modulated radiation therapy using a dataset from a multi-institutional clinical trial (JCOG1015A1). Radiat. Oncol. 2022, 17, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Xu, T.; Liu, Y.; Dou, S.; Li, F.; Guan, X.; Zhu, G. Weekly cetuximab concurrent with IMRT aggravated radiation-induced oral mucositis in locally advanced nasopharyngeal carcinoma: Results of a randomized phase II study. Oral Oncol. 2015, 51, 875–879. [Google Scholar] [CrossRef] [PubMed]
- Köstler, W.J.; Hejna, M.; Wenzel, C.; Zielinski, C.C. Oral Mucositis Complicating Chemotherapy and/or Radiotherapy: Options for Prevention and Treatment. CA A Cancer J. Clin. 2001, 51, 290–315. [Google Scholar] [CrossRef] [Green Version]
- Scully, C.; Epstein, J.; Sonis, S. Oral mucositis: A challenging complication of radiotherapy, chemotherapy, and radiochemotherapy: Part 1, pathogenesis and prophylaxis of mucositis. Head Neck 2003, 25, 1057–1070. [Google Scholar] [CrossRef] [PubMed]
- Shu, Z.; Zeng, Z.; Yu, B.; Huang, S.; Hua, Y.; Jin, T.; Tao, C.; Wang, L.; Cao, C.; Xu, Z.; et al. Nutritional Status and Its Association with Radiation-Induced Oral Mucositis in Patients with Nasopharyngeal Carcinoma During Radiotherapy: A Prospective Study. Front. Oncol. 2020, 10, 594687. [Google Scholar] [CrossRef]
- Elting, L.S.; Cooksley, C.D.; Chambers, M.S.; Garden, A.S. Risk, Outcomes, and Costs of Radiation-Induced Oral Mucositis Among Patients with Head-and-Neck Malignancies. Int. J. Radiat. Oncol. Biol. Phys. 2007, 68, 1110–1120. [Google Scholar] [CrossRef]
- Saito, N.; Imai, Y.; Muto, T.; Sairenchi, T. Low body mass index as a risk factor of moderate to severe oral mucositis in oral cancer patients with radiotherapy. Support. Care Cancer 2012, 20, 3373–3377. [Google Scholar] [CrossRef]
- Rosenthal, D.I.; Trotti, A. Strategies for Managing Radiation-Induced Mucositis in Head and Neck Cancer. Semin. Radiat. Oncol. 2009, 19, 29–34. [Google Scholar] [CrossRef]
- Chong, V.; Ong, C. Nasopharyngeal carcinoma. Eur. J. Radiol. 2008, 66, 437–447. [Google Scholar] [CrossRef]
- Xia, P.; Fu, K.K.; Wong, G.W.; Akazawa, C.; Verhey, L.J. Comparison of treatment plans involving intensity-modulated radiotherapy for nasopharyngeal carcinoma. Int. J. Radiat. Oncol. 2000, 48, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Lahat, D.; Adali, T.; Jutten, C. Multimodal data fusion: An overview of methods, challenges, and prospects. Proc. IEEE 2015, 103, 1449–1477. [Google Scholar] [CrossRef] [Green Version]
- Boehm, K.M.; Khosravi, P.; Vanguri, R.; Gao, J.; Shah, S.P. Harnessing multimodal data integration to advance precision oncology. Nat. Rev. Cancer 2021, 22, 114–126. [Google Scholar] [CrossRef] [PubMed]
- Lipkova, J.; Chen, R.J.; Chen, B.; Lu, M.Y.; Barbieri, M.; Shao, D.; Vaidya, A.J.; Chen, C.; Zhuang, L.; Williamson, D.F.; et al. Artificial intelligence for multimodal data integration in oncology. Cancer Cell 2022, 40, 1095–1110. [Google Scholar] [CrossRef]
- Teng, X.; Zhang, J.; Ma, Z.; Zhang, Y.; Lam, S.; Li, W.; Xiao, H.; Li, T.; Li, B.; Zhou, T.; et al. Improving radiomic model reliability using robust features from perturbations for head-and-neck carcinoma. Front. Oncol. 2022, 12, 974467. [Google Scholar] [CrossRef]
- Lam, S.-K.; Zhang, Y.; Zhang, J.; Li, B.; Sun, J.-C.; Liu, C.Y.-T.; Chou, P.-H.; Teng, X.; Ma, Z.-R.; Ni, R.-Y.; et al. Multi-Organ Omics-Based Prediction for Adaptive Radiation Therapy Eligibility in Nasopharyngeal Carcinoma Patients Undergoing Concurrent Chemoradiotherapy. Front. Oncol. 2022, 11, 792024. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Lam, S.; Yu, T.; Teng, X.; Zhang, J.; Lee, F.K.-H.; Au, K.-H.; Yip, C.W.-Y.; Wang, S.; Cai, J. Integration of an imbalance framework with novel high-generalizable classifiers for radiomics-based distant metastases prediction of advanced nasopharyngeal carcinoma. Knowl.-Based Syst. 2021, 235, 107649. [Google Scholar] [CrossRef]
- Li, B.; Zheng, X.; Zhang, J.; Lam, S.; Guo, W.; Wang, Y.; Cui, S.; Teng, X.; Zhang, Y.; Ma, Z.; et al. Lung Subregion Partitioning by Incremental Dose Intervals Improves Omics-Based Prediction for Acute Radiation Pneumonitis in Non-Small-Cell Lung Cancer Patients. Cancers 2022, 14, 4889. [Google Scholar] [CrossRef]
- Li, B.; Ren, G.; Guo, W.; Zhang, J.; Lam, S.-K.; Zheng, X.; Teng, X.; Wang, Y.; Yang, Y.; Dan, Q.; et al. Function-Wise Dual-Omics analysis for radiation pneumonitis prediction in lung cancer patients. Front. Pharmacol. 2022, 13, 971849. [Google Scholar] [CrossRef]
- Hansen, C.; Bertelsen, A.; Zukauskaite, R.; Johnsen, L.; Bernchou, U.; Thwaites, D.; Eriksen, J.; Johansen, J.; Brink, C. Prediction of radiation-induced mucositis of H&N cancer patients based on a large patient cohort. Radiother. Oncol. 2020, 147, 15–21. [Google Scholar] [CrossRef]
- Li, P.-J.; Li, K.-X.; Jin, T.; Lin, H.-M.; Fang, J.-B.; Yang, S.-Y.; Shen, W.; Chen, J.; Zhang, J.; Chen, X.-Z.; et al. Predictive Model and Precaution for Oral Mucositis During Chemo-Radiotherapy in Nasopharyngeal Carcinoma Patients. Front. Oncol. 2020, 10, 596822. [Google Scholar] [CrossRef] [PubMed]
- Dodd, M.J.; Miaskowski, C.; Shiba, G.H.; Dibble, S.L.; Greenspan, D.; MacPhail, L.; Paul, S.M.; Larson, P. Risk factors for chemotherapy-induced oral mucositis: Dental appliances, oral hygiene, previous oral lesions, and history of smoking. Cancer Investig. 1999, 17, 278–284. [Google Scholar] [CrossRef]
- Zwanenburg, A.; Vallières, M.; Abdalah, M.A.; Aerts, H.J.W.L.; Andrearczyk, V.; Apte, A.; Ashrafinia, S.; Bakas, S.; Beukinga, R.J.; Boellaard, R.; et al. The Image Biomarker Standardization Initiative: Standardized Quantitative Radiomics for High-Throughput Image-based Phenotyping. Radiology 2020, 295, 328–338. [Google Scholar] [CrossRef] [Green Version]
- van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin, J.-C.; Pieper, S.; Aerts, H.J.W.L. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef] [Green Version]
- Lowekamp, B.C.; Chen, D.T.; Eibanez, L.; Eblezek, D. The Design of SimpleITK. Front. Neuroinform. 2013, 7, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grégoire, V.; Levendag, P.; Ang, K.K.; Bernier, J.; Braaksma, M.; Budach, V.; Chao, C.; Coche, E.; Cooper, J.S.; Cosnard, G.; et al. CT-based delineation of lymph node levels and related CTVs in the node-negative neck: DAHANCA, EORTC, GORTEC, NCIC, RTOG consensus guidelines. Radiother. Oncol. 2003, 69, 227–236. [Google Scholar] [CrossRef]
- Gabryś, H.S.; Buettner, F.; Sterzing, F.; Hauswald, H.; Bangert, M. Design and Selection of Machine Learning Methods Using Radiomics and Dosiomics for Normal Tissue Complication Probability Modeling of Xerostomia. Front. Oncol. 2018, 8, 35. [Google Scholar] [CrossRef]
- Buettner, F.; Miah, A.B.; Gulliford, S.L.; Hall, E.; Harrington, K.J.; Webb, S.; Partridge, M.; Nutting, C.M. Novel approaches to improve the therapeutic index of head and neck radiotherapy: An analysis of data from the PARSPORT randomised phase III trial. Radiother. Oncol. 2012, 103, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Lundberg, S.M.; Lee, S.I. A unified approach to interpreting model predictions. Adv. Neural Inf. Process. Syst. 2017, 30. [Google Scholar] [CrossRef]
- Satheeshkumar, P.S.; El-Dallal, M.; Mohan, M.P. Feature selection and predicting chemotherapy-induced ulcerative mucositis using machine learning methods. Int. J. Med. Inform. 2021, 154, 104563. [Google Scholar] [CrossRef] [PubMed]
- Rossi, L.; Bijman, R.; Schillemans, W.; Aluwini, S.; Cavedon, C.; Witte, M.; Incrocci, L.; Heijmen, B. Texture analysis of 3D dose distributions for predictive modelling of toxicity rates in radiotherapy. Radiother. Oncol. 2018, 129, 548–553. [Google Scholar] [CrossRef] [PubMed]
- Sanguineti, G.; Sormani, M.P.; Marur, S.; Gunn, G.B.; Rao, N.; Cianchetti, M.; Ricchetti, F.; McNutt, T.; Wu, B.; Forastiere, A. Effect of Radiotherapy and Chemotherapy on the Risk of Mucositis During Intensity-Modulated Radiation Therapy for Oropharyngeal Cancer. Int. J. Radiat. Oncol. 2012, 83, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Dean, J.A.; Wong, K.H.; Welsh, L.C.; Jones, A.-B.; Schick, U.; Newbold, K.L.; Bhide, S.A.; Harrington, K.J.; Nutting, C.M.; Gulliford, S.L. Normal tissue complication probability (NTCP) modelling using spatial dose metrics and machine learning methods for severe acute oral mucositis resulting from head and neck radiotherapy. Radiother. Oncol. 2016, 120, 21–27. [Google Scholar] [CrossRef] [Green Version]
- Giraud, P.; Giraud, P.; Gasnier, A.; El Ayachy, R.; Kreps, S.; Foy, J.-P.; Durdux, C.; Huguet, F.; Burgun, A.; Bibault, J.-E. Radiomics and Machine Learning for Radiotherapy in Head and Neck Cancers. Front. Oncol. 2019, 9, 174. [Google Scholar] [CrossRef] [Green Version]
- Moreno, A.C.; Frank, S.J.; Garden, A.S.; Rosenthal, D.I.; Fuller, C.D.; Gunn, G.B.; Reddy, J.P.; Morrison, W.H.; Williamson, T.D.; Holliday, E.B.; et al. Intensity modulated proton therapy (IMPT)–The future of IMRT for head and neck cancer. Oral Oncol. 2019, 88, 66–74. [Google Scholar] [CrossRef]
- Plevová, P. Prevention and treatment of chemotherapy- and radiotherapy-induced oral mucositis: A review. Oral Oncol. 1999, 35, 453–470. [Google Scholar] [CrossRef]
- Melo, W.W.P.; Aragão, W.A.B.; Baia-Da-Silva, D.C.; Nascimento, P.C.; Lima, R.R.; de Souza-Rodrigues, R.D. Effects of Photobiomodulation on Oral Mucositis: Visualization and Analysis of Knowledge. Life 2022, 12, 1940. [Google Scholar] [CrossRef]
- Araújo, S.N.M.; Luz, M.H.B.A.; da Silva, G.R.F.; Andrade, E.M.L.R.; Nunes, L.C.C.; Moura, R.O. Cancer patients with oral mucositis: Challenges for nursing care. Rev. Latino-Am. Enferm. 2015, 23, 267–274. [Google Scholar] [CrossRef] [Green Version]
- Villa, A.; Vollemans, M.; De Moraes, A.; Sonis, S. Concordance of the WHO, RTOG, and CTCAE v4.0 grading scales for the evaluation of oral mucositis associated with chemoradiation therapy for the treatment of oral and oropharyngeal cancers. Support. Care Cancer 2021, 29, 6061–6068. [Google Scholar] [CrossRef] [PubMed]




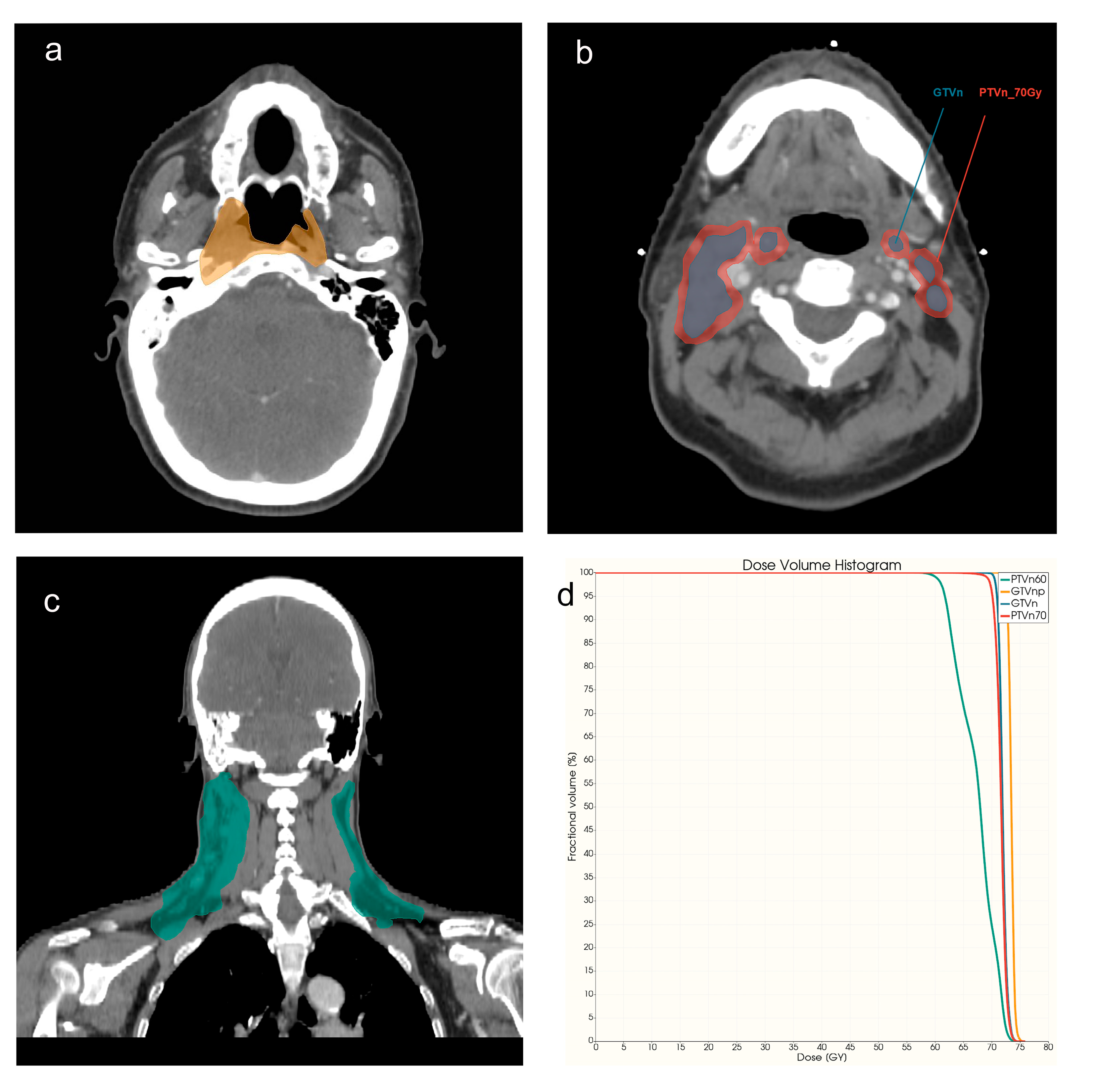
| VOIs | Descriptions of VOI | Imaging Modalities/Images |
|---|---|---|
| GTVnp | Gross tumor volume of primary NPC tumor | CECT, cT1WI, T2WI, DVH |
| GTVn | Metastatic lymph nodes area | CECT, DVH |
| PTVn_70Gy | Regions of nodal planning target volume with | DVH |
| the prescribed dose level of 70Gy | ||
| PTVn_60Gy | PTVn with the prescribed dose level of 60Gy | DVH |
| Name of Model | Methods |
|---|---|
| GTVnp_RD | Integration of radiomics and dosiomics GTVnp data before feature selection |
| GTVnp_R_CECTcT1T2 | Integration of radiomics GTVnp data from CECT, cT1WI, T2WI before feature selection |
| GTVnp_R_CECTcT1 | Integration of radiomics GTVnp data from CECT and cT1WI before feature selection |
| GTVnp_R_cT1T2 | Integration of radiomics GTVnp data from cT1WI and T2WI before feature selection |
| GTVnp_R_cT1 | Single radiomics data from CT1WI |
| GTVnp_R_CECT | Single radiomics data from CECT |
| GTVnp_R_T2 | Single radiomics data from T2WI |
| GTVnp_D | Single dosiomics data from GTVnp |
| GTVn_RD | Integration of radiomics and dosiomics data from GTVn before feature selection |
| GTVn_R | Single radiomics data from GTVn |
| GTVn_D | Single dosiomics data from GTVn |
| PTVn_D | Integration of 60 and 70 Gy dosiomics data before feature selection |
| PTVn_60Gy_D | Single dosiomics data from PTVn_60Gy |
| PTVn_70Gy_D | Single dosiomics data from PTVn_70Gy |
| R | Integration of all radiomics data before feature selection |
| D | Integration of all dosiomics data before feature selection |
| C | Single clinical data |
| C&D | Combine selected clinical and dosiomics data for modeling |
| C&R | Combine selected clinical and radiomics data for modeling |
| RD | Integration of radiomics and dosiomics data before feature selection |
| C&RD | Combine selected clinical and RD data for modeling |
| C>Vnp RD | Combine selected clinical and GTVnp RD data for modeling |
| R&D | Combine selected radiomics and dosiomics data for modeling |
| C&R&D | Combine selected clinical, radiomics and dosiomics data for modeling |
| Characteristics | AOM < Grade 3 (Mild AOM) | AOM ≥ Grade 3 (Severe AOM) | p Value |
|---|---|---|---|
| Total Number | 191 (78.9%) | 51 (21.1%) | |
| Age, mean ± SD, years | 54.89 ± 12.25 | 50.9 ± 10.60 | 0.036 * |
| 18–65 | 149 (61.6%) | 44 (18.1%) | |
| ≥65 | 42 (17.4%) | 7 (2.9%) | 0.192 |
| Gender | |||
| Male | 135 (55.8%) | 41 (16.9%) | |
| Female | 56 (23.1%) | 10 (4.1%) | 0.167 |
| Treatment | 0.004 * | ||
| RT alone | 27 (11.2%) | 0 | |
| CRT | 164 (67.8%) | 51 (21.1%) | 0.031 * |
| T stage | |||
| T1 | 15 (6.2%) | 3 (0.1%) | |
| T2 | 8 (3.3%) | 5 (2.1%) | |
| T3 | 137 (56.6%) | 28 (11.6%) | |
| T4 | 31 (12.8%) | 15 (6.2%) | |
| N stage | 0.091 | ||
| N1 | 28 (11.2%) | 1 (0.4%) | |
| N2 | 142 (58.7%) | 45 (18.6%) | |
| N3 | 20 (8.2%) | 5 (2.1%) | |
| Pathology | |||
| Non-keratinizing squamous cell | 175 (72.3%) | 48 (19.8%) | 0.556 |
| Keratinizing squamous-cell carcinoma | 16 (6.6%) | 3 (1.3%) | 0.487 |
| Past health condition | |||
| Past health good | 92 (38.0%) | 27 (11.2%) | |
| Basic diseases/cancer | 99 (40.9%) | 24 (9.9%) | 0.545 |
| Allegory of History | |||
| No known drug allergies | 176 (72.7%) | 46 (19.0%) | |
| Allergy history | 15 (6.2%) | 5 (2.1%) | 0.653 |
| Vision | |||
| Normal | 189 (78.1%) | 51 (21.1%) | |
| With eye impairment | 2 (0.8%) | 0 | 0.463 |
| Hearing | |||
| Normal | 186 (76.9%) | 48 (19.8%) | |
| With hearing impairment | 5 (2.1%) | 3 (1.2%) | 0.247 |
| Habits | |||
| Smoking | 9 (3.7%) | 6 (2.5%) | 0.044 * |
| Non-smoker | 182 (75.2%) | 45 (18.6%) | |
| Drinking | 4 (1.7%) | 1 (0.4%) | |
| No alcohol consumption | 187 (77.3%) | 50 (20.7%) | 0.953 |
| Height, mean ± SD, cm | 163.4 ± 8.5 | 165.0 ± 8.0 | 0.561 |
| Body weight, mean ± SD, kg | 63.1 ± 11.9 | 66.2 ± 14.6 | |
| 1st week of RT | 1.599 | ||
| 2nd week of RT | 62.0 ± 11.8 | 64.9 ± 14.5 | 1.5 |
| 3rd week of RT | 61.2 ± 11.4 | 63.9 ± 14.1 | 0.116 |
| 4th week of RT | 60.2 ± 11.3 | 62.8 ± 14.0 | 1.418 |
| BMI | |||
| 1st week of RT | |||
| <25 | 131 (54.1%) | 32 (13.2%) | |
| ≥25 | 60 (24.8%) | 19 (7.9%) | 0.429 |
| 2nd week of RT | |||
| <25 | 131 (54.1%) | 51 (21.1%) | |
| ≥25 | 60 (24.8%) | 22 (9.1%) | 0.116 |
| 3rd week of RT | |||
| <25 | 131 (54.1%) | 31 (12.8%) | |
| ≥25 | 55 (22.7%) | 20 (8.3%) | 0.153 |
| 4th week of RT | |||
| <25 | 142 (58.7%) | 34 (14.0%) | |
| ≥25 | 49 (20.2%) | 17 (7.0%) | 0.274 |
| Variables | p-Value | 95% Confidence Interval | |
|---|---|---|---|
| Lower 95% Bound | Upper 95% Bound | ||
| Age (18, 65) | 0.802 | 0.345 | 2.274 |
| T | 0.007 * | ||
| T 1 | 0.591 | 0.149 | 2.96 |
| T 2 | 0.069 | 0.881 | 29.854 |
| T 3 | 0.024 * | 0.195 | 0.891 |
| RT alone | 0.998 | 0 | . |
| Smoker | 0.043 * | 1.037 | 10.683 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dong, Y.; Zhang, J.; Lam, S.; Zhang, X.; Liu, A.; Teng, X.; Han, X.; Cao, J.; Li, H.; Lee, F.K.; et al. Multimodal Data Integration to Predict Severe Acute Oral Mucositis of Nasopharyngeal Carcinoma Patients Following Radiation Therapy. Cancers 2023, 15, 2032. https://doi.org/10.3390/cancers15072032
Dong Y, Zhang J, Lam S, Zhang X, Liu A, Teng X, Han X, Cao J, Li H, Lee FK, et al. Multimodal Data Integration to Predict Severe Acute Oral Mucositis of Nasopharyngeal Carcinoma Patients Following Radiation Therapy. Cancers. 2023; 15(7):2032. https://doi.org/10.3390/cancers15072032
Chicago/Turabian StyleDong, Yanjing, Jiang Zhang, Saikt Lam, Xinyu Zhang, Anran Liu, Xinzhi Teng, Xinyang Han, Jin Cao, Hongxiang Li, Francis Karho Lee, and et al. 2023. "Multimodal Data Integration to Predict Severe Acute Oral Mucositis of Nasopharyngeal Carcinoma Patients Following Radiation Therapy" Cancers 15, no. 7: 2032. https://doi.org/10.3390/cancers15072032
APA StyleDong, Y., Zhang, J., Lam, S., Zhang, X., Liu, A., Teng, X., Han, X., Cao, J., Li, H., Lee, F. K., Yip, C. W., Au, K., Zhang, Y., & Cai, J. (2023). Multimodal Data Integration to Predict Severe Acute Oral Mucositis of Nasopharyngeal Carcinoma Patients Following Radiation Therapy. Cancers, 15(7), 2032. https://doi.org/10.3390/cancers15072032